NBR 18801 - Sistema de Gestao Da Seguranca e Saude No Trabalho - Requisitos

Neuroradiology/Pictorial Essay
Rev. Argent. Radiol. 2013;77(4):275-283 275
Introduction
The objective of this pictorial essay is to describe and provide examples of intracranial imaging findings of tuberous sclero-sis (TS) extracted from our case series.Tuberous sclerosis is a neurocutaneous syndrome formerly described by Bourneville in 18801 (also known as Bournev-ille disease). This entity is an inherited autosomal dominant disease caused by mutation or deletion of two genes: one on chromosome 9, known as TSC1, and the other one on chromosome 16, known as TSC22.This neurocutaneous disease is characterized by the presence of a clinical triad (Vogt triad) of mental retardation, seizures and skin lesions (sebaceous adenoma, also called facial an-giofibroma). All three signs are present in 30% of the cases.Diagnosis of the tuberous sclerosis complex (TSC) is made on the basis of clinical features, using major and minor diag-nostic criteria3 (table 1). Based on these parameters, clinical diagnosis is considered to be:• Definite: when either two major criteria or one major crite-
rion with two minor criteria are met.• Probable: when one major criterion and one minor crite-
rion are met.• Possible: when wither 1 major criterion or two or more mi-
nor criteria are met.In our study, only intracranial findings are detailed.Within neurological signs and symptoms, seizures are the most common (82%). Seizures may be of any type except the so called petit mal (absence seizures).Mental retardation occurs in 48% of cases and it may be very severe, mainly in patients who had a very early seizure onset.
AbstractTuberous sclerosis is a neurocutaneous disease characterized by the clinical triad (Vogt triad) of mental retardation, seizures and skin lesions (sebaceous adenoma). It is also characterized by typical intracranial findings that lead to this diagnosis.The aim of this pictorial essay is to describe and provide examples of intracranial findings characteristic of tuberous sclerosis using images from our case series.Keywords: cortical tubers; subependymal hamartomas; intracranial lesions; neurocutaneous disease
Tuberous sclerosis: evaluation of intracranial lesionsJ. Docampo*, M. Cabrini, C. Bruno and C. Morales.
Fundación Científica del Sur, Lomas de Zamora, Province of Buenos Aires, ArgentinaReceived: May 2013; Accepted: September 2013.©SAR
Table 1: Diagnostic criteria for tuberous sclerosis3.
Major Criteria Age at onset
Facial angiofibroma Infancy to adulthoodUngual fibroma Adolescence to adulthoodShagreen patch InfancyHypomelanotic macule InfancyCortical tuber Fetal lifeSubependymal hamartoma Childhood to adolescenceSubependymal giant-cell astrocytoma Infancy to adolescenceRetinal hamartoma Infancy Cardiac rhabdomyoma Fetal lifeRenal angiomyolipoma Childhood to adulthoodLymphangiomyomatosis Adolescence to adulthood Minor criteria Multiple pits in dental enamel Hamartomatous rectal polyps Bone cysts Cerebral white-matter radial migration lines Gingival fibromas Retinal achromic patch “Confetti” skin lesions (groups of small, lightly pigmented spots) Multiple renal cysts

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
276 Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
There is a correlation between the number and volume of cortical tubers, the age of onset of seizures and the degree of mental retardation: the earlier cortical tubers develop the earlier seizures occur, hence, the greater degree of mental retardation. The number and anatomic location of cortical tubers may play an important role in the development of mental retardation4.However, some individuals with TS never had seizures and have a normal intelligence quotient. In addition, other neu-rological findings may occur, such as hyperactivity, behavioral abnormalities, autism and attention deficit.
Development
The main cerebral abnormality in TS is related to dysplastic stem cells, which give rise to dysplastic glia and neurons that are unable to differentiate, migrate or organize properly5.
Subependymal hamartomas
Subependymal hamartomas, also known as subependymal nodules, are small lesions which histologically consist of giant cells with features of neurons and astrocytes. These hamarto-
Figure 1 Axial CT scan of a one-year-old male patient that shows hyperdense, calcified small nodules of subependymal location, consistent with subependymal hamartomas and cortical hypodense images consistent with tubers.
Figure 2 MRI on axial T1-weighted sequence without contrast agent (a) and with gadolinium (b) in a 2-year-old male patient with a subependymal hamartoma that enhances after contrast administration (arrow).
a b

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
277
Figure 3 Axial MRI in a 7-year-old female patient. The scan shows a large, ovoid and solid intraventricular mass located on the right lateral ventricle. The mass is hyperintense on T2, isointense on T1 and is significantly enhanced after the administration of paramagnetic contrast agents. This image is consistent with a subependymal giant cell astrocytoma.
Figure 4 Cortical tubers. The axial T2-weighted image shows a hyperintense lesion on the left frontal subcortical white matter involving two adjacent gyri and called “sulcal island” (black arrow). The coronal T2-weighted image sows a hyperintense lesion located in the core of an expanded gyrus, called “gyral core” (white arrow).

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
278 Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
mas are located on the wall of the lateral ventricles and their appearance on computed tomography (CT) and magnetic resonance imaging (MRI) varies with the age of the patient. Their size is variable, but no greater than 10 mm in diameter.On CT scans, subependymal hamartomas are isodense to the white matter, but in older patients they may calcify and be-come hyperdense (fig. 1). Even if hamartomas calcify progres-
sively during the first two decades of life, a calcified nodule is hardly found in patients younger than 1 year of age. Regard-ing the location of hamartomas, they either protrude into the lateral ventricles or are “embedded” in the contour of the caudate nuclei, being bilateral in 95% of the cases.On MRI, subependymal hamartomas in newborns are slightly hyperintense on T1-weighted images compared with the
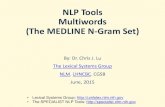
Figure 5 Parenchymal cyst. Cystic lesion, which is hyperintense on T2-weighted image (b) and hypointense on T1-weighted image (a) and FLAIR (c), located in the periventricular white matter, adjacent to the occipital prolongation of the right lateral ventricle (arrows).
Figure 6 White matter hamartomas. CT scan and MRI in a 2-year-old patient with a lesion in the white matter located on the left external capsule (arrows). CT scan shows a hyperdense lesion correlated with calcification, while on MRI, the lesion appears hypointense on T2-weighted imaging and hyperintense on T1-weighted imaging.

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
279
white matter and of heterogeneous intensity on T2-weighted images, due to the hypomyelination of the white matter. As myelination occurs, nodules become isointense to the white matter on T1- and T2-weighted images. If they calcify, they are markedly hypointense on gradient echo sequences (GRE). Post-contrast paramagnetic uptake is variable (fig. 2), with an absence of enhancement being more frequent1,2.
Subependymal astrocytomas
Subependymal giant cell astrocytomas are histologically be-nign tumors formed by giant cells which present features of astrocytes and neurons. The age of onset is between 8 and 18 years old, and their typical location is near the foramen of Monro. Subependymal astrocytomas may cause obstructive hydrocephaly.Compared with subependymal hamartomas, astrocytomas are larger and tend to grow slowly. Their diagnosis and fol-low-up are important, because if they grow and produce ob-structive hydrocephaly, neurosurgery may be required.On CT and MRI, subependymal astrocytomas are similar to subependymal hamartomas. Despite their larger size, they are usually enhanced by paramagnetic contrast agents, and they may calcify and bleed.Differential diagnosis with subependymal hamartomas is de-termined by the follow-up of their evolution, since subep-endymal astrocytomas grow whereas hamartomas do not1,2.Subependymal astrocytomas may also appear as large het-erogeneous intraventricular masses that enhance after intra-venous contrast administration (fig. 3).
Cortical tubers
Cortical tubers are benign hamartomatous lesions, which rarely become malignant. They may be single or multiple (more frequent) and they most commonly occur in the frontal lobes, followed by the parietal, occipital and temporal lobes (in decreasing order). Histologically they consist of bizarre giant cells, dense fibrillary gliosis and disorganized myelin sheaths.On CT scan, tubers appear hyperdense in newborns and in-fants, while adjacent subarachnoid spaces are usually wid-ened. However, they become hypodense throughout years and may also calcify.On MRI, in the first years of life cortical tubers appear slightly hyperintense on T1-weighted sequences with respect to the white matter, and hypointense on T2-weigthed images. As the brain myelinates, tubers become iso-hypointense on T1-weighted images and hyperintense on T2-weighted images.
Figure 7 Radial migration lines. FLAIR sequence shows a hy-perintense line extending towards the cortex (straight arrows) at the level of the periventricular white matter adjacent to the occipital prolongation of the left lateral ventricle. Parenchy-mal cysts (curved arrows) are also present. Both findings are characteristic of tuberous sclerosis.
Figure 8 White matter lesion. FLAIR sequence demonstrates a thick hyperintense band extending from the periventricular white matter to the cortex (arrows).
Figure 9 The gradient-echo image shows hypointense small nodules on the right lateral ventricle wall, corresponding to calcified subependymal hamartomas (arrows).

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
280 Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
FLAIR sequence has an enhanced sensitivity in the diagnosis of cortical tubers both in children and adults. Cortical tubers appear as hyperintense images of diffuse limits at the site where the lesions are located1,2. When tubers calcify, they often appear hypointense on GRE sequences and slightly hy-perintense on T1-weighted images.Some authors divide cortical tubers into two types (fig. 4): gy-ral core and sulcal island6-8. A gyral core appears hyperintense on T2-weighted images and hypointense on T1-weighted im-aged, located in the inner core of an expanded (widened) gyrus, with a cortex of normal thickness. Sulcal islands are lesions in which the subcortical white matter appears hyper-intense on T2-weighted images and iso-hypointense on T1-weighted images, involving two adjacent gyri. Their cortex is of normal thickness.Tubers may also occur in the cerebellum, with similar features as those seen in supratentorial tubers. Cerebellar tubers ap-pear hyperintense on T2-weighted images and iso-hypoin-tense on T1-weighted images. According to various series, these lesions occur in 10-24.1% of cases9.
Parenchymal cysts
Even if these lesions are ubiquitous in its location, they are mostly found in the periventricular white matter. The clinical significance of these lesions is unknown2.On CT scan, parenchymal cysts appear as round hypodense images. On MRI, they appear hyperintense on T2-weighted images and hypointense on T1-weighted images and FLAIR (fig. 5).
White matter hamartomas
These lesions are formed by giant cells that are 5 to 10 times larger than astrocytes with features of neurons and glial cells.White matter harmartomas are of variable size. While small lesions are punctiform, hyperintense on T2-weighted images and FLAIR, large lesions have various appearances: they can be linear, cuneiform or form a conglomerate. However, the most common appearance is a linear pattern extending from the periventricular region to the cortex, known as “radial mi-gration lines”.
Figure 10 (a) Axial T2-weighted image in a 1-year-old patient with subependymal hamartomas in both lateral ventricles (white arrows), and cortical tubers (circle). (b) On diffusion weighted imaging, subependymal hamartomas are isointense to the white matter (arrows), while on apparent diffusion coefficient, subependymal hamartomas are isointense or slightly hypointense to the white matter (arrows). This might be related to calcification of hamartomas. Cortical tubers are hyperintense on apparent diffusion coefficient (circle), with facilitated diffusion.
a b c

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
Rev. Argent. Radiol. 2013;77(4):275-283
J. Docampo et al.
281
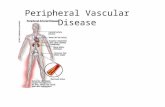
Figure 11 Monovoxel Spectroscopy with PRESS sequences, echo time 25ms; (a) normal side and (b) assessment of a cortical tuber, showing a decrease in the N-acetyl aspartate peak, an increase in the myo-inositol peak and a normal choline peak.
a
b

Rev. Argent. Radiol. 2013;77(4):275-283
Tuberous sclerosis: evaluation of intracranial lesions
282
On CT scan, these lesions are usually slightly hypodense and may also calcify (fig. 6), while on MRI they are hyperintense on T2-weighted images and FLAIR (figs. 7 and 8). They rarely enhance after contrast administration.Some authors report that these lesions are identical to trans-mantle cortical dysplasias10.
FLAIR and susceptibility-weighted imaging
In MRI, FLAIR and GRE sequences play a key role. On the one hand, the FLAIR sequence is more sensitive than T2-weighted imaging for the diagnosis of cortical tubers (which appear as hyperintense with diffuse borders at the subcortical level) and more accurate for identifying white matter lesions. GRE imag-ing is particularly helpful for diagnosing calcified lesions. Cal-cium appears as hypointense on GRE sequences, while on all other conventional sequences it may appear with various signal intensities or even be undetected. Nevertheless, new magnetic susceptibility sequences are currently available, known as sus-ceptibility weighted imaging (SWI) and susceptibility weighted angiographies (SWAN), which are more sensitive than echo gradient sequences for the detection of calcification.On GRE sequences, calcified subependymal hamartomas usually appear as hypointense small nodules along the walls of the lateral ventricles (fig. 9).
Magnetic resonance diffusion weighted imaging and spectroscopy
On diffusion weighted imaging (DWI), cortical tubers show an increase in the apparent diffusion coefficient (ADC), which reflects an expansion of the extracellular space and is due to the presence of astroglyosis and hypomyelination11. Subep-endymal hamartomas may, in turn, have changes in diffusion as a result of calcification. These lesions are generally isoin-tense to healthy parenchyma on DWI and ADC (fig. 10).As regards to the magnetic resonance spectroscopy findings in cortical tubers, there is no increase in choline (Cho) that might suggest increased mitosis; instead, there is a significant reduction in the N-actetyl aspartate/creatine (NAA/Cr) and NAA/(Cho+Cr) ratios at the expense of a decrease in NAA (fig. 11). The reduction in NAA is due to the fact that cells forming cortical tubers produce less NAA than neurons12.
An increase in myo-inositol has also been found in cortical tubers, which might be explained by the presence of gliosis or immature neurons13.Subependymal hamartomas cannot be assessed by spectros-copy because of their periventricular location, since the cere-brospinal fluid alters the spectrum.
Conclusion
We should be aware of and keep in mind the typical intracra-nial findings of tuberous sclerosis, since these constitute the major and minor diagnostic criteria for this disease.The most frequent intracranial findings are subependymal hamartomas and cortical tubers. We should also be aware of the fact that intraventricular giant cell astrocytomas may cause hydrocephaly and that these lesions are usually located near the foramen of Monro, causing its obstruction.
Conflicts of interest The authors declare no conflicts of interest.
References
1. Hart B, Depper M, Clericuzio C. Síndromes neurocutáneos. En: Orrison WW, editor. Neurorradiología. Madrid: Harcourt; 2001. p. 1732-49.
2. Barkovich AJ. Facomatosis. En: Barkovich AJ. Neuroimagenología pediátri-ca. Madrid: Marbán; 2001. p. 417-29.
3. Crino PB, Nathanson KL, Henske EP. The tuberous sclerosis complex. N Engl J Med. 2006;355:1345-56.
4. Shepherd CW, Houser OW, Gomez MR. MR fi ndings in tuberous sclerosis complex and correlation with seizure develop ment and mental impair-ment. AJNR Am J Neuroradiol. 1995;16:149-55.
5. Barkovich AJ, Gressens P, Evrard P. Formation, maturation, and disorders of brain neocortex. AJNR Am J Neuroradiol. 1992;13: 423-46.
6. Griffi ths PD, Martland TR. Tuberous sclerosis complex: the role of neuro-radiology. Neuropediatrics. 1997;28:244-52.
7. Nixon JR, Houser OW, Gómez MR, Okazaki H. Cerebral tuberous sclerosis: MR imaging. Radiology. 1989;170:869-73.
8. Takanashi J, Sugita K, Fujii K, Niimi H. MR evaluation of tuberous sclerosis: increased sensitivity with fl uid-attenuated inversion recovery and relation to severity of seizures and mental retardation. AJNR Am J Neuroradiol. 1995;16:1923-8.
9. Vaughn J, Hagiwara H, Katz J, Roth J, Devinsky O, Weiner H, Milla S. MRI characterization and longitudinal study of focal cerebellar lesions in a young tuberous sclerosis cohort. AJNR Am J Neuroradiol. 2013; 34:655-59.
10. Baron Y, Barkovich AJ. MR imaging of tuberous sclerosis in neonates and young infants. AJNR Am J Neuroradiol. 1999;20:907-16.
11. Fırat AK, Karakaş HM, Erdem G, Yakıncı C, Bıçak U. Diffusion weighted MR fi ndings of brain involvement in tuberous sclerosis. Diagn Interv Radiol. 2006;12:57-60.
12. Mukonoweshuro W, Wilkinson I, Griffi ths PD. Proton MR spectro scopy of cortical tubers in adults with tuberous sclerosis complex. AJNR Am J Neuroradiol. 2001;22:1920-5.
13. Baskin HJ Jr. The pathogenesis and imaging of the tuberous sclerosis com-plex. Pediatr Radiol. 2008;38:936-52.