
Type A Behavior, Personality Hardiness, and …contrada/Contrada (1989).pdf · Type A Behavior,...
9
Journal of Personality and Social Psychology Copyright 1989 by the American PsychologicalAssociation,Inc. 1989, Vol. 57, No. 5,895-903 0022-3514/89/$00.75 Type A Behavior, Personality Hardiness, and Cardiovascular Responses to Stress Richard J. Contrada RutgersmThe State University of New Jersey Type A behavior and hardiness were examined as predictors of cardiovascular responses to stress in 68 male undergraduates. Systolic and diastolic blood pressure (SBP and DBP) and heart rate were monitored while subjects performed a difficult mirror-tracing task. Type A assessments based on the Structured Interview, but not those based on the Jenkins Activity Survey, were associated with significantly enhanced SBP and DBP elevations. Hardiness was associated with significantly reduced DBP responsiveness. In addition, a significant interaction indicated that the Type B-high hardiness group showed the least DBP reactivity. A near-significant interaction (p = .06) suggested that Type B-high hardiness subjects also reported the least anger. Further exploration of the data indicated that the challenge component of hardiness accounted for its relationship to DBP reactivity. These results have implications both for the psychophysiologic study of Type A behavior and for under- standing the health-promoting effects of hardiness. Interest in the effects of personality on health and illness has grown considerably in recent years. One factor that has drawn attention to this topic is the extensive literature examining Type A behavior as a contributor to coronary heart disease (CHD; Houston & Snyder, 1988). Type A behavior consists of competi- tive achievement striving, hostility, impatience, and vigorous speech and motor mannerisms. Type B refers to the relative ab- sence of these characteristics and a more relaxed style of coping. Initially, epidemiological work provided rather consistent evi- dence that individuals exhibiting Type A behavior show a greater risk of developing CHD than their Type B counterparts (Cooper et al., 1981 ). However, more recent studies have failed to confirm earlier findings (Shekelle, Gale, & Norusis, 1985; Shekelle, Hulley, et al., 1985). Two recent meta-analyses have helped to clarify the status of Type A behavior as a coronary risk factor. The first (Booth- Kewley & Friedman, 1987) included both cross-sectional and prospective studies and suggested that Type A behavior is reli- ably associated with CHD. The second meta-analysis (Mat- thews, 1988) differed in that it focused exclusively on prospec- tive studies, had access to more recent findings, and used different decision rules in aggregating data across studies. Re- suits indicated that Type A behavior predicts CHD (a) when Type A is assessed using a Structured Interview (SI; Dembroski, 1978; Rosenman, 1978), but not when measured using the Jen- kins Activity Survey (JAS; Jenkins, 1978; a self-administered questionnaire) and (b) in population-based studies that exam- I thank Lee Jussim, Suzanne Ouellette Kobasa, David Krantz, and three anonymous reviewers for their critical comments on an earlier version of this article. I am also grateful to Mark Patane for his assis- tance in conducting the second session, Jean Landeau for rating Struc- tured Interview tapes, and Susan Hedges for coding verbalization data. Correspondence concerning this article should be addressed to Rich- ard J. Contrada, Department of Psychology, Tillett Hall, Rutgers Uni- versity, New Brunswick, New Jersey 08903. 895 ined initial CHD in subjects who were healthy at intake, but not in studies of high-risk individuals. As noted by Friedman and Booth-Kewley (1988), the two meta-analyses agree in supporting the hypothesis that Type A behavior is related to CHD but raise several issues regarding the nature of that relationship. Most germane to the present study are questions about the magnitude of the Type A-CHD rela- tionship. Even in population-based studies in which Type A was assessed by Structured Interview, results indicate only a modest association with CHD. The Type A variable identifies as coro- nary prone many individuals who do not develop CHD and as noncoronary prone many individuals who do. Efforts to increase predictive validity have primarily taken the approach of evaluating separately the component behaviors reflected in global Type A assessments based on the SI. This has led to the discovery that hostility and other anger-related variables may constitute the "toxic" elements of Type A behav- ior (Dembroski & Costa, 1987). Less attention has been given to the study of Type A behavior in conjunction with other per- sonality factors that may contribute to coronary risk. The Mat- thews (1988) and Booth-Kewley and Friedman (1987) meta- analyses identified several personality constructs that appear promising in this regard, given their relationships to CHD in studies in which Type A was not measured. The epidemiological literature on Type A behavior has stimu- lated a considerable amount of research examining mecha- nisms that may explain the relationship between Type A and CHD. This work is based on the hypothesis that coronary risk is enhanced by cardiovascular and other physiological responses associated with psychological stress and that these responses are more pronounced in Type A individuals. Emerging from this research are three trends that parallel epidemiological findings: (a) Psychophysiological research has more often yielded posi- tive results where Type A is assessed by SI rather than by ques- tionnaire (Contrada, Wright, & Glass, 1985); (b) reported asso- ciations account for what is, at best, only a small proportion of
Transcript of Type A Behavior, Personality Hardiness, and …contrada/Contrada (1989).pdf · Type A Behavior,...

Journal of Personality and Social Psychology Copyright 1989 by the American Psychological Association, Inc. 1989, Vol. 57, No. 5,895-903 0022-3514/89/$00.75
Type A Behavior, Personality Hardiness, and Cardiovascular Responses to Stress
Richard J. Contrada RutgersmThe State University of New Jersey
Type A behavior and hardiness were examined as predictors of cardiovascular responses to stress in 68 male undergraduates. Systolic and diastolic blood pressure (SBP and DBP) and heart rate were monitored while subjects performed a difficult mirror-tracing task. Type A assessments based on the Structured Interview, but not those based on the Jenkins Activity Survey, were associated with significantly enhanced SBP and DBP elevations. Hardiness was associated with significantly reduced DBP responsiveness. In addition, a significant interaction indicated that the Type B-high hardiness group showed the least DBP reactivity. A near-significant interaction (p = .06) suggested that Type B-high hardiness subjects also reported the least anger. Further exploration of the data indicated that the challenge component of hardiness accounted for its relationship to DBP reactivity. These results have implications both for the psychophysiologic study of Type A behavior and for under- standing the health-promoting effects of hardiness.
Interest in the effects of personality on health and illness has grown considerably in recent years. One factor that has drawn attention to this topic is the extensive literature examining Type A behavior as a contributor to coronary heart disease (CHD; Houston & Snyder, 1988). Type A behavior consists of competi- tive achievement striving, hostility, impatience, and vigorous speech and motor mannerisms. Type B refers to the relative ab- sence of these characteristics and a more relaxed style of coping. Initially, epidemiological work provided rather consistent evi- dence that individuals exhibiting Type A behavior show a greater risk of developing CHD than their Type B counterparts (Cooper et al., 1981 ). However, more recent studies have failed to confirm earlier findings (Shekelle, Gale, & Norusis, 1985; Shekelle, Hulley, et al., 1985).
Two recent meta-analyses have helped to clarify the status of Type A behavior as a coronary risk factor. The first (Booth- Kewley & Friedman, 1987) included both cross-sectional and prospective studies and suggested that Type A behavior is reli- ably associated with CHD. The second meta-analysis (Mat- thews, 1988) differed in that it focused exclusively on prospec- tive studies, had access to more recent findings, and used different decision rules in aggregating data across studies. Re- suits indicated that Type A behavior predicts CHD (a) when Type A is assessed using a Structured Interview (SI; Dembroski, 1978; Rosenman, 1978), but not when measured using the Jen- kins Activity Survey (JAS; Jenkins, 1978; a self-administered questionnaire) and (b) in population-based studies that exam-
I thank Lee Jussim, Suzanne Ouellette Kobasa, David Krantz, and three anonymous reviewers for their critical comments on an earlier version of this article. I am also grateful to Mark Patane for his assis- tance in conducting the second session, Jean Landeau for rating Struc- tured Interview tapes, and Susan Hedges for coding verbalization data.
Correspondence concerning this article should be addressed to Rich- ard J. Contrada, Department of Psychology, Tillett Hall, Rutgers Uni- versity, New Brunswick, New Jersey 08903.
895
ined initial CHD in subjects who were healthy at intake, but not in studies of high-risk individuals.
As noted by Friedman and Booth-Kewley (1988), the two meta-analyses agree in supporting the hypothesis that Type A behavior is related to CHD but raise several issues regarding the nature of that relationship. Most germane to the present study are questions about the magnitude of the Type A - C H D rela- tionship. Even in population-based studies in which Type A was assessed by Structured Interview, results indicate only a modest association with CHD. The Type A variable identifies as coro- nary prone many individuals who do not develop CHD and as noncoronary prone many individuals who do.
Efforts to increase predictive validity have primarily taken the approach of evaluating separately the component behaviors reflected in global Type A assessments based on the SI. This has led to the discovery that hostility and other anger-related variables may constitute the "toxic" elements of Type A behav- ior (Dembroski & Costa, 1987). Less attention has been given to the study of Type A behavior in conjunction with other per- sonality factors that may contribute to coronary risk. The Mat- thews (1988) and Booth-Kewley and Friedman (1987) meta- analyses identified several personality constructs that appear promising in this regard, given their relationships to CHD in studies in which Type A was not measured.
The epidemiological literature on Type A behavior has stimu- lated a considerable amount of research examining mecha- nisms that may explain the relationship between Type A and CHD. This work is based on the hypothesis that coronary risk is enhanced by cardiovascular and other physiological responses associated with psychological stress and that these responses are more pronounced in Type A individuals. Emerging from this research are three trends that parallel epidemiological findings: (a) Psychophysiological research has more often yielded posi- tive results where Type A is assessed by SI rather than by ques- tionnaire (Contrada, Wright, & Glass, 1985); (b) reported asso- ciations account for what is, at best, only a small proportion of
896 RICHARD J. CONTRADA
the variance (Houston, 1983); and (c) the association between Type A and physiologic reactivity to stress is greater when this relationship is examined separately for hostility (e.g., Dem- broski, MacDougall, Shields, Petitto, & Lushene, 1978).
Further investigation of hostility and other components of Type A may determine more precisely which aspects of the be- havior pattern are most strongly associated with physiological responses that may promote CHD. However, as in the predic- tion of CHD, it also might be useful to examine Type A behav- ior in the context of other personality characteristics, particu- larly those that themselves show a relationship to health. It is reasonable to hypothesize that personality characteristics that are conceptually distinct from Type A behavior and its compo- nents, but that also bear a relationship to physical health or illness, may account for some of the variance in disease and in disease-promoting physiological responses that is left unex- plained by Type A.
One variable worth examining in this regard is hardiness, a personality dimension that is believed to confer resistance against the effects of psychological stress (Kobasa, 1979). Har- diness is a composite consisting of internal locus of control (vs. powerlessness), commitment(vs, alienation), and challenge (vs. threat). In a series of retrospective (Kobasa, 1979, 1982; Ko- basa, Maddi, & Courington, 1981) and prospective (Kobasa, Maddi, & Kahn, 1982) studies, results were obtained that sug- gest that hardiness may exert a protective effect against reported illness.
Recent studies have raised both conceptual and methodologi- cal criticisms regarding hardiness research (e.g., Funk & Hous- ton, 1987; Hull, Van Treuren, & Virnelli, 1987). One concern is whether hardiness embodies a unitary construct, as originally proposed, or a set of three independent dimensions. Another is that hardiness appears to promote health independently of stress, rather than operating as a buffer by reducing illness pri- marily among individuals experiencing high stress levels (Co- hen & Edwards, 1989; Funk & Houston, 1987; Hull et al., 1987). These issues typically have been investigated in research oriented toward the prediction of adaptive outcomes, such as psychological distress or reports of physical illness.
Relatively little effort has been devoted to identifying mecha- nisms that may mediate the effects of hardiness on health out- comes. There is evidence to suggest that hardy individuals per- ceive stressful events as more positive and controllable than in- dividuals low in hardiness (Allred & Smith, 1989; Rhodewalt & Agustsdottir, 1984; Rhodewalt & Zone, 1989). Thus it is pos- sible that hardiness short-circuits the stress response by influ- encing the processes whereby psychological threat is appraised. However, it has yet to be demonstrated that hardy individuals show reduced physiological responsiveness when confronted by laboratory stressors.
It is the question of whether hardiness is related to physiologi- cal responses to stress that forms a basis for the present study. To the degree that hardiness protects against the development of physical disease through mechanisms associated with psy- chological stress, it may be predicted that individuals high in hardiness will show less pronounced physiological responses to a stressor than those low in hardiness. In the absence of such a finding, pathways to disease that do not necessarily involve stress, such as cigarette smoking, poor diet, and failure to detect
and/or act on physical symptoms, might be regarded as more plausible explanations for data suggesting that hardiness is health promoting. Since Type A behavior appears to be associ- ated with enhanced physiological reactivity, it would be useful to determine whether hardiness contributes to the prediction of reactivity independently of any association between hardiness and Type A. To the extent that this is the ease, it would suggest that research on the psychophysiology of Type A behavior might benefit from a consideration of hardiness and, perhaps, other personality characteristics that influence the stress response.
Accordingly, a psychophysiological experiment was con- ducted to assess the independent and conjoint effects of Type A behavior and hardiness on subjective and cardiovascular re- sponses to a frustrating psychomotor task. Previous work does not provide a specific basis for predicting an interaction be- tween Type A behavior and hardiness. Therefore, it was ex- pected that Type A behavior would be positively associated with physiological reactivity to the task, and that hardiness would be inversely associated with reactivity, such that physiological responses would be greatest among Type A subjects low in har- diness, and lowest among Type B subjects high in hardiness. It also was predicted that Type A effects based on SI assessments would be stronger than those based on the JAS.
M e t h o d
Subjects
Subjects were 68 male introductory psychology students who partici- pated in partial fulfillment of course requirements. Subjects ranged in age from 18 to 22 years (M = 21.1).
Measurement of Type A Behavior and Hardiness
The principal measure of Type A behavior was the student version of the SI, administered by the author, who was trained in the technique by Ray H. Rosenman. The interviews were tape-recorded and reviewed independently by an auditor who had been trained by Theodore M. Dembroski. Behavior pattern assessments were made using a 4-point scale (A1 = 4, A2 = 3, X = 2, and B = 1). Degree of agreement between the two raters' discrete classifications was 75%. Intercorrelation of the 4-point ratings yielded a value of.87. The 4-point ratings were averaged to construct a continuous Type A score for use in correlational and regression analyses. For descriptive purposes, a dichotomous measure of Type A behavior was derived by combining discrepant ratings, with the use of a procedure recommended by MacDougall, Dembroski, and Mustane (1979): A1/A2 and A/X = A; B/X = B (there were no A-B disagreements, nor did any subject receive a Type X classification from both raters). This yielded 35 Type As and 33 Type Bs. Subjects also completed Form T of the JAS (Krantz, Glass, & Snyder, 1974).
Hardiness was assessed through the use of five questionnaires. The Alienation From Work and Alienation From Self scales (Maddi, Ko- basa, & Hoover, 1979) were used to measure commitment. The External Locus of Control Scale (Rotter, Seeman, & Liverant, 1962) and Power- lessness Scale (Maddi et al., 1979) were used to measure control. The Security scale of the California Life Goals Evaluation Schedule (Hahn, 1966) was used to measure challenge. For each of these measures, high scores reflect a relative lack of hardiness. Following procedures de- scribed by Kobasa et al. (1982), the appropriate scale scores were stan- dardized and then summed to create measures of commitment and con- trol. Because challenge was measured by only one scale (Security), its scores were doubled before adding together the five standardized scores

TYPE A, HARDINESS, AND STRESS 897
to construct a composite hardiness measure. A median split was used to derive a dichotomous measure of hardiness on the basis of this overall index.
Measurement of Cardiovascular Responses
Measurements of systolic and diastolic blood pressure (SBP and DBP) were obtained with an Arteriosonde 1216 (Roche). The com- pressing cuff and transducer were placed over the brachial artery of the subject's nondominant arm. Heart rate (HR) was monitored as digital pulsation, with the use of a photocell plethysmograph attached to the second finger of the nondominant hand. Readings were taken during the 30-s interval beginning immediately after the compressing blood pressure cuff had deflated. A digital display indicated the number of pulses for the 30-s period, which was doubled in order to express HR in beats per minute (bpm). Physiological recording equipment was located in an observation room adjacent to the experimental chamber, where the subject could be monitored by means of closed-circuit television.
Experimental Task
The mirror-tracing task consisted of a 96 × 96 cm wooden platform in which was cut a channel measuring 1 cm wide and 1 crn deep that formed the shape of a six-pointed star. Distance from the apex of one point of the star to its opposite measured 48 era. The sides of the chan- nel were lined with conductive material wired to a 24-era stylus. Contact between the stylus and the sides of the channel completed an electric circuit powered by a 12-V direct current source. Completion of the cir- cuit activated a buzzer. Adjoining one edge of the platform at a 90* angle was a second 96 × 96 cm wooden panel, on which was mounted a 48 × 48 cm mirror. Direct visual access to the star was prevented by a third, 56 × 56 cm wooden panel that rested on 4 wooden legs at a height of 24 cm above the platform. The reflection oftbe star in the mirror could readily be observed by looking over the third panel.
Successful performance required that the subject use the stylus to trace the star, guided only by its reflection, without touching the sides of the channel. This is virtually impossible to do without considerable practice, and none oftbe subjects in this study completed a single trac- ing in the allotted 5 rain. Factors contributing to difficulty were (a) nar- rowness of the channel and (b) the fact that mirror images are reversed. The first factor makes it difficult to negotiate even the straight edges of the star without touching the sides; the second leads to problems in deciding which way to turn at the c o m m . Because these aspects of mir- ror-tracing are not immediately obvious, the task is deceptively difficult, and can be quite frustrating.
Affective Measures
Affective responses to task performance were measured using the State-Trait Personality Inventory (Spielberger, Jacobs, & Russell, 1983), which contains three 10-item subscales: Anger, Anxiety, and Curiosity. Instructions requested that the subject respond with reference to his feelings while working on the mirror-tracing task. The Anger and Anxi- ety scales were used to assess subjective distress. The Curiosity scale was included to detect positive appraisals of the task situation, such as might he expected from Type Bs or subjects high in hardiness. It contains items reflecting interest, desire to explore, and inquisitiveness.
Procedure
Subjects participated individually in two sessions. At the first session, I greeted the subject and escorted him to a small office where the pur- pose of the study was described as an attempt to determine the effects of personality on subjective and physiological correlates of psychomotor
activity. Informed consent was obtained at this point. The experimenter then administered the SI. Following the interview, the JAS and hardi- ness questionnaires were completed in an order individually random- ized for each subject. An appointment for the second session then was scheduled, and the subject was thanked and dismissed.
Session 2 was conducted by a second male experimenter who was unaware of the hypotheses under study as well as the subject's Type A assessment and hardiness scores. The subject was escorted to a sound- attenuated experimental room, where the experimenter reiterated the purposes of the study. A baseline period ensued, during which time the subject was asked to sit quietly and relax. Measurements of SBP, DBP, and HR were taken at 2-min intervals, until SBP values remained rela- tively stable (-+5 mmHg) across two successive readings, after a mini- mum of 8 min had elapsed. Means for the final two readings on each cardiovascular measure were taken as baseline values.
Following the baseline period, the experimenter reentered the experi- mental room, placed the mirror-tracing task on the table, and gave the subject a single sheet of paper containing task instructions. The experi- menter then left the room, after explaining that any further communica- tion would take place over an intercom system. Instructions described the mirror-tracing task as a measure of spatial ability and hand-eye co- ordination, and indicated that the subject was to attempt to complete at least one tracing, without activating the buzzer, within a 5-min period. It was stated that "about 50%" of the subjects participating in the project had been able to do this, and that the main concern of the investigators was that the subject give his best effort. These instructions were devel- oped on the basis of research indicating that Type As are most likely to show enhanced physiological activity in response to tasks characterized by moderate levels of difficulty (Contrada et al., 1985).
The instructions went on to request that the subject "think aloud" while working on the task. The subject was encouraged to verbalize whatever thoughts and feelings he might experience, whether or not they were related to the immediate situation. It was explained that these ver- balizations would be used to determine the information processing style used by the subject in working on the task.
When the subject was ready to proceed, the experimenter activated a tape recorder (connected to the hidden microphone serving the inter- com system from the experimental room) and then instructed the sub- ject to begin working. Blood pressure and HR measurements were initi- ated 5 s later, and every 60 s thereafter, for the next 5 min. After record- ing the final measurements, the experimenter instructed the subject to stop working, reentered the experimental room, and administered the postexperimentai questionnaire. Following completion of the question- naire, the first experimenter conducted a postexperimental interview and debriefing.
Data Reduction and Analysis
The principal mode of statistical analysis was multiple regrcssion analysis, since both predictors (Type A and hardiness) and dependent measures (cardiovascular activity and affect) reflect continuous dimen- sions. However, in order to maintain comparability with most previous research on Type A, which has taken an analysis of variance approach,
Verbalization instructions were included both to support the cover story and as a means of acquiring data reflecting subjective reactions to task performance. Verbalizations were transcribed and coded by two raters who were unaware of subjects' Type A classifications and hardi- ness scores. Coding categories included swearing, laughter, perfor- mance attributions, and expression of positive or negative affect. There were no significant effects of Type A behavior or hardiness on amount of verbalization (ps ~ .09). Analysis of verbalization content indicated few statistically reliable relationships with Type A, hardiness, or cardio- vascular reactivity; those that were obtained appeared uninterpretable.
898 RICHARD J. CONTRADA
significant regression effects were described by reporting means for groups formed on the basis of the dichotomous Type A and hardiness measures described earlier. Crossing the dichotomous Type A and har- diness classifications yielded the following numbers of subjects in each category: Type A-high hardiness, 21; Type A-low hardiness, 14; Type B-high hardiness, 13; Type B-low hardiness, 20.
As in previous research, physiological reactivity was measured as the difference between baseline and task values for each cardiovascular measure. Preliminary analysis indicated that reactivity on each of the cardiovascular measures showed no reliable changes over the five task readings, and that this pattern held, regardless ofSI, JAS, and hardiness scores (ps > .20). Therefore, a single index of reactivity was computed for each variable by averaging across the five change scores. Baseline values from which change scores were derived were included in the re- gression model in order to remove variance attributable to initial values (Wilder, 1968).
Results
Intercorrelations Among Type A and Hardiness Measures
Intercorrelations between the Type A and hardiness mea- sures are presented in Table 1. The SI and JAS showed a moder- ate degree of association (r =.38, p < .01). Relationships among the hardiness components were similarly modest in magnitude (rs ranging from .28 to .49, ps < .05). Intercorrelations between the SI and each of the hardiness components, as well as the com- posite hardiness index, were low and nonsignificant (rs ranging from - . 18 to -.06). The JAS showed a similar dissociation with hardiness (rs from - . 18 to -.02), except for a significant rela- tionship with control (r = - .28, p < .05), indicating that sub- jects scoring in the Type A direction tended to report feeling capable of influencing the events in their lives.
Table 1 also presents the internal consistencies of the Type A and hardiness measures. Reliability coefficients for all measures are acceptable, except for Challenge (Cronbach's a = .56).
Resting Cardiovascular Activity
A series of regression analyses was conducted to determine the relationships between Type A and hardiness and cardiovas- cular baselines. The only significant effect was a Type A × Har- diness interaction for resting SBP values, F(I , 64) = 4.54, p < .04. Among Type Bs, subjects high in hardiness had a lower rest-
Table 1 Internal Consistency and lntercorretations of the Hardiness and Type A Measures
Measure 1 2 3 4 5 6
1. Challenge (.56) .28* .34** .74** -.02 -.06 2. Commitment (.75) .49** .76** -.14 -.18 3. Control (.83) .78** -.28* -.11 4. Hardiness Composite (.86) -.18 -.15 5. Jenkins Activity Survey (.73) .38** 6. Structured Interview (.87)
Note. Cronbach alpha coefficients are given in parentheses, except for the Structured Interview, where the interrater correlation is presented. *p<.05. **p<.01.
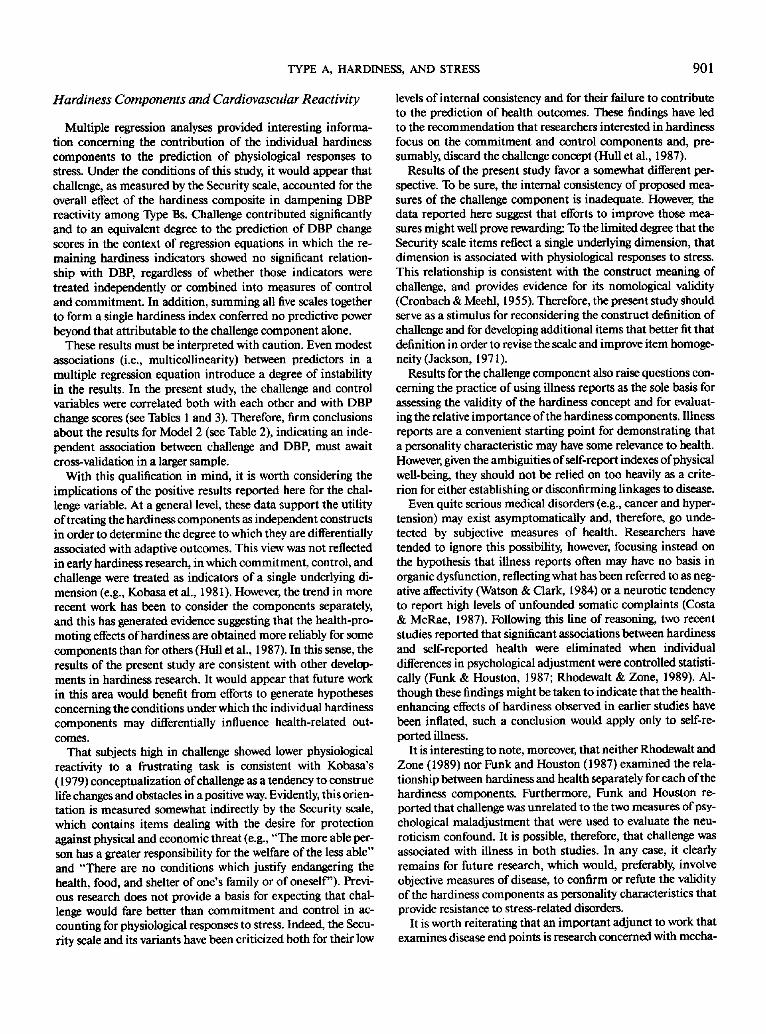
Figure 1. Diastolic blood pressure (DBP) elevations as a function of Type A and hardiness classifications.
ing SBP than those low in hardiness (Ms = 98.4 mmHg and 105.2 mmHg, respectively); by contrast, among Type As, those high in hardiness had a higher resting SBP than those low in hardiness (Ms = 109.8 mmHg and 101.7 mmHg, respectively). No other effect approached significance for any of the cardio- vascular measures (ps > . 18).
Cardiovascular Reactivity
As expected, a regression analysis for SBP change scores yielded a significant main effect for Type A, F(I, 63) = 4.97, p < .03. Type As showed significantly greater reactivity than Type Bs (Ms = 20.1 mmHg and 15.2 mmHg). Whereas subjects low in hardiness tended to have higher SBP elevations than those high in hardiness (Ms = 19.1 mmHg and 16.3 mmHg), neither the hardiness main effect nor the Type A X Hardiness interaction was significant (ps > .40). 2
Also consistent with predictions was a Type A main effect for DBP change scores, F(1, 63) = 6.54, p < .02. As in the case of SBP, Type As showed significantly greater DBP responses than their Type B counterparts (Ms = 14.5 mmHg and 10.9 mmHg, respectively). There was also a hardiness main effect, F( 1, 63) = 7.54, p < .01. As expected, DBP elevations were significantly higher among subjects with low hardiness scores compared with those high in hardiness (Ms = 14.0 mmHg and 1 l . l mmHg, respectively). The two main effects were qualified by a Type A X Hardiness interaction, F(1, 63) = 4.22, p < .05. The relevant data are depicted in Figure 1. It can be seen that the interaction reflected particularly low DBP elevations among Type B sub- jects with high hardiness scores, the group expected to be least reactive.
An analysis of HR change scores yielded only a nonsignifi-
2 It seems unlikely that the Type A × Hardiness interaction for SBP baseline contributed to the Type A main effect for SBP change scores. Type A subjects had slightly higher SBP baselines than Type Bs (Ms = 106.6 mmHg and 102.5 mmHg, respectively, ns), and SBP baselines showed a nonsignificant trend toward an inverse relationship with change scores (p = . 16). Therefore, higher SBP baselines tended to be associated with lower SBP change scores, working against the obtained Type A main effect.

TYPE A, HARDINESS, AND STRESS 899
Table 2 Three Regression Models Predicting DBP Reactivity From Type A and Hardiness
Predictor Beta weight
Model 1: Hardiness composite a
TypeA .28* Hardiness .82** Type A × Hardiness -.62*
Model 2: Three hardiness components b
Type A .31 * Challenge .76* Type A × Challenge -.70*
Model 3: Five hardiness scales c
TypeA .31"* Challenge .88** Type A × Challenge -.81"
Note. The regression models are described in the text. Only significant terms are presented in the table. Not shown are regression results for DBP baseline values, which were significant in each model. a F(4, 63) = 6.09, p < .0005, corrected R 2 = .23. b F(8, 59) = 3.71, p < .002, corrected R 2 = .24. OF(12, 55) = 2.82, p < .005, corrected R 2 = .25. *p < .05. **p <.01.
cant trend toward a Type A effect, F( I , 63) = 2.74, p = . 10. Type As showed somewhat higher HR elevations than Type Bs, which was in the expected direction (Ms = 2.3 bpm and -1 .7 bpm). Neither hardiness nor the Type A × Hardiness interaction ap- proached significance (ps > .40).
The foregoing analyses were repeated substituting JAS scores as the Type A measure. Only a significant hardiness main effect for DBP, duplicating the result reported earlier, approached sig- nificance (all other ps > . 10).
Effects o f Type A and Hardiness on Affective Measures
Regression analysis of State Anger scores yielded a reliable hardiness main effect, F( I , 63) = 4.13, p < .05, and a near- significant Type A X Hardiness interaction, F(I , 64) = 3.68, p = .06. As reflected by the marginal interaction, the hardiness main effect was carried primarily by the Anger scores of the Type B-high hardiness group (M = 14.0), which were lower than those of Type B-low hardiness subjects (M = 16.0) and the two Type A groups (both Ms = 16.9). No other effects ap- proached significance for any of the state affect scales (ps > . 10).
Correlations between Anger ratings and cardiovascular change scores only approached significance in the case of DBP (r = . 19, p = . 11). This suggests that the effects of Type A behav- ior and hardiness on anger were largely independent of the reac- tivity effects.
Hardiness Components and Cardiovascular Reactivity
In order to explore the relative contributions of the individual components of hardiness in predicting DBP reactivity, two ad- ditional multiple regression analyses were carried out. One in-
eluded the following predictors: DBP baseline values, SI Type A assessments, individual scores on the five scales that make up the hardiness composite, and product terms reflecting interac- tions between Type A ratings and each of the hardiness scales.
The second analysis differed in that the External Locus of Control and Powerlessness scales were combined into a single measure of control, and the Alienation from Self and Alienation from Work scales were combined into a single measure of com- mitment. The Security scale was included as a measure of chal- lenge and, as in the first series of regressions, product terms were constructed to reflect the interaction between Type A and each hardiness component. Thus, the two regression analyses allow a comparison of two levels of decomposition of the overall hardiness variable: One resolves hardiness into measures of its three constituent constructs, the other into five individual scale scores.
Significant effects are presented in Table 2, which also sum- marizes the initial regression analysis that used the overall har- diness index. Because the number of predictors in the models varies, each capitalizes on chance to a different degree. There- fore, the R 2 coefficients were adjusted using the shrinkage cor- rection formula described by Olkin and Pratt (1958). Inspec- tion of these data suggests a number of conclusions. First, after correction for shrinkage, the three models are shown to account for a similar, statistically significant portion of the variability in DBP responses to the task. Second, each model contains a term reflecting a hardiness effect that adds significantly t ° the predic- tion of DBP responses above and beyond the contribution of Type A behavior. Third, the relationship between hardiness and DBP responses largely reflects a single hardiness component, challenge. Whether the remaining four scales are considered in- dividually (Table 2, Model 3), combined into control and com- mitment scores (Table 2, Model 2), or summed together with challenge scores to generate a single composite index of hardi- ness (Table 2, Model 1), they add little to the ability of the chal- lenge component to predict individual differences in DBP re- sponses to the task. The only exception appeared in Model 2 in the form of a nonsignificant trend toward a main effect for the control component (p = .08).
Table 3 presents simple correlations between control, chal- lenge, and overall hardiness and DBP change scores. It can be seen that the pattern of results for challenge resembles that of the composite hardiness index. High scores (indicating low challenge) were associated with heightened DBP reactivity to the task, and this relationship is evident among Type Bs but not among Type As. Similarly, DBP reactivity tended to be greater
Table 3 Correlations Between Significant Hardiness Predictors and DBP Reactivity
Predictor Type A Type B Combined
Challenge -.06 .45*** .19 Control .13 .38** .21" Hardiness composite .11 .44** .22*
Note. N = 68 (33 Type B and 35 Type A). *p<.10. **p<.05. ***p<.01.

900 RICHARD J. CONTRADA
among subjects who reported a lack of control, and this re- lationship was also somewhat stronger among Type Bs than Type As.
DBP in Type A research might reflect qualitative variations in the tasks used to induce reactivity in those studies.
Discussion Hardiness and Cardiovascular Reactivity
The results of this study suggest the following observations regarding the role of Type A behavior and personality hardiness in accounting for physiological responses to stress. First, the data are consistent with previous studies demonstrating that Type A assessments based on the SI show a modest but reliable association with cardiovascular reactivity. Second, individual differences in reactivity that are left unexplained by SI Type A assessments are significantly related to other aspects of person- ality encompassed by the term hardiness. Third, an exploration of the relationship between hardiness and cardiovascular re- sponses to stress supports the utility of examining separately the individual characteristics that make up the hardiness com- posite. In particular, the stress-dampening effects of hardiness in the present study were largely attributable to the challenge component.
Type A Behavior and Cardiovascular Reactivity
As expected, Type A assessments based on the SI were associ- ated with enhanced SBP and DBP responses to task perfor- mance. The HR data yielded only a nonsignificant tendency toward greater reactivity among Type As (p = . 10). By contrast, the JAS was unrelated to reactivity. These results are consistent with the preponderance of previous findings demonstrating that the SI is more strongly associated with physiological reactivity than the JAS (Contrada et al., 1985). Moreover, as noted earlier, these reactivity data are congruent with epidemiological find- ings that support the validity of SI assessments in the prediction of CHD in population-based studies, but draw into question the status of the JAS as a measure of coronary-prone behavior (Matthews, 1988). In view of these observations, it would seem incumbent on the investigator who relies on the JAS as a mea- sure of Type A behavior to justify its use on some basis other than its relevance to CHD.
That Type A effects were obtained for SBP also accords with earlier studies in that positive results have been observed more consistently for SBP than for any other cardiovascular parame- ter. However, the fact that a significant Type A effect was ob- tained for DBP but not for HR is somewhat surprising, because HR effects have been obtained more frequently than DBP effects in previous research. Both the absence of a significant Type A-B effect for HR and the overall low level of HR reactiv- ity (M = 1.0 bpm) may be consequences of a cognitive require- ment of mirror-tracing (close attention to sensory inputs), which has been associated with reduced cardiac rate (Williams, 1986). This same factor may account for the positive DBP effects, because sensory intake also appears to produce vaso- constriction in skeletal muscles, which would tend to increase peripheral resistance, and could raise DBP (Williams, 1986). Whatever the explanation, mirror-tracing does seem to elicit pronounced DBP elevations, as seen in the present study as well as in a recent investigation by Kasprowicz, Manuck, and Krantz (1988). This suggests that inconsistencies in findings for
Analyses using the composite hardiness index indicated that DBP responsiveness was significantly lower among subjects with high hardiness scores than among those low in hardiness. The main effects of Type A and hardiness on DBP responses were qualified by a significant interaction indicating that the combination of a Type B behavior classification and high hardi- ness scores was associated with lowest DBP reactivity. Although an interaction was not specifically predicted, it was expected that Type B subjects high in hardiness would show the lowest levels of cardiovascular response.
These data provide initial support for the notion, implicit in the hardiness construct, that the hardy individual possesses some attribute that dampens the body's response to psychologi- cal stress. This conclusion should be viewed guardedly, because two recent studies unexpectedly found hardiness to be associ- ated with enhanced cardiovascular responsiveness to psycholog- ical stress (Allred & Smith, 1989; Van Treuren & Hull, 1987). Note, however, that these unanticipated findings involved SBP and HR, not DBP. Moreover, AUred and Smith reported a mar- ginally significant trend toward reduced finger pulse volume in hardy subjects during anticipation of the experimental task. Re- ductions in finger pulse volume, like the DBP elevations re- ported here, reflect the constriction of blood vessels resulting from increased sympathetic nervous system activity. Thus, it may tentatively be concluded that hardiness is associated with lower levels of a physiologic response pattern that was elicited by some feature of the mirror-tracing task used in the present study and, perhaps, during the anticipation phase of the Allred and Smith study.
The fact that hardiness exerted a greater modulating effect on the stress response among Type B as compared with Type A individuals deserves comment. Although it would be of theoret- ical interest if Type As were less likely than Type Bs to benefit from the health-promoting effects of hardiness, clearly it would be premature to conclude this on the basis of the present investi- gation. Indeed, in another study relevant to this issue, Kobasa, Maddi, and Zola (1983) reported data suggesting that hardiness may exert a greater health-protective effect among Type As, rather than among Type Bs. However, the interaction term re- flecting that effect fell short of statistical significance. In addi- tion, Kobasa et al. (1983) measured Type A behavior using the JAS, whereas the DBP results reported here were based on SI assessments. It is generally recognized that the SI and the JAS measure substantially different aspects of the Type A behavior pattern. Behavioral classifications derived from the SI are based mainly on manifest hostility and the use of vigorous speech and motor mannerisms, whereas the JAS is largely a self-report measure of a pressured drive to succeed (Matthews, Krantz, Dembroski, & MacDougall, 1982). It remains for future re- search to determine how the specific Type A behaviors reflected in SI and JAS assessments may interact with hardiness in deter- mining health outcomes.
TYPE A, HARDINESS, AND STRESS 901
Hardiness Components and Cardiovascular Reactivity
Multiple regression analyses provided interesting informa- tion concerning the contribution of the individual hardiness components to the prediction of physiological responses to stress. Under the conditions of this study, it would appear that challenge, as measured by the Security scale, accounted for the overall effect of the hardiness composite in dampening DBP reactivity among Type Bs. Challenge contributed significantly and to an equivalent degree to the prediction of DBP change scores in the context of regression equations in which the re- maining hardiness indicators showed no significant relation- ship with DBP, regardless of whether those indicators were treated independently or combined into measures of control and commitment. In addition, summing all five scales together to form a single hardiness index conferred no predictive power beyond that attributable to the challenge component alone.
These results must be interpreted with caution. Even modest associations (i.e., multicollinearity) between predictors in a multiple regression equation introduce a degree of instability in the results. In the present study, the challenge and control variables were correlated both with each other and with DBP change scores (see Tables 1 and 3). Therefore, firm conclusions about the results for Model 2 (see Table 2), indicating an inde- pendent association between challenge and DBP, must await cross-validation in a larger sample.
With this qualification in mind, it is worth considering the implications of the positive results reported here for the chal- lenge variable. At a general level, these data support the utility of treating the hardiness components as independent constructs in order to determine the degree to which they are differentially associated with adaptive outcomes. This view was not reflected in early hardiness research, in which commitment, control, and challenge were treated as indicators of a single underlying di- mension (e.g., Kobasa et al., 198 I). However, the trend in more recent work has been to consider the components separately, and this has generated evidence suggesting that the health-pro- moting effects of hardiness are obtained more reliably for some components than for others (Hull et al., 1987). In this sense, the results of the present study are consistent with other develop- ments in hardiness research. It would appear that future work in this area would benefit from efforts to generate hypotheses concerning the conditions under which the individual hardiness components may differentially influence health-related out- comes.
That subjects high in challenge showed lower physiological reactivity to a frustrating task is consistent with Kobasa's (1979) conceptualization of challenge as a tendency to construe life changes and obstacles in a positive way. Evidently, this orien- tation is measured somewhat indirectly by the Security scale, which contains items dealing with the desire for protection against physical and economic threat (e.g., "The more able per- son has a greater responsibility for the welfare of the less able" and "There are no conditions which justify endangering the health, food, and shelter of one's family or of oneself"). Previ- ous research does not provide a basis for expecting that chal- lenge would fare better than commitment and control in ac- counting for physiological responses to stress. Indeed, the Secu- rity scale and its variants have been criticized both for their low
levels of internal consistency and for their failure to contribute to the prediction of health outcomes. These findings have led to the recommendation that researchers interested in hardiness focus on the commitment and control components and, pre- sumably, discard the challenge concept (Hull et al., 1987).
Results of the present study favor a somewhat different per- spective. To be sure, the internal consistency of proposed mica- sures of the challenge component is inadequate. However, the data reported here suggest that efforts to improve those mea- sures might well prove rewarding: To the limited degree that the Security scale items reflect a single underlying dimension, that dimension is associated with physiological responses to stress. This relationship is consistent with the construct meaning of challenge, and provides evidence for its nomological validity (Cronbach & Meehl, 1955). Therefore, the present study should serve as a stimulus for reconsidering the construct definition of challenge and for developing additional items that better fit that definition in order to revise the scale and improve item homoge- neity (Jackson, 1971 ).
Results for the challenge component also raise questions con- cerning the practice of using illness reports as the sole basis for assessing the validity of the hardiness concept and for evaluat- ing the relative importance of the hardiness components. Illness reports are a convenient starting point for demonstrating that a personality characteristic may have some relevance to health. However, given the ambiguities of self-report indexes of physical well-being, they should not be relied on too heavily as a crite- rion for either establishing or disconfirming linkages to disease.
Even quite serious medical disorders (e.g., cancer and hyper- tension) may exist asymptomatically and, therefore, go unde- tected by subjective measures of health. Researchers have tended to ignore this possibility, however, focusing instead on the hypothesis that illness reports often may have no basis in organic dysfunction, reflecting what has been referred to as neg- ative affectivity (Watson & Clark, 1984) or a neurotic tendency to report high levels of unfounded somatic complaints (Costa & McRae, 1987). Following this line of reasoning, two recent studies reported that significant associations between hardiness and self-reported health were eliminated when individual differences in psychological adjustment were controlled statisti- cally (Funk & Houston, 1987; Rhodewalt & Zone, 1989). Al- though these findings might be taken to indicate that the health- enhancing effects of hardiness observed in earlier studies have been inflated, such a conclusion would apply only to self-re- ported illness.
It is interesting to note, moreover, that neither Rhodewalt and Zone (1989) nor Funk and Houston (1987) examined the rela- tionship between hardiness and health separately for each of the hardiness components. Furthermore, Funk and Houston re- ported that challenge was unrelated to the two measures of psy- chological maladjustment that were used to evaluate the neu- roticism confound. It is possible, therefore, that challenge was associated with illness in both studies. In any case, it clearly remains for future research, which would, preferably, involve objective measures of disease, to confirm or refute the validity of the hardiness components as personality characteristics that provide resistance to stress-related disorders.
It is worth reiterating that an important adjunct to work that examines disease end points is research concerned with mecha-

902 RICHARD J. CONTRADA
nisms that may culminate in illness, such as physiological re- sponses to stress. Note that stress-response dampening repre- sents only one process whereby hardiness may promote health. For example, there is evidence that hardy individuals engage in health-promoting practices, such as proper diet and personal hygiene (Wiebe & McCal lum, 1986), and may be less likely to report physical discomfort (Van Treuren & Hull, 1987). Further examinat ion of factors such as physiological reactivity, health- promoting behaviors, and reactions to symptoms may lead to a better understanding of the relationship between hardiness and physical well-being.
C o n c l u s i o n
This study demonstrates that weak associations between Type A behavior and physiological reactivity may, in part, re- flect a failure to assess other sources of variation in reactivity. Specifically, although individual differences in reactivity are likely to reflect constitutional and environmental influences (Krantz & Manuck, 1984), the present data support the hypoth- esis that personality hardiness contributes to this variation as well. This finding has implications for understanding the health- promoting effects of hardiness, because the sympathetic ner- vous system activity underlying heightened DBP responses might reflect processes involved in the development of physical disorders. Results of the present study also support the utility of a more multivariate approach in research concerned with the relationship between personality and health.
Re fe rences
Allred, K. D., & Smith, T. W. (1989). The hardy personality: Cognitive and physiological responses to evaluative threat. Journal of Personal- ity and Social Psychology, 56, 257-266.
Booth-Kewley, S., & Friedman, H. S. (1987). Psychological predictors of heart disease: A quantitative review. Psychological Bulletin, 101, 343-362.
Cohen, S., & Edwards, J. R. (1989). Personality characteristics as mod- erators of the relationship between stress and disorder. In R. W. J. Neufeld (Ed.), Advances in the investigation of psychological stress (pp. 235-283). New York: Wiley.
Contrada, R. J., Wright, R. A., & Glass, D. C. (1985). Psychophysiologic correlates of Type A behavior: Comments on Houston (1983) and Holmes (1983). Journal of Research in Personality, 19, 12-30.
Cooper, T., Detre, T., Weiss, S. M., Bristow, J. D., Carleton, R., Dustan, H. E, Eliot, R. S., Feinleib, M., Jesse, M. J., Klocke, E J., Schwartz, G. E., Shields, J. L., & Stallones, R. A. ( 1981 ). Coronary prone behav- ior and coronary heart disease: A critical review. Circulation, 63, 1199-1215.
Costa, P. T., & McCrae, R. R. (1987). Hypochondriasis, neuroticism, and aging: When are somatic complaints unfounded? American Psy- chologist, 40, 19-28.
Cronbach, L. J., & Meehl, E E. (1955). Construct validity in psychologi- cal tests. Psychological Bulletin, 52, 281-302.
Dembroski, T. M. (1978). Reliability and validity of methods used to assess coronary-prone behavior. In T. M. Dembroski, S. M. Weiss, J. L. Shields, S. G. Haynes, & M. Feinleib (Eds.), Coronary-prone behavior (pp. 95-106). New York: Springer-Verlag.
Dembroski, T. M., & Costa, E (1987). Coronary prone behavior: Com- ponents of the Type A pattern and hostility. Journal of Personality, 55, 211-235.
Dembroski, T. M., MacDougall, J. M., Shields, J. L., Petitto, J., & Lus-
hene, R. (1978). Components of the Type A coronary-prone behavior pattern and cardiovascular responses to psychomotor challenge. Jour- nal of Behavioral Medicine, 1, 159-176.
Friedman, H. S., & Booth-Kewley~ S. (1988). Validity of the Type A construct: A reprise. Psychological Bulletin, 104, 381-384.
Funk, S. C., & Houston, B. K. (1987). A critical analysis of the Hardi- ness Scale's validity and utility. Journal of Personality and Social Psy- chology, 53, 572-578.
Hahn, M. E. (1966). California life goals evaluation schedule. Palo Alto, CA: Western Psychological Services.
Houston, B. K. (1983). Psychophysiological responsivity and the Type A behavior pattern. Journal of Research in Personality, 17, 22-39.
Houston, B. K., & Snyder, C. R. (1988). TypeA behaviorpattern: Re- search, theo~ and practice. New York: Wiley.
Hull, J. G., Van Treuren, R. R., & VirneUi, S. (1987). Hardiness and health: A critique and alternative approach. Journal of Personality and Social Psychology, 53, 518-530.
Jackson, D. N. (1971). The dynamics of structured personality tests: 1971. Psychological Review, 78, 229-248.
Jenkins, C. D. (1978). A comparative review of the interview and ques- tionnaire methods in the assessment of the coronary-prone behavior pattern. In T. M. Dembroski, S. M. Weiss, J. L. Shields, S. G. Haynes, & M. Feinleib (Eds.), Coronary-prone behavior (pp. 71-88). New York: Springer-Vedag.
Kasprowicz, A. L., Manuck, S. B., & Krantz, D. S. (1988). Reproduc- ibility of individual differences in cardiovascular response to behav- ioral and physical challenge. Psychophysiology, 25, 46 I. (From Ab- stracts of papers presented at the Twenty-Eighth Annual Meeting of the Society for Psychophysiological Research, 1988)
Kobasa, S. C. (1979). Stressful life events, personality, and health: An inquiry into hardiness. Journal of Personality and Social Psychology, 37, l - l I.
Kobasa, S. C. (1982). Commitment and coping in stress-resistance among lawyers. Journal of Personality and Social Psychology, 42, 707-717.
Kobasa, S. C., Maddi, S. R., & Courington, S. (1981). Personality and constitution as mediators in the stress-illness relationship. Journal of Health and Social Behavior, 22, 368-378.
Kobasa, S. C., Maddi, S. R., & Kahn, S. (1982). Hardiness and health: A prospective study. Journal of Personality and Social Psychology,, 42, 168-177.
Kobasa, S. C., Maddi, S. R., & Zola, M. A. (1983). Type A and hardi- ness. Journal of Behavioral Medicine, 6, 41-51.
Krantz, D. S., Glass, D. C., & Snyder, M. L. (1974). Helplessness, stress level, and the coronary-prone behavior pattern. Journal of Experi- mental Social Psychology, 10, 284-300.
Krantz, D. S., & Manuck, S. B. (1984). Acute psychophysiologic reactiv- ity and risk of cardiovascular disease: A review and methodological critique. Psychological Bulletin, 96, 435--464.
MacDougall, J. M., Dembroski, T. M., & Musante, L. (1979). The structured interview and questionnaire methods of assessing coro- nary-prone behavior in male and female college students. Journal of Behavioral Medicine, 2, 71-83.
Maddi, S. R., Kobasa, S. C., & Hoover, M. (1979). An alienation test. Journal of Humanistic Psychology, 19, 73-76.
Matthews, K. A. (1988). Coronary heart disease and Type A behaviors: Update on and alternative to the Booth-Kewley and Friedman (1987) quantitative review. Psychological Bulletin, 104, 373-380.
Matthews, K. A., Krantz, D. S., Dembroski, T. M., & MacDougall, J. M. (1982). Unique and common variance in Structured Interview and Jenkins Activity Survey measures of the Type A behavior pattern. Journal of Personality and Social Psychology, 42, 303-3 ! 3.
Olkin, J., & Pratt, J. W. (1958). Unbiased estimation of certain correla- tion coefficients. Annals of Mathematical Statistics, 29, 201-211.
TYPE A, HARDINESS, AND STRESS 903
Rhodewalt, F., & Agustsdottir, S. (1984). On the relationship of hardi- ness to the Type A behavior pattern: Perception.of life events versus coping with life events. Journal of Research in Personality, 18, 212- 223.
Rhodewalt, E, & Zone, J. B. (1989). Appraisal of life change, depres- sion, and illness in hardy and nonhardy women. Journal of Personal- ity and Social Psychology, 56, 81-88.
Rosenman, R. H. (1978) The interview method of assessment of the coronary-prone behavior pattern. In T. M. Dembroski, S. M. Weiss, J. L. Shields, S. G. Haynes, & M. Feinleib (Eds.), Coronary-prone behavior (pp. 55-69). New York: Springer-Verlag.
Rotter, J. B., Seeman, M., & Liverant, S. (1962). Internal vs. external locus of control of reinforcement: A major variable in behavior study. In N. E Washburne (Ed.), Decisions, values, and groups (pp. 473- 516). London: Pergamon.
Shekelle, R. B., Gale, M., & Norusis, M. (1985). Type A score (Jenkins Activity Survey) and risk of recurrent coronary heart disease in the Aspirin Myocardial Infarction Study. American Journal of Cardiol- ogy, 56, 221-225.
Shekelle, R. B., Huiley, S. B., Neaton, J. D., Billings, J. H., Borhani, N. O., Gerace, T. A., Jacobs, D. R., Lasser, N. L., Mittlemark, M. B., & Stamler, J. (1985). The MRFIT behavior pattern study: II. Type A behavior pattern and incidence of coronary heart disease. American Journal of Epidemiology, 122, 559-570.
Spielberger, C. D., Jacobs, G., & Russell, S. (1983). Assessment of anger: The State-Trait Anger Scale. In J. N. Butcher & C. D. Spielberger (Eds.), Advances in personality assessment (Vol. 2). I-Iillsdale, N J: Erl- baum.
Van Treuren, R. R., & Hull, J. G. (1987, Aa~gust). Hardiness and the perception of symptoms. Paper presented at the 95th Annual Conven- tion of the American Psychological Association, New York.
Watson, D., & Clark, L. A. (1984). Negative affectivity: The disposition to experience aversive emotional states. Psychological Bulletin, 96, 465--490.
Wiebe, D. J., & McCallum, D. M. (1986). Health practices and hardi- ness as mediators in the stress-illness relationship. Health Psychology,, 5, 425--438.
Wilder, J. E (1968). Stimulus and response: The law of initial values. Baltimore, MD: Williams & Wilkens.
Williams, R. B. (1986). Patterns of reactivity and stress. In K. A. Mat- thews, S. M. Weiss, T. Detre, T. M. Dembroski, B. Falkner, S. B. Ma- nuck, & R. B. Williams (Eds.), Handbook of stress, reactivity, and cardiovascular disease (pp. 109-125). New York: Wiley.
Received November 30, 1988 Revision received March 17, 1989
Accepted May 9, 1989 •
Members of Underrepresented Groups: Reviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals, the APA Publications and Communications Board would like to invite your participation. Manuscript reviewers are vital to the publication process. As a reviewer, you would gain valuable experience in publishing. The P&C Board is particularly interested in encouraging members of underrepresented groups to participate more in this process.
If you are interested in reviewing manuscripts, please write to Leslie Cameron at the address below. Please note the following important points:
To be selected as a reviewer, you must have published articles in peer-reviewed journals. The experience of publication provides a reviewer with the basis for preparing a thorough, objec- tive evaluative review.
To select the appropriate reviewers for each manuscript, the editor needs detailed informa- tion. Please include with your letter your vita. In your letter, please identify which APA jour- nal you are interested in and describe your area of expertise. Be as specific as possible. For example, "social psychology" is not sufficient--you would need to specify "social cognition" or "attitude change" as well.
• Reviewing a manuscript takes time. If you are selected to review a manuscript, be prepared to invest the necessary time to evaluate the manuscript thoroughly.
Write to Leslie Cameron, Journals Office, APA, 1400 N. Uhle Street, Arlington, Virginia 22201.













![EstimatingClimateTrends:Applicationto ...bering of hardiness zones, were published as early as 1938 by Harvard University’s Arnold Arboretum [3]. The most recent USDA hardiness zone](https://static.fdocuments.us/doc/165x107/5f477ccb9e94114fe7241d94/estimatingclimatetrendsapplicationto-bering-of-hardiness-zones-were-published.jpg)




