
Tuesday Case Conference. Introduction What is Tenofovir disoproxil fumarte (TDF)? How Nucleotide RTI...
32
Tuesday Case Conference
-
Upload
eugene-bradford -
Category
Documents
-
view
217 -
download
0
Transcript of Tuesday Case Conference. Introduction What is Tenofovir disoproxil fumarte (TDF)? How Nucleotide RTI...

Tuesday Case Conference

Introduction
• What is Tenofovir disoproxil fumarte (TDF)?
• How Nucleotide RTI work
• Nephrotoxicity of NtRTI
• Is TDF Nephrotoxic?– In vitro evidence– Epidemiologic evidence

What is tenofovir disoproxil fumarate (TDF)?
• Orally administered pro-drug of tenofovir• Tenofovir is a nucleotide analogue inhibitor of reverse
transcriptase (NtRTI)– Others in the family are Adefovir and Cidofovir, well described
nephrotoxins– Tenofovir similar to Adefovir– The only NtRTI used for treatment of HIV
TDF
• Single Agent– Viread
• marketed for the treatment of HIV since 2001
• Combination– Truvada
• Fixed-dose combination – TDF and emtricitabine (NRTI), 2004
– Atripla• Fixed-dose triple combination of
– TDF, emtricitabine (NRTI) and efavirenz (NNRTI), 2006

Reverse Transcriptase Inhibitors
• Competitive substrate inhibitors– Nucleoside RTI (NRTI)– Nucleotide RTI (NtRTI)
• Non-competitive substrate inhibitor– Non-nucleoside RTI (NNRTI)
www.web-books.com/.../Images/HIV_Cycle.jpg
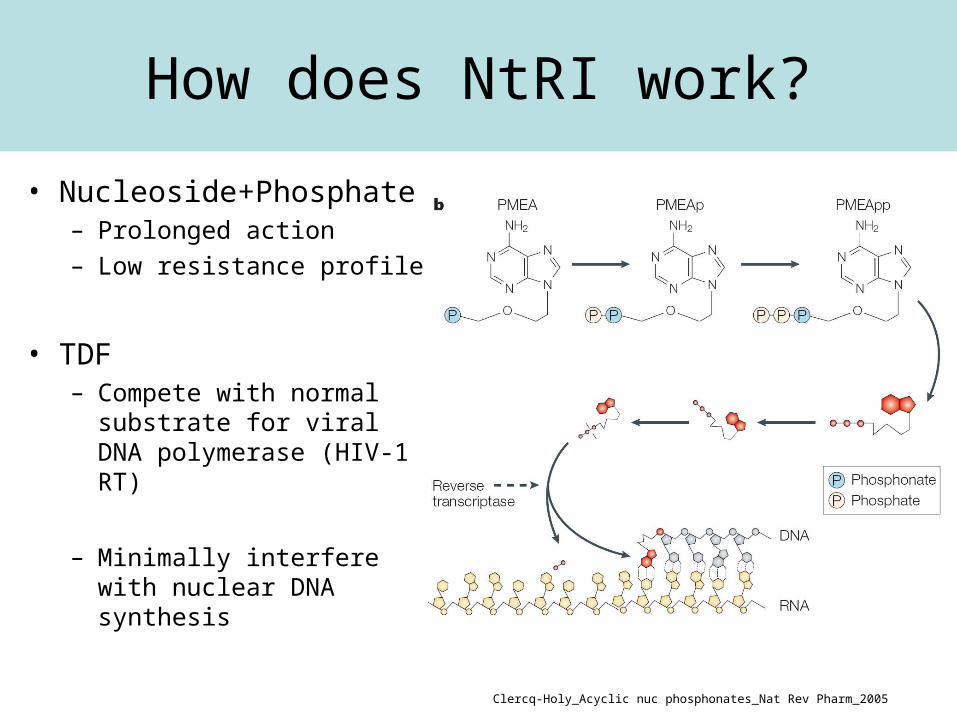
How does NtRI work?
• Nucleoside+Phosphate– Prolonged action– Low resistance profile
• TDF– Compete with normal
substrate for viral DNA polymerase (HIV-1 RT)
– Minimally interfere with nuclear DNA synthesis
Clercq-Holy_Acyclic nuc phosphonates_Nat Rev Pharm_2005

TDF in treatment of HIV infectionClercq-Holy_Acyclic nuc phosphonates_Nat Rev Pharm_2005
Regimen with TDF
• >80% of patients with HIV RNA (<50 copies per ml) at 48 weeks

Is TDF nephrotoxic?
• Potential for nephrotoxicity– Similar structure to Adefovir,
known nephrotoxin– Accumulation in renal
proximal tubule• Vd of 0.8 L/kg• Minimally protein bound (<8%)• Mainly excreted in urine,
unchanged pro-drug from
– The Mitochondrial Cytopathy Hypothesis
TDF
Blood Lumen
OAT1
MRP
ProximalTubule

TDF is eliminated through the Kidney
TenofovirTenofovir
Potential for accumulation of high concentration of TDF
in proximal tubule cells
MRP 2 / 4
ATP

Mechanisms of Tubular ToxicityThe Mitochondrial Cytopathy Hypothesis
http://www.retroconference.org/2002/Posters/13560.pdf

In vitro study

In vitro assessment of mitochondrial toxicity
The effect of TDF and other NRTIs on mtDNA synthesis
Birkus-Cihlar_Assmt of Mitochondrial Toxicity in Human CellsTreated with Tenofovir_AAC_2002
Tenofovir has little mitochondrial toxicity
In vitro study

In vitro studyEffects of tenofovir and cidofovir on the human renal proximal
tubule epithelial cells
Cihlar-Hitchcock_TFV exhibits low cytotoxicity in various human cell types comariosn with other NRTI_Antiviral Res_2002
Inhibition of cell proliferation Effects on viability
TDF with low cytotoxicity in proximal tubule epithelial cells

Does TDF have nephrotoxic effect?
• in vitro study – TDF is a weak inhibitor of mamalian DNA
polymerases• Has not decreased mtDNA levels • Shows low cytotoxicity
• Epidemiologic study…

Epidemiology
• Phase I/II – Barditch-Crovo P et al, Antimicrob Agents Chemother. 2001– The Johns Hopkins University School of Medicine– N = 49– Tenofovir: 75mg, 150 mg, 300 mg, or 600 mg– No renal abnormalities at 28 days
• Phase II – Schooley, et al, AIDS. 2002– University of Colorado– RCT– N = 181– Tenofovir: 75mg, 150 mg, or 300 mg– No renal abnormalities after 48 weeks

Clinical TrialsGilead-Sponsored Clinical Studies of TDF
Naive
Exp.
Exp.
Naive
Tx-
Week 24517TDF/FTC vs. CBVGS934
Week 48 550TDF vs. PlaceboGS907
TDF vs. Placebo
TDF vs. d4T
Comparison
1853
186
600
N
Week 48*GS902
Results AvailableStudy
Week 144GS903
TOTAL
Naive
Exp.
Exp.
Naive
Tx-
Week 24517TDF/FTC vs. CBVGS934
Week 48 550TDF vs. PlaceboGS907
TDF vs. Placebo
TDF vs. d4T
Comparison
1853
186
600
N
Week 48*GS902
Results AvailableStudy
Week 144GS903
TOTAL
In all of these studies the rates of renal abnormalities were similar between TDF and control arms.
Clinical Trial
• Multicenter, RCT
• FU of 144 weeks
TDF + 3TC + EFV vs. d4T + 3TC + EFV

GS903
Izzedine-Deray_Long-term renal safety of TFV_NephDialTranp_2005

GS903Incidences of elevated serum creatinine and hypophosphatemia
Izzedine-Deray_Long-term renal safety of TFV_NephDialTranp_2005
(-0.2) (-0.1)

GS903Calculated Creatinine Clearance Through Week 144
Izzedine-Deray_Long-term renal safety of TFV_NephDialTranp_2005
Conclusion:
-Renal safety profile between 2 groups was similar
-Incidence of renal failure and hypophosphatemia were reversible
-No patient developed Fanconi syndrome

Conclusion from Clinical Trial
• Double-blind, placebo-controlled studies– No difference in incidence of renal events
between TDF and placebo groups
• No TDF-related toxic side effects were noted in the recommended drug combination regimes of TDF
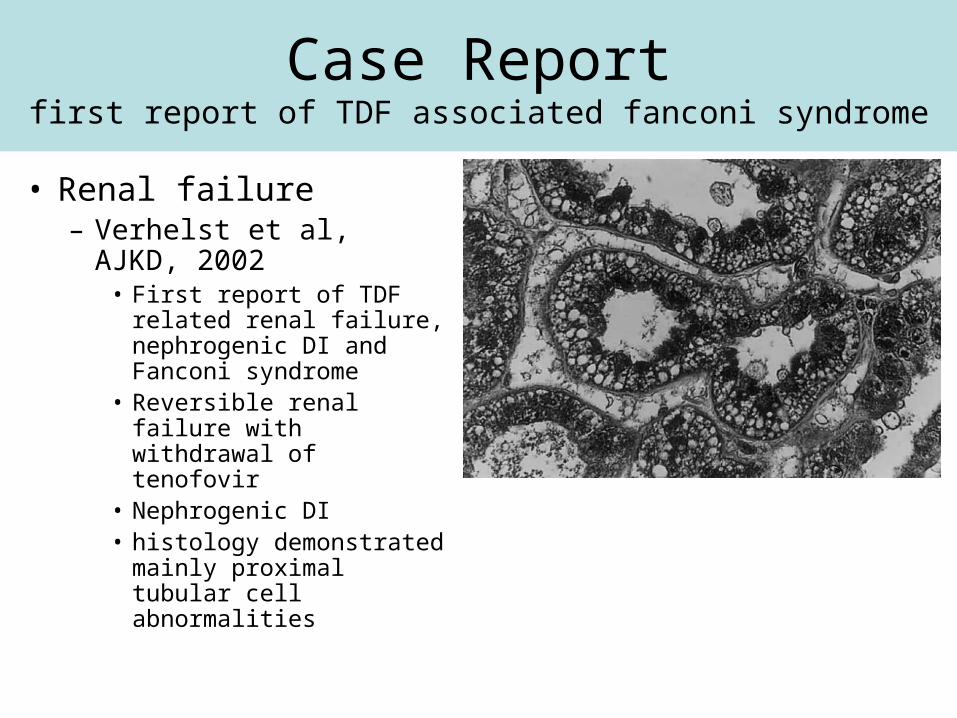
Case Reportfirst report of TDF associated fanconi syndrome
• Renal failure– Verhelst et al, AJKD,
2002• First report of TDF
related renal failure, nephrogenic DI and Fanconi syndrome
• Reversible renal failure with withdrawal of tenofovir
• Nephrogenic DI• histology demonstrated
mainly proximal tubular cell abnormalities

Fanconi Syndrome
GlucosePhosphateBicarbonateSodiumAmino Acids
Hypophosphatemia, acidosis, glycosuria, aminoaciduria, hypokalemia = FANCONI SYNDROME
XX
X
Phosphate
Proximal Tubule Cell

• Literature search for published case reports of TDF related ARF
• 1990 - 2005

Tenofovir- associated Renal Dysfunction literature review
Characteristic N=27
Age; years 45.5 (31 – 65)
Concurrent ARV; n(%)
Ritonavir
Didanosine
21 (77)
9 (33)
Time to diagnosis; months 11.3 (1 – 29)
Diabetes insipidus; n (%) 5 (18)
Zimmermann-Braden_TFD associated acute and ckd, HIV / AIDS, 2006

Characteristic (N=27)
Baseline creatinine; mg/dL 0.9 (0.5 – 2.1)
Peak creatinine; mg/dL 3.9 (0.89 – 20) P < .05
Post creatinine; mg/dL 1.2 (0.67 – 2.6) P < .05
Fanconi Syndrome; n (%) 16 (59)
Return to baseline creatinine; n (%) 22 (81)
Urine protein; n (%) 6/17 (35)
Hemodialysis; n (%) 2 (7)
Mean (range) unless otherwise specified
Tenofovir- associated Renal Dysfunction literature review
Zimmermann-Braden_TFD associated acute and ckd, HIV / AIDS, 2006

Tenofovir-induced Fanconi syndromeliterature review
• Other features– Acidosis, Hypokalemia– When checked TDF levels were elevated
• In all cases acidosis, hypokalemia, hypophosphatemia and glycosuria resolved after discontinuation of TDF
• Biopsy findings (8)– Proximal acute tubular necrosis (ATN)

Tenofovir-induced Fanconi syndrome
• Retrospective review of the FDA Adverse Event Reporting System
• 2001-2006

Gupta_Tenofovir associated fanconi_AIDS pt care_2008
Conclusion from case reports
• Potential role of drug interactions– Ritonavir
• has been shown to increase serum TDF by >30%• Inhibitor of MRP-2 -> increase proximal tubular concentration
of TDF by decreasing secretion
– Didanosine• Coadministration with TDF may increase serum
concentration of didanosine -> proximal tubular dysunfction
• Polymorphism in the renal tublar drug transporter– variant MRP 2 or 4

The End


















