
Triple-negative breast cancer: making the most of a misnomer
11
REVIEW ARTICLE Triple-negative breast cancer: making the most of a misnomerNicole MCCARTHY, 1 Gillian MITCHELL, 2 Michael BILOUS, 3 Nicholas WILCKEN 4 and Geoffrey J. LINDEMAN 5,6,7 1 Wesley Medical Centre, Brisbane, Queensland; 2 Peter MacCallum Cancer Centre, Melbourne, Victoria; 3 Healthscope Pathology, Norwest Private Hospital, Sydney, New South Wales; 4 Westmead Hospital, University of Sydney, Sydney, New South Wales; 5 The Walter and Eliza Hall Institute of Medical Research, 6 Royal Melbourne Hospital, and 7 University of Melbourne, Melbourne, Victoria, Australia Abstract Triple-negative breast cancer (TNBC) is defined by its lack of (or minimal) estrogen receptor and progest- erone receptor expression, together with the absence of human epidermal growth factor receptor 2 over- expression or gene amplification. It can be a particularly aggressive form of breast cancer, often characterized by early systemic relapse. This subtype, absent from traditional pathology classifications, has quietly crept into the oncologist’s lexicon over the last decade and aroused considerable research interest. Based on tumor pathology, immunohistochemistry and gene profiling studies, TNBC is likely to represent a heterogeneous mix of breast cancer subtypes. This observation will have important implications for the selection of optimal therapies, which are yet to be defined. This article reviews recent insights in the classification and ontogeny of TNBC, current approaches to its management and promising therapeutic targets that are forming the basis for innovative early and late phase clinical trials. Key words: basal-like, BRCA1, cell-of-origin, EGFR, luminal progenitor, PARP. INTRODUCTION Triple-negative breast cancer (TNBC), characterized by tumors that exhibit little or no estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) expression, can be a particularly aggressive form of breast cancer. These tumors are unlikely to respond to anti-estrogen therapy (using selective estrogen response modulators or aro- matase inhibitors) or HER2 antagonists. Patients with TNBC currently have no established treatment options other than chemotherapy. Gaining a better understand- ing of the processes that underpin breast tumorigenesis is an important step in developing new and effective targeted therapies. 1 This article consists of three parts; the first examines recent insights in the classification and ontogeny of TNBC, the second summarizes current knowledge and treatment approaches to TNBC and the third discusses recent developments that are informing future potential therapies. BREAST CANCER SUBTYPES: WORK IN PROGRESS A workable classification of breast cancer should be one that enables the stratification of tumor subtypes with similar molecular hard-wiring and biological behavior. For oncologists, this approach maximizes the ability to estimate patient prognosis and, importantly, to identify predictors of tumor response. This concept is of increas- ing relevance in the design of clinical trials investigating targeted therapies, where it is becoming perilous to ignore the heterogeneity of breast cancer and thereby include patients on study whose tumors fail to express the target. Correspondence: Professor Geoffrey Lindeman, BSc(Med), MBBS(Hons), FRACP, PhD. Stem Cells and Cancer Division, The Walter and Eliza Hall Institute of Medical Research, 1G Royal Parade, Parkville, Vic. 3052, Australia. Email: [email protected] Accepted for publication 20 January 2012. Asia–Pacific Journal of Clinical Oncology 2012; 8: 145–155 doi:10.1111/j.1743-7563.2012.01533.x © 2012 Blackwell Publishing Asia Pty Ltd
-
Upload
nicole-mccarthy -
Category
Documents
-
view
214 -
download
1
Transcript of Triple-negative breast cancer: making the most of a misnomer
REVIEW ARTICLE
Triple-negative breast cancer: making the mostof a misnomerajco_1533 145..155
Nicole MCCARTHY,1 Gillian MITCHELL,2 Michael BILOUS,3 Nicholas WILCKEN4 andGeoffrey J. LINDEMAN5,6,7
1Wesley Medical Centre, Brisbane, Queensland; 2Peter MacCallum Cancer Centre, Melbourne, Victoria; 3HealthscopePathology, Norwest Private Hospital, Sydney, New South Wales; 4Westmead Hospital, University of Sydney, Sydney, New SouthWales; 5The Walter and Eliza Hall Institute of Medical Research, 6Royal Melbourne Hospital, and 7University of Melbourne,Melbourne, Victoria, Australia
Abstract
Triple-negative breast cancer (TNBC) is defined by its lack of (or minimal) estrogen receptor and progest-erone receptor expression, together with the absence of human epidermal growth factor receptor 2 over-expression or gene amplification. It can be a particularly aggressive form of breast cancer, often characterizedby early systemic relapse. This subtype, absent from traditional pathology classifications, has quietly creptinto the oncologist’s lexicon over the last decade and aroused considerable research interest. Based on tumorpathology, immunohistochemistry and gene profiling studies, TNBC is likely to represent a heterogeneousmix of breast cancer subtypes. This observation will have important implications for the selection of optimaltherapies, which are yet to be defined. This article reviews recent insights in the classification and ontogenyof TNBC, current approaches to its management and promising therapeutic targets that are forming thebasis for innovative early and late phase clinical trials.
Key words: basal-like, BRCA1, cell-of-origin, EGFR, luminal progenitor, PARP.
INTRODUCTION
Triple-negative breast cancer (TNBC), characterizedby tumors that exhibit little or no estrogen receptor(ER), progesterone receptor (PR) and human epidermalgrowth factor receptor 2 (HER2) expression, can be aparticularly aggressive form of breast cancer. Thesetumors are unlikely to respond to anti-estrogen therapy(using selective estrogen response modulators or aro-matase inhibitors) or HER2 antagonists. Patients withTNBC currently have no established treatment optionsother than chemotherapy. Gaining a better understand-ing of the processes that underpin breast tumorigenesisis an important step in developing new and effective
targeted therapies.1 This article consists of three parts;the first examines recent insights in the classificationand ontogeny of TNBC, the second summarizes currentknowledge and treatment approaches to TNBC and thethird discusses recent developments that are informingfuture potential therapies.
BREAST CANCER SUBTYPES:WORK IN PROGRESS
A workable classification of breast cancer should be onethat enables the stratification of tumor subtypes withsimilar molecular hard-wiring and biological behavior.For oncologists, this approach maximizes the ability toestimate patient prognosis and, importantly, to identifypredictors of tumor response. This concept is of increas-ing relevance in the design of clinical trials investigatingtargeted therapies, where it is becoming perilous toignore the heterogeneity of breast cancer and therebyinclude patients on study whose tumors fail to expressthe target.
Correspondence: Professor Geoffrey Lindeman, BSc(Med),MBBS(Hons), FRACP, PhD. Stem Cells and Cancer Division,The Walter and Eliza Hall Institute of Medical Research, 1GRoyal Parade, Parkville, Vic. 3052, Australia.Email: [email protected]
Accepted for publication 20 January 2012.
bs_bs_banner
Asia–Pacific Journal of Clinical Oncology 2012; 8: 145–155 doi:10.1111/j.1743-7563.2012.01533.x
© 2012 Blackwell Publishing Asia Pty Ltd

Currently, breast cancer is simply defined using con-ventional histopathology accompanied by immunophe-notyping. To date, pathologists have described morethan 18 histological subtypes2 that can exhibit distinctand diverse clinical behavior. Immunophenotyping ismost often used to define ER, PR and HER2 expression.Increasingly, other markers, such as Ki-67 or geneexpression scores (such as Oncotype DX),3 are beingutilized as adjunct descriptors. In the last decade, geneexpression profiling has provided an important addi-tional framework for stratifying breast cancer, althoughits place in clinical practice is still being established.
Molecular classification of breast cancer
At least six distinct molecular subtypes have been iden-tified (luminal A and B, basal-like, claudin-low, HER2overexpressing and normal breast-like), each associatedwith distinct molecular features.4–6 The claudin-lowsubtype appears to be enriched for mesenchymal andstem cell features.7,8 Intriguingly, the gene expressionprofiles of several of various tumor subtypes is remark-ably similar to normal epithelial cell subtypes present inmammary tissue.9–11 These observations give rise to thepossibility that different subtypes of breast cancer maybe due to genetic mutations arising in distinct cells in thenormal breast epithelial hierarchy (Fig. 1). Alternatively,tumors could also undergo ‘reprogramming’ to resemble
distinct cellular subtypes.1,12 Moreover, several of thesebreast tumor molecular subtypes may manifest as triple-negative tumors. Importantly, most basal-like breasttumors exhibit a triple-negative phenotype, as outlinedbelow.
The term ‘basal-like’ was originally coined due to theperceived molecular similarity between these tumorsand basally located cells in normal breast epithelium.However, this term may be suboptimal13 as luminal pro-genitor cells also express certain basal markers such ascytokeratins (CK) 5/6. These rapidly dividing luminalcells, which are descendants of the multi-potent basalbreast stem cell, produce the mature ER-positive andER-negative luminal cells that line breast ducts. It nowseems likely that the luminal progenitor cell is a keytarget cell that gives rise to basal-like breast cancer.9 Thisobservation is based on the finding that luminal progeni-tor cell numbers are generally expanded and exhibitaberrant growth properties in pre-neoplastic tissue fromBRCA1 mutation carriers, who are prone to developingbasal-like tumors.10,11 Indeed, recent work using mousemodels has provided convincing evidence that luminalprogenitors are the cell of origin for BRCA1-associatedtumors.14,15
Mutations in the BRCA1 and BRCA2 genes arecharacterized by impaired DNA repair by homolo-gous recombination. Indeed, heterozygous germ-line
Figure 1 The molecular profiles ofdifferent breast cancer subtypes (listedright) show striking similarities todistinct epithelial cell types in normalbreast tissue.9–11 ER, estrogen recep-tor; lum, luminal; PR, progesteronereceptor.
146 N McCarthy et al.
© 2012 Blackwell Publishing Asia Pty Ltd Asia–Pac J Clin Oncol 2012; 8: 145–155
mutations are associated with up to an 85% lifetime riskof breast cancer.16 There is a well-established associationbetween BRCA1 and the development of TNBC,17 withrecently published data suggesting that BRCA1 silencingmay occur in up to 20% of sporadic TNBC.18 Thisassociation has important clinical implications, as theefficacy of some chemotherapeutics and targeted thera-pies will be influenced by the inactivation of DNA repairpathways that rely on BRCA1 function.19
TNBC – a heterogeneous grouping
TNBC comprises an assortment of histological subtypes.Most present as infiltrating ductal carcinomas not oth-erwise specified that are generally larger in size and ofhigher pathological grade at the time of diagnosis thanother breast cancer subtypes. This subtype accounts formost TNBC. Other less common subtypes that can alsocarry a poor prognosis include high-grade metaplasticcarcinomas, myoepithelial carcinomas or neuroendo-crine carcinomas. TBNC with a generally better prog-nosis include low-grade apocrine carcinomas, medullarycarcinomas, secretory carcinomas and adenoid cysticcarcinomas, as well as low-grade metaplastic carcino-mas.20 The identification of these pathologically distinctsubtypes has direct clinical relevance for the selection orsparing of patients from intensive systemic chemo-therapy. Recent gene expression profiling has identifiedsix TNBC subtypes that display unique profiles andontologies. These have been described as basal-like (BL1and BL2), an immunomodulatory (IM), a mesenchymal(M), a mesenchymal stem-like (MSL), and a luminalandrogen receptor (LAR) subtype, and provide potentialinsights that could inform the selection of therapy.21
Distinguishing features for
basal-like tumors?
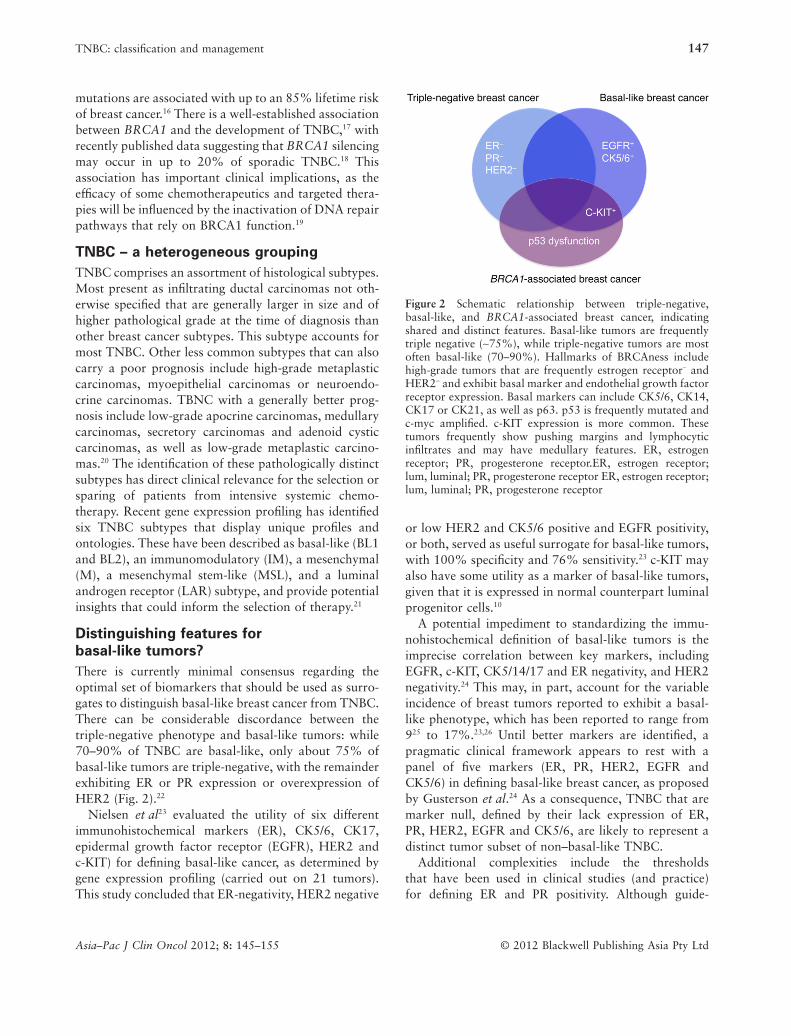
There is currently minimal consensus regarding theoptimal set of biomarkers that should be used as surro-gates to distinguish basal-like breast cancer from TNBC.There can be considerable discordance between thetriple-negative phenotype and basal-like tumors: while70–90% of TNBC are basal-like, only about 75% ofbasal-like tumors are triple-negative, with the remainderexhibiting ER or PR expression or overexpression ofHER2 (Fig. 2).22
Nielsen et al23 evaluated the utility of six differentimmunohistochemical markers (ER), CK5/6, CK17,epidermal growth factor receptor (EGFR), HER2 andc-KIT) for defining basal-like cancer, as determined bygene expression profiling (carried out on 21 tumors).This study concluded that ER-negativity, HER2 negative
or low HER2 and CK5/6 positive and EGFR positivity,or both, served as useful surrogate for basal-like tumors,with 100% specificity and 76% sensitivity.23 c-KIT mayalso have some utility as a marker of basal-like tumors,given that it is expressed in normal counterpart luminalprogenitor cells.10
A potential impediment to standardizing the immu-nohistochemical definition of basal-like tumors is theimprecise correlation between key markers, includingEGFR, c-KIT, CK5/14/17 and ER negativity, and HER2negativity.24 This may, in part, account for the variableincidence of breast tumors reported to exhibit a basal-like phenotype, which has been reported to range from925 to 17%.23,26 Until better markers are identified, apragmatic clinical framework appears to rest with apanel of five markers (ER, PR, HER2, EGFR andCK5/6) in defining basal-like breast cancer, as proposedby Gusterson et al.24 As a consequence, TNBC that aremarker null, defined by their lack expression of ER,PR, HER2, EGFR and CK5/6, are likely to represent adistinct tumor subset of non–basal-like TNBC.
Additional complexities include the thresholdsthat have been used in clinical studies (and practice)for defining ER and PR positivity. Although guide-
Figure 2 Schematic relationship between triple-negative,basal-like, and BRCA1-associated breast cancer, indicatingshared and distinct features. Basal-like tumors are frequentlytriple negative (~75%), while triple-negative tumors are mostoften basal-like (70–90%). Hallmarks of BRCAness includehigh-grade tumors that are frequently estrogen receptor- andHER2- and exhibit basal marker and endothelial growth factorreceptor expression. Basal markers can include CK5/6, CK14,CK17 or CK21, as well as p63. p53 is frequently mutated andc-myc amplified. c-KIT expression is more common. Thesetumors frequently show pushing margins and lymphocyticinfiltrates and may have medullary features. ER, estrogenreceptor; PR, progesterone receptor.ER, estrogen receptor;lum, luminal; PR, progesterone receptor ER, estrogen receptor;lum, luminal; PR, progesterone receptor
TNBC: classification and management 147
© 2012 Blackwell Publishing Asia Pty LtdAsia–Pac J Clin Oncol 2012; 8: 145–155

lines have been published to help standardizeimmunohistochemical reporting, various studies definethe hormone-receptor positivity range as �125–27 to�10%28,29 expression and HER2 overexpression thateither exceeds 1027,28 or 30%.25,26,29 Current recommen-dations by the American Society of Clinical Oncologyand the College of American Pathologists includereporting of �1% of tumor cell nuclei staining as beingER positive and PR positive, while uniform, intensemembrane staining of >30% of invasive tumor cells isrequired to diagnose HER2 overexpression.30 It is alsowell recognized that differences in sample fixation andlaboratory techniques can influence the reliability andreproducibility of immunohistochemical analysis.30,31
In addition, breast cancer specimens (particularly thoseexhibiting equivocal immunohistochemical staining)should routinely undergo further testing for HER2 geneamplification by fluorescence in situ hybridization, chro-mogenic in situ hybridization or silver-enhanced in situhybridization.30,32,33
In summary, TNBC defines a heterogeneous mix ofbreast tumors at multiple levels, which include diversetumor histology, imprecise marker characterization andcomplexities in establishing robust cut-offs for receptorexpression. This heterogeneity has the very real poten-tial to obscure important positive findings in clinicaltrials, particularly those based on targeting specificmolecular aberrations present in a subset of TNBC. Anumber of clinical trials are currently underway evalu-ating distinct molecular targets in TNBC, generallywithout patient stratification based on the tumorsubtype or expression of the molecular target. It is there-fore possible that that the power to elicit a tumorresponse will be diminished and that unplanned, retro-spective subset analysis may be required to gain insightsin tumor response and resistance.
CLINICAL CHARACTERISTICS OF TNBC
Epidemiology and risk factors
Overall, TNBC accounts for a minority (about 15%) ofall invasive breast cancers. Higher rates of TNBC thanother breast cancers have been reported in youngerwomen, women of African and Hispanic ethnicity andwomen in lower socioeconomic groups.34–36 Comparedwith luminal breast cancer, patients with basal-likebreast cancer (defined by immunohistochemistry) weremore likely to have a higher body mass index, waist-to-height ratio, experience menarche at a younger age,higher parity, younger age at first full-term pregnancyand shorter duration of breastfeeding.37 Parity, which
generally appears to provide long-term protectionagainst hormone receptor-positive breast cancer, maybe associated with a short-term increase in risk forTNBC.38 It has been suggested that the profound expan-sion of mammary stem cells during pregnancy couldaccount for this observation.39
Screening
Compared to other breast cancer subtypes, a lower pro-portion of TNBC is detected radiographically.28 Thetypical mammographic features of malignancy (irregularshape, speculated margins and calcifications) are lessfrequently observed in association with triple-negativetumors. By contrast, these tumors most often appearas circumscribed masses with indistinct margins andno associated micro-calcifications.40 These features aresuggestive of a more rapid rate of tumor growth and,consequently, alternative imaging modalities for thedetection of early TNBC, such as magnetic resonanceimaging, or more frequent screening schedules may berequired.40
Prognosis
In general, TNBC (infiltrating ductal carcinomasubtype) is associated with a poor prognosis andaccounts for a disproportionately high percentage ofbreast cancer deaths in the first 5 years following diag-nosis.28 These patients have a higher risk of earlyrelapse, which peaks 1–3 years post-diagnosis and thendrops quickly thereafter.28 Consequently, patients withTNBC are thought to be at no increased risk of deathfrom 5 years post-diagnosis and, according to the resultsof a pooled analysis of 12 studies and 10 159 patients,they may be at lower risk of death in the longer term(>10 years).41 TNBC is more likely to produce earlyvisceral metastases and is associated with a lower riskfor bone involvement.28
TREATMENT STRATEGIES FOR TNBC
There is no clear consensus regarding the optimal man-agement of TNBC. The limited available options, com-bined with generally poorer prognosis of this disease,have stimulated great interest in identifying novelmolecular markers that could serve as potential thera-peutic targets. A number of novel classes of drugs areunder investigation or clinical development. This hasheightened the importance of stratifying tumors of thebasis of expression of key markers, to ensure that tar-geted therapies will be applied to an appropriate patientcohort in clinical trials.
148 N McCarthy et al.
© 2012 Blackwell Publishing Asia Pty Ltd Asia–Pac J Clin Oncol 2012; 8: 145–155

Chemotherapy
At present, chemotherapy forms the mainstay of treat-ment with the use of many agents including alkylatingagents, anthracyclines, taxanes, platinum agents and theepothilone ixabepilone.42 However, as TNBC is a rela-tively newly defined subgroup of breast cancers, mostolder clinical trials do not differentiate between breastcancer in terms of ER, PR and HER2 status, are thereare relatively few data on optimal chemotherapy regi-mens. This is now an area of very active research, withover 40 chemotherapy trials in TNBC currently listed onthe US National Institutes of Health ClinicalTrials.govwebsite http://www.clinicaltrials.gov.
Commonly used treatment regimens includeanthracycline-based regimens such as fluorouracil,doxorubicin and cyclophosphamide; and fluorouracil,epirubicin, and cyclophosphamide. Anthracyclines mayalso be used in combination with taxanes; for example,docetaxel, doxorubicin, and cyclophosphamide; pacli-taxel, doxorubicin, and cyclophosphamide. A numberof studies (in most instances with small patient numbers)have been retrospectively evaluated to gain an under-standing of the merits and limitations of anthracyclinesand taxanes in TNBC.43 In general, it seems that anthra-cyclines may be superior to cyclophosphamide, methotr-exate and fluorouracil,44,45 and that there is additionalbenefit for the taxanes in the adjuvant setting.46,47 Anewer agent, ixabepilone, has shown evidence foractivity,48–52 but its relative efficacy compared to otherregimens is not known.
One difficulty in evaluating benefit is the paradoxicalobservation that in-breast complete response rates(pCR) can be quite high in neoadjuvant chemotherapystudies, even though this subtype has a far shorterdisease free and overall survival (OS) than other sub-types.43,53 This so-called ‘triple-negative paradox’ isthought to be driven by higher relapse rates among thosepatients whose tumors are not completely eradicated bychemotherapy.19 In this setting, residual risk for recur-rence and disease progression chemotherapy remainshigh.42
Emerging evidence also supports the explorationof platinum-salt therapy, a treatment that potentiallyexploits the link between TNBC and BRCA1 dysfunc-tion. These agents generate intra- and inter-strand cross-links, leading to double strand breaks. In cells that lackthe capacity for high fidelity double strand DNA breakrepair using homologous recombination, this couldprovide a therapeutic advantage. Most studies have beensmall or contained asymmetric comparator arms. A
single-center neoadjuvant study demonstrated higherpCR with platinum-based neoadjuvant chemotherapyfor TNBC than for non-TNBC; however, OS wasworse.54 Another phase III study showed a borderlineadvantage to adding cisplatin to epirubicin in metastaticdisease.55 One study that has received recent attention isa phase II neoadjuvant study of 28 patients with TNBCwho received cisplatin.56 Six of these patients achieved apCR, two of whom harbored pathogenic BRCA1 muta-tions. Factors associated with a good pathologicalresponse included lower levels of tumor BRCA1 expres-sion and evidence for BRCA1 promoter methylation.These findings suggest a strong benefit for BRCA1mutation carriers and some potential benefit whereBRCA1 levels are diminished. However, the pCR ratefor non-BRCA1 patients of 15% approximated thereported response rates observed in another neoadju-vant study using a docetaxel containing regimen.57
Radiotherapy
There is emerging evidence to support a specialrelevance for radiotherapy in the treatment of TNBC.The rate of locoregional recurrence (as well as distantrecurrence) appears to be higher among this subtype.58,59
A single institution study recently suggested thatlocoregional recurrence rates were higher for womenwith T1-2N0 TNBC who underwent a modified radicalmastectomy without adjuvant radiotherapy comparedwith breast-conserving therapy.60 This intriguing obser-vation will require prospective investigation, particu-larly to determine whether molecular and biologicaltumor characteristics, including BRCA1 status, contrib-ute to differential outcomes in the TNBC subtype.61
Since existing management algorithms tend to focuson primary tumor size and lymph node status, furtherresearch will be required to incorporate additionalbiologically relevant parameters.
TARGETED APPROACHES TOTHERAPY FOR TNBC
There is currently great interest in identifying novelmolecular markers that could serve as potential thera-peutic targets in TNBC. A variety of genetic lesions orbiological pathways appear to be enriched in TNBC.These include the presence of mutation or loss ofBRCA1, p53, PTEN and the activation of the mamma-lian target of rapamycin (mTOR) or Notch pathways.There is also interest in targeting putative cancer stemcells, which to date have largely been defined on anoperational basis through enrichment for tumor
TNBC: classification and management 149
© 2012 Blackwell Publishing Asia Pty LtdAsia–Pac J Clin Oncol 2012; 8: 145–155

sphere formation, an epithelial–mesenchymal transitionphenotype or aldehyde dehydrogenase ALDH andCD44hiCD24- expression. Here, targeting signalingpathways that include interleukin (IL)-6, IL-8 or trans-forming growth factor (TGF)b, receptor tyrosine kinasessuch as EGFR, platelet-derived growth factor receptorPDGFR, vascular endothelial growth factor receptorVEGFR, and MET, intracellular kinases such as SRC,focal adhesion kinase FAK, extracellular signal-regulated kinases (ERK)1/2 and c-Jun N-terminal kinase(JNK1/2), are either undergoing preclinical investigationor clinical development. The search for these and othertargeted therapies has heightened the importance ofsub-stratifying tumors on the basis of the expression ofthese key markers to ensure that targeted therapies willbe applied to the appropriate patient cohort in clinicaltrials.
Poly-ADP-ribose polymerase
(PARP) inhibitors
The pathways used to repair DNA damage vary accord-ing to the type of lesion. Single-strand DNA breaks areusually repaired by base-excision repair, a process medi-ated by PARP1 and possibly PARP2, which are membersof a large family of polymerases. Double-strand DNAlesions are repaired by homologous recombination,mediated by the products of BRCA1 and BRCA2,62 aswell as non-homologous end-joining (NHEJ).
Inhibition of PARP1 renders the base-excision repairpathway ineffective, and the consequent accumulationof single-strand breaks is thought to predispose to theincreased formation of double-strand breaks. As therepair of double-strand breaks requires BRCA1, thera-peutic PARP1 inhibition should result in genomic insta-bility and the consequent death of cells with BRCA1dysfunction, as occurs with BRCA-associated breastcancer, with minimal toxicity to normal cells (Fig. 3).This process, whereby the impairment of either BRCA1or PARP1 results in cell survival, but the impairmentof both results in cell death, is referred to as syntheticlethality.16 More recent reports suggest that this is acomplex interaction and that synthetic lethality onlyoccurs if there is additional, PARP inhibitor-drivenactivation of non-homologous end-joining.63
As noted above, phenotypic similarities betweenTNBC and BRCA1-associated breast cancer suggest acommon etiology. It has been hypothesized that TNBCmay be associated with an acquired underlying defect inBRCA1 pathways that may confer susceptibility to PARPinhibition. Furthermore, as ionizing radiation and somechemotherapeutics act by inducing double-strand DNA
breaks, the concurrent inhibition of base-excision repaircould be expected to result in increased cytotoxicity.16,62
Recent PARP inhibitor studies have been reviewed byChionh et al.64 A phase I trial of oral agent olaparib,a PARP inhibitor, for BRCA-associated breast-cancerin 60 patients with advanced solid tumors (nine withbreast cancer, 22 with BRCA1 or BRCA2 mutation)identified 400 mg twice daily as the maximum tolerateddose.65 Durable objective anti-tumor activity was limitedto patients with BRCA-associated ovarian, breast orprostate cancer, although not all patients with BRCAmutation benefited. In a subsequent phase II trial,women with measurable, recurrent breast cancer asso-ciated with germ line BRCA1 or BRCA2 mutations weresequentially allocated to receive olaparib 400 mg twicedaily (n = 27; 13 with TNBC) or 100 mg twice daily(n = 27; 16 with TNBC). A superior objective responsewas observed in the 400 mg twice daily cohort (41 vs22%). Median progression-free survival (PFS) was 5.7and 3.8 months, respectively.66,67
PARP inhibitors have been tested in a phase I settingin metastatic TNBC.64 Olaparib in combination withweekly paclitaxel demonstrated impressive responserates; however, an acceptable dose intensity was notachieved due to neutropenia.68 Another agent, veliparib,is being evaluated in combination with cisplatin andvinorelbine in TNBC.69 This agent is also being testedwith metronomic cyclophosphamide in a randomized
Figure 3 Mechanism of action of poly-ADP-ribose poly-merase (PARP) inhibitors in tumor cells following exposureto DNA-damaging agents. BRCA-deficient cells treated withPARP inhibitors are subject to synthetic lethality as both thehomologous recombination and base excision repair pathwaysare inactivated.
150 N McCarthy et al.
© 2012 Blackwell Publishing Asia Pty Ltd Asia–Pac J Clin Oncol 2012; 8: 145–155

phase II study.70 A number of other phase II and IIIstudies of PARP inhibitors are recruiting or inprogress.64
EGFR inhibitors
TNBC is often associated with the overexpression ofEGFR, where it may be associated with worse disease-specific survival.71 EGFR inhibitors have so far demon-strated a limited clinical benefit in TNBC. For example,a phase II trial comparing cetuximab with and withoutcarboplatin in 102 women with metastatic TNBC dem-onstrating overall response rates of 18 and 6%, respec-tively.72 These results suggest that EGFR overexpressionalone may not automatically confer sensitivity to EGFRinhibitors. In lung cancer, EGFR amplification ratherthan overexpression predicts response to the EGFRinhibitors cetuximab73 and erlotinib.74 Further researchwill be needed to determine whether particular subsetsof TNBC are more sensitive to EGFR targeting.
Antiangiogenic agents
TNBC is associated with abnormal microvascularproliferation, a process that plays an important role inbreast cancer growth, invasion and metastasis. VEGFRand platelet derived growth factor PDGR, critical modu-lators of this process, are targeted by antiangiogenicagents such as bevacizumab and sunitinib. A phase IIItrial of 722 patients with metastatic breast cancer (233with TNBC) demonstrated that the addition of bevaci-zumab to paclitaxel chemotherapy prolonged medianPFS from 5.9 to 11.8 months (HR 0.60; P < 0.001) andwas associated with a higher 1-year survival rate (81.2vs. 73.4%, P = 0.01). However, median OS was unal-tered (26.7 vs. 25.2 months, respectively, HR 0.88;P = 0.16).75 Approval for bevacizumab in breast cancerhas since been withdrawn in the UK and the USA. It isnoteworthy, however, that a subset analysis revealedthat in patients with ER-negative and PR-negativedisease, PFS increased from 4.6 to 8.8 months (HR 0.53;95% CI 0.40–0.70). Whether this agent has selectiveactivity in a subset of TNBC remains to be tested;however, the role of bevacizumab has been tested in theadjuvant setting in the BEATRICE trial which is nowclosed and the results are pending.76
A phase II trial demonstrated that sunitinib, a multi-targeted tyrosine kinase inhibitor, confers a responserate of 11% in women with metastatic breast cancer anda response rate of 15% in women with TNBC.77 Furtherclinical trials investigating the role of sunitinib and othertyrosine kinase inhibitors are underway.
Other novel investigational agents
Iniparib was originally classified as a PARP inhibitorand entered clinical trials as a PARP inhibitor, withinitial results demonstrating its efficacy in metastaticTNBC. However, more recent preclinical and clinicalinvestigations did not demonstrate the pharmacologicaland clinical characteristics previously reported for otherPARP inhibitors such as oliparib or veliparib, and itspotency as a PARP inhibitor has been questioned. It isnow recognized that iniparib induces gamma-H2AX (amarker of DNA damage) and cell cycle arrest in G2/Min tumor cell lines, where it may potentiate the effectof DNA damaging agents78–80 However, the precisemolecular mechanism accounting for these observationsremains to be determined.
Preclinical studies revealed that iniparib had anti-proliferative activity in TNBC cell lines, where it poten-tiated the activity of gemcitabine and carboplatin. Initialclinical trials demonstrated that iniparib was well toler-ated alone and in combination with standard chemo-therapy.81 A phase II trial of 120 women with TNBCfound that the addition of iniparib to gemcitabine/carboplatin therapy prolonged median OS by4.6 months (12.3 vs. 7.7 months for gemcitabine/carboplatin therapy with and without iniparib, respec-tively, P = 0.014).82 The combination was more effectivethan gemcitabine/carboplatin alone in terms of overallresponse rate (52.5 vs. 32.3%; P = 0.023), clinicalbenefit rate (55.7 vs. 33.9%; P = 0.015) and median PFS(5.9 vs. 3.6 months; P = 0.012), without incrementaltoxicity.
Based on these promising findings, a phase III multi-center comparative trial of gemcitabine/carboplatin withand without iniparib in women with metastatic TNBCwas undertaken.83 The primary purpose of this clinicaltrial was to determine the effect on OS and PFS by theaddition of iniparib to the combination of gemcitabineand carboplatin.84 The study demonstrated a safetyprofile that was consistent with that of the prior phaseII study.82 However, the addition of iniparib togemcitabine/carboplatin did not meet the pre-specifiedcriteria for significance for co-primary end-points of OS(11.1 vs 11.8%; P = 0.28) and PFS (4.1 vs 5.1 months;P = 0.027) in patients with mTNBC. This outcomeunderscores the potential importance of precisely defin-ing the TNBC study group, as well as the target(presumably susceptibility to DNA damage) in futurestudies.
TNBC has recently been recognized to include alarge proportion of cases that exhibit PTEN loss and
TNBC: classification and management 151
© 2012 Blackwell Publishing Asia Pty LtdAsia–Pac J Clin Oncol 2012; 8: 145–155

mTOR activation, providing a rationale for investigat-ing mTOR inhibitors.85 Early results from in vitrostudies also suggest that mTOR inhibitors could sensi-tize a subset of TNBC cancers to EGFR inhibitors.86
BH3 mimetics represent a promising class of drugsthat may have relevance for TNBC and basal-like breastcancer.87 These target certain members of the pro-survival BCL-2 family, which are commonly overex-pressed in breast cancer.87,88 The oral agent navitoclax isshowing promise in certain lymphoid malignancies89 buthas yet to be evaluated in breast cancer.
CONCLUSION
TNBC belong to a heterogeneous subset of breastcancers that are frequently associated with a poorprognosis. Although a clinically convenient descriptor,TNBC can include tumors with diverse histological phe-notypes and molecular profiles as well as distinct clinicalbehavior and responses to therapy. A sensitive andspecific panel of immunohistochemical biomarkers isrequired to help define these various subtypes moreprecisely.
Currently, there is no consensus regarding the optimalmanagement of TNBC. Although chemotherapy iscurrently the mainstay of treatment; optimal treatmentregimens have yet to be established. There is someevidence to support the use of anthracycline-based ortaxane-based therapy, together with recent evidenceto support platinum-based therapy in the setting ofBRCA1-deficiency.
Novel classes of biological targeting agents that targetmolecular pathways implicated in certain TNBC arecurrently of tremendous research interest. Among agrowing list of promising agents, examples includePARP inhibitors, EGFR inhibitors and antiangiogenicagents. The successful clinical translation of these agentswill necessarily require the strategic selection of suitablestudy groups that takes account of the precise breasttumor subtype and presence of the tumor target.Increasingly, another prerequisite includes the prospec-tive collection and study of tumor (and other tissue)samples from clinical trial patients, to help fuel ourunderstanding of the mechanisms of tumor response orresistance.
ACKNOWLEDGMENTS
This review was written by the authors followinga workshop on TNBC, carried out with financialsupport from Sanofi-Australia. The authors thank Scius
Solutions for editorial assistance in the preparation ofthis manuscript; whose contribution was funded bySanofi-Australia. GJL is supported by a National Healthand Medical Research Council Research Fellowship(637307).
REFERENCES
1 Lindeman GJ, Visvader JE. Insights into the cell of origin inbreast cancer and breast cancer stem cells. Asia Pac J ClinOncol 2010; 6: 89–97.
2 WHO. Classification of Tumours Vol. 4. Pathology andGenetics Tumours of the Breast and Female GenitalOrgans, 3rd edn. IARC, Paris 2003.
3 Paik S, Shak S, Tang G et al. A multigene assay to predictrecurrence of tamoxifen-treated, node-negative breastcancer. N Engl J Med 2004; 351: 2817–26.
4 Sorlie T, Perou CM, Tibshirani R et al. Gene expressionpatterns of breast carcinomas distinguish tumor subclasseswith clinical implications. Proc Natl Acad Sci U S A 2001;98: 10869–74.
5 Perou CM, Sorlie T, Eisen MB et al. Molecular portraits ofhuman breast tumours. Nature 2000; 406: 747–52.
6 Sotiriou C, Neo SY, McShane LM et al. Breast cancerclassification and prognosis based on gene expression pro-files from a population-based study. Proc Natl Acad Sci US A 2003; 100: 10393–8.
7 Hennessy BT, Gonzalez-Angulo AM, Stemke-Hale Ket al. Characterization of a naturally occurring breastcancer subset enriched in epithelial-to-mesenchymal tran-sition and stem cell characteristics. Cancer Res 2009; 69:4116–24.
8 Prat A, Perou CM. Deconstructing the molecular portraitsof breast cancer. Mol Oncol 2011; 5: 5–23.
9 Visvader JE. Keeping abreast of the mammary epithelialhierarchy and breast tumorigenesis. Genes Dev 2009; 23:2563–77.
10 Lim E, Vaillant F, Wu D et al. Aberrant luminal progeni-tors as the candidate target population for basal tumordevelopment in BRCA1 mutation carriers. Nat Med 2009;15: 907–13.
11 Lim E, Wu D, Pal B et al. Transcriptome analyses of mouseand human mammary cell subpopulations reveal multipleconserved genes and pathways. Breast Cancer Res 2010;12: R12.
12 Visvader JE. Cells of origin in cancer. Nature 2011; 469:314–22.
13 Gusterson B. Do ‘basal-like’ breast cancers really exist?Nat Rev Cancer 2009; 9: 128–34.
14 Molyneux G, Geyer FC, Magnay FA et al. BRCA1 basal-like breast cancers originate from luminal epithelial pro-genitors and not from basal stem cells. Cell Stem Cell 2010;7: 403–17.
15 Lindeman GJ, Visvader JE. Cell fate takes a slug in BRCA1-associated breast cancer. Breast Cancer Res 2011; 13: 306.
152 N McCarthy et al.
© 2012 Blackwell Publishing Asia Pty Ltd Asia–Pac J Clin Oncol 2012; 8: 145–155

16 Ashworth A. A synthetic lethal therapeutic approach:poly(ADP) ribose polymerase inhibitors for the treatmentof cancers deficient in DNA double-strand break repair.J Clin Oncol 2008; 26: 3785–90.
17 Foulkes WD, Stefansson IM, Chappuis PO et al. GermlineBRCA1 mutations and a basal epithelial phenotype inbreast cancer. J Natl Cancer Inst 2003; 95: 1482–5.
18 Gonzalez-Angulo AM, Timms KM, Liu S et al. Incidenceand outcome of BRCA mutations in unselected patientswith triple receptor-negative breast cancer. Clin Cancer Res2011; 17: 1082–9.
19 Adamo B, Anders CK. Stratifying triple-negative breastcancer: which definition(s) to use? Breast Cancer Res 2011;13: 105.
20 Oakman C, Viale G, Di LA. Management of triple negativebreast cancer. Breast 2010; 19: 312–21.
21 Lehman BD, Bauer JA, Chen X. Identification of humantriple-negative breast cancer subtypes and preclinicalmodels for selection of targeted therapies. J Clin Invest2011; 121: 2750–67.
22 Bertucci F, Finetti P, Cervera N et al. How basal aretriple-negative breast cancers? Int J Cancer 2008; 123:236–40.
23 Nielsen TO, Hsu FD, Jensen K et al. Immunohistochemicaland clinical characterization of the basal-like subtype ofinvasive breast carcinoma. Clin Cancer Res 2004; 10:5367–74.
24 Gusterson BA, Ross DT, Heath VJ, Stein T. Basal cytoker-atins and their relationship to the cellular origin and func-tional classification of breast cancer. Breast Cancer Res2005; 7: 143–8.
25 Cheang MC, Voduc D, Bajdik C et al. Basal-like breastcancer defined by five biomarkers has superior prognosticvalue than triple-negative phenotype. Clin Cancer Res2008; 14: 1368–76.
26 Nofech-Mozes S, Trudeau M, Kahn HK et al. Patterns ofrecurrence in the basal and non-basal subtypes of triple-negative breast cancers. Breast Cancer Res Treat 2009;118: 131–7.
27 Colleoni M, Cole BF, Viale G et al. Classical cyclophos-phamide, methotrexate, and fluorouracil chemotherapy ismore effective in triple-negative, node-negative breastcancer: results from two randomized trials of adjuvantchemoendocrine therapy for node-negative breast cancer.J Clin Oncol 2010; 28: 2966–73.
28 Dent R, Trudeau M, Pritchard KI et al. Triple-negativebreast cancer: clinical features and patterns of recurrence.Clin Cancer Res 2007; 13: 4429–34.
29 Thike AA, Cheok PY, Jara-Lazaro AR, Tan B, Tan P, TanPH. Triple-negative breast cancer: clinicopathological char-acteristics and relationship with basal-like breast cancer.Mod Pathol 2010; 23: 123–33.
30 Wolff AC, Hammond ME, Schwartz JN et al. AmericanSociety of Clinical Oncology/College of American Patho-logists guideline recommendations for human epidermal
growth factor receptor 2 testing in breast cancer. ArchPathol Lab Med 2007; 131: 18–43.
31 Bloom K, Harrington D. Enhanced accuracy and reliabilityof HER2/neu immunohistochemical scoring using digitalmicroscopy. Am J Clin Pathol 2004; 121: 620–30.
32 Penault-Llorca F, Bilous M, Dowsett M et al. Emergingtechnologies for assessing HER2 amplification. Am J ClinPathol 2009; 132: 539–48.
33 Van der Vijver M, Bilous M, Hanna W et al. Chromogenicin situ hybridisation for the assessment of HER2 status inbreast cancer: an international validation ring study. BreastCancer Res 2007; 9: R68.
34 Carey LA, Perou CM, Livasy CA et al. Race, breast cancersubtypes, and survival in the Carolina Breast Cancer Study.JAMA 2006; 295: 2492–502.
35 Lara-Medina F, Perez-Sanchez V, Saavedra-Perez D et al.Triple-negative breast cancer in Hispanic patients: highprevalence, poor prognosis, and association with meno-pausal status, body mass index, and parity. Cancer 2011;117: 3658–69.
36 Kurian AW, Fish K, Shema SJ, Clarke CA. Lifetime risksof specific breast cancer subtypes among women in fourracial/ethnic groups. Breast Cancer Res 2010; 12: R99.
37 Millikan RC, Newman B, Tse CK et al. Epidemiology ofbasal-like breast cancer. Breast Cancer Res Treat 2008;109: 123–39.
38 Britt K, Ashworth A, Smalley M. Pregnancy and the riskof breast cancer. Endocr Relat Cancer 2007; 14: 907–33.
39 Asselin-Labat ML, Vaillant F, Sheridan JM et al. Controlof mammary stem cell function by steroid hormone signal-ling. Nature 2010; 465: 798–802.
40 Yang WT, Dryden M, Broglio K et al. Mammographicfeatures of triple receptor-negative primary breast cancersin young premenopausal women. Breast Cancer Res Treat2008; 111: 405–10.
41 Blows FM, Driver KE, Schmidt MK et al. Subtyping ofbreast cancer by immunohistochemistry to investigate arelationship between subtype and short and long term sur-vival: a collaborative analysis of data for 10,159 cases from12 studies. PLoS Med 2010; 7: e1000279.
42 Carey LA. Directed therapy of subtypes of triple-negativebreast cancer. Oncologist 2011; 16 (Suppl. 1): 71–8.
43 Hudis CA, Gianni L. Triple-negative breast cancer:an unmet medical need. Oncologist 2011; 16 (Suppl. 1):1–11.
44 Leo AD, Desmedt C, Bartlett JM et al. HER2 and TOP2Aas predictive markers for anthracycline-containing chemo-therapy regimens as adjuvant treatment of breast cancer: ameta-analysis of individual patient data. Lancet Oncol2011; 12: 1134–42.
45 Gluz O, Nitz UA, Harbeck N et al. Triple-negative high-risk breast cancer derives particular benefit from doseintensification of adjuvant chemotherapy: results of WSGAM-01 trial. Ann Oncol 2008; 19: 861–70.
TNBC: classification and management 153
© 2012 Blackwell Publishing Asia Pty LtdAsia–Pac J Clin Oncol 2012; 8: 145–155

46 Loesch D, Greco FA, Senzer NN et al. Phase III multicentertrial of doxorubicin plus cyclophosphamide followed bypaclitaxel compared with doxorubicin plus paclitaxelfollowed by weekly paclitaxel as adjuvant therapy forwomen with high-risk breast cancer. J Clin Oncol 2010;28: 2958–65.
47 Hugh J, Hanson J, Cheang MC et al. Breast cancer sub-types and response to docetaxel in node-positive breastcancer: use of an immunohistochemical definition in theBCIRG 001 trial. J Clin Oncol 2009; 27: 1168–76.
48 Rak Tkaczuk KH. Ixabepilone as monotherapy or in com-bination with capecitabine for the treatment of advancedbreast cancer. Breast Cancer 2011; 5: 1–14.
49 Ibrahim NK. Ixabepilone development across the breastcancer continuum: a paradigm shift. Cancer Manag Res2010; 2: 169–79.
50 Perez EA, Patel T, Moreno-Aspitia A. Efficacy of ixabepi-lone in ER/PR/HER2-negative (triple-negative) breastcancer. Breast Cancer Res Treat 2010; 121: 261–71.
51 Pivot XB, Li RK, Thomas ES et al. Activity of ixabepilonein oestrogen receptor-negative and oestrogen receptor-progesterone receptor-human epidermal growth factorreceptor 2-negative metastatic breast cancer. Eur J Cancer2009; 45: 2940–6.
52 Baselga J, Zambetti M, Llombart-Cussac A et al. Phase IIgenomics study of ixabepilone as neoadjuvant treatmentfor breast cancer. J Clin Oncol 2009; 27: 526–34.
53 Liedtke C, Mazouni C, Hess KR et al. Response to neoad-juvant therapy and long-term survival in patients withtriple-negative breast cancer. J Clin Oncol 2008; 26: 1275–81.
54 Sirohi B, Arnedos M, Popat S et al. Platinum-based chemo-therapy in triple-negative breast cancer. Ann Oncol 2008;19: 1847–52.
55 Nielsen D, Dombernowsky P, Larsen SK, Hansen OP,Skovsgaard T. Epirubicin or epirubicin and cisplatin asfirst-line therapy in advanced breast cancer. A phase IIIstudy. Cancer Chemother Pharmacol 2000; 46: 459–66.
56 Silver DP, Richardson AL, Eklund AC et al. Efficacyof neoadjuvant cisplatin in triple-negative breast cancer.J Clin Oncol 2010; 28: 1145–53.
57 Smith IC, Heys SD, Hutcheon AW et al. Neoadjuvantchemotherapy in breast cancer: significantly enhancedresponse with docetaxel. J Clin Oncol 2002; 20: 1456–66.
58 Meyers MO, Klauber-Demore N, Ollila DW et al. Impactof breast cancer molecular subtypes on locoregional recur-rence in patients treated with neoadjuvant chemotherapyfor locally advanced breast cancer. Ann Surg Oncol 2011;18: 2851–7.
59 Zaky SS, Lund M, May KA et al. The negative effect oftriple-negative breast cancer on outcome after breast-conserving therapy. Ann Surg Oncol 2011; 18: 2858–65.
60 Abdulkarim BS, Cuartero J, Hanson J, Deschenes J,Lesniak D, Sabri S. Increased risk of locoregional recur-rence for women with T1-2N0 triple-negative breast cancer
treated with modified radical mastectomy without adju-vant radiation therapy compared with breast-conservingtherapy. J Clin Oncol 2011; 29: 2852–8.
61 Trainer AH, James PA, Mann GB, Lindeman GJ. Breastconservation versus mastectomy in triple-negative breastcancer: two steps forward, one step back? J Clin Oncol2011; 29: 4722–3.
62 Comen EA, Robson M. Poly(ADP-ribose) polymeraseinhibitors in triple-negative breast cancer. Cancer J 2010;16: 48–52.
63 Patel AG, Sarkaria JN, Kaufmann SH. Nonhomologousend joining drives poly(ADP-ribose) polymerase (PARP)inhibitor lethality in homologous recombination-deficientcells. Proc Natl Acad Sci U S A 2011; 108: 3406–11.
64 Chionh F, Mitchell G, Lindeman GJ, Friedlander M, ScottCL. The role of poly adenosine diphosphate ribose poly-merase inhibitors in breast and ovarian cancer: currentstatus and future directions. Asia Pac J Clin Oncol 2011; 7:197–211.
65 Fong PC, Boss DS, Yap TA et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carri-ers. N Engl J Med 2009; 361: 123–34.
66 Tutt A, Robson M, Garber JE et al. Oral poly(ADP-ribose)polymerase inhibitor olaparib in patients with BRCA1 orBRCA2 mutations and advanced breast cancer: a proof-of-concept trial. Lancet 2010; 376: 235–44.
67 Chan SL, Mok T. PARP inhibition in BRCA-mutatedbreast and ovarian cancers. Lancet 2010; 376: 211–3.
68 Dent R, Lindeman GJ, Clemons M et al. Safety and efficacyof the oral PARP inhibitor olaparib (AZD2281) in combi-nation with paclitaxel for the first- or second-line treatmentof patients with metastatic triple-negative breast cancer:results from the safety cohort of a phase I/II multicentertrial. J Clin Oncol 2010; 28 (Suppl. 15): Abstract 1018.
69 NIH Clinical Trials. Study NCT01104259: veliparib,cisplatin, and vinorelbine ditartrate in treating patientswith recurrent and/or metastatic breast cancer. 2010[updated 5 January 2012; cited 27 February 2012].Available from: http://clinicaltrials.gov/ct2/show/record/NCT01104259.
70 NIH Clinical Trials. Study NCT01306032: ABT-888 withcyclophosphamide in refractory BRCA-positive ovarian,primary peritoneal or ovarian high-grade serous carci-noma, fallopian tube cancer, triple-negative breast cancer,and low-grade non-hodgkin’s lymphoma. 2011[updated13 January 2012; cited 27 February 2012]. Available from:http://clinicaltrials.gov/ct2/show/NCT01306032?term=NCT01306032&rank=1.
71 Liu D, He J, Yuan Z et al. EGFR expression correlates withdecreased disease-free survival in triple-negative breastcancer: a retrospective analysis based on a tissue microar-ray. Med Oncol 2011; doi:10.1007/s12032-011-9827-x[Epub ahead of print].
72 Carey LA, Rugo HS, Marcom PK et al. TBCRC001:EGFR inhibition with cetuximab added to carboplatin in
154 N McCarthy et al.
© 2012 Blackwell Publishing Asia Pty Ltd Asia–Pac J Clin Oncol 2012; 8: 145–155

metastatic triple-negative (basal-like) breast cancer. J ClinOncol 2008; 26 (Suppl. 15): Abstract 1009.
73 Hirsch FR, Herbst RS, Olsen C et al. Increased EGFR genecopy number detected by fluorescent in situ hybridizationpredicts outcome in non-small-cell lung cancer patientstreated with cetuximab and chemotherapy. J Clin Oncol2008; 26: 3351–7.
74 Tsao MS, Sakurada A, Cutz JC et al. Erlotinib in lungcancer – molecular and clinical predictors of outcome.N Engl J Med 2005; 14: 133–44.
75 Miller K, Wang M, Gralow J et al. Paclitaxel plus bevaci-zumab versus paclitaxel alone for metastatic breast cancer.N Engl J Med 2007; 357: 2666–76.
76 NIH Clinical Trials, NIH. Study NCT00528567.BEATRICE study: a study of avastin (bevacizumab)adjuvant therapy in triple negative breast cancer.2007 [updated 15 February 2012; cited 27 February2012]. Available from: http://clinicaltrials.gov/ct2/show/NCT00528567.
77 Burstein HJ, Elias AD, Rugo HS et al. Phase II study ofsunitinib malate, an oral multitargeted tyrosine kinaseinhibitor, in patients with metastatic breast cancer previ-ously treated with an anthracycline and a taxane. J ClinOncol 2008; 26: 1810–6.
78 Ossovskaya V, Lim CU, Schools G, Kalurupalle S,Roninson I, Broude E. Cell Cycle effects of iniparib, aPARP inhibitor, in combination with gemcitabine andcarboplatin in the MDA-MB-468(-) triple-negative breastcancer (TNBC) cell line. Cancer Res 2010; 70 (Suppl. 2):Abstract P5-06-09.
79 Ossovskaya V, Lim CU, Schools G, Kalurupalle S,Roninson I, Broude E. The chemosensitizing propertiesof iniparib in combination with DNA-damaging agentsin the MDA-MB-468(-) triple-negative breast cancer(TNBC) cell line. Cancer Res 2011; 71 (Suppl. 1): AbstractLB-401.
80 Ossovskaya V, Canino E, Giritharan G, Kim KA, Ilic D,Krtolica A. Targeting of induced cancer stem cells withiniparib in combination with carboplatin and gemcitabine.Cancer Res 2011; 71 (Suppl. 1): Abstract LB-386.
81 Mahany JJ, Lewis N, Heath EI et al. A phase IB studyevaluating BSI-201 in combination with chemotherapy insubjects with advanced solid tumors. J Clin Oncol 2008;26 (Suppl. 15): Abstract 3579.
82 O’Shaughnessy J, Osborne C, Pippen J et al. Final efficacyand safety results of a randomized phase II study of theparp inhibitor Iniparib (BSI-201) in combination withgemcitabine/Carboplatin (G/C) in metastatic triple negativebreast cancer (TNBC). Ann Oncol 2010; 21 (Suppl. 8):Abstract LBA-11.
83 NIH Clinical Trials, NIH. Study NCT00938652: a phase 3,multi-center study of gemcitabine/carboplatin, with orwithout BSI-201, in patients with ER-, PR-, and Her2-negative metastatic breast cancer. 2009 [updated 13 June2011; cited 27 February 2012]. Available from: http://clinicaltrials.gov/ct2/show/record/NCT00938652.
84 O’Shaughnessy J, Schwartzberg L, Dansi M et al.A randomized phase III study of iniparib (BSI-201) incombination with gemcitabine/carboplatin (G/C) in meta-static triple-negative breast cancer (TNBC). J Clin Oncol2011; 29 (Suppl.): Abstract 1007.
85 Berrada N, Delaloge S, Andre F. Treatment of triple-negative metastatic breast cancer: toward individualizedtargeted treatments or chemosensitization? Ann Oncol2010; 21 (Suppl. 7): vii30–35.
86 Liu T, Yacoub R, Taliaferro-Smith LD et al. Combinatorialeffects of lapatinib and rapamycin in triple-negative breastcancer cells. Mol Cancer Ther 2011; 10: 1460–9.
87 Oakes SR, Vaillant F, Lim E et al. Sensitization of BCL-2-expressing breast tumors to chemotherapy by the BH3mimetic ABT-737. Proc Natl Acad Sci U S A 2011; 109:2766–71.
88 Dawson SJ, Makretsov N, Blows FM et al. BCL2 in breastcancer: a favourable prognostic marker across molecularsubtypes and independent of adjuvant therapy received.Br J Cancer 2010; 103: 668–75.
89 Mason KD, Khaw SL, Rayeroux KC et al. The BH3mimetic compound, ABT-737, synergizes with a range ofcytotoxic chemotherapy agents in chronic lymphocyticleukemia. Leukemia 2009; 23: 2034–41.
TNBC: classification and management 155
© 2012 Blackwell Publishing Asia Pty LtdAsia–Pac J Clin Oncol 2012; 8: 145–155


















