
“It’s a ‘Tried and True’ Tuesday!” March 10, 2009 Mr. Houghteling.
Upload
truongkhuongCategory
view
216download
0
Travel Medicine Travel Medicine Tried, True and NewTried, True and New
Marc ShawMarc Shaw FRGS, FRGS, FRNZCGP, FRNZCGP, FFTM (ACTM), FFTM RCPS (FFTM (ACTM), FFTM RCPS (GlasGlas), ), DipTravMedDipTravMed
Associate Professor, James Cook University, Associate Professor, James Cook University, QldQld, Australia, Australia
Medical DirectorMedical DirectorWORLDWISE Travellers Health Centres, Auckland, NZWORLDWISE Travellers Health Centres, Auckland, NZ
WORLDWISEWORLDWISE OnLINE (OnLINE (worldwise.co.nzworldwise.co.nz))‘‘Travel Health Information for ProfessionalsTravel Health Information for Professionals’’

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
TravellersTravellers’’ Medicine and HealthMedicine and HealthTravel Medicine is THETHE new interdisciplinary field:
Traditional disciplinesTraditional disciplines→→ Travel related and can be applied toTravel related and can be applied to……•• epidemiologyepidemiology MalariaMalaria•• diagnosisdiagnosis SARSSARS•• managementmanagement Alt MedicineAlt Medicine•• prevention prevention RabiesRabies•• therapy/ self Rxtherapy/ self Rx Travellers DiarrhoeaTravellers Diarrhoea•• informatics informatics Emerging Infectious DiseasesEmerging Infectious Diseases
Goals of Travel Medicine:Goals of Travel Medicine:•• to protect travellers from disease and deathto protect travellers from disease and death•• to minimise impact of illness/ accidents by principles of self Rto minimise impact of illness/ accidents by principles of self Rx x •• to travel with consideration + respect to others and their landsto travel with consideration + respect to others and their lands•• to apply the same principles (travellersto apply the same principles (travellers’’ health) to all travellershealth) to all travellers

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
TravellersTravellers’’ Medicine and HealthMedicine and Health
• The ART of TRAVEL MEDICINE lies in the careful selection of necessary preventive strategies … avoiding those measures which may cause unnecessary fear, adverse events, untoward expense, or stressful inconvenience
• Only in exceptional circumstances should travel health recommendations be as restrictive as to ‘advise a traveller to abandon travel plans’
• The question we all need to ask is:
‘HOW can folk travel rather than SHOULD they’!

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Changing Times … Now
Now, the travel health issues of the day are:Now, the travel health issues of the day are:
•• 1. Disease Surveillance:1. Disease Surveillance:•• Is either Globally and Regionally focused Is either Globally and Regionally focused •• Surveys by Tracking DiseaseSurveys by Tracking Disease
WHO WHO CDCCDC Satellite imagerySatellite imagery•• Responds with frontline dealing OutbreaksResponds with frontline dealing Outbreaks
Singapore and Hong KongSingapore and Hong Kong
•• 2. Safety and Security: the Terrorism risk2. Safety and Security: the Terrorism risk•• Personal Security Personal Security •• Biosecurity Biosecurity
•• 3. The Traveller3. The Traveller•• Appropriateness of advice for type of travel: holiday, expeditioAppropriateness of advice for type of travel: holiday, expedition etcn etc•• Affect of the traveller on the host nations and vice versaAffect of the traveller on the host nations and vice versa•• The effect of Migrants and their travel to new regionsThe effect of Migrants and their travel to new regions

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Changing Times Changing Times …… NowNow
Now, the travel health issues of the day are:
•• 4. Environmental Travel4. Environmental Travel• Remote sports events• Media awareness of the Globe• Expeditions and adventure• Religious travellers
•• 5. Development of strategic alliances5. Development of strategic alliances• Working with corporate and travel companies• Working with Governments• Global ‘linkups’• Crisis management and emergency responders• Destination image and reputation promoters• Health tourism marketers – medical travel

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
VaccinesVaccines
Routine:Routine: childhood vaccines, updated vaccines
Recommended:Recommended: hepatitis A/B, typhoid …
Required: Required: yellow fever, cholera, meningitis …
Remote:Remote: rabies, Japanese encephalitis plague ...
Overview of Vaccines Overview of Vaccines –– an updatean update

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Disease Prevention Disease Prevention …… ‘‘Hot to trotHot to trot’’ ......
Decision on vaccinations• The ““Eclectic EightEclectic Eight”” shots for travel to devel. countries > 1/12
• Hepatitis A
• Hepatitis B
• Measles
• Spreads via airborne respiratory infections
• Typhoid
• Tetanus
• Spreads via soil contaminated with animal excreta
• Survives well in the tropics
• Diphtheria
• Spreads via airborne respiratory infections
• Diphtheria: in devel. countries and Areas of the Soviet Union
• Polio
• Faecal oral spread ( poor hygiene and sanitation )
• Rabies

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Recommended Recommended (for most travellers):(for most travellers):
Hepatitis A
Hepatitis B
Influenza
Pneumococcus
Typhoid
Travellers Diarrhoea ETEC
Travel VaccinationsTravel Vaccinations
Required Required (under certain circs):(under certain circs):
Yellow Fever
Polio
Cholera
Meningitis
Q‐fever
Remote or specialised:Remote or specialised:
Rabies
Japanese encephalitis
Tuberculosis
Tick borne encephalitis
Anthrax
Plague
Smallpox

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Snap TherapySnap Therapy…… the SIX pointer!the SIX pointer!
1. Alimentary Hygiene DOESAlimentary Hygiene DOES work but is not reality … too impractical for most travellers!
2. WHO recommend: WHO recommend: 1 1 teaspteasp salt+8 salt+8 teaspteasp sugar in 1 L potable H20sugar in 1 L potable H20
Food should be started as soon as the patient can eat
3. ORS OK because electrolytes/ sterility of mixtures, HOWEVER ORS had no influenceORS had no influence on symptoms, thus soups, juices etc
4. Wait ‘til get ongoing diarrhoeal symptomsget ongoing diarrhoeal symptoms b4 Rx
5. With TD parameters being met …
Loperamide + antibiotic combo. = illness few hrsLoperamide + antibiotic combo. = illness few hrs
6. IMMUNISATIONIMMUNISATION ag. ETEC good for 3 months ‐ 60% effective
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
MENINGITISMENINGITIS
•Widespread endemicity…
Meningitis belt of Sub‐Sahara
Meningococcal ACYW
Polysaccharide
4 strains in vaccine in NZ, AustNOT for type B
Non‐conjugated
Single dose vaccine Single dose vaccine ‐‐ NZ / NZ / AustAust brands: brands: MencevaxMencevax, , MenomuneMenomune …… lasts 2lasts 2‐‐3 yrs 3 yrs
Compulsory for annual pilgrimage of Muslims to Compulsory for annual pilgrimage of Muslims to HajHaj and and UmraUmra, Saudi Arabia, Saudi Arabia
No longer No longer ‘‘compulsorycompulsory’’ for travel to Nepal highlandsfor travel to Nepal highlands……

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Viral haemorrhagic disease• 200,000 / year and 30,000 deaths → liver failure AND multi‐organ collapse
• Virus similar to those of: dengue fever, JE, TBE, West Nile
• Virus is mosquito borne• Humans accidental hosts
• In forest pattern, monkeys are prime host, humans: accidental• Primary mosquito vector = Ae. africanus / bromeliae
• live in holes and cracks in upper parts of forest trees
• Incubation in Humans: 12‐21/7
• Legally vaccination is required for visas & borders
• Can only be given by Health Dept registered clinics
• Travellers must carry certificate of vaccination
• Single dose vaccine in NZ and Australia, Stamaril, and effective for 10 years+
• to be given in ages over 6‐9 mths ‐ confers immunity in > 95% vaccinees
• safe: 150 million doses/4 years and ~ 30 deaths
YELLOW FEVERYELLOW FEVERTravel disease reviewTravel disease review

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Individual Risk of Yellow FeverIndividual Risk of Yellow Fever
Africa: (highest risk July – Oct)
Risk of Yellow Fever Disease for 2 week stay:
1: 10,0001: 2,000Endemic areas
1: 13,0001: 250Epidemic (infected areas)
DeathIllnessYellow fever disease Activity

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Individual Risk of Yellow FeverIndividual Risk of Yellow Fever
South America: (highest risk Jan‐Mar)
Risk of Yellow Fever Disease for 2 week stay:
(10 times lower risk than Africa )
1: 100,0001: 20,000Endemic areas)
1: 13,0001: 2,500Epidemic (infected areas)
DeathIllnessYellow fever disease Activity
Practic
al
Practic
al Punc
hpoint
Punchp
oint
Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
RABIESRABIES
ENCOUNTERS WITH ANIMALS: PROBLEMS FOR TRAVELLERS!
RABIES IS PRESENT WORLDWIDERABIES IS PRESENT WORLDWIDE except in:• UK, Switzerland, Norway, Malta, Japan, Oceania, ‘Australia’, NZ
Rabies is 100% fatal if untreatedRabies is 100% fatal if untreated• 50,000+ year die from the disease … 30,000 in India, ??? In Africa • Transmitted via broken skin and the bite of infected animal ( esp. dogs )• 80% caused by dogs … in Bangkok, 5‐8% dogs have rabies
• ALL bites or licks should be considered as possible exposure
• Once bitten, then– clean wound with soap – apply povidone‐iodine– get to clinic to start vaccinations: initiated within 48 hours
Travel disease reviewTravel disease review

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
WORLDWISE STUDY OF 54 TRAVELLERS WORLDWISE STUDY OF 54 TRAVELLERS
Geographical region where exposure occurred:Geographical region where exposure occurred:South East Asia:South East Asia: 45 (83.3%)45 (83.3%)
Thailand: 19 (35.2%)Thailand: 19 (35.2%)India: 10 (18.5%)India: 10 (18.5%)Vietnam: 4 (7.4%)Vietnam: 4 (7.4%)Indonesia: 3 (5.6%)Indonesia: 3 (5.6%)
Central/South America:Central/South America: 5 (9.3%)5 (9.3%)Peru: 3 (5.6%)Peru: 3 (5.6%)Ecuador: 1(1.9%)Ecuador: 1(1.9%)
Africa: Africa: 3 (5.6%)3 (5.6%)Zimbabwe: 1(1.9%)Zimbabwe: 1(1.9%)Kenya: 1(1.9%)Kenya: 1(1.9%)
USA:USA: 1(1.9%)1(1.9%)
Mexican Free tailed batMexican Free tailed bat
RABIESRABIES
There was an adult to child ratio 5:1
The highest exposure risk group was in those aged 16‐30 years
Dogs = commonest animals – 2/3 of incidents.
Commonest sites animal exposure to body = thigh/lower leg (48.1%), and the hand (18.5%).

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
PrePre‐‐exposure exposure Vaccination (NZ and Australia):Cell derived Vaccine is inactivated‐virus vaccineHDCV ( human )
3‐dose series IM or WHO sanctioned IDDays 0, 7, and 21 or 28
Who Should Consider PreWho Should Consider Pre‐‐exposure Vaccination?exposure Vaccination?
1. Travel to endemic countries >30 days1. Travel to endemic countries >30 days in rural rabies area Mainly Asia (except Taiwan and Japan), Africa, Latin America.
2. At risk occupations2. At risk occupations,, avocations or activities, e.g. hunters, forest rangers, laboratory workers, spelunkers (!) …etc
RABIESRABIES

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
JAPANESE ENCEPHALITISJAPANESE ENCEPHALITIS
•• Rate of the disease for travellers: 1/1,000,000Rate of the disease for travellers: 1/1,000,000
•• Fatality rate of JE is 20Fatality rate of JE is 20‐‐30% ...30% ...
•• Est average ... 1/300 JEV infections = symptEst average ... 1/300 JEV infections = sympt
• About 50,000 cases annually in Asia
• In areas where JE is endemic annual incidence ranges from 1‐10 per 10,000 population Asia
• Mainly affects children under 15 years in endemic areas, with nearly universal exposure by adulthood, with about 10% of susceptible population infected per year (Asia)
•• Low risk disease for travellersLow risk disease for travellers
•• Of those that survive ...Of those that survive ... 2525‐‐40% serious neurol. Sequelae40% serious neurol. Sequelae
•• Majority infections are subclinicalMajority infections are subclinical
Travel disease reviewTravel disease review

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
JAPANESE ENCEPHALITIS
• CDC estimate risk for travellers spending time in rural destinations during the season of risk as bet. 1 case /5000/week to 1 case /20,000/week
• Risk for individual travellers is highly variable, principle factors contributing to risk in Asia are:
• Travel during the transmission season
• Exposure in rural areas, especially for extended periods
• Childhood and age >50 years more at risk for developing symptomatic illness after infection
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
TUBERCULOSIS
• 1 in 3 affected
• No really effective vaccine
• 50% adults
• 70% children• Extra‐pulmonary
• Mantoux 2‐step• 2 tests a week apart
• CXR … if indicated
Travel disease reviewTravel disease review

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Signs and Symptoms:• incubation 3 ‐ 14/7, av. 4 ‐ 7/7
• acute febrile period ( day 2‐10 ) infective
• Severe flu’‐like: infants & children beware!
• Temperature, Rash, Pain!
• Sudden‐onset fever, headaches, breakbone, URTI, rashes (recurring ),
pruritus /desquamation, taste changes, Photophobia
• Haemorrhagic signs: petechiae, bleeding gums, epistaxis,
GI haemorrhage, menorrhagia.
• LAB: neutropenia, lymphcytosis, inc. LFTs, thrombocytopenia
DENGUE FEVER

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Prevention:
• understanding behaviour. and feeding of vector mosquito
• Aedes indoors during the daytime … plants, containers
• knowing peaks of biting times (either side of dusk and dawn)
• screening/air‐conditioning
• spray rooms with insecticides
• DEET
• PERMETHRIN
DENGUE FEVER DENGUE FEVER –– Management for TravellersManagement for Travellers
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Arboviral, in the family Togaviridae, and
transmitted to humans by the bite of infected
Aedes and Culexmosquitoes including the
daytime‐biting Aedes aegypti and Ae. albopictus species.
The disease is similar to Dengue Fever: NO VACCINE
• CF first isolated from blood of febrile patient in Tanzania 1953
• Since identified in west, central and southern Africa and many areas of Asia
• 2006 ‐ there WERE significant reported outbreaks on the Indian Ocean islands of Madagascar, Mayotte, Mauritius, Réunion, and the Seychelles
• Chikungunya Fever outbreak currently significantly reported in India and Indonesia
Transmission thought to occur mainly between mosquitoes and monkeys
Travel disease reviewTravel disease reviewCHIKUNGUNYA FEVERCHIKUNGUNYA FEVER
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Management is supportive: bed rest, fluids, and mild
pain meds: paracetamol/ibuprofen to relieve sympts
The disease ‘invariably’ follows a benign course,
with few cases severe enough to require hospital admission
Prevention of CF – as FOR DENGUE FEVER
• Minimise mosquitoes by e.g. burning Mosquito coils
• Use of a ‘knock down’ insecticide in sleeping and living areas at dusk.
• Understand the feeding patterns of mosquito. early morning for 2‐3 hours after daybreak and in the afternoon 2‐3 hours before dusk.
• 30% to 50% DEET
• Clothing may also be sprayed with Permethrin
• Stay in well‐screened / Aircon accommodation that is well screened
• Avoid perfumes: mosquitoes are attracted to scents.
CHIKUNGUNYA FEVERCHIKUNGUNYA FEVER
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
∗ MALARIA = Most Important of all tropical diseases• 300‐500 mill. cases/year, 2‐3mill. deaths
• 200‐300 children die from malaria each hour
• 90% malaria is in Sub‐Saharan Africa
• 30,000 travellers/yr from indust countries get malaria
• 1/100 travellers who get falciparum will die
∗ Anopheles mosquito• female, dusk to dawn
• semi‐immunity possible
∗ 4 species of Plasmodium… falciparum, malariae
vivax, ovale (hypnozoite)
Malaria Malaria

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
SEQUENCE
1. Sporozoites injected by female mosquito
2. Rapid localisation in hepatocytes ( this may take 30 min)
3. Transform, multiply and develop into tissue schizonts(pre‐erythrocytic stage of infection approx. 5 ‐16 days)
4. Tissue schizonts rupture, releasingmerozoites which go into blood, merozoites invade erythrocytes (erythrocytic stage)
5. Rupture of infected erythrocytes ‐ febrile attacks every 48 hrs
6. Repeating cycle
7. Continued transmission
……
Malaria Malaria –– Life CycleLife Cycle
Practic
al
Practic
al Punc
hpoint
Punchp
oint
Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
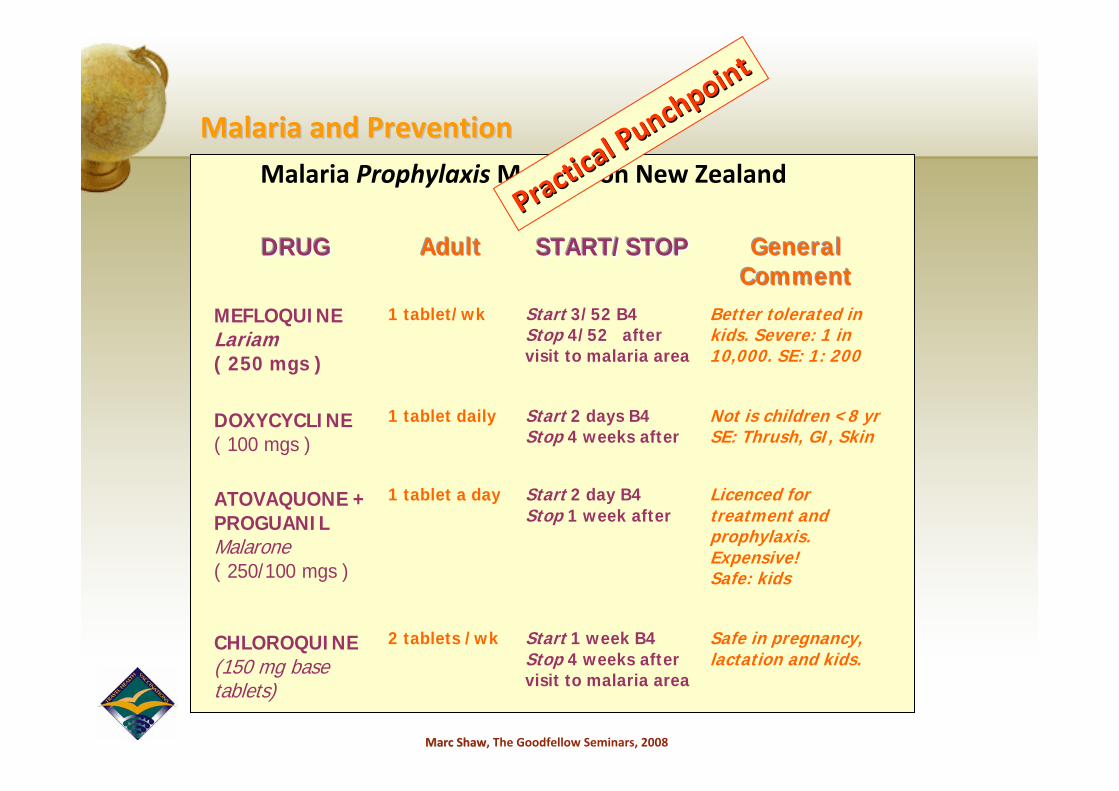
Malaria ProphylaxisMedication New Zealand
DDDRRRUUUGGG
AAAddduuulllttt
SSSTTTAAARRRTTT///SSSTTTOOOPPP
GGGeeennneeerrraaalll
CCCooommmmmmeeennnttt MEFLOQUINE Lariam ( 250 mgs )
1 tablet/wk Start 3/52 B4 Stop 4/52 after visit to malaria area
Better tolerated in kids. Severe: 1 in 10,000. SE: 1: 200
DOXYCYCLINE ( 100 mgs )
1 tablet daily
Start 2 days B4 Stop 4 weeks after
Not is children <8 yrSE: Thrush, GI, Skin
ATOVAQUONE + PROGUANIL Malarone ( 250/100 mgs )
1 tablet a day
Start 2 day B4 Stop 1 week after
Licenced for treatment and prophylaxis. Expensive! Safe: kids
CHLOROQUINE (150 mg base tablets)
2 tablets /wk
Start 1 week B4 Stop 4 weeks after visit to malaria area
Safe in pregnancy, lactation and kids.
Malaria and PreventionMalaria and Prevention
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Statistics for malaria risk for 1 month of travel without chemoprophylaxis(adapted from Steffen and Jong “Traveler’s and Immigrant’s Health”)
• Oceania 1:5
• Africa (sub Saharan) 1:50
• South Asia 1:250
• South East Asia 1:2,500
• South America 1:5,000
• Mexico and Central America 1:10,000
• 6% or more /month on no chemoprophylaxis in rural humid partsof West Africa acquire malaria
Malaria and PreventionMalaria and Prevention

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
•• ATOVAQUONE / PROGUANIL ATOVAQUONE / PROGUANIL (MALARONE ):(MALARONE ):250 mg atovaquone / 100 mg proguanil
4 tabs, daily, single dose x 3/7Take at the same time each day, WITH food or a milky drink
•• MEFLOQUINE MEFLOQUINE (LARIAM): 250 mgs(LARIAM): 250 mgsWeight is greater than 60 kgs:
3 tabs, stat; 2 tabs, 6‐8 hours later; 1 tab, 6‐8 hours later
If your weight is between 45 and 60 kgs:
3 tabs, stat; 2 tabs, 6‐8 hours later
Malaria and Self Treatment MedicationMalaria and Self Treatment Medication
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• MALARIA PREVENTION CAN BE CRITICAL IN THE TROPICS
• Armament: insect repellant
• Education: clothing, insect sprays, mosquito net, minimisation of mosquitoes bites
• Prophylaxis: antimalarial medication …
• Management of Malaria:
• A = Awareness i.e. Risk assessment
• B = Bite avoidance i.e. Personal protective measures
• C = Chemoprophylaxis/self‐Rx
• D = Diagnosis
Practic
al
Practic
al Punc
hpoint
Punchp
oint
Malaria: Prevention and ManagementMalaria: Prevention and Management

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Such dis‐ease will usually be dependant upon ‐
• ITINERARY of travel • detailed itinerary of overseas trip, including
• air‐travel direction, places, duration of travel
• type of accommodation, rural or urban
• TYPE of travelling• Season, climate, temperature and altitude of the trip
• Medications• General Practitioner letter RE dis‐eases and medications
• 2 caches
• Get medications from home and not from abroad
NonNon‐‐Communicable DisCommunicable Dis‐‐easeease

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
JET LAG CAN BE MINIMISED
• Symptoms:
• fatigue, lack of sleep, red. appetite, headache, poor conc.
• Management:
• Fly West rather than East
• Adjust to destination time ASAP!!
• At prescribed times:
• take MELATONIN
• get or avoid light exposure
• Avoid alcohol; it interferes with REM sleep.
• Sleeping pills can be helpful.
JetLagJetLag and Airand Air‐‐traveltravel

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
AIR TRAVEL AIR TRAVEL
• Conditions likely to deteriorate with altitude• Cardiovascular disease
• Respiratory disease
• Haemopoietic disease
• Motility problems
• Bowel and bladder problems
• Recent abdominal/ thoracic/ENT surgery
• Venous stasis problems
• Middle ear and sinus diseases
• Significant psychiatric disease

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Air Travel Air Travel …… ‘‘rules of thumbrules of thumb’’
• “Rules of Thumb”
• Patient able to walk 100 metres to aircraft carrying hand luggage
• Patient should have control of sphincters
• No M.I. within 10 days of travel
• No stroke within 14 days of travel
• Patient/assistant:give own medications and feed/toilet self
• International travel >36 weeks pregnancy not recommend.

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• Alcohol and Drugs• Needs of corporate travellers• Loneliness and familiars: relationships/sex, taboos• Temptations: drugs and alcohol, penalties, additives to drugs etc …• Travel distress…air, sea, phobias, fatigue, timetables, waiting• Dealing with moral and cultural issues:
–poverty, beggars–religions–women in society
• Violence and theft: dealing with ‘bad’ company• Illness and brainwashing
All travellers need to have humourAll travellers need to have humour……Whatever turns your crank!Whatever turns your crank!
Lifestyle Lifestyle –– the issues!the issues!

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Counterfeit drugsCounterfeit drugs
•• Counterfeit drugs est. to represent 10% of the global market in Counterfeit drugs est. to represent 10% of the global market in medicines, rising to almost 33% medicines, rising to almost 33% in some parts of the developing worldin some parts of the developing world
•• One indicator is European Union customs statistics, which showedOne indicator is European Union customs statistics, which showed a 4 x increase 2007 with 497 a 4 x increase 2007 with 497 border seizures of 2.7 million medicinesborder seizures of 2.7 million medicines
•• Although lifestyle drugs such as Viagra dominated, hauls also inAlthough lifestyle drugs such as Viagra dominated, hauls also incl. cl. signifsignif. nos. of drugs to treat . nos. of drugs to treat hypercholesterolaemiahypercholesterolaemia, osteoporosis, and hypertension, osteoporosis, and hypertension
•• A recent analysis of A recent analysis of artemisininartemisinin group drugs for malaria in group drugs for malaria in Kenya+CongoKenya+Congo showed nearly showed nearly 33% were fake, rising to 77% for injectable forms33% were fake, rising to 77% for injectable forms
•• The public health effect is clear: poor quality medicines cause The public health effect is clear: poor quality medicines cause harm harm –– they may lack active they may lack active ingredients of contain toxic onesingredients of contain toxic ones
Financial TimesFinancial Times, London, London
DRUGS AND PERSONAL HEALTHDRUGS AND PERSONAL HEALTH

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• PERSONAL PREPARATION BEFORE TRAVEL• Essential ‐ especially for the youthful O/E‐er!!
• finances• ( card/spare $ ), medical kit + personalmedications
• coping strategies under stress• preparedness for ‘newness’
• prepare for bereavement• home / away contact addresses
• plans ‘on arrival’• accommodation
• travel
• culture adaptation
Safety and SecuritySafety and Security

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
PERSONAL ACCIDENTS, PERSONAL ACCIDENTS, INJURY and MUGGINGINJURY and MUGGING
•• > 75% of travellers concerned re safety when travelling overseas> 75% of travellers concerned re safety when travelling overseas(Leggat from Amex Data, 1999)
•• Accidents remain the most prevent. cause of travellers deathsAccidents remain the most prevent. cause of travellers deaths• … most are avoidable!!
•• ““WesternersWesterners”” travelling in developing countriestravelling in developing countries = ““richrich”” = MUGGINGMUGGING
‐ even tattered “leather jackets” can be valuable!
Message: Message: ‘‘carry just what you need, basic carry just what you need, basic –– but with low profilebut with low profile’’
•• Tasmanian Medical students going to overseas rotations reportTasmanian Medical students going to overseas rotations report… ‘ assaults, harassments and accidents are of increasing concern, and pre‐travel counselling essential on avoiding getting into danger’
The Need for Insurance for Travellers?The Need for Insurance for Travellers?

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
British Airways ‐ Boeing 777‐236ERLondon, United Kingdom17th January, 2008
• Plane landed 1000 ft short of runway
• It skidded through grass and came to rest on the edge of runway
• Passengers evacuated through emerg. slides
• 18 needed treatments for minor injuries
• After demands for increased thrust, the engines failed to respond
• Pilot managed to "glide" the airliner over houses, airport buildings and a busy road B4 "belly flopping" it onto grass 150 ft inside the perimeter fence ‐ 1000 ft short of runway
• Pilots had received no warning that the plane was losing power due to a problem with the plane was losing power due to a problem with the aircraft's alarm systemsaircraft's alarm systems
Aircraft crashes still Aircraft crashes still biggest fear of travellersbiggest fear of travellers
ALWAYS
BIGPUB
LICITY!
!
ALWAYS
BIGPUB
LICITY!
!
1:10,000,000 chance of dying1:10,000,000 chance of dying

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
ENVIRONMENTAL ENVIRONMENTAL CONSIDERATIONSCONSIDERATIONS
The irony is that Environment is usually a big reason for travelThe irony is that Environment is usually a big reason for travel!!
Planning Planning is essential to understand intended environment(s)There are numerous indicators of environmental health, one of those principally requiring consideration is air pollutionair pollution::
All large cities in developing countries have All large cities in developing countries have significant air pollutionsignificant air pollution
ChinaChina …… 9 of 10 global 9 of 10 global citiescities with worst pollutionwith worst pollutionParticulates (airborne parts <10 Particulates (airborne parts <10 μμm m diamdiam) ) in mcg/cubic metre: in mcg/cubic metre:
Stockholm 9, Mexico City 279, Lanzhou China 732Stockholm 9, Mexico City 279, Lanzhou China 732
Ho Chi MinhHo Chi Minh City 3 million motor‐cycles 90% have 2 stroke engines2 stroke enginesThese are worst offenders re suspended particulate matter and hydrocarbon emissions

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Managing the EnvironmentManaging the Environment
Given that air pollution has been found to affect residents healGiven that air pollution has been found to affect residents health in both th in both short and longshort and long‐‐term studies, there is no reason to think that travellers are term studies, there is no reason to think that travellers are not impacted by it. Nevertheless the nature and extent of the rinot impacted by it. Nevertheless the nature and extent of the risk are yet sk are yet to be determinedto be determined.
What does this mean for travel health provider?What does this mean for travel health provider?
1.1. Advice needs to be tailoredAdvice needs to be tailored for traveller to urban environment
2.2. Patients with e.g. COPD should consider travelling with a Patients with e.g. COPD should consider travelling with a ‘‘rescue cocktailrescue cocktail’’of 3 other drugs for use during exacerbations: an additional bronchodilator, oral steroid, appropriate antibiotic.

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
PLANNING THE TRIPPLANNING THE TRIP
• Personal Preparation
• PreventativeTopical disease advice
Current up‐to‐date health issues
STDs, HIV, AIDS
Loneliness
Drugs and alcohol issues
Familiars for the long term traveller/ expat
Understanding the culture
Travel distress…air, sea, phobias, fatigue, timetables, waiting
Plans ‘on arrival’…accommodation, travel, adapt. to ‘newness’
Adaptation to the local climate: weather, mores, attiudes

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
EnvironmentEnvironment……altitude sickness altitude sickness = acute mountain sickness AMS= acute mountain sickness AMS
• ALTITUDE SICKNESS CAN BE MINIMISED
•• SYMPTOMS:SYMPTOMS:• headaches, dizziness, fatigue,
• sleep disturbance, loss of appetite
• nausea and vomiting
•• 4 BASIC RULES4 BASIC RULES to avoid dying of AMS!• Learn early symptoms of AMS and how to recognise them
• Never ascend to sleep at a new altitude with any AMS symptoms
• Descend, if symptoms are getting worse whilst at the same alt.
• Ascend slowly to high altitudes
• Acetazolamide, DEXAMETHASONE and Ibuprofen ?
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
EnvironmentEnvironment
SWIMMING IN FRESH WATER CAN BE RISKYThe larvae in fresh water …
BILHARZIA = SCHISTOSOMIASISBILHARZIA = SCHISTOSOMIASIS
• Parasite infection caused by schistosomes (worms or blood flukes )
• from fresh water snails • 4 main types pathogen• 200 mill. cases/year (200,000 die)• 30+ countries
• Africa (70% chance), Mid. East, SE Asia, Central and South America
Symptoms, Diagnosis and Follow‐up
Treatment…Praziquantel
Practic
al
Practic
al Punc
hpoint
Punchp
oint

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
FIRST AIDFIRST AID Remedies! Remedies!
What to treat whilst travellingWhat to treat whilst travelling……• Assistance in diagnosis of simple dis‐orders• Skin conditions, respiratory tract infections,
bowel infections
How to treat itHow to treat it……• Self treatment of various diseases
•guide to recognition and management•simple, practical management protocols
• Self treatment of diseases like malaria•depending on location and duration of travel
Medical kitsMedical kits……•WHAT to take and HOW to use whatever it is that’s taken and WHEN to seek advice!!• BIG THREE: Iodine, antibiotic, anti‐diarrhoeal• Prophylactics: ‘Don’t be a dick’!!

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
Outbreaks over the last 12 months Outbreaks over the last 12 months –– Pacific RegionPacific Region•• Typhoid Typhoid –– Samoa (2), Marshall Islands (3), Fiji (2), NZ, TongaSamoa (2), Marshall Islands (3), Fiji (2), NZ, Tonga•• Dengue Dengue –– Cooks, Fiji, Samoa, New Caledonia, Australia, TongaCooks, Fiji, Samoa, New Caledonia, Australia, Tonga
American Samoa, Palau, Tahiti, Yap (Micronesia) American Samoa, Palau, Tahiti, Yap (Micronesia) •• Leptospirosis Leptospirosis –– Wallis and Futuna, New CaledoniaWallis and Futuna, New Caledonia•• Diarrhoea Diarrhoea –– Fiji, PalauFiji, Palau•• Pertussis Pertussis –– PNG, Yap, Federated PNG, Yap, Federated •• ZikaZika –– YapYap•• Q Fever Q Fever –– AustraliaAustralia•• Rubella Rubella –– AustraliaAustralia•• Measles Measles –– Fiji, AustraliaFiji, Australia•• Mumps Mumps –– Fiji, AustraliaFiji, Australia•• InfluenzaInfluenza ‐‐ KiribatiKiribati•• Murray RiverMurray River ‐‐ AustraliaAustralia THE MESSAGE IS: these regions are not as well THE MESSAGE IS: these regions are not as well
developed medically as developed medically as AustAust and NZ. and NZ. Travellers should not expect the health Travellers should not expect the health
care services to be of equivalencecare services to be of equivalence
Current Disease Outbreaks:Current Disease Outbreaks:

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
• CDC‐Travel• www.cdc.gov/travel
• ISTM• www.istm.org
• WHO International Travel and Health• www.who.int/ith/english/index.htm
• Worldwise OnLINE (Professional)• www.worldwise.co.nz ( New Zealand advice )
• CIA Factbook• www.cia.gov/cia/publications/factbook
• U.S. Department of State• www.travel.state.gov
• NaTHNaC• www.nathnac.org
• Travel Essentials (New Zealand Consumers‐ FREE)• www.travel‐essentials.co.nz
Sources of ReferenceSources of Reference

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
SAFETY AND SAFETY AND SECURITY OVERSEASSECURITY OVERSEAS
•• DFAT, Aust.DFAT, Aust. www.dfat.gov.auwww.dfat.gov.au
•• MFAT, NZMFAT, NZ www.safetravel.govt.nzwww.safetravel.govt.nz
•• USAUSA‐‐CIA World Fact Book CIA World Fact Book www.odci.gov/cia/publications/factbook/index.htmlwww.odci.gov/cia/publications/factbook/index.html
•• USAUSA‐‐US State Department Travel AdvisoriesUS State Department Travel Advisorieswww.travel.state.gov/travel_warnings.htmlwww.travel.state.gov/travel_warnings.html
•• Foreign and Commonwealth OfficeForeign and Commonwealth Office www.fco.gov.ukwww.fco.gov.uk/travel/travel
•• Global Incident MapGlobal Incident Map www.globalincidentmap.com/home.phpwww.globalincidentmap.com/home.php•• James Cook UniversityJames Cook University
www.jcu.edu.au/school/sphtm/antonbreinl/centers/disaster/index.hwww.jcu.edu.au/school/sphtm/antonbreinl/centers/disaster/index.htmtm
There are numerous sources There are numerous sources …… it is just a matter of knowing WHERE to go!!it is just a matter of knowing WHERE to go!!

Marc ShawMarc Shaw, The Goodfellow Seminars, 2008
•• Yellow Fever CertificationYellow Fever Certification – needs to have travel medicine
•• ISTMISTM• Certificate of Knowledge (CTH)
•• ASTM&H ASTM&H • Certificate of Knowledge in Clinical Tropical Medicine and
Travelers Health
•• University CoursesUniversity Courses• Australia: JCU (Public Hlth)• Universities: Glasgow, London,
Univ. of Otago, Wits in Sth Africa
•• Worldwise Annual CoursesWorldwise Annual Courses• Held 2 x a year for Nurses and 1 x a yr for Doctors
Courses in Travel MedicineCourses in Travel Medicine


















