TUTORIAL 02/04/2015 ECG/X-RAY/DATA INTERPRETATION.
13
TUTORIAL 02/04/2015 ECG/X-RAY/DATA INTERPRETATION
-
Upload
jasmine-york -
Category
Documents
-
view
223 -
download
1
Transcript of TUTORIAL 02/04/2015 ECG/X-RAY/DATA INTERPRETATION.
TUTORIAL 02/04/2015
ECG/X-RAY/DATA INTERPRETATION
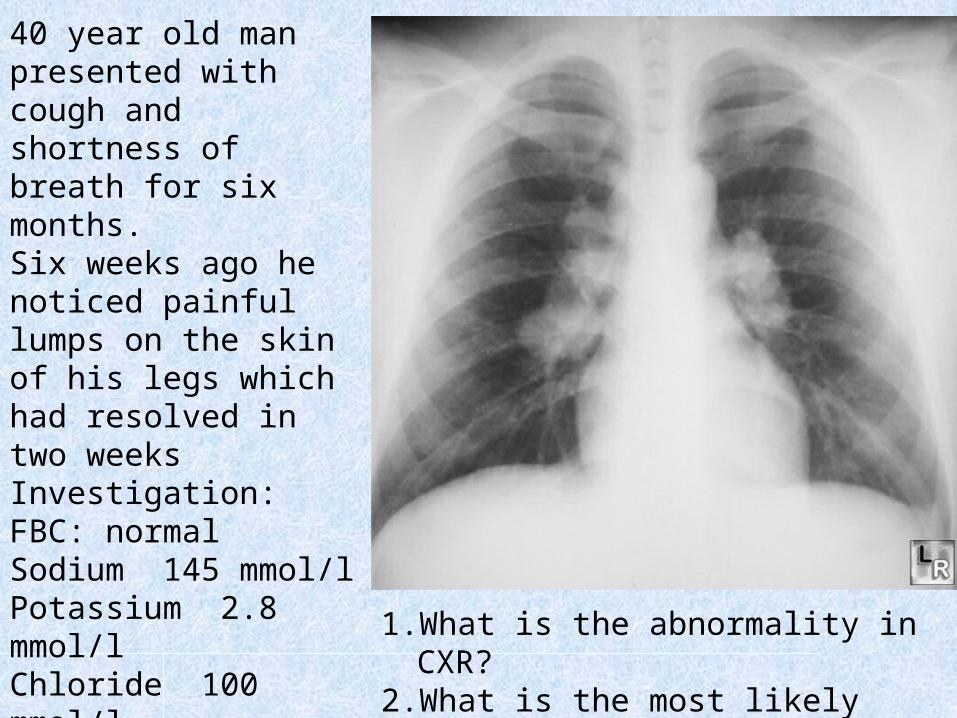
40 year old man presented with cough and shortness of breath for six months.Six weeks ago he noticed painful lumps on the skin of his legs which had resolved in two weeks Investigation:FBC: normalSodium 145 mmol/lPotassium 2.8 mmol/lChloride 100 mmol/lUrea 2.4 mmol/lSerum creatinine 83 µmol/lCalcium 3.4 mmol/l
1. What is the abnormality in CXR?
2. What is the most likely diagnosis?
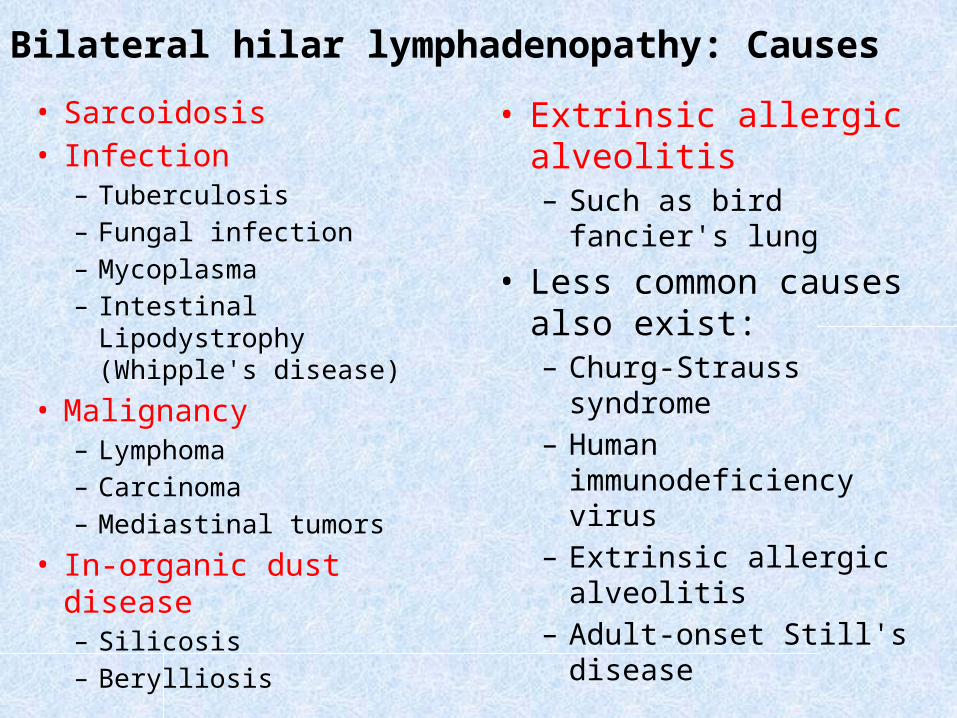
• Sarcoidosis• Infection
– Tuberculosis– Fungal infection– Mycoplasma– Intestinal Lipodystrophy
(Whipple's disease)
• Malignancy– Lymphoma– Carcinoma– Mediastinal tumors
• In-organic dust disease– Silicosis– Berylliosis
• Extrinsic allergic alveolitis– Such as bird
fancier's lung
• Less common causes also exist:– Churg-Strauss
syndrome– Human
immunodeficiency virus
– Extrinsic allergic alveolitis
– Adult-onset Still's disease
Bilateral hilar lymphadenopathy: Causes
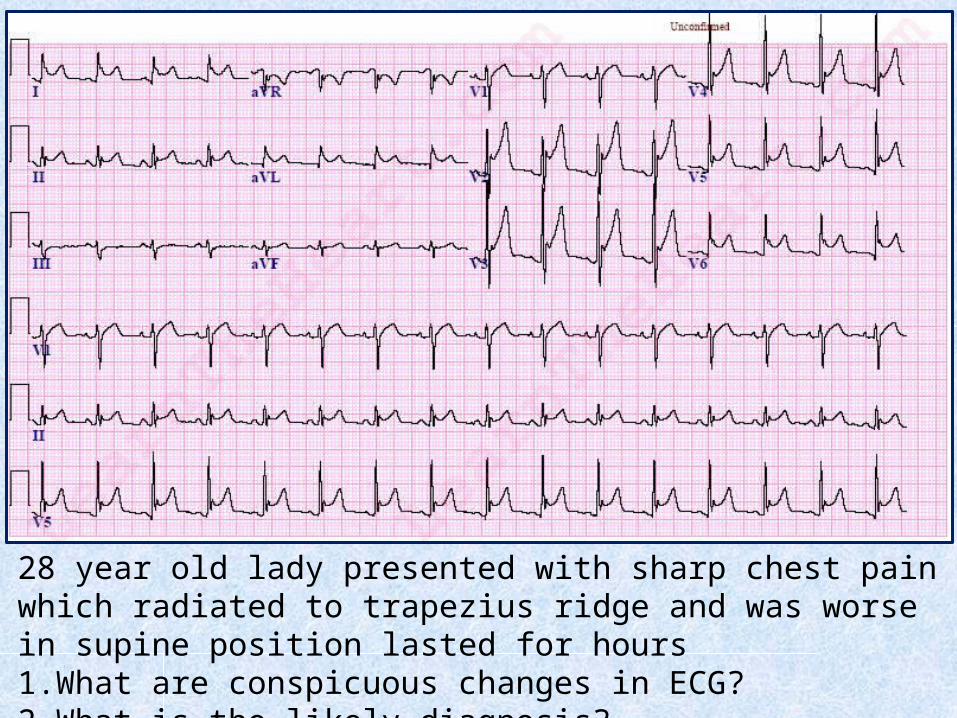
28 year old lady presented with sharp chest pain which radiated to trapezius ridge and was worse in supine position lasted for hours1. What are conspicuous changes in ECG? 2. What is the likely diagnosis?
Idiopathic causes• Infectious conditions:
– Viral– Bacterial– TB
• Inflammatory disorders:– RA – SLE – Scleroderma– Rheumatic fever
• Metabolic disorders:– Renal failure– Hypothyroidism– Hypercholesterolemia
• Cardiovascular disorders:– Acute MI – Dressler syndrome– Aortic dissection
• Miscellaneous causes:– Iatrogenic, – Neoplasms, – Drugs, – Irradiation, – Cardiovascular
procedures– Trauma
Pericarditis: Causes:
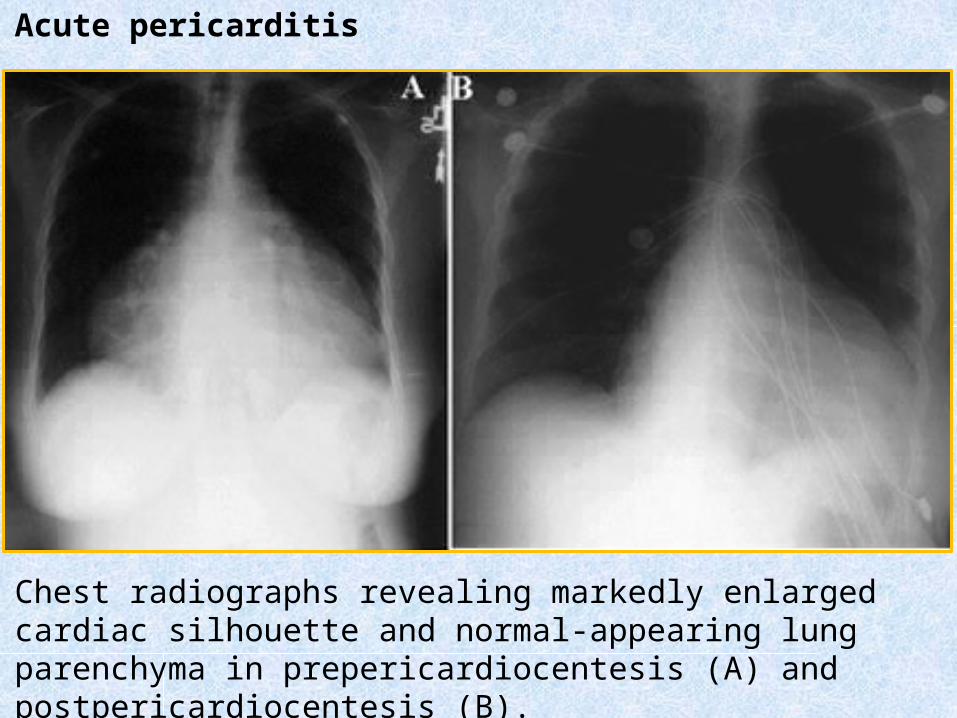
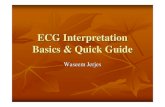
Chest radiographs revealing markedly enlarged cardiac silhouette and normal-appearing lung parenchyma in prepericardiocentesis (A) and postpericardiocentesis (B).
Acute pericarditis
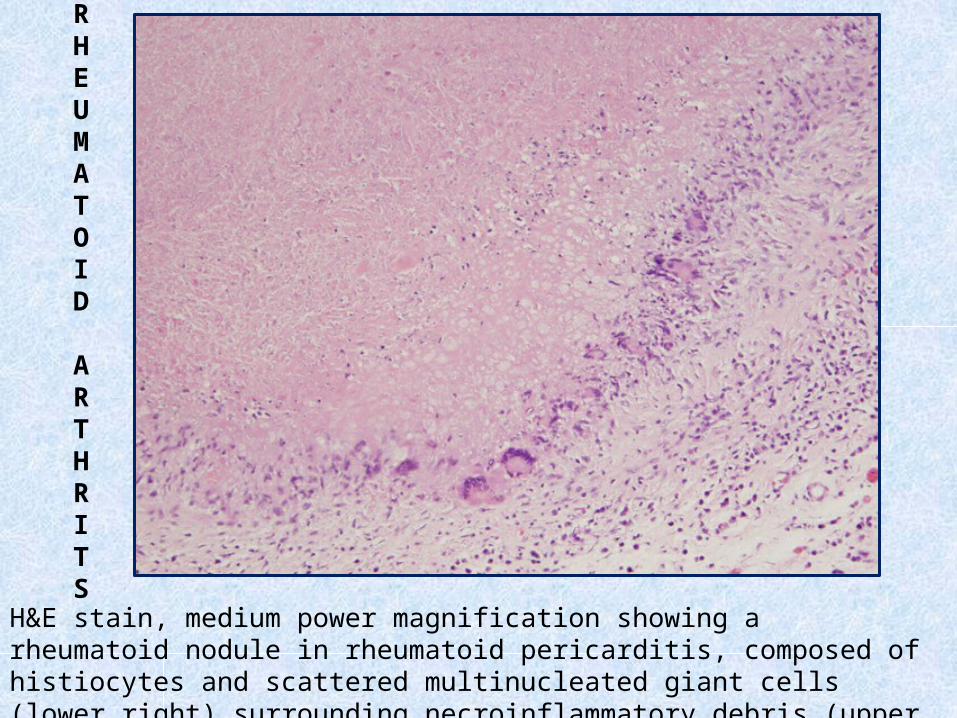
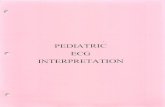
H&E stain, medium power magnification showing a rheumatoid nodule in rheumatoid pericarditis, composed of histiocytes and scattered multinucleated giant cells (lower right) surrounding necroinflammatory debris (upper left)
RHEUMATOID
ARTHRITS
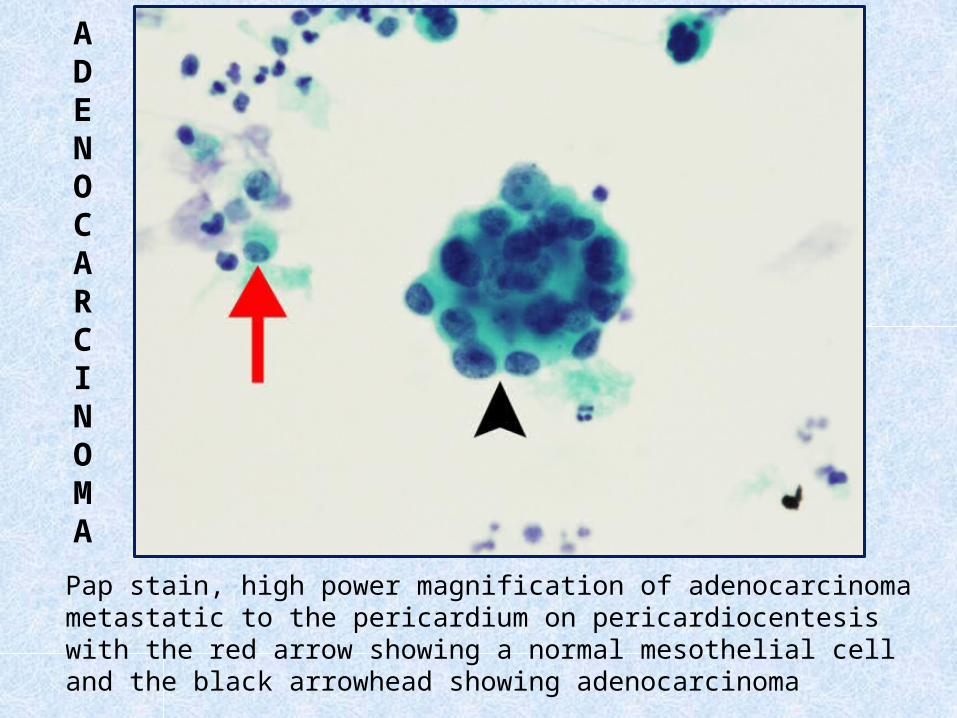
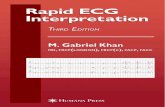
Pap stain, high power magnification of adenocarcinoma metastatic to the pericardium on pericardiocentesis with the red arrow showing a normal mesothelial cell and the black arrowhead showing adenocarcinoma
ADENOCARCINOMA
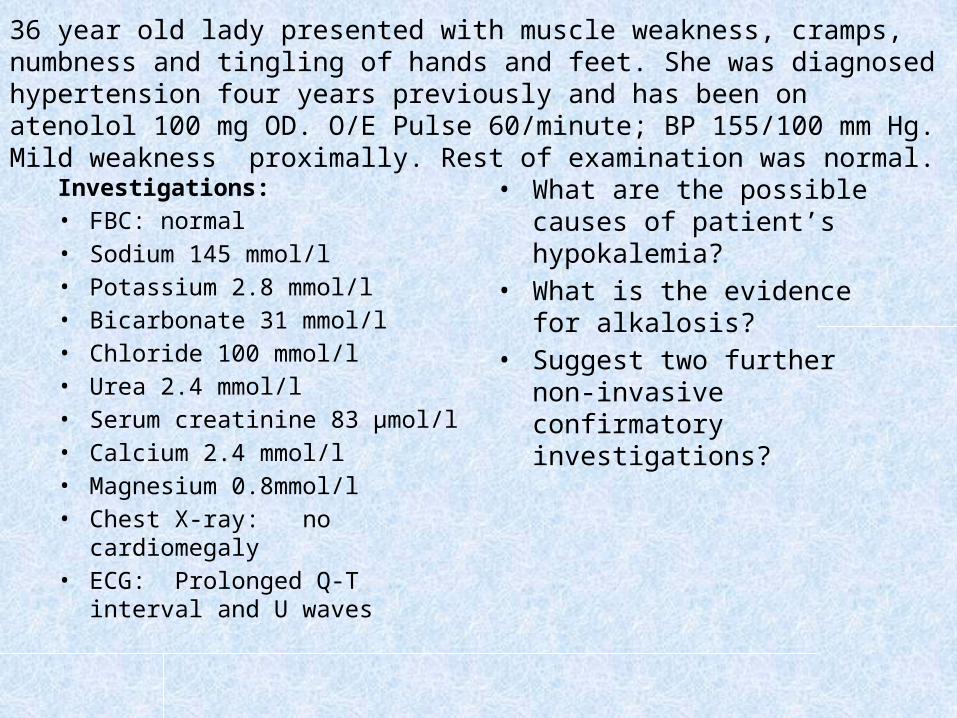
Investigations:• FBC: normal• Sodium 145 mmol/l• Potassium 2.8 mmol/l• Bicarbonate 31 mmol/l• Chloride 100 mmol/l• Urea 2.4 mmol/l• Serum creatinine 83 µmol/l• Calcium 2.4 mmol/l• Magnesium 0.8mmol/l• Chest X-ray: no
cardiomegaly• ECG: Prolonged Q-T
interval and U waves
• What are the possible causes of patient’s hypokalemia?
• What is the evidence for alkalosis?
• Suggest two further non-invasive confirmatory investigations?
36 year old lady presented with muscle weakness, cramps, numbness and tingling of hands and feet. She was diagnosed hypertension four years previously and has been on atenolol 100 mg OD. O/E Pulse 60/minute; BP 155/100 mm Hg. Mild weakness proximally. Rest of examination was normal.
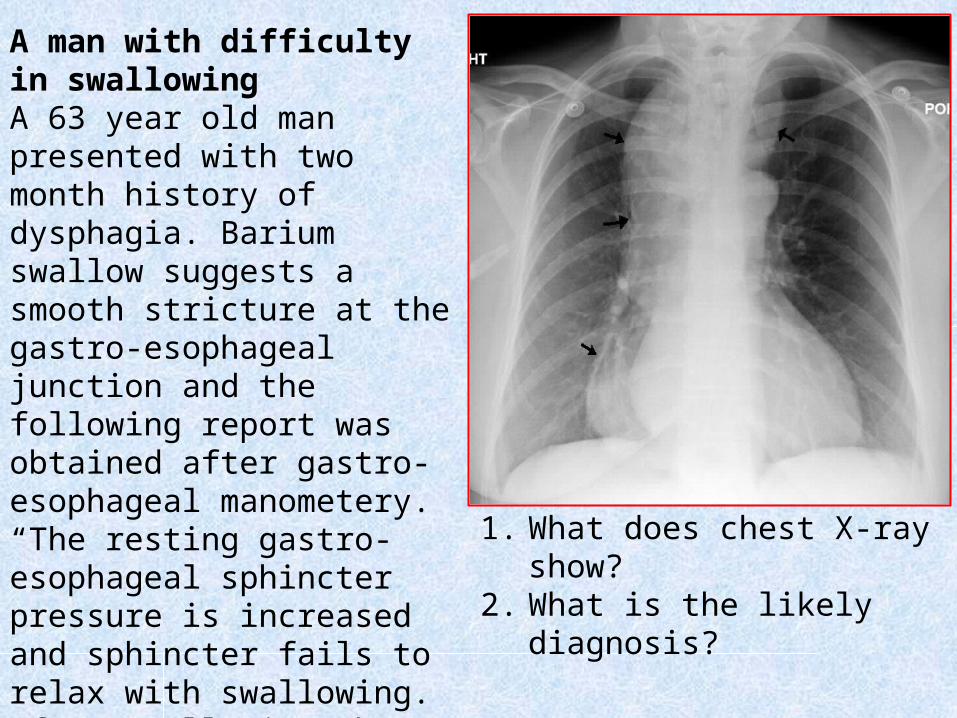
1. What does chest X-ray show?
2. What is the likely diagnosis?
A man with difficulty in swallowingA 63 year old man presented with two month history of dysphagia. Barium swallow suggests a smooth stricture at the gastro-esophageal junction and the following report was obtained after gastro-esophageal manometery.“The resting gastro-esophageal sphincter pressure is increased and sphincter fails to relax with swallowing. After swallowing there are no peristaltic contractions occurring simultaneously.”
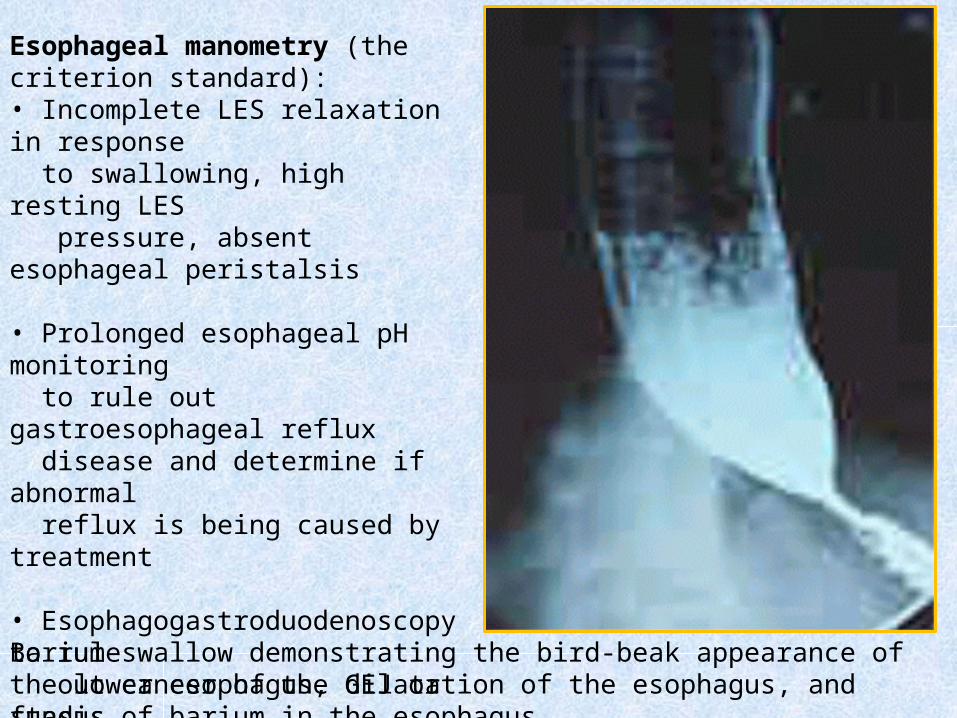
Barium swallow demonstrating the bird-beak appearance of the lower esophagus, dilatation of the esophagus, and stasis of barium in the esophagus.
Esophageal manometry (the criterion standard): • Incomplete LES relaxation in response to swallowing, high resting LES pressure, absent esophageal peristalsis • Prolonged esophageal pH monitoring to rule out gastroesophageal reflux disease and determine if abnormal reflux is being caused by treatment
• Esophagogastroduodenoscopy to rule out cancer of the GEJ or fundus• Concomitant endoscopic ultrasonography if a tumor is suspected
A 40 year old man presented with fatigue, fever and painful goitre. The results of investigations were as follows:• Hb 14.3 g/dl• WBC 11.2 x 109/l
• ESR 100 mm in the first hour• T4 32.4pmol/l (NR 9.4 – 24.5)• TSH ˂ 0.1mU/l (NR 0.5 – 5.5 )• Radio-iodine 131 thyroid scan: uptake at 4 hours ˂ 5%
(normal range 6 -18%)
1. What are the lab result abnormalities?2. What is the most likely diagnosis?3. What treatment is required?
A man with painful goitre
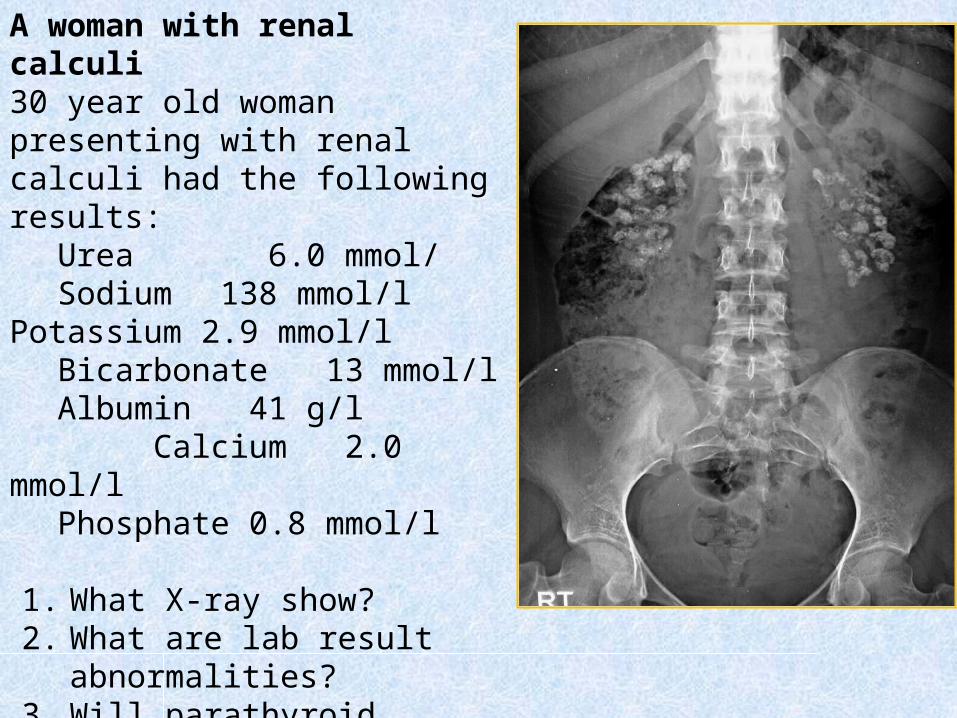
A woman with renal calculi30 year old woman presenting with renal calculi had the following results:
Urea 6.0 mmol/Sodium 138 mmol/lPotassium 2.9 mmol/lBicarbonate 13 mmol/lAlbumin 41 g/l
Calcium 2.0 mmol/lPhosphate 0.8 mmol/l
1. What X-ray show?2. What are lab result
abnormalities?3. Will parathyroid hormone
concentration prove high or low ?