
UC SF Carotid Body Tumor UC SF Mass Left Side of Neck PDFs...A. Malignant carotid body tumor B....
9
1 UC SF VASCULAR SURGERY • UC SAN FRANCISCO Carotid Body Tumor How to Get It Out Charles Eichler, MD San Francisco, Ca April 16, 2015 UC SF VASCULAR SURGERY • UC SAN FRANCISCO Mass Left Side of Neck • 55yo m with 10 yr hx of mass on left side of neck—assx except for swelling • 5 yrs ago, attempted resection • f/u neck radiation • Represents 6 months ago -5cm mass UC SF VASCULAR SURGERY • UC SAN FRANCISCO CT-intensely enhancing mass splaying carotid bifrucation UC SF VASCULAR SURGERY • UC SAN FRANCISCO
Transcript of UC SF Carotid Body Tumor UC SF Mass Left Side of Neck PDFs...A. Malignant carotid body tumor B....
1
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Carotid Body TumorHow to Get It Out
Charles Eichler, MD
San Francisco, Ca
April 16, 2015
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
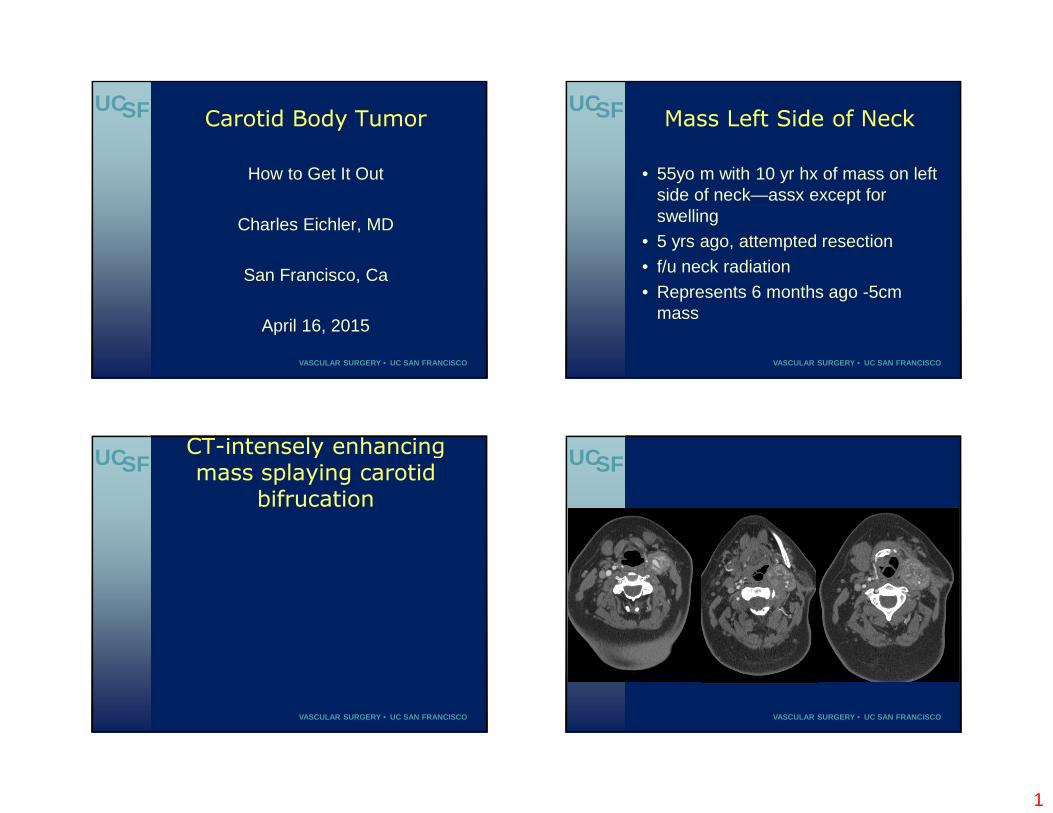
Mass Left Side of Neck• 55yo m with 10 yr hx of mass on left
side of neck—assx except for swelling
• 5 yrs ago, attempted resection
• f/u neck radiation
• Represents 6 months ago -5cm mass
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
CT-intensely enhancing mass splaying carotid
bifrucationUCSF
VASCULAR SURGERY • UC SAN FRANCISCO
2
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
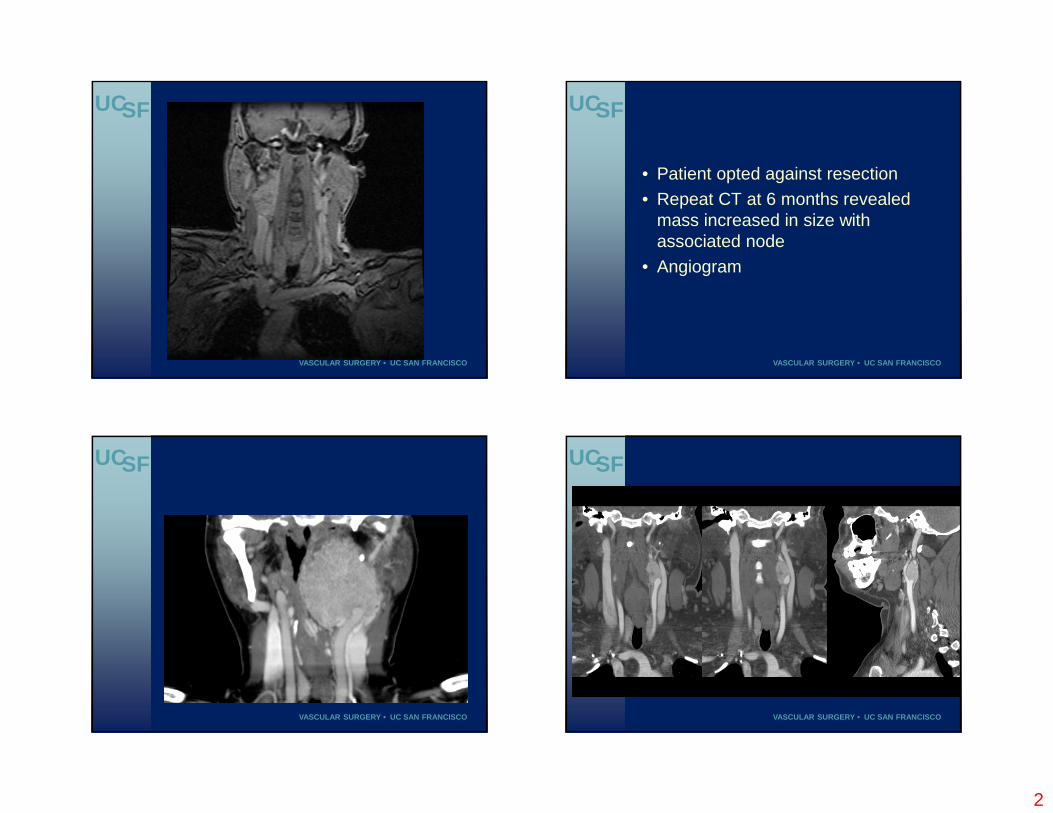
• Patient opted against resection
• Repeat CT at 6 months revealed mass increased in size with associated node
• Angiogram
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO

3
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• DX???
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
What is the most likely diagnosis?
A. Malignant carotid body tumor
B. Schwannoma
C. SarcomaD. Metastatic disease
E. None of the above
67%
0%
22%
0%
11%
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Paragangliomas Uncommon neuroendocrine tumors arising from extraadrenal paraganglia of the autonomic nervous system
Head/neck-carotid bifrucation---CBT
Most common-1:30,000
4
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Presentation
• Painless neck mass
• Functionally active tumor is extremely rare
• Cranial neuropathy in very large tumors
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
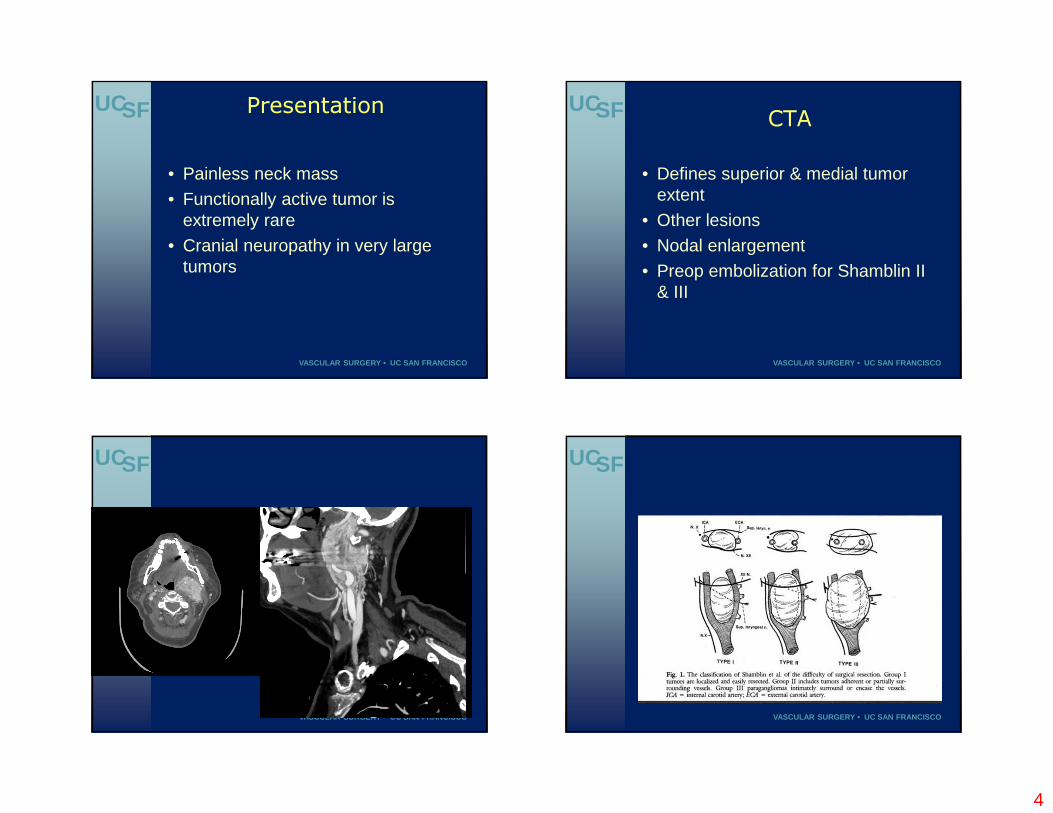
CTA• Defines superior & medial tumor
extent
• Other lesions
• Nodal enlargement
• Preop embolization for Shamblin II & III
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
5
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• Tumors are most often benign
• Malignancy seen in 6-10%-usually dx’d by resection and evidence of local invasion
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Surgical management only curative rx
Challenging-cr n injury>15% as well as high risk of vascular comlplication
Predicted by Shamblin class
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
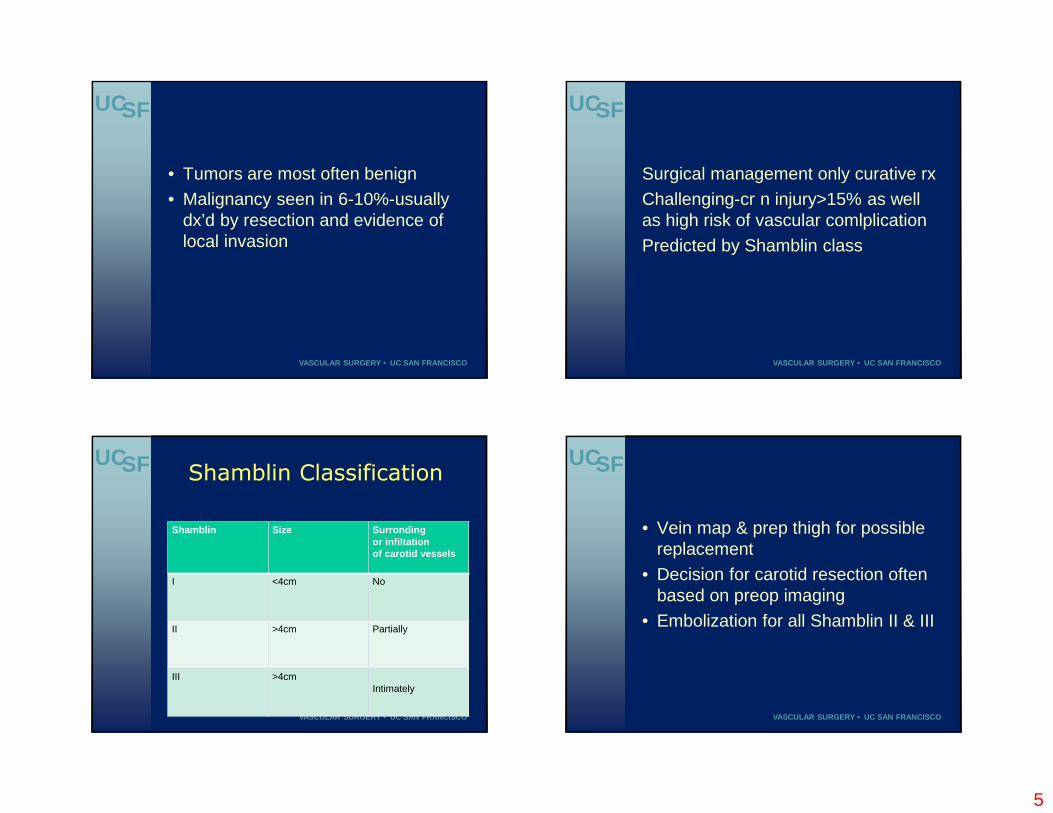
Shamblin ClassificationShamblin Size Surronding
or infiltationof carotid vessels
I <4cm No
II >4cm Partially
III >4cmIntimately
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• Vein map & prep thigh for possible replacement
• Decision for carotid resection often based on preop imaging
• Embolization for all Shamblin II & III

6
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
How I do itNasotracheal intubation
Allows for mobilization of the jaw making subluxation of the jaw rare
Work with OHNS for large tumors for resection of styloid process and possible mandibulectomy
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• Vertical incision or transverse
• Develop field bordered by omohyoid, diagartic, IJV, pharynx
• Large tumors require parotid mobilization and diagastric division requiring ID of facial n
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• Identify vagus & hypoglossal nerves early in the dissection
• Superior laryngeal n lies behind the tumor
• Facial, and IX and XI may also be involed with large tumors
• Use of bipolar very helpful
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
• Isolate CCA, ICA & ECA
• Free tumor away from these vessels in cranial to caudal direction
• Bifrucation last
• Resection of ICA with very large tumors
• Measure stump pressures & shunt if appropriate
7
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
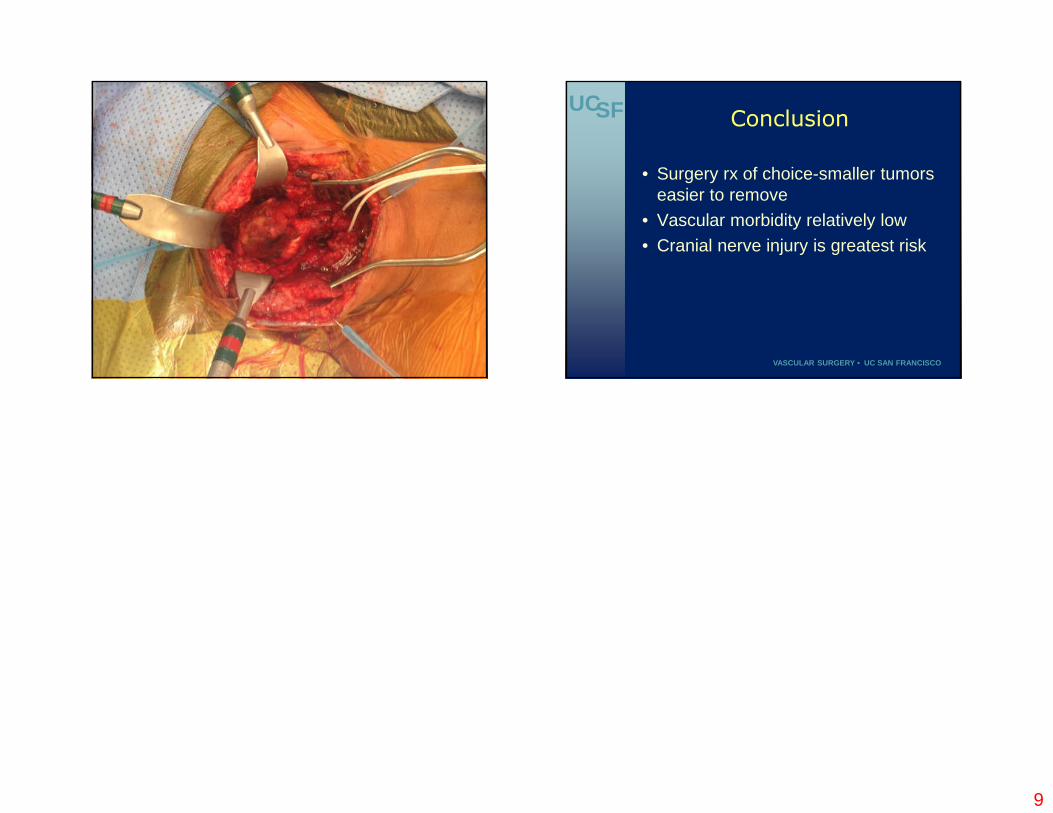
• Completely free tumor away from the vessels
• Resect mass posteriorly from bottom to top extent and remove
• If needed, vein graft replacement
• Close w or w/o drain
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Recent case • Patient presented to OSH large
neck mass
• CTA c/w CBT
• Attempt resection-aborted due to bleeding and unexplained hypotension
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
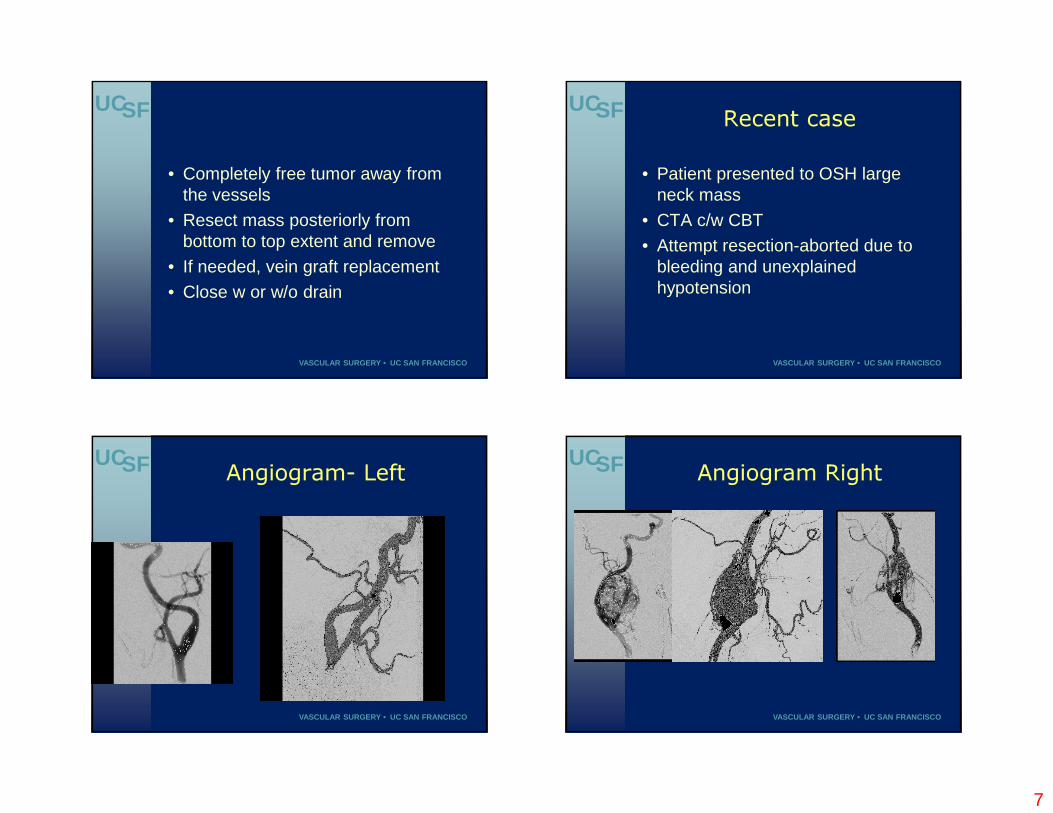
Angiogram- Left UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Angiogram Right

8
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
9
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
UCSF
VASCULAR SURGERY • UC SAN FRANCISCO
Conclusion • Surgery rx of choice-smaller tumors
easier to remove
• Vascular morbidity relatively low
• Cranial nerve injury is greatest risk


















