Triage in Palliative Care Setting_Dr Joseph Ninan
23
Triage in Palliative Care Setting Dr. Joseph Ninan Palliative Care Association of Kota Kinabalu
-
Upload
malaysianhospicecouncil6240 -
Category
Documents
-
view
52 -
download
1
description
10th Malaysian Hospice Congress, Johor Bahru, Malaysia
Transcript of Triage in Palliative Care Setting_Dr Joseph Ninan

Triage in
Palliative Care
Setting Dr. Joseph Ninan
Palliative Care Association of Kota Kinabalu

History
• PCAKK inception in 1993
• Non-profit charitable NGO in 1998
• Community based palliative care service
• Coverage 30km radius from Association building
• Home care service to advanced incurable terminally ill
cancer patients
• One volunteer nurse
• Aim: Pain & symptoms control

Promises
• Seen within 48 Hrs of referral of service
• Weekly visit & more when necessary
• Pain & symptoms control
• Loan of medical equipment
• Dr.’s consultation & visit when necessary

Limitations
• 5 ½ day working
week
• No after office hour
service
• Sunday & public
holidays off

Growth
• 1993 – 2008
• One nurse to 4 nurses and one volunteer Dr.
• Since 2011, 6 nurses & 2 Drs.
• 60 to 80 patients
• Adults Cancer, Paediatric Cancer, Organ Failure.

Difficulties
• Maintenance of weekly visit
• Medical Management
• Increased work stress
• Burn Out
• Lack of hands on training
• Lack of proper medical documentation
• Inadequate at medical management

New Tools
• Phase System
• Karnofsky Performance Scale
• Introduced in August 2008

Phase System
• 1. Stable Phase
• 2. Unstable Phase
• 3. Deteriorating Phase
• 4. Terminal Phase
• 5. Bereavement Phase

Karnofsky Performance
Scale (KPS)
• Classification according to performance
• Assess 3 dimension of Health
1. Activity
2. Work
3. Self Care
• Scale form 100 to 0. Divisions of 10

KPS
100 Normal with no complaints or evidence of disease
90 Able to carry on normal activity but with minor signs of illness present
80 Normal activity but requiring effort. Signs and symptoms of disease more
prominent.
70 Able to care for self, but unable to work or carry on other normal activities.
60 Able to care for most needs, but requires occasional assistance.
50 Considerable assistance and frequent medical care required.
40 In bed more than 50% of the time.
30 Almost completely bedfast.
20 Totally bedfast and requiring extensive nursing care by professionals and/or
family.
10 Comatose or barely rousable.
0 Death

Methodology
• Triage using Phase System.
• KPS use to assesss performance, prognosticate &
determine level of care.

Methodology
• Visitation defined by Phase System
• Stable – once a fortnight & alternate week phone
consultation
• Unstable – Daily or alternate day visitation.
• Deteriorating – Weekly visits.
• Terminal – Daily or alternate day visits.
• Bereavement – One week after funeral conducted.

Data
• Data Collected from 2009
• Looked at
1. Phase & KPS at 1st Home visit
2. Length of stay in Home Care Programme.
3. Place of Death

0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5
No. of
Pati
ents
Phase
Phase at 1st Home Visit
2009
2010
2011

10%
33%
48%
9%
0%
Phase at 1st Home Visit 2011
1 2 3 4 5

0
20
40
60
80
100
120
90 to 70 60 to 40 30 to 10 < 10
No. of
Pati
ent
KPS
KPS on Initial Home Visit 2011
2009
2010
2011

0
20
40
60
80
100
120
90 to 70 60 to 40 30 to 10 < 10
No
. o
f P
ati
ent
KPS
KPS on Initial Home Visit 2011
2009
2010
2011
0
10
20
30
40
50
60
70
80
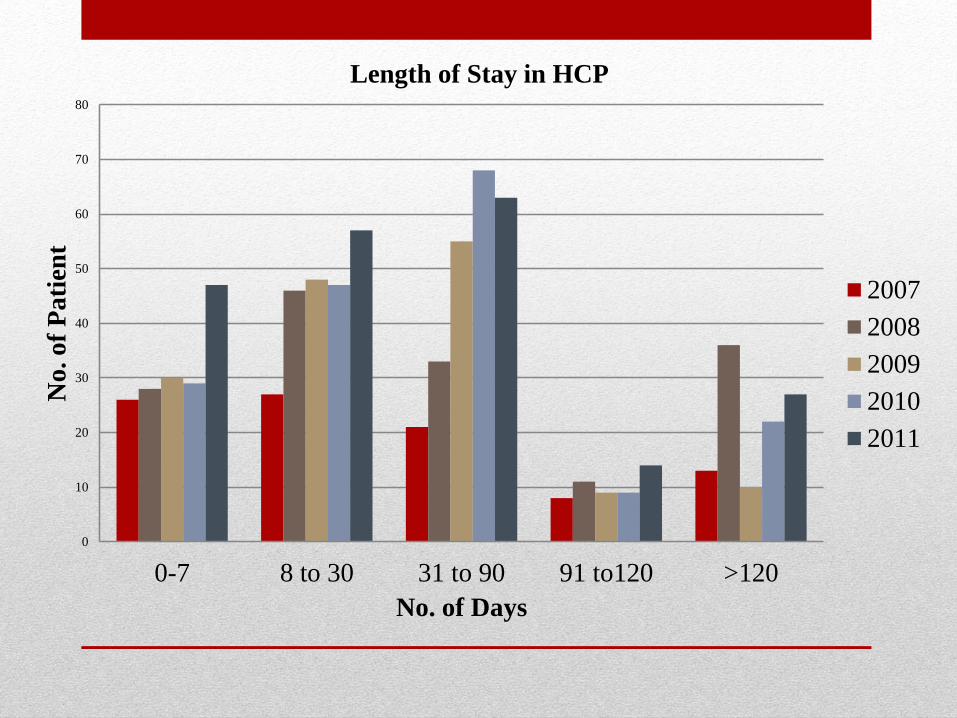
0-7 8 to 30 31 to 90 91 to120 >120
No
. o
f P
ati
ent
No. of Days
Length of Stay in HCP
2007
2008
2009
2010
2011

0
20
40
60
80
100
120
140
2007 2008 2009 2010 2011
No
. o
f P
ati
ent
Year
Place of Death
HOME
PCU
OTHERS

Conclusion
Using the Phase system and Karnofsky
Performance Scale has enabled us to achieve the
followings:
1. Optimal use of limited manpower/resources in
the environment of increasing demand and
expectation from the community/patient/family and
expansion of service.

Conclusion
2. Guideline for the nurses in their visitation.
3. Better job satisfaction for the nurses and reduces
the chances of burn out.
4. Statistically tracking our work load and facilitate
future service development and planning.


Thank You