UA/NSTEMI Guidelines Audio-Webcast: A Presentation & Discussion of Treatment Essentials Based on the...
23
UA/NSTEMI Guidelines Audio-Webcast: A Presentation & Discussion of Treatment Essentials Based on the ACC/AHA Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the ACC/AHA Task Force on Practice Guidelines Writing Committee to Revise the 2002 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction. Presented by: Jeffrey L. Anderson, MD, FACC, Moderator Elliott M. Antman, MD, FACC Robert M. Califf, MD, MACC A. Michael Lincoff, MD, FACC
-
date post
20-Dec-2015 -
Category
Documents
-
view
216 -
download
3
Transcript of UA/NSTEMI Guidelines Audio-Webcast: A Presentation & Discussion of Treatment Essentials Based on the...

UA/NSTEMI Guidelines Audio-Webcast:
A Presentation & Discussion of Treatment Essentials
Based on the ACC/AHA Guidelines for the Management of Patients With Unstable
Angina/Non-ST-Elevation Myocardial Infarction: A Report of the ACC/AHA Task
Force on Practice Guidelines Writing Committee to Revise the 2002 Guidelines for the Management of Patients with Unstable
Angina/Non-ST-Elevation Myocardial Infarction. Presented by:
Jeffrey L. Anderson, MD, FACC, ModeratorElliott M. Antman, MD, FACCRobert M. Califf, MD, MACC
A. Michael Lincoff, MD, FACC

AstraZeneca
Bristol-Myers Squibb
Merck
Sanofi
ThromboVision
DisclosuresJeffrey L. Anderson, MD, FACC

DisclosuresElliott M. Antman, MD, FACC
Accumetrics Inotek Pharmaceuticals Corp.
Amgen, Inc. Integrated Therapeutics Corp.
AstraZeneca Merck
Bayer Healthcare LLC Millennium
Biosite Novartis Pharmaceuticals
Boehringer Mannheim The National Institutes of Health
Beckman Coulter, Inc. Nuvelo, Inc.
Bristol-Myers Squibb Ortho-Clinical Diagnostics, Inc.
Centocor Pfizer, Inc.
CV Therapeutics Roche Diagnostics GmbH
Dade Sanofi-Aventis Research Institute
Dendrion Sanofi-Synthelabo Recherche
Eli Lilly * Schering-Plough
Genentech Sunoz Molecular
GlaxoSmithKline The National Institutes of Health

Abbott Laboratories AstraZeneca Boston Scientific Corautus Genetics, Inc.
Abbott Vascular Devices Aventis Bracco Diagnostics Cordis
Acorn Cardiovascular Aviron Flu Mist Bristol-Myers Squibb Corgentech
Actelion Bayer AG CanAm Bioresearch, Inc. Covalent Group
Acushphere, Inc. Bayer Corp Cardiac Sciences, Inc. Critical Therapeutics, Inc.
Advanced CV Systems Berlex Cardiodynamics CryoVascular Systems, Inc.
Advanced Stent Tech Biocompatibles, Ltd CardioKinetix, Inc. CTS Durham
Agilent Technologies Biogen Caro Research Cubist Pharmaceuticals
Ajinomoto Bioheart Celsion Corp. CV Therapeutics, Inc.
Alexion Biomarin Centocor Dade Behring
Allergan Bionsense Webster, Inc. Chase Medical Daiichi
Alsius Biosite Chugai Biopharmaceuticals, Inc.
Dupont
Amgen Biotronik Coley Pharma Group Dyax
Amylin Pharmaceuticals Biotechnology General Corp
Conceptis Echosens, Inc.
Ark Therapeutics, Ltd. Boehringer Ingleheim Conor Medsystems, Inc. Eclipse Surgical Technologies
DisclosuresRobert M. Califf, MD, MACC

Edwards Lifesciences Genzyme Corporation Inhibitex Medco Health Solutions
Enzon Gilead INO Therapeutics Medicure
Ernst and Young GlaxoSmithKline Integris Medi-Flex, Inc.
Esai Guidant InterMune Pharmaceuticals Medimmune
Ev3, Inc. Guilford Pharmaceuticals ISIS Pharmaceuticals Medtronic
Evalve, Inc. Hemosol IOMED Medtronic Vascular, Inc.
First Circle Medical, Inc. Hewlett Packard Johnson & Johnson Merck
First Horizon Human Genome Sciences Jomed, Inc. MicroMed Tech, Inc.
Flow Cardia, Inc. Humana KAI Pharmaceuticals Millenium Pharmaceutical
Fox Hollow Pharmaceuticals
IDB Medical Kerberos Proximal, Inc. Mitsubishi
Fujisawa Idun Pharmaceuticals, Inc. King Pharmaceuticals Mycosol, Inc.
Genentech Immunex Kuhera Myogen
General Electric Healthcare
Indenix Pharmaceuticals Lilly NABI
General Electric Medical Systems
INFORMD, Inc. Lumen Biomedical NitroMed
Genome Canada InfraReDx MedAcoustics NITROX
DisclosuresRobert M. Califf, MD, MACC

NovaCardia, Inc. Regado Biosciences, Inc.
Summit Vicuron Pharmaceutical
Novartis, AG Group Roche Diagnostic Corp Suneis Wyeth-Ayerst
Novartis Pharmaceutical Roche Holdings, Ltd. Synaptic XOMA
Organon International Roche Labs Synthetic Blood International Xsira Pharmaceutical
Ortho Biotech Salix Pharmaceuticals Terumo Corp XTL Biopharmaceuticals
Osiris Therapeutics, Inc. Sanofi Pasteur The Medicines Company Xylum
Otsuka America Pharmaceutical, Inc.
Sanofi-Aventis Theravance Yamanouchi
Pathway Medical Tech Sanofi-Synthelabo TherOx, Inc.
Pfizer Schering-Plough Titan Pharmaceuticals, Inc.
Pharmacia/Upjohn Scios Valeant Pharmaceuticals
Pharmanetics, Inc. Searle Valentis, Inc.
Pharsight Sicel Technologies Velocimed
Proctor and Gamble Siemens Veridex
Prometheus SmithKlineBeecham Vertex Pharmaceuticals
Recom Managed Systems Spectranetics VIASYS Healthcare, Inc.
DisclosuresRobert M. Califf, MD, MACC

Alexion Pharm Medtronic
Amer Bioscience Novartis
AstraZeneca Pfizer
Atherogenics Pharmacia Upjohn
Biosite Philips
Centocor Orphan Therapeutic
Converge Medical Sankyo
Cordis Sanofi
Dr. Reddy’s Laboratory Scios
Eli Lilly * Takeda America
GlaxoSmithKline The Medicines Company
Glaxo Wellcome Vasogenix
Guilford
DisclosuresA. Michael Lincoff, MD, FACC

19901990 19921992 19941994 19961996 19981998 20002000 2002200219901990
ACC/AHAACC/AHAAMI AMI
R. GunnarR. Gunnar
19941994AHCPR/AHCPR/NHLBINHLBI
UA UA E. BraunwaldE. Braunwald
19961996 19991999 RevRev UpdUpd ACC/AHA AMI ACC/AHA AMI T. Ryan T. Ryan
2004 2004 20072007 Rev Rev Upd Upd ACC/AHA STEMI ACC/AHA STEMI
E. AntmanE. Antman
2000 2002 2000 2002 2007 2007 Rev UpdRev Upd RevRev
ACC/AHA UA/NSTEMI ACC/AHA UA/NSTEMI E. Braunwald J. AndersonE. Braunwald J. Anderson
20042004 20072007
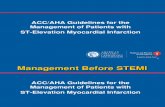
Figure 1. Evolution of Guidelines for Management of Patients with AMI
The first guideline published by the ACC/AHA described the management of patients with acute myocardial infarction (AMI). The subsequent three documents were the Agency for Healthcare and Quality/National Heart, Lung and Blood Institute sponsored guideline on management of unstable angina (UA), the revised/updated ACC/AHA guideline on AMI, and the revised/updated ACC/AHA guideline on unstable angina/non-ST segment myocardial infarction (UA/NSTEMI). The present guideline is a revision and deals strictly with the management of patients presenting with ST segment elevation myocardial infarction (STEMI). The names of the chairs of the writing committees for each of the guidelines are shown at the bottom of each box. Rev, Revised; Upd, Update
Evolution of Guidelines for ACS

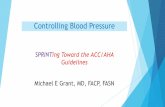
Hospitalizations in the U.S. Due to Acute Coronary Syndromes (ACS)
Acute Coronary Syndromes*
1.57 Million Hospital Admissions - ACS
UA/NSTEMI† STEMI
1.24 million Admissions per year
.33 million Admissions per year
Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69-171. *Primary and secondary diagnoses. †About 0.57 million
NSTEMI and 0.67 million UA.

Risk Stratification

Risk Stratification
1. Integral prerequisite to decision makinga) Intensive initial assessmentb) Continuous clinical assessmentc) Targeted ECG and marker data
2. Risk based on contingent probabilitiesa) Probability of obstructive CAD causing ischemiab) Risk given presence of obstructive CAD
3. Risk scores should be a routine part of assessment throughout the hospital course and periodically after discharge

Risk Assessment Dependent on Contingent Probabilities
• Likelihood of obstructive CAD as cause of symptoms– Dominated by acute
findings• Exam• Symptoms• Markers
– Traditional risk factors are of limited utility
• Does this patient have symptoms due to acute ischemia from obstructive CAD?
• Risk of bad outcome– Dominated by
acute findings• Older age very
important• Hemodynamic
abnormalities critical
• ECG, markers
• What is the likelihood of death, MI, heart failure?

24h 3-4 days 6 months
Ris
k
Physiological monitoring
Periodic physical exams
Cardiac markers
ECG
Time

Risk Scores
TIMI GRACE Future
Histo
ry
AgeHypertensionDiabetesSmoking↑cholesterolFamily historyHistory of CAD
Age Continuous assessment
Pre
sen
tatio
n
Severe anginaAspirin within 7 daysElevated markersST segment deviation
Heart rateSystolic BPElevated markersHeart failureCardiac arrestElevated markersST segment deviation
New markers
Electronic health records

Early Hospital Care

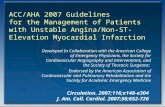
Algorithm for Patients with UA/NSTEMI Managed by an Initial Invasive Strategy
Proceed to Diagnostic Angiography
ASA (Class I, LOE: A)Clopidogrel if ASA intolerant (Class I,
LOE: A)
Diagnosis of UA/NSTEMI is Likely or Definite
Invasive StrategyInitiate A/C Rx (Class I, LOE: A)
Acceptable options: enoxaparin or UFH (Class I, LOE: A) bivalirudin or fondaparinux (Class I, LOE: B)
Select Management StrategyProceed with an
Initial Conservative
Strategy
Anderson JL. J Am Coll Cardiol 2007;50:e1-157. Figure 7
A
B
B1
B2
Prior to AngiographyInitiate at least one (Class I, LOE: A) or both (Class IIa, LOE: B) of the following:
ClopidogrelIV GP IIb/IIIa inhibitor
Factors favoring admin of both clopidogrel and GP IIb/IIIa inhibitor include:
Delay to AngiographyHigh Risk Features
Early recurrent ischemic discomfort

Initiate clopidogrel (Class I, LOE: A) Consider adding IV eptifibatide or tirofiban (Class
IIb, LOE: B)
Conservative StrategyInitiate A/C Rx (Class I, LOE: A):
Acceptable options: enoxaparin or UFH (Class I, LOE: A) or fondaparinux (Class I, LOE: B), but
enoxaparin or fondaparinux are preferable (Class IIA, LOE: B)
Select Management Strategy
ASA (Class I, LOE: A)Clopidogrel if ASA intolerant (Class I, LOE: A)
Diagnosis of UA/NSTEMI is Likely or Definite
Algorithm for Patients with UA/NSTEMI Managed by an Initial Conservative Strategy
Proceed with Invasive Strategy
(Continued)Anderson JL. J Am Coll Cardiol 2007;50:e1-157. Figure 8
C2
C1
A

Any subsequent events necessitating angiography?
EF greater than 0.40
Evaluate LVEF
Low Risk
Cont ASA indefinitely (Class I, LOE A) Cont clopidogrel for at least one month (Class I, LOE A) and ideally up to
1 yr (Class I, LOE B)DC IV GP IIb/IIIa if started previously (Class I, LOE A)
DC A/C Rx (Class I, LOE A)
(Class I, LOE: B)
Proceed to Dx Angiography
Yes
EF 0.40 or less Stress Test
(Class I, LOE: A)
No
Not Low Risk
(Class IIa, LOE: B)
Algorithm for Patients with UA/NSTEMI Managed by an Initial Conservative Strategy
(Continued)
Anderson JL. J Am Coll Cardiol 2007;50:e1-157. Figure 8
(Class I, LOE: A)
(Class IIa, LOE: B)
O
L
MN
K
E-1 E-2
D
(Class I,
LOE: B)

Revascularization and Late Hospital Care

• Cont ASA (Class I, LOE: A)
• DC clopidogrel 5 to 7 d prior to elective CABG (Class I, LOE: B)
• DC IV GP IIb/IIIa 4 h prior to CABG (Class I, LOE: B)
• Cont UFH (Class I, LOE: B); DC enoxaparin 12 to 24 h prior to CABG; DC fondaparinux 24 h prior to CABG; DC bivalirudin 3 h prior to CABG. Dose with UFH per institutional practice (Class I, LOE: B)
• Cont ASA (Class I, LOE A) • LD of clopidogrel if not given
pre angio (Class I, LOE: A) &• IV GP IIb/IIIa if not started
pre angio (Class I, LOE: A)
• DC A/C Rx after PCI for uncomplicated cases (Class I, LOE: B)
• Cont ASA (Class I, LOE: A)• LD of clopidogrel if not
given pre angio (Class I, LOE A)*• DC IV GP IIb/IIIa after
at least 12 h if started pre angio (Class I, LOE: B)
• Cont IV UFH for at least 48 h (Class I, LOE: A) or enoxaparin or fondaparinux for dur of hosp (LOE: A); either DC bivalirudin or cont at a dose of 0.25 mg/kg/hr for up to 72 h at physician‘s discretion (Class I, LOE: B)
Antiplatelet and A/C Rx
at physician’s discretion (Class I, LOE: C)
No significant obstructive
CAD on angiography
CAD on angiography
Medical therapyPCICABG
Select Post Angiography Management Strategy
Dx Angiography
Management after Diagnostic Angiography in Patients with UA/NSTEMI
Anderson JL. J Am Coll Cardiol 2007;50:e1-157. In press. Figure 9
G H
I
J
F

Long-Term Antithrombotic Therapy at Hospital Discharge after UA/NSTEMI
Medical Tx w/o Stent
Bare Metal Stent
Drug Eluting Stent
ASA 162 to 325 mg/d for at least 1 mo, then 75 to 162 mg/d
indefinitely (Class I LOE: A)
&Clopidogrel 75 mg/d for at least
1 mo and up to 1 yr (Class I LOE:B)
Add: Warfarin (INR 2.0 to 2.5) (Class IIb LOE: B)
Continue with dual antiplatelet tx as above.
Indication for Anticoagulation?
ASA 75 to 162 mg/d indefinitely (Class I LOE: A)
& Clopidogrel 75 mg/d at least 1 mo (Class I LOE: A) and up
to 1 yr (Class I LOE: B)
ASA 162 to 325 mg/d for at least 3 to 6 months, then 75
to 162 mg/d indefinitely (Class I LOE: A)
&
Clopidogrel 75 mg/d for at least 1 yr (Class I LOE: B)
Anderson JL. J Am Coll Cardiol 2007;50:e1-157. Figure 11.
UA/NSTEMI Patient
Groups at Discharge
Yes
No

Preparation for Discharge After UA/NSTEMI
• Antiplatelet Rx– ASA 75 - 162 mg/day– Clopidogrel 75 mg/day
• Beta Blocker• ACEI / ARB
– Especially if DM, HF, EF <40%, HTN
• Statin– LDL <100 mg/dL (ideally <70 mg/dL)
• Secondary Prevention Measures– Smoking Cessation– BP <140/90 mm HG or <130/80 mm HG for DM or chronic kidney disease
– HbA1C <7%– BMI 18.5-24.9– Physical Exercise 30-60 min at least 5 days/wk

Panel Discussion