
TURNING THE TIDE - Twin Cities Medical Society - Home€¦ · TURNING THE TIDE Easy Tools for ... 0...
46
1 TURNING THE TIDE Easy Tools for Clinicians to Prevent Type 2 Diabetes Recorded: October 5, 2016 Twin Cities Medical Society In partnership with Minneapolis Department of Health Minnesota Department of Health Minnesota Medical Association
-
Upload
phungkhanh -
Category
Documents
-
view
214 -
download
1
Transcript of TURNING THE TIDE - Twin Cities Medical Society - Home€¦ · TURNING THE TIDE Easy Tools for ... 0...
1
TURNING THE TIDE
Easy Tools for Clinicians to Prevent Type 2 Diabetes
Recorded: October 5, 2016
Twin Cities Medical Society
In partnership with
Minneapolis Department of HealthMinnesota Department of HealthMinnesota Medical Association
2
Turning the TideEasy Tools for Clinicians to Prevent
Diabetes
3 one-half hour segments:
• What is Prediabetes?
• National Diabetes Prevention Program and Local Resources
• Billing and Coding for Reimbursement
Accreditation Statement:
This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education through the joint providership of the Minnesota Medical Association and Twin Cities Medical Society. The Minnesota Medical Association is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.

3
CME Statement:
The Minnesota Medical Association designates this enduring activity for a maximum of 1.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Moderator
Nancy Bauer, Associate Director,
Twin Cities Medical Society and Moderator
4
Turning the Tide:Easy Tools for Clinicians to Prevent
Type 2 Diabetes
Please remember to complete the evaluation and posttest following Segment 3 to obtain CME
credit/certificate of attendance for this webinar.
Thank you for your interest!
Turning the Tide : Easy Tools for Clinicians to Prevent Type 2 Diabetes
Segment 1: The Rise of Prediabetes and Diabetes, and How to Identify
People at Risk
5
Presenter
Kacey Justesen, M.D., Medical Director,
Broadway Family Medicine Clinic, Assistant Professor, University of Minnesota Department of Family Medicine and Community Health
Participants will be able to:
1. Describe prediabetes and the implications for patients
2. Identify those at risk for prediabetes through screening and result interpretation
3. Explain the Diabetes Prevention Program and the resources and information on how to access referral services
4. Discover information on billing and coding for reimbursement of prediabetes screening and program services
Objectives:

6
What is Prediabetes ?• Prediabetes is a reversible condition in which blood
glucose levels are higher than normal, but not high enough to be classified as type 2 diabetes (DM2)
Diabetes• HbA1c ≥ 6.5%• Fasting plasma glucose ≥ 126
mg/dL• 2-hour OGTT glucose ≥ 200
mg/dL
Prediabetes• HbA1c 5.7% ‐ 6.4%
• Fasting plasma glucose 100‐125 mg/dL
• 2‐hour OGTT glucose 140‐199 mg/dL
• People with prediabetes have increased risk of:
Why it Matters
CDC National Diabetes Fact Sheet 2014

7
Prediabetes and diabetes are a continuum
Time (years)
100
200
Fasting Blood Glucose
PDM DM
Lifetime Risk of Diabetes by BMI
0%
20%
40%
60%
80%
100%
WhiteFemale
WhiteMale
BlackFemale
BlackMale
HispanicFemale
HispanicMale
<18.5 18.5 ‐ 24.9 25 ‐ 29.9 30 ‐ 34.9 35+
*Estimated lifetime prevalence of diabetes by sex, race, and BMI category at age 18 todayNarayan et al., JAMA. 2003 Oct 8;290(14):1884-90.
BMI Category
8
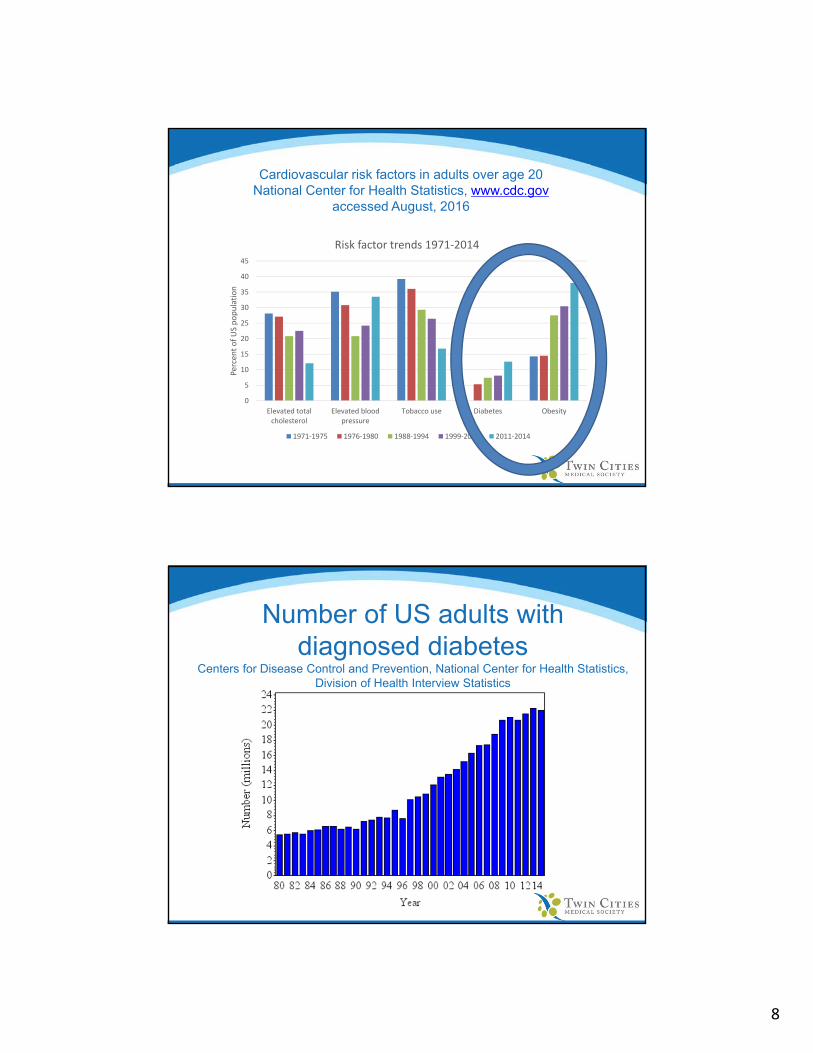
Cardiovascular risk factors in adults over age 20National Center for Health Statistics, www.cdc.gov
accessed August, 2016
0
5
10
15
20
25
30
35
40
45
Elevated totalcholesterol
Elevated bloodpressure
Tobacco use Diabetes Obesity
Percent of US population
Risk factor trends 1971‐2014
1971‐1975 1976‐1980 1988‐1994 1999‐2000 2011‐2014
Number of US adults withdiagnosed diabetes
Centers for Disease Control and Prevention, National Center for Health Statistics, Division of Health Interview Statistics

9
Diabetes prevalence has risen and is at an all-time high
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Percentage of Minnesota
Adults
Year*,**
The diabetes prevalence among adults in MN (2014) is 8.1%.
*Note: Percentages are age‐adjusted to account for any changes in age distribution in the MN population over time.**Percentages reflect an average of 2‐3 years of data.
Sources: Centers for Disease Control and Prevention: National Diabetes Surveillance System. http://apps.nccd.cdc.gov/DDTSTRS/default.aspxMDH analyses of Behavioral Risk Factor Surveillance System Data.
CDC estimates 37% of adults have prediabetes and yet...
• In 2014, only 6.1% of Minnesota adults said they knew that they had prediabetes.
Source: MDH Analyses of Behavioral Risk Factor Surveillance System Displayed on the Diabetes Dashboardhttp://www.health.state.mn.us/diabetes‐dashboard/

10
Rate of diabetes differ across communities
http://www.health.state.mn.us/divs/healthimprovement/data/reports/diabetesincome.html
Why it MattersType of Expense Total Cost in 2012
Extra medical costs due to diabetes & lost productivity
$3.14 billion
Total medical spending for insured Minnesotans with diabetes
$5.2 billion
• Average medical spending for insured Minnesotans with diabetes
• $16,300 per person
ADA. Diabetes Care 36(4):1033‐46.MDH Analyses of the All‐Payer Claims Database http://www.health.state.mn.us/divs/hpsc/hep/publications/costs/20160127_chronicconditions.pdf
11
Why is Prediabetes on the rise?
Pathophysiology of Obesityand Insulin Resistance (IR)
• How obesity => IR is not fully understood, but many defects in insulin signaling have been discovered
Fat and/or Muscle Cell
12
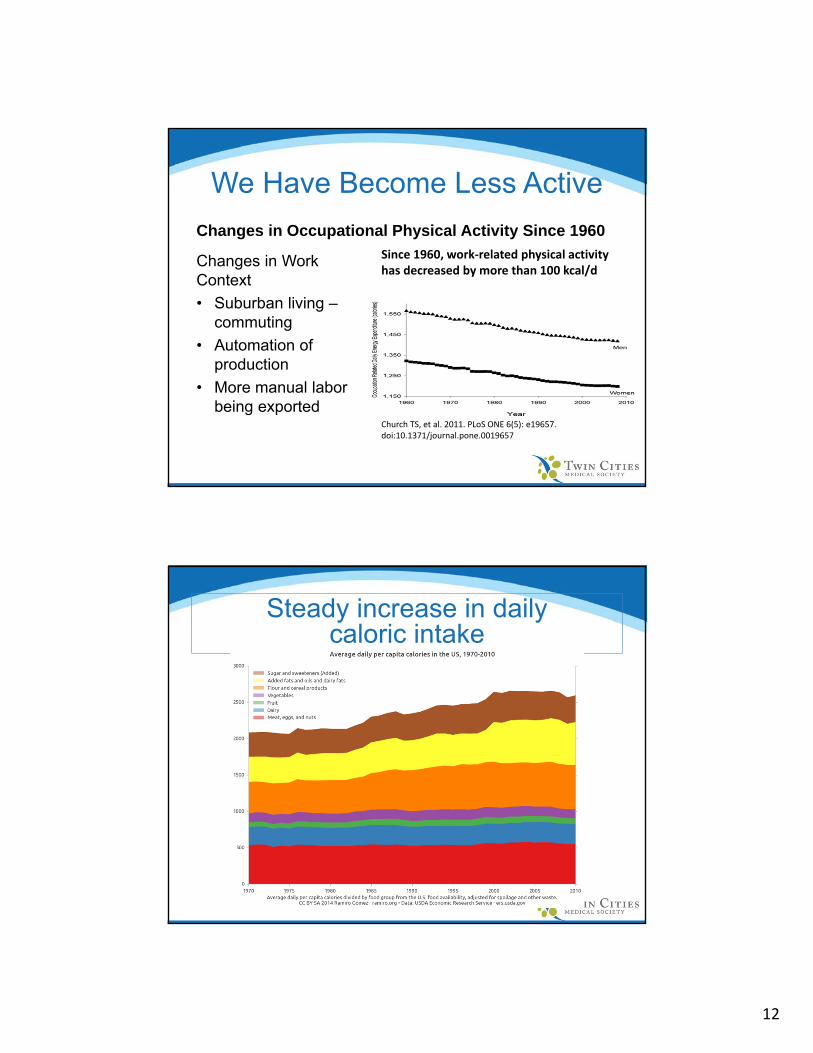
We Have Become Less Active
Changes in Occupational Physical Activity Since 1960
Changes in Work Context
• Suburban living –commuting
• Automation of production
• More manual labor being exported
Church TS, et al. 2011. PLoS ONE 6(5): e19657. doi:10.1371/journal.pone.0019657
Since 1960, work‐related physical activity has decreased by more than 100 kcal/d
Steady increase in daily caloric intake

13
• SCREEN the appropriate patients based on their risks
• TEST with approved screening tests
• ACT TODAY by educating patients regarding prediabetes and the risks and encouraging patient participation in programs proven to decrease their risk of progression to diabetes
We must address this problem STAT!
Integrating Diabetes Preventioninto Your Practice
14
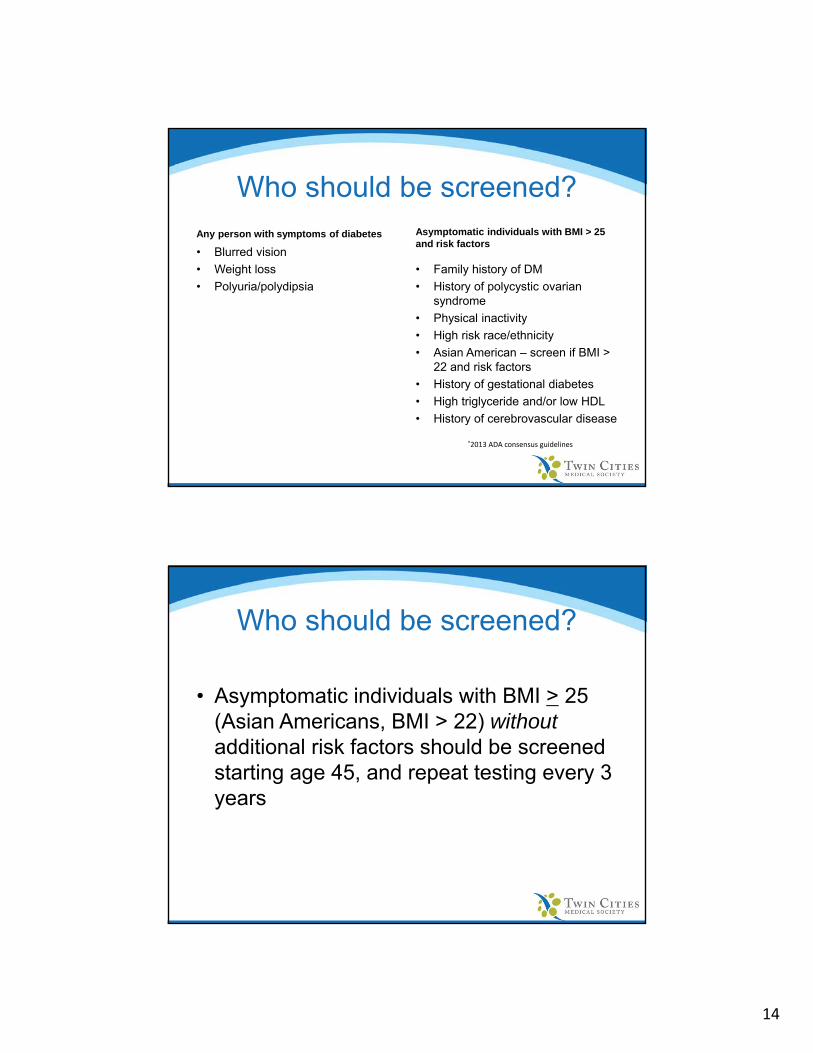
Who should be screened?Any person with symptoms of diabetes
• Blurred vision
• Weight loss
• Polyuria/polydipsia
Asymptomatic individuals with BMI > 25 and risk factors
• Family history of DM
• History of polycystic ovarian syndrome
• Physical inactivity
• High risk race/ethnicity
• Asian American – screen if BMI > 22 and risk factors
• History of gestational diabetes
• High triglyceride and/or low HDL
• History of cerebrovascular disease
*2013 ADA consensus guidelines
• Asymptomatic individuals with BMI > 25 (Asian Americans, BMI > 22) without additional risk factors should be screened starting age 45, and repeat testing every 3 years
Who should be screened?

15
• HbA1c, fasting plasma glucose, and 2 hour OGTT are all approved screening tests
• Remember the prediabetes criteria:
• HbA1c 5.7% - 6.4%
• Fasting plasma glucose 100-125 mg/dL
• 2-hour OGTT glucose 140-199 mg/dL
How to test?
• Practically, the fasting glucose is inexpensive and easy to obtain• If patient is not fasting for the appointment,
consider a screening HbA1c test
• 2 hour OGTTs are rarely performed due to time• 1 and 3 hour OGTT remain the test of choice
for detecting GDM
How to test?

16
• Review the risk of developing DM2• 5 yr risk = 15-30%
• Encourage weight loss by setting specific and attainable goals• Loss of 5-7% body weight has been proven to reduce risk• Exercise! 150 min/week of moderate activity (walking)
• Referral to Registered dietician or certified diabetes educator for further nutrition education
• Referral to National Diabetes Prevention Program (NDPP)• www.cdc.gov/DIABETES/prevention
So your patient has prediabetes, now what? Act today!
What is the National Diabetes Prevention Program?
• It is a year long program starting with 16 weekly sessions then monthly for remainder of the year
• Group sessions
• Goal to lose/maintain > 5-7% of body weight
• Cut down dietary calories & fat
• ≥150 min/week moderate physical activity
• Education & training in behavior modification (Self-monitoring; problem solving)
• Strong support structure (building self esteem, empowerment, social support; accountability)
17
www.cdc.gov/diabetes/prevention
www.preventdiabetesstat.org

18
• Resources to Engage the Health Care Team
• Tools to Engage Patients
• Guides for Integrating Screening, Counseling and Referral for Diabetes Prevention into Practice
CDC/AMA TOOLKIT FOR PROVIDERS
Resources for Patients

19
• Operators provide low- and no-cost options for local classes in Minneapolis and healthy lifestyle resources throughout the state of Minnesota
• Diabetes Prevention Program classes in Minneapolis are offered in a variety of culturally diverse formats
• Translation assistance available for callers (Spanish, Hmong, Somali, Oromo)
• In person and online classes available
Diabetes Prevention ConnectionCall Center for Referrals
• Obesity, prediabetes, and diabetes are closely linked and are on the rise in Minnesota and across the country
• Prediabetes is an easily diagnosable condition
• Prediabetes can be effectively treated and diabetes can be prevented
• Lifestyle intervention has been proven to be effective in delaying the onset of diabetes
• Enrolling patients in National Diabetes Prevention Program classes is easy with the Diabetes Prevention Connection referral phone line
Summary
20
Turning the Tide : Easy Tools for Clinicians to Prevent Type 2 Diabetes
Segment 2: What is the Diabetes Prevention Program and How to Refer to the Diabetes Prevention Connection
Diabetes Unit
PresentersHoua Vue-Her, RD, Ph.D.
Diabetes Prevention PlannerMinnesota Department of HealthDiabetes Unit, Health Promotion and
Chronic Disease Division
Steve Vincent, M.D.
Chief Medical Officer
People’s Center Health Services

21
Overview
• Diabetes in the US and MN
• The National Diabetes Prevention Program
• Diabetes Prevention Program Research Study
• Diabetes Prevention Program‐Structure
• Provider experience referring to DPP
• Dr. Vincent, People’s Center Health Services
• Diabetes Prevention Connection
Setting the Stage
DIABETES • 29.1 million people
• 1 out of every 11 people
• 1 out of 4 people don’t know they have diabetes
Prediabetes• 86 million adults
• 1 out of 3 adults
• 9 out of 10 don’t know they have prediabetes
CDC National Diabetes Statistics Report, 2014

22
CDC Infographic: A Snapshot of Diabetes in The United States, 2015
Setting the Stage
Recap from Dr. Justesen presentation:
• Diabetes and Prediabetes is on the rise
• Few adults with prediabetes in MN know they have it
• Adults in MN household earning less than $35,000/yr are 2.5 times as likely to have diabetes
• Minnesotans with diabetes spend a total of $5.2 billion on medical cost in 2012
Setting the Stage

23
What Can Be Done?
• Research shows if you have prediabetes, losing weight by healthy eating and being more active:
CDC Infographic: A Snapshot of Diabetes in The United States, 2015
Structured lifestyle change programs, like Diabetes Prevention Program, can help!
Goal: to determine if losing modest amounts of weight through improving diet and increasing physical activity, or taking the diabetes drug metformin, could prevent or delay type 2 diabetes in people at high risk for developing the disease.
Major multicenter clinical research study
– 3,234 participants– 27 clinical centers in U.S.– Funded primarily by NIH
The Diabetes Prevention Program Research Study

24
The Diabetes Prevention Program Research Study
• Lifestyle Intervention• One‐on‐one instruction
• Healthcare professional
• Structured program
• Primary goals• 7% weight loss
• 150 minutes/week physical activity
• Attend 16 weekly sessions, follow curriculum covering diet, physical activity and behavior change
• After weekly sessions, attend monthly sessions to reinforce behavior changes
The Diabetes Prevention Program Research Study
• Results – Type 2 diabetes risk reduced for participants in the Lifestyle Intervention
Population Lifestyle Intervention vs.
Placebo
Metformin vs. Placebo
Overall 58% 31%
Seniors (over 60) 71% 11%
White 51% 24%
African American 61% 44%
Hispanic 66% 31%
American Indian 65% 25%
Asian 71% 38%Diabetes Prevention Program Research Group NEJM 2002; 346, No. 6: 393‐403

25
The Diabetes Prevention Program Research Study‐10 Year follow‐up
• 10—year follow‐up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcome Study
• 34% decrease in new cases of diabetes over 10 yearsLancet. 2009 November 14; 374(9702): 1677-1686. doi:10.1016/S0140-6736(09)6147-4.
Year follow‐up‐Continued Lifestyle Intervention• 34% reduced rate compared with placebo• 49% reduced rate in those age 60 and older compared with placebo • Delayed type 2 diabetes by about 4 years compared with placebo• Reduced hemoglobin A1c and fasting glucose compared with
placebo
Metformin • 18% reduced rate compared with placebo• Delayed diabetes by 2 years compared with placebo • Reduced hemoglobin A1c and fasting glucose compared with
placebo

26
It worked! Now what?
• Translating the program from an individual based format to a group based format
• Testing the translations
• Find a selection of translational studies based on the DPP at:
http://icanpreventdiabetes.org/articles/
• Expanding the program
• Congress authorized CDC to lead the NDPP
• Payment for the program
Diabetes Prevention Program Structure
• Group based
• Facilitated by a trained Lifestyle Coach
• Offers group education & support over minimum 22 hour long sessions• 16 weekly sessions (over six months)
• Monthly sessions for the remainder of the year
• In‐person or online

27
DPP Curriculum Curriculum Focus Session Number and Topic
Behavior Change Skills
Control the external environment
Psychological and emotional Skills
1. Introduction to the Program2. Get Active to Prevent Type 2 Diabetes
(T2)3. Track Your Activity4. Eat Well to Prevent T25. Track Your Food6. Get More Active7. Burn More Calories Than You Take In8. Shop and Cook to Prevent T29. Manage Stress10. Find Time for Fitness11. Cope with Triggers 12. Keep Your Heart Healthy13. Take Charge of Your Thoughts14. Get Support15. Eat Well Away from Home16. Stay Motivated to Prevent T2
Who is Eligible for the DPP?
• Adults 18 years and older
• BMI ≥24 unless of Asian ancestry (then BMI≥22)
• Not Pregnant
• Do not have type 1 or 2 diabetes
• And has one of the following:• Diagnosis of prediabetes by a blood test
• Diagnosis of gestational diabetes
• Score of 5 or more on prediabetes risk test

28
CDC Paper Risk Test
• A score of 5 or greater indicates a person is at increased risk for having prediabetes
• Available at ‐ https://doihaveprediabetes.org/prediabetes‐risk‐test.html
DPP Delivery Settings
• Hospitals and Clinics• Community organizations
• Faith‐based organizations• Workplaces
• Senior Centers• And more……
29
DPP Payment
• DPP coverage for people on Medicaid
• Growing DPP coverage for private and public employees
• Medicare coverage starting in 2018
DPP in Action:People’s Center Health Services
Steven R. Vincent, MD, Medical DirectorNawal Hirsi, B.S., NutritionAbiin Mohamud, C.M.A.
Nimco Abas
We Can Prevent Diabetes Program2014 ‐ 2015Grant funded

30
DPP in Action:People’s Center Health Services
• Federally Qualified Health Center located in the Cedar Riverside neighborhood of Minneapolis
• Predominantly East African community from Somalia and Ethiopia – a majority of our patients
• Diverse urban mix of other patients not from East Africa
Neighborhood Demographics

31
DPP in Action:People’s Center Health Services
2014
• Instructors from YMCA with bilingual coaches
• 16 weeks
• Group instruction and discussion
• YMCA gym membership
• Gift card incentives: $10, based on attendance and/or group weight loss
• If truly motivated, incentives not important
DPP in Action:People’s Center Health Services
2015
• YMCA grant concluded; participants apply for YMCA discount membership
• Walking in apartment buildings and outdoors
• 2 Groups led by staff: Nawal Hirsi, B.S.
• Somali speaking participants
• English speaking participants

32
DPP in Action:People’s Center Health Services
Recruitment of participants• Registry for BMI >24.9, care coordinator contacted patient about We Can Prevent Diabetes, scheduled clinic visit for lab tests and education with dietitian if appropriate
• Referral from providers in EMR to Dietitian
• Warm hand off by providers to care coordinator–worked the best when identified as having pre‐diabetes
DPP in Action:People’s Center Health Services
• Morning and afternoon class times, mindful of Muslim mid‐day prayers
• Reminder calls were important• The day before• The morning of the class
• Consistent staff helpful: one coordinator, one coach
• Arrangement of transportation for participants proved crucial for attendance

33
DPP in Action:People’s Center Health Services
• Enrolled 167 participants into classes
• 38% male, 62% female; 84% black or African American, 4% Native American and 10% white. 56% spoke Somali as their primary language
• Total weight loss for People’s Center participants was 477 pounds.
80%
20%
Attendance of 4+ Sessions (n = 117)
Attended 4+ Session Did not attend 4+ sessions
14
53
18
11
5
5% weight reduction 7% weight reduction 10% weight reduction
Percent of Participan
ts
Amount of Weight Reduction
End of Study Weight Reduction
Peoples (n = 117) Total (n = 1154)
DPP in Action:People’s Center Health Services
Keys to Success
• PCP has conversation about pre‐diabetes diagnosis and recommends DPP to patient
• Instructors from same community as the participants
• Reminder calls and transportation
• Class times considerate to community

34
DPP in Action:People’s Center Health Services
The Story of Awil• He absorbed everything he learned in class• He brought what he learned home to his wife; they changed their meals and shopping
• He started going to the gym regularly• He sponsored friends with guest memberships at gym
• He had a large weight loss and his HGBA1C became normal
DPP in Action:People’s Center Health Services
2016 – 2017
Kelly Coughlin, RD, LD, CDE
• Three new DPP classes planned in partnership with University of Minnesota Extension SNAP Health and Nutrition Education
• Culturally Adapted Somali Class– Somali Speakers
• Culturally Adapted Ethiopian Class – Oromo Speakers
• English Speaking Class

35
We’ve come a long way…... but there are still gaps to providing the DPP
Referral Challenge
• Difficult to know where DPP classes are in the community
• Challenging to recruit enough at risk people into the program
Solution??Diabetes Prevention Connection: Call Center Pilot

36
Diabetes Prevention Connection:Referral Call Center Pilot
Populate Class Database
Promote DPP and Diabetes Prevention Connection
Referral to Call CenterCall Center confirms
eligibility & match caller to DPP class
Call Center Follows‐up
Caller Starts DPP Class
The Patient Experience
Providers give call center information to patient OR have clinic staff help patient make the call in clinic
1) Eligibility screening2) Class preferences including: in person or online, time, location,
language and more3) Warm hand off to DPP program coordinator
Call center agents will follow‐up with caller to confirm enrollment in DPP class and send them a letter with class information
Prior to starting the class DPP program coordinator will make reminder calls to participants
37
Summary
• Diabetes is growing problem
• 1 in 3 may have prediabetes but only 6% know it in MN
• The DPP has been proven to prevent or delay type 2 diabetes
• Physicians have a key role to play in testing those at risk and referring to the DPP
• Promote and use the Diabetes Prevention Connection to easily refer your patients
1‐888‐6HEALTH (1‐888‐643‐2584)Diabetes Prevention Connection

38
For more information contact:
Houa Vue‐Herhoua.vue‐[email protected]‐201‐5433
Or visit our website at: http://www.health.state.mn.us/diabetes/programs/
Best Practice: Screening & Referral
pat ient s for prediabetes usingt he CDC Prediabetes ScreeningTest (or t he Amer ican DiabetesAssociat ion Diabetes Risk Test )
pat ient s for prediabetes usingone of three blood tests
to help prevent diabetes byreferr ing pat ients w ith
prediabetes to a diabetesprevent ion program

39
Turning the Tide : Easy Tools for Clinicians to Prevent Type 2 Diabetes
Segment 3: Payment
Presenters
JoAnne Wolf, RHIT, CPC, CEMC, Coding Manager, Children’s Health Network
Sandy Lien, County Relationship Manager,
MEDICA State Public Programs
Nicole Evans, MA, Provider Trainer, MHCP, Minnesota Department of Human Services

40
Billing for ScreeningICD-10 Diagnosis Codes:
• Obesity• BMI = to or greater than 24• Elevated Blood Glucose• Previous Dx of Gestational Diabetes • Personal Hx of Gestational Diabetes• No Previous Dx of Diabetes• Encounter for Screening for Diabetes
Diagnostic Tests/ CPT Codes:Hemoglobin A1C: 83036 | Fasting Glucose: 82947 |2 hr Glucose (OGTT) : 82947, 82950
Billing for Counseling
ICD-10 Diagnosis Codes
• Obesity
• BMI 24 or greater
• Elevated Glucose
• History of Gestational Diabetes
• Dietary Counseling
• Prediabetes – New ICD-10-CM code effective 10/1/16

41
Billing for CounselingCodes and Authorized Providers: For all CPT/HCPCS Codes: -U7 modifier should be used when reporting services of a physician extender (non-enrolled APRNs)
• Medical Nutrition Therapy (MNT)• Enrolled licensed dieticians and nutritionists
• Education/Training for Patient Self-Management
• Enrolled PAs and APRNs• Physician Extenders
• Outpatient Evaluation and Management (E/M) Services
• Enrolled MD or NPP
Billing for CounselingDocumentation Requirements: All of the following codes are time-based, therefore time must be documented
• Medical Nutrition Therapy (MNT)• Detailed summary of the face-to-face counseling with the patient
• For group codes 97804 and G0271, document # of pts in group
• Education/Training Pt Self-Management• Detailed summary of the face-to-face education with the patient
• For group codes 98961 and 98962, document # of pts in group

42
Billing for CounselingDocumentation Requirements (continued):
• Outpatient E/M Services• When more than ½ of the E/M is spent in counseling, the level
can be billed based solely on the total amount of face-to-face time
• Documentation must show above: Example: “More than ½ of this visit was spent in counseling – Total time: 40 minutes” = 99215
• Very detailed summary of the counseling must also be documented
New Patient Visits Established Patient Visits
99201 10 minutes 99211 5 minutes
99202 20 minutes 99212 10 minutes
99203 30 minutes 99213 15 minutes
99204 45 minutes 99214 25 minutes
99205 60 minutes 99215 40 minutes
Who Can Refer to the DPP• Best-practice for ensuring insurance
coverage
• Document screening & counseling
• Include patient’s primary care provider (MD or APRN) name & link to Prediabetes diagnosisin the DPP referral note
• Have patient check insurance coverage beforecalling the Diabetes Prevention Connection –sliding scale & free classes are available
• Questions: Call DHS Provider Hotline (800) 366-5411

43
Determining Coverage for DPP
• Members call customer service• Providers call provider services• Code 0403T should be billed for the DPP
• Medica example• Considered a preventive benefit; no copays• Covered for fully insured group plans,
Medicaid and Individual• Self-Insured – determined by the employer
Health Plan Coding ContactsHealth Plan Provider/Claims Services
(coding, eligibility, benefits, claims, billing)Web site
BCBS, Blue Plus
651‐662‐52001‐800‐262‐0820
https://www.bluecrossmn.com/healthy/public/personal/home/providers/
www.bluecrossmn.com
HealthPartners952‐883‐7699888‐663‐6464
www.healthpartners.com
Medica
1‐800‐458‐5512option 1, then option 1 for the automated system,
or option 2 to speak with a representative
https://www.medica.com/providers/administrative‐resources/administrative‐manuals
www.medica.com
PreferredOne763‐847‐4000 1‐800‐940‐5049
www.perferredone.com
Sandfordwww.sanfordhealthplan.com/providerlogin or
Member Services at 1‐800‐752‐5863www.sandfordhealthplan.org
UCare612‐676‐33001‐888‐531‐1493
www.ucare.org

44
Process: How to Bill for the DPPif the patient has coverage (Medicaid/Commercial)
Eligible Providers• Organizations must have
full or pending CDC recognition as DPRP to provide the National DPP to MHCP recipients
• Clinics/ billable organizations will use code 0403T for DPP
Medicare: New DPP Coverage
Coming in 2018
• DPP First preventative service model to be expanded in to the Medicare Program
• https://innovation.cms.gov/initiatives/medicare-diabetes-prevention-program/

45
Diabetes Prevention Connection
Help Us Turn The Tide!
• Physicians/Clinicians: Refer ready patients to the Diabetes Prevention Connection for DPP Classes
• Clinics: Work with patients & insurers to determine cost coverage
• The Diabetes Prevention Connection offers:
• Matching & follow-up for DPP class enrollment• Scheduling convenience to meet patient needs• Cultural and language translation support

46
Twin Cities Medical Society1300 Godward Street NE, Suite 2000
Minneapolis, MN 55413
612.623.2885
www.MetroDoctors.com


















