Tuberculosis in Children
13
Tuberculosis In Children Dr. Ayesha Abdul Razzaq
-
Upload
mobin-ur-rehman-khan -
Category
Documents
-
view
23 -
download
1
description
specifics in pediatrics tuberculosis
Transcript of Tuberculosis in Children

Tuberculosis In Children
Dr. Ayesha Abdul Razzaq

Introduction And Epidemiology
• Tuberculosis is a multi-systemic infectious disease caused by Mycobacterium TB
• New cases reported worldwide are 4,452,860.• Among this 157,135 or 3.5% are children.• In areas where it is endemic, tuberculosis
remains a major, often unrecognized cause of disease and death among children.

Clinical Syndromes Associated with TB


Diagnostic Studies• MICROBIOLOGIC STUDIES
• Detection of M TB bacilliLight microscopy: ziehlnelson, kinyoun or giemsa stainsFluorescence microscopy: light emitting diode (e.g. Primo star iLED) and aura
mine stain.Uses: diagnosis of TB, monitoring of treatment response.High specificity.• Detection of M TB growthSolid medium: egg based ( e.g. lowenstein-jensen, ogawa), agar based ( e.g.
Middle brook 7H10 or 7H11) and thin or thick layer plated agar.Liquid medium: (e.g. Middle brook 7H9), fluorescent (e.g. MGIT960), colorimetric
(e.g. BacT/ALERT), microscopical (e.g. TB drug susceptibility test kit), radiometric (e.g. BACTEC 460), and manometric ( VersaTREK).
Uses: diagnosis of TB, species identification, DST, treatment response.Solid medium high specificity, Liquid medium both.

Diagnostic Studies
• Detection of mycobacterial antigensLipoarabinomannan, with assay in urine (e.g. Clearview TB ELISA
and determine TB-LAM Ag).Antigen MPB64, with immunochromatographic assay.Uses: diagnosis and species identificationHigh sensitivity and specificity in HIV• Detection of M TB DNAPositive or negative smear samples ( sputum, gastric aspirates
and others)Uses: diagnosis, species, DST, treatment response.Moderate sensitivity

Diagnostic Studies
• HISTOPATHOLOGICAL STUDIES• Tissue samples stained with hematoxylin and eosin or
papanicolaou stainUses: Diagnosis
• IMMUNE RESPONSE STUDIES• TST ( sensitivity 70 -80%)• IGRA [stimulation with M TB specific antigens e.g. ESAT plus CFP-
10 with or without TB 7.7, detection by ELISPOT assay (e.g. T-SPOT.TB), ELISA (e.g. QuantiFERON-TB Gold)]. Sensitivity 75-90%
Uses: Identification of infection• Antibody test: None

Diagnostic Studies
• BODY FLUID STUDIES• Adenosine deaminase with colorimetric method• Interferon-ɣ, on ELISA or ELISPOT assay.• Lysozyme (muramidase), identified with
turbidimetric method.Uses: Diagnosis, treatment response• Composite measures ( protein, glucose, lactate. or LDH)
• IMAGING STUDIES• Radiography, CT, MRI, ultrasonographyUses: Diagnosis and treatment response

Diagnosis And Classification

ManagementFirst Line
DrugsMode & Mechanism
of action Main adverse effects Daily dose mg/kg
(range);[maximum]
Isoniazid (INH) Bactericidal-Inhibits cell wall synthesis
Hepatitis; Peripheral neuropathy
10 (10-15) [300mg]
Rifampin (RMP)
Bactericidal & sterilizing-Inhibits RNA synthesis
Hepatitis; Orange discoloration of secretions; Drug-drug interactions
15 (10-20) [600mg]
Pyrazinamide(PZA)
Sterilizing- Disrupts energy metabolism
Hepatitis; Arthralgia 35 (30-40) [2000mg]
Ethambutol (EMB)
Bacteriostatic-Inhibits cell wall synthesis
Visual disturbance (acuity, colour vision)
20 (15-25) [1200mg]
Streptomycin (SM)
Bacteriostatic-Inhibits protein synthesis-Use not advised in children.
Oto- & nephro-toxic 17.5 (15-20) [1000mg]
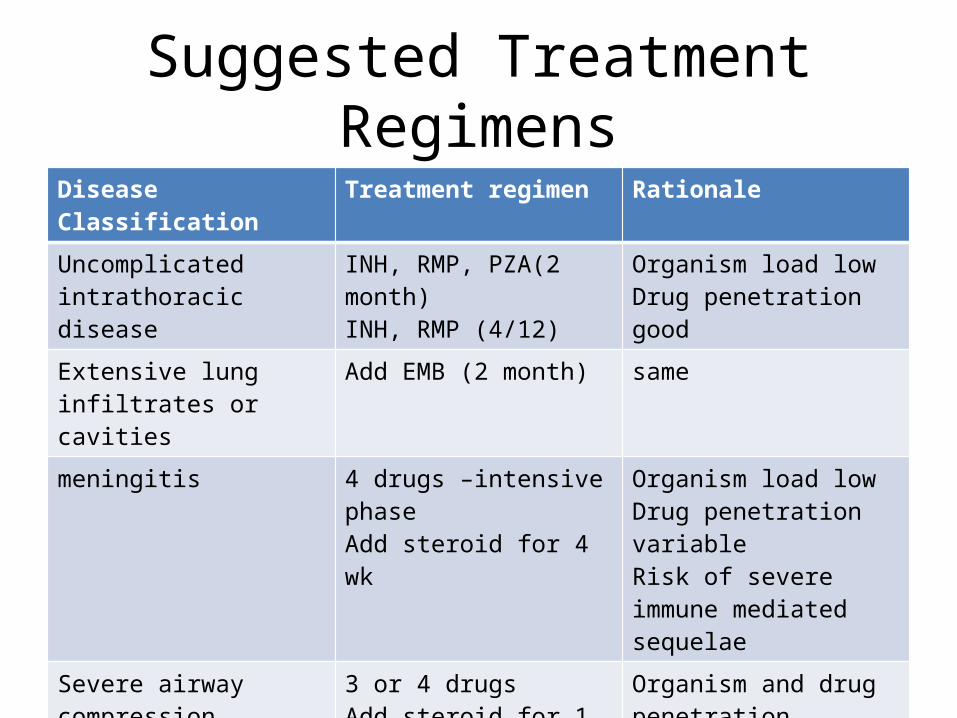
Suggested Treatment RegimensDisease Classification Treatment regimen Rationale
Uncomplicated intrathoracic disease
INH, RMP, PZA(2 month)INH, RMP (4/12)
Organism load lowDrug penetration good
Extensive lung infiltrates or cavities
Add EMB (2 month) same
meningitis 4 drugs –intensive phaseAdd steroid for 4 wk
Organism load lowDrug penetration variableRisk of severe immune mediated sequelae
Severe airway compression 3 or 4 drugsAdd steroid for 1 month
Organism and drug penetration variable,
Recent exposure/infectionNo active disease
INH (6-9 months)INH,RMP (3 months)
Organism load very lowDrug penetration good

Drug Resistant TB
• MDR TB: Resistance to INH and RIF.• EDR TB: MDR + resistance to a floroquinolone
and a second line injectable agent.• DR TB is seen in children expose to a person
with infectious DR TB and someone who died during treatment for TB or who is not adhering to therapy or someone who is undergoing re-treatment for TB.

Conclusion
• If case detection is improved and preventive therapy and curative treatment are made more accessible globally, the mortality and morbidity can be reduced.
THANK YOU!