TYPE 2 DIABETES · Presentation • Insidious onset (asymptomatic many yrs) • generally not...
34
TYPE 2 DIABETES
Transcript of TYPE 2 DIABETES · Presentation • Insidious onset (asymptomatic many yrs) • generally not...
TYPE 2 DIABETES
Diagnosis
• ADA criteria 1997
Random plasma glucose >11.1mmol/l with symptoms
orFasting plasma glucose(FPG) >7.0 mmoll-1
or2 hour plasma glucose (OGTT) >11.1 mmoll-1
each must be confirmed on a subsequent day

Diabetes: WHO
• Diabetes Mellitus-FPG or 2HPG or both
• Impaired glucose tolerance-FPG and 2HPG
• Impaired fasting glucose-FPG <7 mmoll-1 and 2HPG < 7.8 mmoll-1

Pathophysiology
• Insulin resistance and relative insulin deficiency/ defective secretion
• Not immune mediated• No evidence of β cell destruction• Increased risk with age, obesity and ↓
physical activity• Strong genetic predisposition

Adapted from 2. Buse JB et al. In Williams Textbook of Endocrinology. 10th ed. Philadelphia, Saunders, 2003:1427–1483; 3. Buchanan TA Clin Ther 2003;25(suppl B):B32–B46; 4. Powers AC. In: Harrison’s Principles of Internal Medicine. 16th ed. New York: McGraw-Hill, 2005:2152–2180; 5. Rhodes CJ Science 2005;307:380–384.
The pathophysiology of type 2 diabetes
HyperglycaemiaLiver
Insulin deficiency
Excess glucose output Insulin resistance (decreased glucose
uptake))
Pancreas
Muscle and fat
Excess glucagon
Islet
Diminishedinsulin
Diminishedinsulin
Alpha cellproduces excess glucagon
Beta cellproduces less insulin

Presentation
• Insidious onset (asymptomatic many yrs)• generally not ketosis• Tendency to be obese• Macrovascular/microvascular complications
at presentation• Not insulin dependent but may be insulin
requiring

Specific types of diabetes
• Genetic defects of β cell insulin secretory defects (MODY genes), mitochondrial DNA (MELAS)
• Diseases of exocrine pancreaspancreatitis, cancer, haemachromatosis, cystic fibrosis
• Endocrinopathiescushings, acromegaly, phaeochromocytoma

Current Treatment Type 2 Diabetes
Diet, Lifestyle change and Metformin
Sulphonlyurea
Poglitazone
Metformin Intolerant
Or
HbA1C ≥ 7 %
Add
On Triple Therapy
Insulin Regimens
New Therapy
New Therapy
Development of Oral Therapies
• Sulphonlyurea The hypoglycemic action of sulphamides was discovered in 1945
• Metformin was first described in the scientific literature in 1957
• Thiazolidinedione sometimes referred to as 'glitazones' were introduced in 1997
Insulin 1922
Problems With Existing Therapies
• Sulphonlyurea Therapy
• Glitazone Therapy
• Insulin combinations
• Weight gain 2.6kg (UKPDS 1998)
• Weight gain 4.5 kg (obesity review 2007)
• 43 % ↑ Myocardial Infarction (NEJM 2007)
• Weight Gain 4 kg (UKPDS 1998)
Why Treat Diabetes
• Hyperglycaemia at diagnosis type 2 diabetes associated with increase risk of CVD (UKPDS, 1999)
• Hyperglycaemia after a glucose load shown to be associated with CVD (Whitehall, 1980, Honolulu, 1987)
• HbA1C associated with increase risk death from macrovascular disease (Finland, 1997,Germany, 1996)
• No threshold effect demonstrated
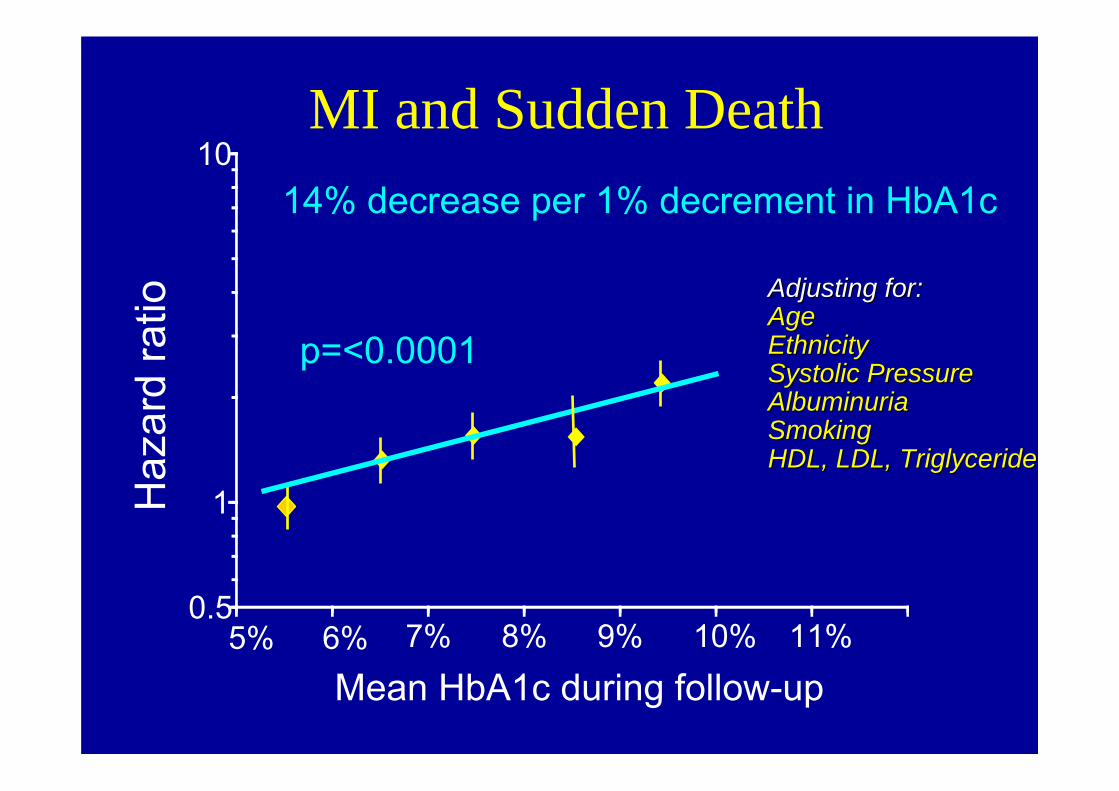
MI and Sudden Death
Mean HbA1c during follow-up
Haz
ard
ratio
14% decrease per 1% decrement in HbA1c
p=<0.0001
0.5
1
10
5% 6% 7% 8% 9% 10% 11%
Adjusting for:Adjusting for:AgeAgeEthnicityEthnicitySystolic PressureSystolic PressureAlbuminuriaAlbuminuriaSmokingSmokingHDL, LDL, TriglycerideHDL, LDL, Triglyceride

0
1
2
3
4
5
6
5 6 7 8 9 10Mean HbA1c(%) during follow-up
Microvascular Disease
Myocardial infarctionIncidence% per year
MI and Microvascular disease by HbA1c
UKPDSUKPDS
Adjusted to age,sex, ethnicity
n = 4585
UKPDS 35.BMJ 2000;321: 405-12

All Cause Mortality
0.5
1
4
5 6 7 8 9 10 11
Updated mean HbA1c (%)
14% decrement per 1% difference in HbA1c
p<0.0001HazardHazardratioratio

Treatment of Type 2 Diabetes
• First line– Diet and lifestyle changes and Metformin
• Second line– Sulphonlyura– Gliptins– Glitazone
• Third line– Add on any of above– Basal Insulin– BD Insulin

Metformin
• First line drug in all patients regardless of weight• Mechanism of action is reduction in hepatic
glucose output and increased insulin sensitivity• Not associated with hypoglycaemia• Start small dose (500mg) and titrate upwards
– With or after food to reduce side effects– Slow release metformin
• Sulphonlyurea, Glitazone, Gliptins and Insulin can be added to metformin therapy
• Renal failure

Sulphonlyurea Therapy
• Add on to Metformin• Lowers blood glucose by stimulating insulin
release• Can induce hypoglycaemia• Timing of dose not crucial but consider 30
min before breakfast (↓ plasma levels)• Role of sulphonlyureas in management is
changing

Glitazone Therapy
• New class of drug• Decreases glucose output by liver and
decreases peripheral insulin resistance• Two licensed at present which is restricted
– Rosiglitazine– Pioglitazone
• Time to effect ≈ 8 weeks• Contraindicated in liver disease and CCF
Rosiglitazone vs Pioglitazone
• Recent evidence rosiglitazone is associated with significant increase risk of MI and death from cardiovascular causes
• No such effect with Pioglitazone• Pioglitazone lower risk of deaths from MI,
stroke• Position statement risk vs benefits

Insulin Secretagogues
• Post prandial glucose regulators• Second line drugs• Rapid onset of action and short duration• Avoidance of hypoglycaemia• Nateglinide or Repaglinide

α Glucosidase Inhibitors
• Inhibit glucose absorption in small bowel• Effective in control of post prandial
hypoglycaemia• Cause GI upset
Incretin Effect (GLP-1 Pathway)
• described initially in 1964 it refers to the amplification of the insulin response to an oral glucose load
• The effect is mediated by two intestinally secreted hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) which act on specific receptors of the ß cells to produce insulin

GLP-1 effects in humans
Adapted from 1Nauck MA, et al. Diabetologia 1993;36:741–744; 2Larsson H, et al. Acta Physiol Scand 1997;160:413–422; 3Nauck MA, et al. Diabetologia 1996;39:1546–1553; 4Flint A, et al. J Clin Invest 1998;101:515–520; 5Zander et al. Lancet 2002;359:824–830.
GLP-1 secreted upon the ingestion of food
1.β-cell:enhances glucose-dependent
insulin secretion in the pancreas1
3.Liver:reduces hepatic glucose
output2
2.α-cell:suppresses postprandial
glucagon secretion1
4.Stomach:slows the rate of
gastric emptying3
5.Brain:promotes satiety and
reduces appetite4,5

Incretin Effect in Type 2 Diabetes
• The incretin effect is diminished in patients with type 2 diabetes
• GIP secretion is normal, but its action is diminished
• GLP-1 secretion is diminished, but its action is preserved
• Glucagon secreted from pancreatic α-cells is also elevated in type 2 diabetes (GLP-1 suppresses glucagon secretion from pancreatic α-cells in a glucose-dependent manner, suppressing hepatic glucose output)

Incretins and glycaemic control
Adapted from 7. Drucker DJ. Cell Metab. 2006;3:153–165. 8. Miller S, St Onge EL. Ann Pharmacother 2006;40:1336-1343.
Active GLP-1 and GIP
Release of incretin gut hormones
Pancreas
Bloodglucose control
GI tract
Glucagon from alpha cells
(GLP-1)Glucose dependent
Alpha cells
Increased insulin and decreasedglucagon reduce hepatic glucose output
Glucose dependentInsulin
from beta cells(GLP-1 and GIP)
Beta cells
Insulinincreases peripheral glucose uptake
Ingestion of food
DPP-4enzyme rapidly
degrades incretins

Gila Monster
The Gila monster is a venomous Lizard native to US and Mexico. Anadult Gila monster can consume its entire yearly energy budget in three or four mealsExendin-4 was discovered by serendipity in the salivary glands of the Gila monsterThe lizard hormone has 53% homology with human GLP-1

Therapeutic Agents using the GLP-I Pathway
• GLP-1 receptor agonists– Exenatide (naturally occurring but bioengineered)
– Liraglutide (GLP-1 analogue)
• DPP-IV Inhibitors– Sitagliptin – Vidagliptin– Saxagliptin

GLP-1• BYETTA® was authorised by the European Medicines
Evaluation Agency (EMEA) in November 2006• BYETTA® is indicated for the treatment of type 2 diabetes
mellitus in combination with metformin, and/or sulphonylureain patients who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies
Exenatide Summary of Product Characteristics 2006Fixed dose, pre-filled pens
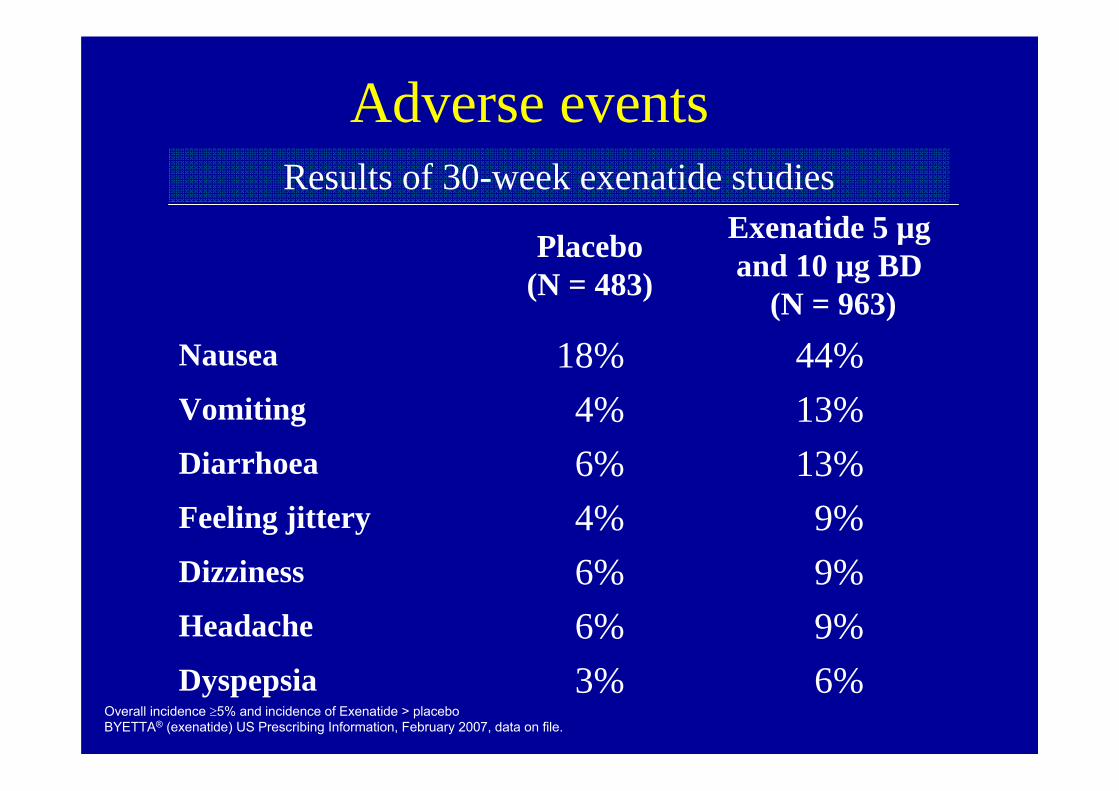
Overall incidence ≥5% and incidence of Exenatide > placeboBYETTA® (exenatide) US Prescribing Information, February 2007, data on file.
Results of 30-week exenatide studies
Placebo (N = 483)
Exenatide 5 µg and 10 µg BD
(N = 963)Nausea 18% 44%Vomiting 4% 13%Diarrhoea 6% 13%Feeling jittery 4% 9%Dizziness 6% 9%Headache 6% 9%Dyspepsia 3% 6%
Adverse events
Sitagliptin (DPP-4 inhibitor)• Sitagliptin is an orally administered DPP-4
inhibitor
• Improvement in glycaemic control is mediated by increasing the levels of active incretin hormones (GLP-1, GIP) leading to
• Decreased glucagon
• Increased insulin
• Sitagliptin improves glycaemic control as monotherapy or add on therapy to metformin or pioglitazone
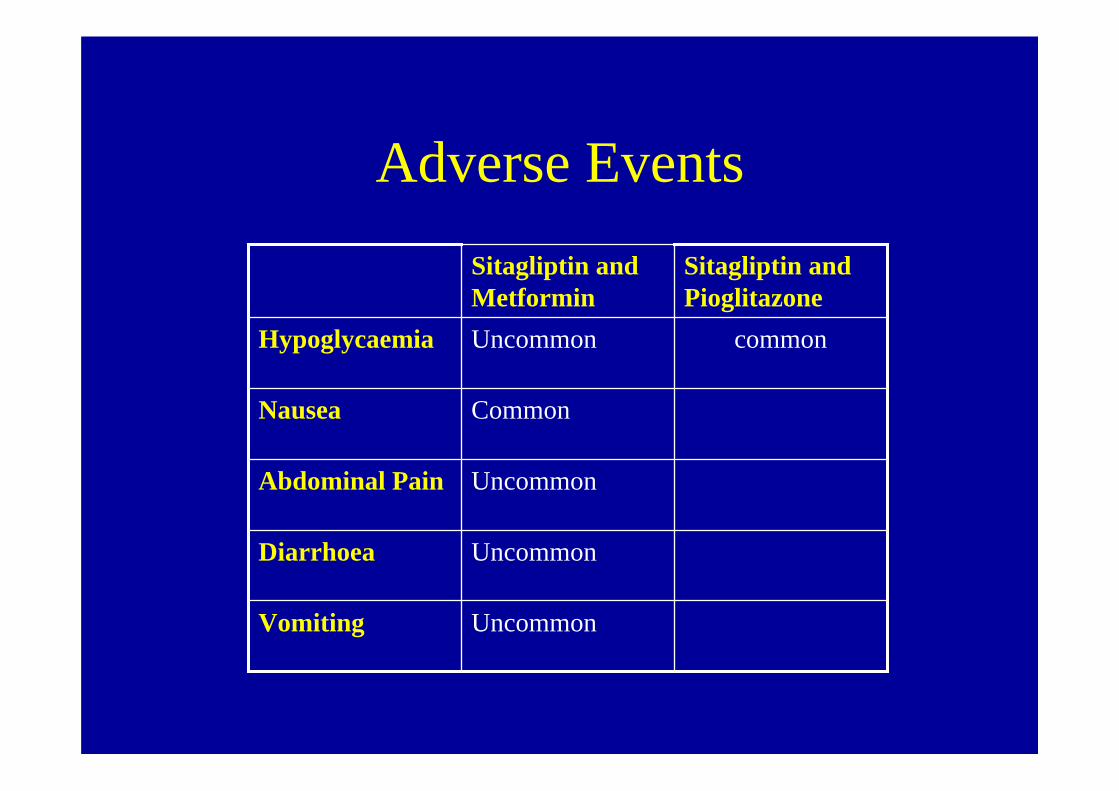
Adverse Events
UncommonVomiting
UncommonDiarrhoea
UncommonAbdominal Pain
CommonNausea
commonUncommonHypoglycaemia
Sitagliptin and Pioglitazone
Sitagliptin and Metformin
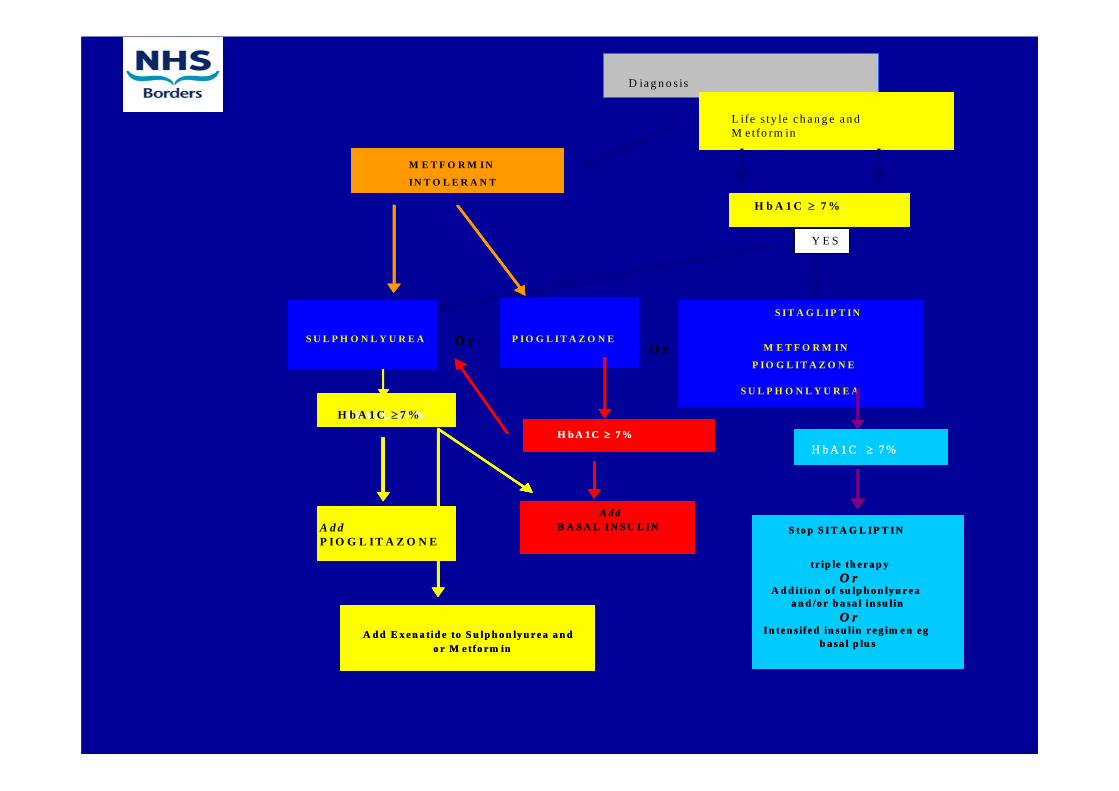
D I A G N O S I S
A n d / O r
L I F E S T Y L E I N T E R V E N T I O N
A N D
M E T F O R M I N
c o n s id e r
A d d to
o r
O r
Y E S
A d dP IO G L IT A Z O N E
A d dP IO G L IT A Z O N E
O rS U L P H O N L Y U R E A P I O G L I T A Z O N E
S I T A G L I P T I N
M E T F O R M IN
P IO G L IT A Z O N E
S U L P H O N L Y U R E A
M E T F O R M IN
IN T O L E R A N T
H b A 1 C ≥ 7 %
O rO rS U L P H O N L Y U R E A P I O G L I T A Z O N E
S I T A G L I P T I N
M E T F O R M IN
P IO G L IT A Z O N E
S U L P H O N L Y U R E A
M E T F O R M IN
IN T O L E R A N T
H b A 1 C ≥ 7 %
O r
A d dB A S A L I N S U L I N
H b A 1 C ≥ 7 %
S to p S I T A G L IP T I N
tr ip le th e r a p yO r
A d d it io n o f s u lp h o n ly u r e a a n d /o r b a s a l in s u l in
O rIn te n s ife d in su l in r e g im e n e g
b a sa l p lu sA d d E x e n a t id e to S u lp h o n ly u r e a a n d
o r M e tfo rm in
H b A 1 C ≥ 7 %
H b A 1 C ≥ 7 %
A d dB A S A L I N S U L I N
A d dB A S A L I N S U L I N
H b A 1 C ≥ 7 %H b A 1 C ≥ 7 %
S to p S I T A G L IP T I N
tr ip le th e r a p yO r
A d d it io n o f s u lp h o n ly u r e a a n d /o r b a s a l in s u l in
O rIn te n s ife d in su l in r e g im e n e g
b a sa l p lu s
S to p S I T A G L IP T I N
tr ip le th e r a p yO r
A d d it io n o f s u lp h o n ly u r e a a n d /o r b a s a l in s u l in
O rIn te n s ife d in su l in r e g im e n e g
b a sa l p lu sA d d E x e n a t id e to S u lp h o n ly u r e a a n d
o r M e tfo rm inA d d E x e n a t id e to S u lp h o n ly u r e a a n d
o r M e tfo rm in
H b A 1 C ≥ 7 %
H b A 1 C ≥ 7 %
L ife s ty le c h a n g e a n d M e tfo rm in
D ia g n o s is
A d dP I O G L IT A Z O N E
H b A 1 C ≥ 7 %
Y E S
Summary
• Type 1 diabetes requires diet and insulin treatment
• Type 2 requires diet, oral hypoglycaemic agents and or insulin
• Choice is agent depends on patient weight and ability to tolerate drug

Any Questions ?