
Trial enrolment of Late Presenters - vaccineenterprise.org · Trial enrolment of Late Presenters...
22
Trial enrolment of Late Presenters numbers and challenges from PROMISE trial Lynda Stranix-Chibanda, A.Coletti, K McCarthy, P. Flynn, M.G. Fowler and the PROMISE study team
Transcript of Trial enrolment of Late Presenters - vaccineenterprise.org · Trial enrolment of Late Presenters...

TrialenrolmentofLatePresentersnumbersandchallengesfromPROMISEtrial
LyndaStranix-Chibanda,A.Coletti,KMcCarthy,P.Flynn,M.G.FowlerandthePROMISEstudyteam

PROMISEstudy• Randomizedcontrolledtrialbeganin2010• TodetermineoptimalantiretroviralstrategytopreventverticaltransmissionofHIVandmaintainmaternalandinfanthealth
• Acrossdiversecaresettings:– 1077HSwhereARTandformulafeedingstandard– 1077FF/BFwhereotherantiretroviralstrategieswerestandardplusformulafeeding(FF)orbreastfeeding(BF)

70sitesin15countries
StudyDesign• HealthyHIV-infectedwomen• Didnot meetlocalcriteriaforART• Randomlyassignedtodifferentantiretroviralstrategiestoassess:– preventionofverticaltransmissionduringpregnancyandpost-delivery
– infantsafety– maternalhealth

Antepartum Component cessation of breastfeeding
Completefollow-up in
AP Component
Completefollow-up in
PP Component
PostpartumComponent
Maternal Health Component
Antepartum Component
completefollow-up
Late Presenters
During Pregnancy During Breastfeeding After Weaning
Completefollow-up in
MH Component
Labor andDelivery
During PregnancyIMPAACT 1077BF Components
104weeks1550
3400
3650

KeyEligibilityforLPregistration
• HIV infection by rapid testing• No prior ARV exposure in current pregnancy• In labour or within 72 hours after delivery• Infant healthy and alive with birth weight at least 2 kg
(if delivered prior to registration)• Maternal CD4+ cell count not required prior to registration
(but exclude if known to be less than 350)• No other maternal lab values required prior to registration

RationaleforLPregistration
• Estimates were that up to 30% of women delivering in resource limited settings were Late Presenters
• Testing in labour is feasible• ARV prophylaxis reduces transmission even when
started in labour or postpartum• To complete screening procedures in good time for
Postpartum randomization

QuestionsforDiscussion• How many LPs (what proportion) are expected?• What procedures will be put in place to obtain informed
consent and register LPs before delivery? • How feasible will it be to complete the registration process
(using the Subject Enrollment System) before delivery?• What procedures will be put in place to ensure that study
drug kits with corresponding SIDs are available in the labour ward?
• What other operational issues or challenges might you foresee for LP registration?
2010
0
50
100
150
200
250
Apr-11
May-11
Jun-11
Jul-1
1
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Jul-1
2
Aug-12
Sep-12
Oct-12
Nov-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-1
3
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Jul-1
4
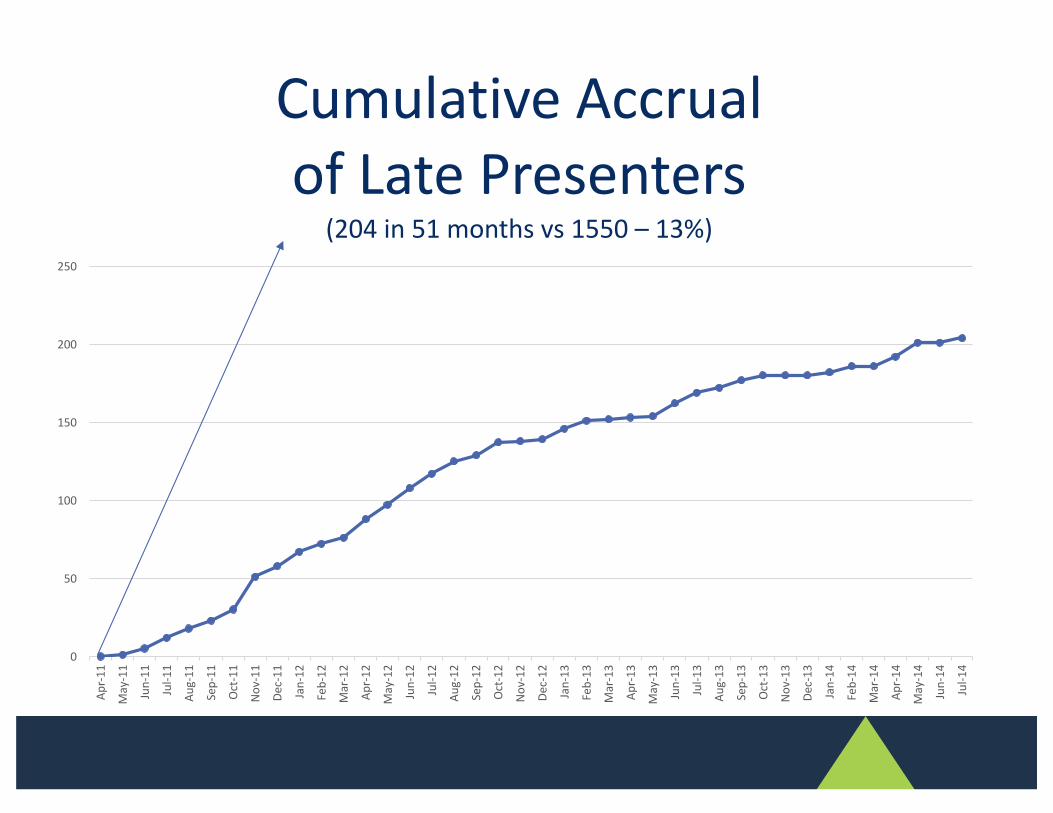
CumulativeAccrualofLatePresenters
(204in51monthsvs1550– 13%)

ChallengeswithEnrollment
• Primarily operational– Difficult to access Late Presenters– Entry procedures cumbersome– Highly vulnerable psychosocially
• Gained valuable experience (both the sites and protocol writing teams)
ØTop tips from PROMISE with input from P1115 study team and sites

Access• Participants identified in labour ward or postnatal ward
ØStudy staff work offsite• Deliveries 24/7
ØStudy staff work shiftsØProvide ‘talk time’ to labour ward staff
• Obstetric/neonatal complications in those with no ANC– Retained in postnatal ward longer than usual– Medical needs prioritized over studyØ Individualized tracking of timeframe for entry visit, and
follow-up visit (widen study windows)

EntryVisitTimelines30mins-1hour
•Sensitizationofpotentialparticipant•Reviewofmedicalrecordsforpotentialeligibilityà INFORMSTUDYCLINIC
3-5hours
•InformedConsentProcess
35mins•MaternalHIVtest(Sample#1)
40mins•MaternalandNeonatalhistoryandphysicalexamination
15mins•InitialNeonateblooddraw(viralloadandSOEtests)
15mins•ConfirmatoryHIVtestforneonate>1hourafterinitialblooddraw
30-45mins
•Pharmacy
12
Example
ALLDE
PTSONHIGHAL
ERT

EntryProcedures• Not particularly tricky for PROMISE :
– Informed consent for study entry (mother-infant pair)
– Subject Enrolment System (internet based)
– Counselling (infant feeding, HIV pre-test)
– Blood draws (HIV confirmation, baseline CD4 and safety)
– Study drug dispensing• Completed in postnatal ward or at study clinic
ØEngage obstetric team (all stakeholders), baby wagonØFacilitate rapid disclosure to dad/gogo vs very creative
home visit plan
EntryProcedures• Very tricky consenting session and enrolment, at times :
– Hadn’t fully accepted new HIV positive status– Low prior knowledge of HIV and PMTCT– Low literacy– No privacy in postnatal ward– Postpartum exhaustion– Early discharge homeØEngage obstetric team, promote PIHTC for partnersØ Internet connectivity offsite for SES

Vulnerability• Impoverished, underserved communities• Psychologically distraught• Non-disclosure of HIV status and trial participation• No social support• Unwell
– Doubt full comprehension of trial particulars– Doubt consent is truly informed– Doubt ability to comply with trial schedule– Risk of loss to follow-up

Vulnerability• Impoverished, underserved communities
ØReadily mapped for more efficient resource allocation• Psychologically distraught
Ø Intense supportive counselling, and again …ØScreen for depression, and again …ØRevisit IC discussion, and again … ØVisit reminders, and again …
• Non-disclosureØFacilitate the disclosure process (ask about Intimate
Partner Violence)

Vulnerability• No social support
ØSupport groups for study participantsØEngage community for referral structures (psychological
support and income generation)
• Unwell Ø Initiate ARTØMonitor more frequently (risk low adherence, poor infant
health outcomes)
ØFrequent infant HIV testing

Conclusion• A stakeholders/community engagement plan is
invaluableØ Know your population’s needs
• Site operations can be devised to account for difficulties associated with recruitment around the time of deliveryØ Plan aheadØ Look out for obstacles and ethical dilemmasØ Hire ‘on the ball’ recruiters
• Adequate resources must be allocated to recruiting team and to address vulnerability Ø Optimize accrual rateØ Improve retention
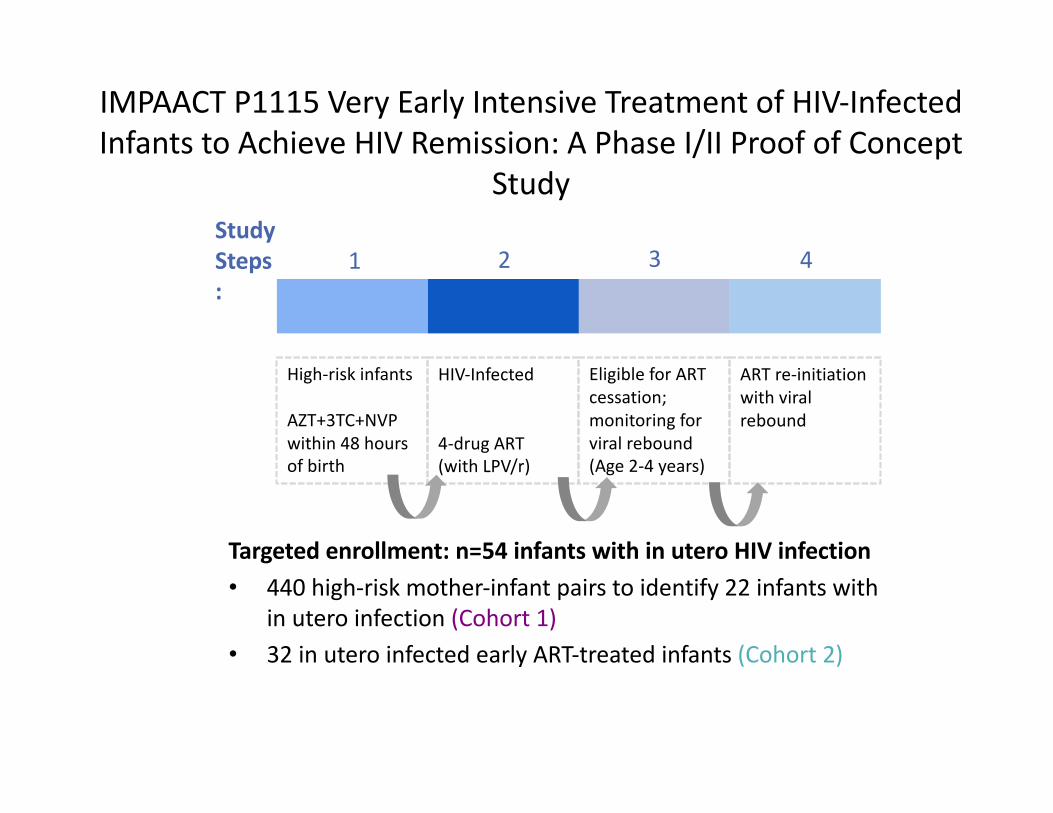
IMPAACTP1115VeryEarlyIntensiveTreatmentofHIV-InfectedInfantstoAchieveHIVRemission:APhaseI/IIProofofConcept
Study
Targetedenrollment:n=54infantswithinuteroHIVinfection• 440high-riskmother-infantpairstoidentify22infantswith
inuteroinfection(Cohort1)• 32inuteroinfectedearlyART-treatedinfants(Cohort2)
StudySteps:
1 2 3 4
High-riskinfants
AZT+3TC+NVPwithin48hoursofbirth
HIV-Infected
4-drugART(withLPV/r)
EligibleforARTcessation;monitoringforviralrebound(Age2-4years)
ARTre-initiationwithviralrebound
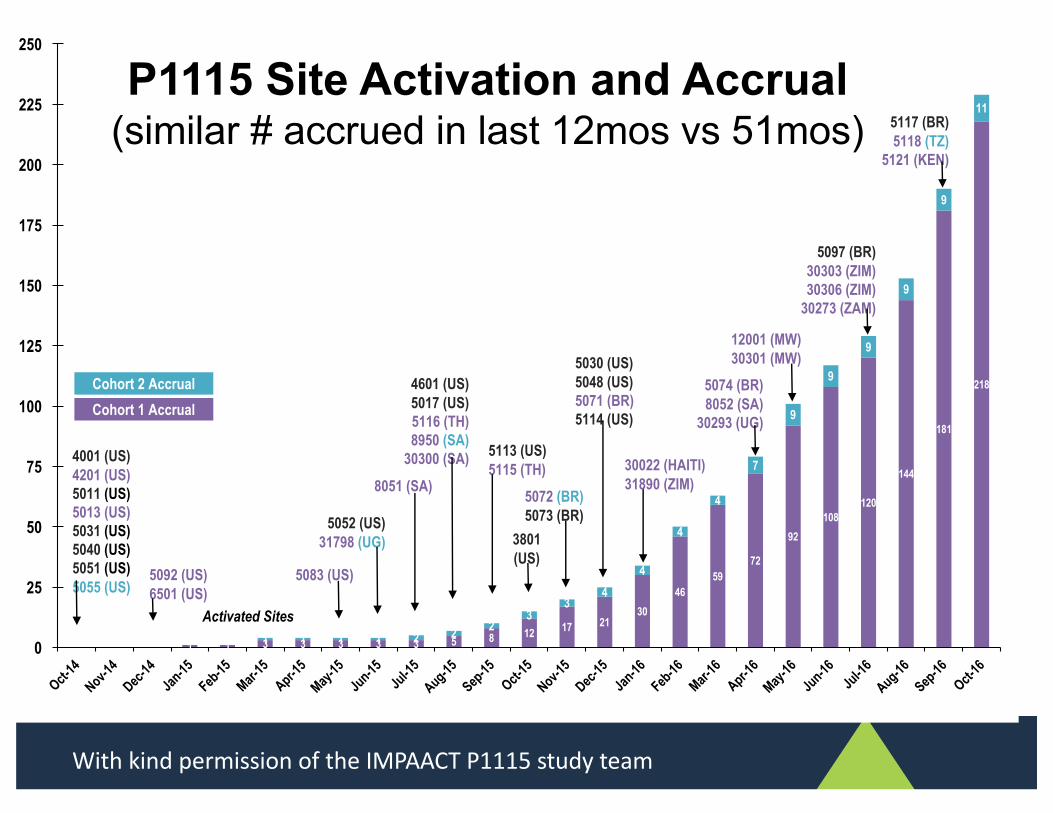
1 1 3 3 3 3 3 5 8 12 17 2130
4659
72
92108
120
144
181
218
1 1 1 1 2 2 23
34
4
4
4
7
9
9
9
9
9
11
0
25
50
75
100
125
150
175
200
225
250
5052 (US)31798 (UG)
4601 (US)5017 (US)5116 (TH)8950 (SA)
30300 (SA) 5113 (US)5115 (TH)
5072 (BR)5073 (BR)
8051 (SA)
Activated Sites
4001 (US)4201 (US)5011 (US)5013 (US)5031 (US)5040 (US)5051 (US)5055 (US)
5092 (US)6501 (US)
5083 (US)
3801 (US)
5030 (US)5048 (US)5071 (BR)5114 (US)
30022 (HAITI)31890 (ZIM)
5074 (BR)8052 (SA)
30293 (UG)
12001 (MW)30301 (MW)
5097 (BR)30303 (ZIM)30306 (ZIM)
30273 (ZAM)
Cohort 2 AccrualCohort 1 Accrual
5117 (BR)5118 (TZ)
5121 (KEN)
P1115 Site Activation and Accrual(similar # accrued in last 12mos vs 51mos)
WithkindpermissionoftheIMPAACTP1115studyteam




















