
Treuman Katz Center for Pediatric Bioethics - 2009 Conference The Adolescent’s Role in End-of-Life...
19
Treuman Katz Center for Pediatric Bioethics - 2009 Conference The Adolescent’s Role in End-of-Life Decision Making Ethics versus Policy Lainie Friedman Ross, MD, PhD Carolyn and Matthew Bucksbaum professor of Clinical Ethics Professor, Depts of Pediatrics, Medicine, Surgery & the College Associate Director, MacLean Center for Clinical Medical Ethics University of Chicago
-
Upload
judith-beasley -
Category
Documents
-
view
214 -
download
0
Transcript of Treuman Katz Center for Pediatric Bioethics - 2009 Conference The Adolescent’s Role in End-of-Life...
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
The Adolescent’s Role in End-of-Life Decision Making
The Adolescent’s Role in End-of-Life Decision Making
Ethics versus PolicyEthics versus Policy
Lainie Friedman Ross, MD, PhDLainie Friedman Ross, MD, PhD
Carolyn and Matthew Bucksbaum professor of Clinical EthicsProfessor, Depts of Pediatrics, Medicine, Surgery & the College
Associate Director, MacLean Center for Clinical Medical EthicsUniversity of Chicago
Carolyn and Matthew Bucksbaum professor of Clinical EthicsProfessor, Depts of Pediatrics, Medicine, Surgery & the College
Associate Director, MacLean Center for Clinical Medical EthicsUniversity of Chicago

Treuman Katz Center for Pediatric Bioethics - 2009 Conference
OBJECTIVESOBJECTIVES• To clarify the roles of the parents, the To clarify the roles of the parents, the
minor, and the state for decisions regarding minor, and the state for decisions regarding effective life-saving treatment for childreneffective life-saving treatment for children
• To consider the roles of the parents, the To consider the roles of the parents, the minor, and the state for decisions where minor, and the state for decisions where effective life-saving treatment does not effective life-saving treatment does not existexist
• To consider whether and when reasons To consider whether and when reasons mattermatter
• To clarify the roles of the parents, the To clarify the roles of the parents, the minor, and the state for decisions regarding minor, and the state for decisions regarding effective life-saving treatment for childreneffective life-saving treatment for children
• To consider the roles of the parents, the To consider the roles of the parents, the minor, and the state for decisions where minor, and the state for decisions where effective life-saving treatment does not effective life-saving treatment does not existexist
• To consider whether and when reasons To consider whether and when reasons mattermatter
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
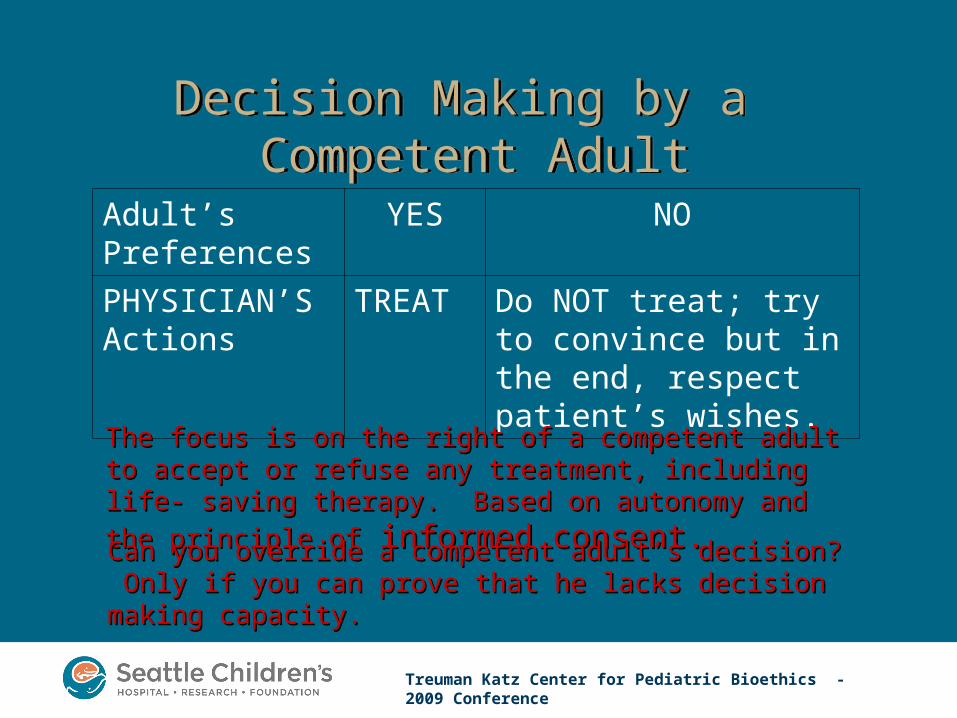
Decision Making by a Competent Adult
Decision Making by a Competent Adult
Adult’s Preferences
YES NO
PHYSICIAN’S Actions
TREAT Do NOT treat; try to convince but in the end, respect patient’s wishes.
The focus is on the right of a competent adult to accept or The focus is on the right of a competent adult to accept or refuse any treatment, including life- saving therapy. Based on refuse any treatment, including life- saving therapy. Based on
autonomy and the principle ofautonomy and the principle of informed consent. informed consent.
Can you override a competent adult’s decision? Only if you Can you override a competent adult’s decision? Only if you can prove that he lacks decision making capacity.can prove that he lacks decision making capacity.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Decision Making in PediatricsDecision Making in Pediatrics• Children are presumed incompetent and unable
to make decisions.• Parents are presumed to be the decision makers.
– Parents are guided by the “Best Interest” principle.
• Parental authority can be overridden if the state believes that the parents are abusive or neglectful.– State has the authority to ensure that the
child’s “Basic Needs” or “Basic Interests” are met.
• Concept of basic interests by John Rawls.
• Children are presumed incompetent and unable to make decisions.
• Parents are presumed to be the decision makers.– Parents are guided by the “Best Interest” principle.
• Parental authority can be overridden if the state believes that the parents are abusive or neglectful.– State has the authority to ensure that the
child’s “Basic Needs” or “Basic Interests” are met.
• Concept of basic interests by John Rawls.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
New trend to show greater respect for minor refusals, particularly when
parents agree with them.
New trend to show greater respect for minor refusals, particularly when
parents agree with them.
• In re E.G. (IL, 1989) [17 years]• Billy Best (MA, 1994) [16 years]• Starchild Abraham Cherrix (VA, 2006)
[15 years]• Dennis Lindberg (WA, 2007) [14 years]
• In re E.G. (IL, 1989) [17 years]• Billy Best (MA, 1994) [16 years]• Starchild Abraham Cherrix (VA, 2006)
[15 years]• Dennis Lindberg (WA, 2007) [14 years]
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
The Trend is Not AbsoluteThe Trend is Not Absolute
• Daniel Hauser (MN 2009) [13 years]– Unable to read (learning disability)– Mom supported his decision; Father
did not.
• Daniel Hauser (MN 2009) [13 years]– Unable to read (learning disability)– Mom supported his decision; Father
did not.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
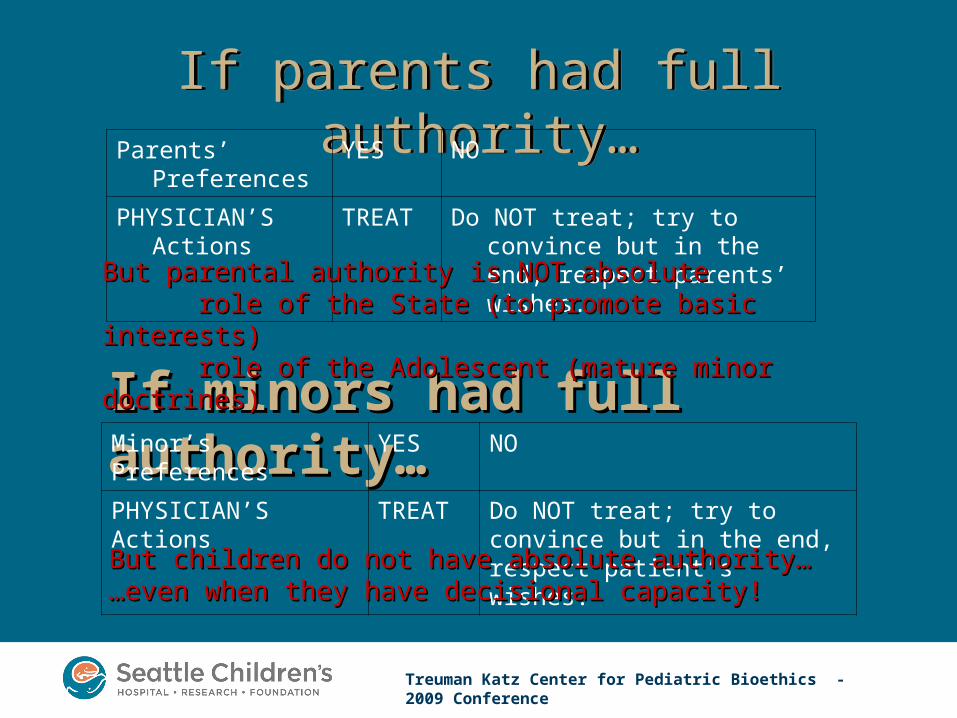
If parents had full authority…If parents had full authority…Parents’ Preferences YES NO
PHYSICIAN’S Actions
TREAT Do NOT treat; try to convince but in the end, respect parents’ wishes.
If minors had full authority…If minors had full authority…Minor’s Preferences YES NO
PHYSICIAN’S Actions TREAT Do NOT treat; try to convince but in the end, respect patient’s wishes.
But parental authority is NOT absoluteBut parental authority is NOT absoluterole of the State (to promote basic interests)role of the State (to promote basic interests)role of the Adolescent (mature minor doctrines)role of the Adolescent (mature minor doctrines)
But children do not have absolute authority…But children do not have absolute authority………even when they have decisional capacity!even when they have decisional capacity!
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
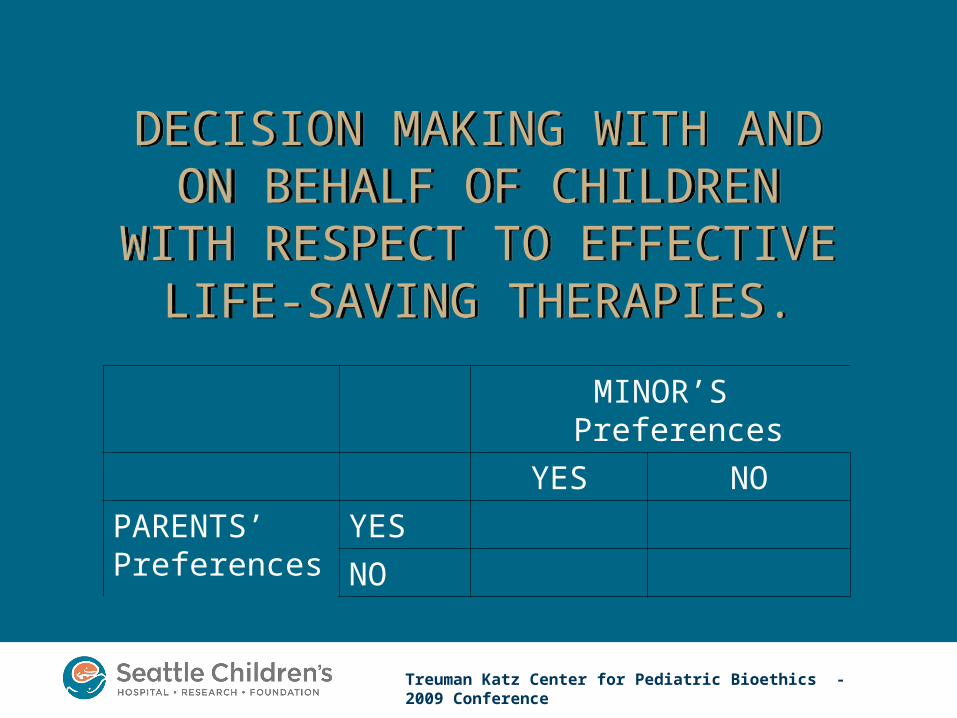
MINOR’S Preferences
YES NO
PARENTS’Preferences
YES
NO
DECISION MAKING WITH AND ON BEHALF OF CHILDREN
WITH RESPECT TO EFFECTIVE LIFE-SAVING THERAPIES.
DECISION MAKING WITH AND ON BEHALF OF CHILDREN
WITH RESPECT TO EFFECTIVE LIFE-SAVING THERAPIES.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
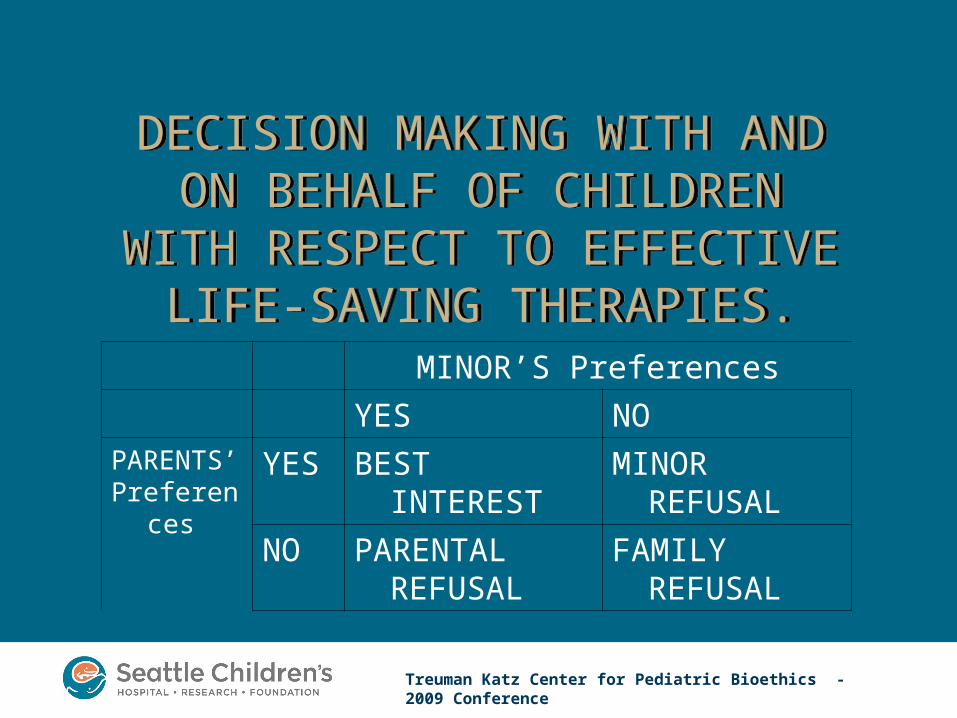
MINOR’S Preferences
YES NOPARENTS’Preferences
YES BEST INTEREST MINOR REFUSAL
NO PARENTAL REFUSAL
FAMILY REFUSAL
DECISION MAKING WITH AND ON BEHALF OF CHILDREN
WITH RESPECT TO EFFECTIVE LIFE-SAVING THERAPIES.
DECISION MAKING WITH AND ON BEHALF OF CHILDREN
WITH RESPECT TO EFFECTIVE LIFE-SAVING THERAPIES.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
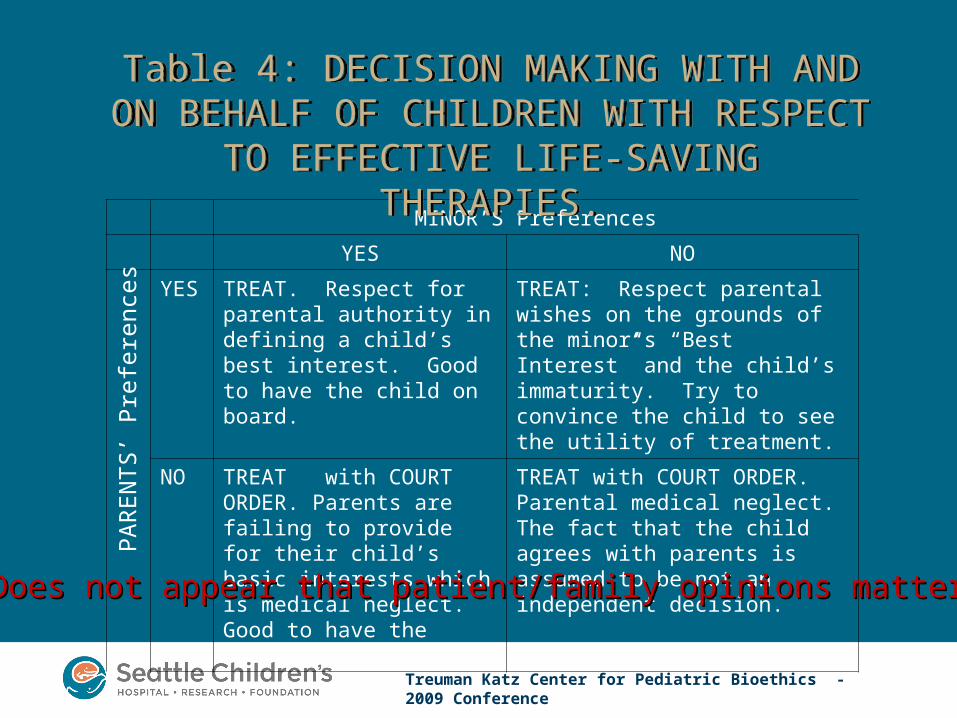
MINOR’S Preferences
YES NO
YES TREAT. Respect for parental authority in defining a child’s best interest. Good to have the child on board.
TREAT: Respect parental wishes on the grounds of the minor’s “Best Interest” and the child’s immaturity. Try to convince the child to see the utility of treatment.
NO TREAT with COURT ORDER. Parents are failing to provide for their child’s basic interests which is medical neglect. Good to have the child on board.
TREAT with COURT ORDER. Parental medical neglect. The fact that the child agrees with parents is assumed to be not an independent decision.
Table 4: DECISION MAKING WITH AND ON BEHALF OF CHILDREN WITH RESPECT TO
EFFECTIVE LIFE-SAVING THERAPIES.
Table 4: DECISION MAKING WITH AND ON BEHALF OF CHILDREN WITH RESPECT TO
EFFECTIVE LIFE-SAVING THERAPIES.
Does not appear that patient/family opinions matter!Does not appear that patient/family opinions matter!
PA
RE
NT
S’ P
refe
renc
es
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
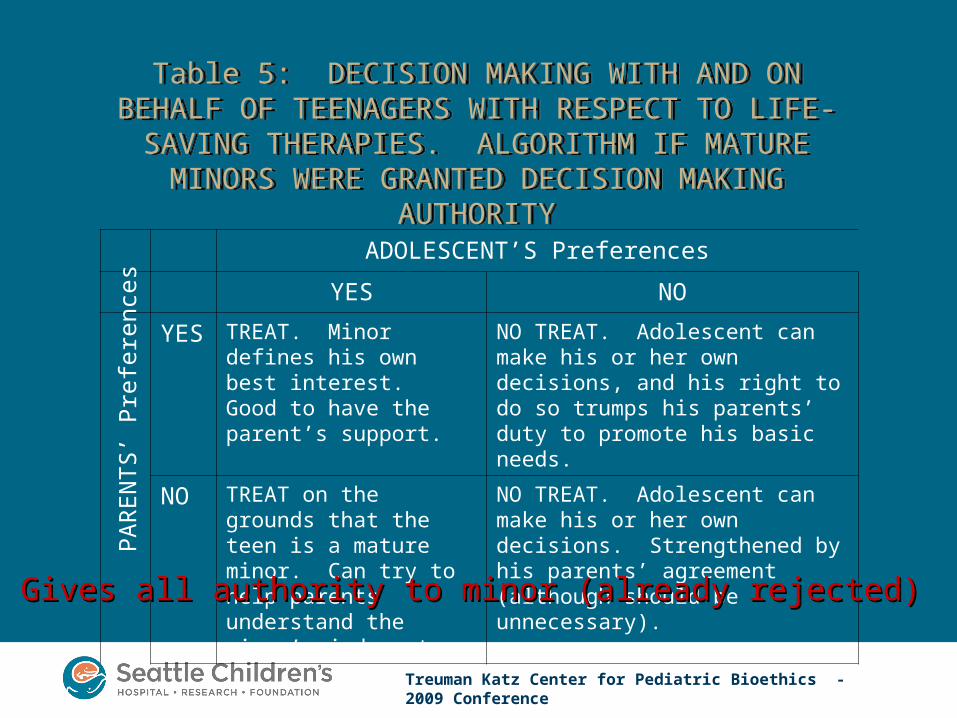
Table 5: DECISION MAKING WITH AND ON BEHALF OF TEENAGERS WITH RESPECT TO LIFE-SAVING
THERAPIES. ALGORITHM IF MATURE MINORS WERE GRANTED DECISION MAKING AUTHORITY
Table 5: DECISION MAKING WITH AND ON BEHALF OF TEENAGERS WITH RESPECT TO LIFE-SAVING
THERAPIES. ALGORITHM IF MATURE MINORS WERE GRANTED DECISION MAKING AUTHORITY
ADOLESCENT’S Preferences
YES NO
YES TREAT. Minor defines his own best interest. Good to have the parent’s support.
NO TREAT. Adolescent can make his or her own decisions, and his right to do so trumps his parents’ duty to promote his basic needs.
NO TREAT on the grounds that the teen is a mature minor. Can try to help parents understand the minor’s judgment.
NO TREAT. Adolescent can make his or her own decisions. Strengthened by his parents’ agreement (although should be unnecessary).
Gives all authority to minor (already rejected)Gives all authority to minor (already rejected)
PA
RE
NT
S’ P
refe
renc
es

Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Table 6: DECISION MAKING WITH AND ON BEHALF OF TEENAGERS WITH RESPECT TO EFFECTIVE LIFE-SAVING
THERAPIES. WHAT ACTUALLY HAPPENS.
Table 6: DECISION MAKING WITH AND ON BEHALF OF TEENAGERS WITH RESPECT TO EFFECTIVE LIFE-SAVING
THERAPIES. WHAT ACTUALLY HAPPENS.
ADOLESCENT’S Preferences
YES NO
YES TREAT: In the minor’s best interest (as determined by parents and minor)
TREAT. Parents define the minor’s best interest. Minor can avoid treatment by convincing parents or by running away.
NO TREAT Go to COURT on the grounds that parents are medically neglectful. Can also assert that the minor is acting as a mature minor.
TREAT /NO TREAT BASED ON COURT RULING. Argue to treat based on both 1) Parents are neglectful; and 2) that teen lacks decisional capacity to make an independent decision. Courts moving to respect the teenager’s decision. This is particularly true when the teen and parent agree.
The authority of both parents and adolescents is limited by State The authority of both parents and adolescents is limited by State Authority and the need to promote the minor’s “basic interests”Authority and the need to promote the minor’s “basic interests”
PA
RE
NT
S’ P
refe
ren
ces
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
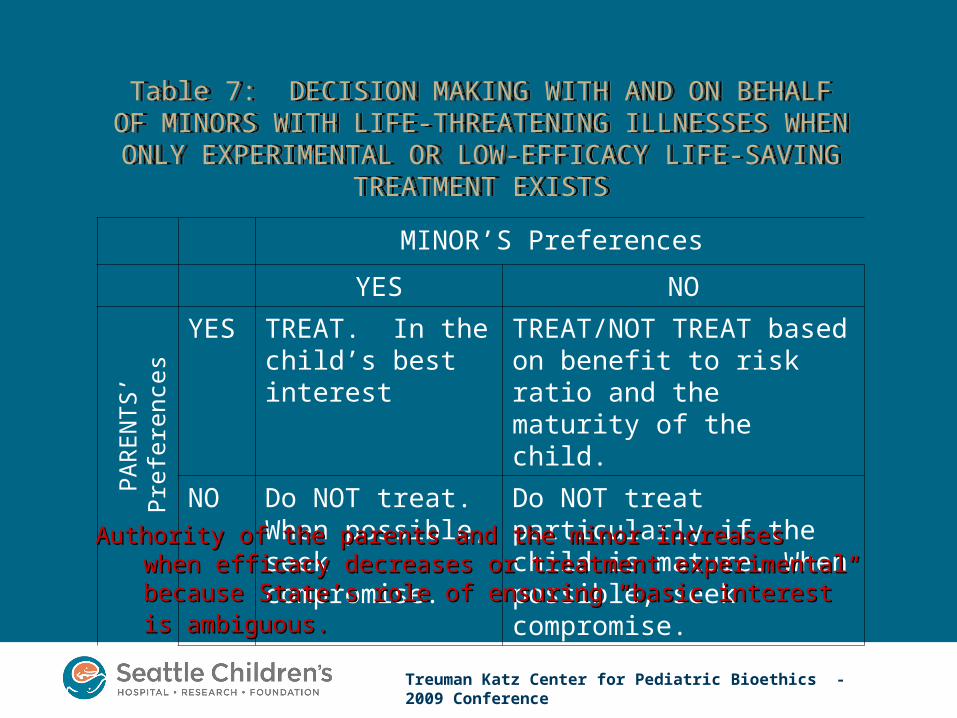
Table 7: DECISION MAKING WITH AND ON BEHALF OF MINORS WITH LIFE-THREATENING ILLNESSES WHEN
ONLY EXPERIMENTAL OR LOW-EFFICACY LIFE-SAVING TREATMENT EXISTS
Table 7: DECISION MAKING WITH AND ON BEHALF OF MINORS WITH LIFE-THREATENING ILLNESSES WHEN
ONLY EXPERIMENTAL OR LOW-EFFICACY LIFE-SAVING TREATMENT EXISTS
MINOR’S Preferences
YES NO
YES TREAT. In the child’s best interest
TREAT/NOT TREAT based on benefit to risk ratio and the maturity of the child.
NO Do NOT treat. When possible, seek compromise.
Do NOT treat particularly if the child is mature. When possible, seek compromise.
Authority of the parents and the minor increases when efficacy Authority of the parents and the minor increases when efficacy decreases or treatment experimental because State’s role of decreases or treatment experimental because State’s role of ensuring “basic interest” is ambiguous.ensuring “basic interest” is ambiguous.
PA
RE
NT
S’
Pre
fere
nces
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Do reasons matter?Do reasons matter?
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Consider, again, the 4 casesConsider, again, the 4 cases• In re E.G. (IL, 1989)
– Jehovah Witness: Refusal of blood.
• Billy Best (MA, 1994)– Born Again Christian: Wanted both CAM (complementary
and alternative medicine) and prayer.
• Starchild Abraham Cherrix (VA, 2006)– Religious beliefs are not mentioned; only the desire for
CAM.– Compromise of a combo of CAM and XRT
• Dennis Lindberg (WA, 2007)– Jehovah Witness: Refusal of blood
• In re E.G. (IL, 1989)– Jehovah Witness: Refusal of blood.
• Billy Best (MA, 1994)– Born Again Christian: Wanted both CAM (complementary
and alternative medicine) and prayer.
• Starchild Abraham Cherrix (VA, 2006)– Religious beliefs are not mentioned; only the desire for
CAM.– Compromise of a combo of CAM and XRT
• Dennis Lindberg (WA, 2007)– Jehovah Witness: Refusal of blood
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
And why the 5th case is differentAnd why the 5th case is different• Daniel Hauser’s family is Roman Catholic and
believes in the "do no harm" philosophy of the Nemenhah Band, a Missouri-based religious group that believes in natural healing methods. – The Nemenhah Band claims to be a group of American
Indian healers; however, their practices have been criticized by many Native Americans.
– Nemenhah group’s leader, Phillip Landis, has been convicted of fraud in two states for misleading investors in an alternative-health mushroom-growing business.
– On its website, the Nemenhah Band offers you the opportunity to be adopted into the band and become a natural healer for $250.
• Daniel Hauser’s family is Roman Catholic and believes in the "do no harm" philosophy of the Nemenhah Band, a Missouri-based religious group that believes in natural healing methods. – The Nemenhah Band claims to be a group of American
Indian healers; however, their practices have been criticized by many Native Americans.
– Nemenhah group’s leader, Phillip Landis, has been convicted of fraud in two states for misleading investors in an alternative-health mushroom-growing business.
– On its website, the Nemenhah Band offers you the opportunity to be adopted into the band and become a natural healer for $250.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Court-Mediated Disputes Between Physicians and Families over the Medical Care of Children by Derry Ridgway. Arch Pediatr Adolesc Med 2005; 15: 891-896.
Court-Mediated Disputes Between Physicians and Families over the Medical Care of Children by Derry Ridgway. Arch Pediatr Adolesc Med 2005; 15: 891-896.
• 65 judicial opinions from 50 identified disputes between 1912-1998.
• Impossible to count or characterize the relevant court decisions that are not accompanied by published opinions so it is not known how representative these 50 cases are.
• Impossible to count or characterize those cases that do not go to court.
• 65 judicial opinions from 50 identified disputes between 1912-1998.
• Impossible to count or characterize the relevant court decisions that are not accompanied by published opinions so it is not known how representative these 50 cases are.
• Impossible to count or characterize those cases that do not go to court.
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Court DecisionsCourt Decisions• Overall 80% of cases favored physicians.
– Did not change across time and was not affected by patient characteristics (age, sex, or disease).
• Physicians more likely to succeed against religious objections [27 of 30 or 90%] versus [13 of 20 or 65%]– Religious cases can cite Prince v Massachusetts which
states that parents can choose to be martyrs but they CANNOT make martyrs of their children.
• But remember: NOT all cases of refusals go to court. So whether refusals based on religion is more or less likely to go to court may determine to what extent “reasons matter”.
• Clearly some reasons will be easily overridden (a green Martian told me to refuse).
• Overall 80% of cases favored physicians.– Did not change across time and was not affected by
patient characteristics (age, sex, or disease).
• Physicians more likely to succeed against religious objections [27 of 30 or 90%] versus [13 of 20 or 65%]– Religious cases can cite Prince v Massachusetts which
states that parents can choose to be martyrs but they CANNOT make martyrs of their children.
• But remember: NOT all cases of refusals go to court. So whether refusals based on religion is more or less likely to go to court may determine to what extent “reasons matter”.
• Clearly some reasons will be easily overridden (a green Martian told me to refuse).
Treuman Katz Center for Pediatric Bioethics - 2009 Conference
Concluding ThoughtsConcluding Thoughts• The evolving position by many courts, state
legislatures, and health care providers to respect FAMILY REFUSALS in cases of life-threatening illness when an effective treatment exists is morally inconsistent with our obligation to protect and promote the basic medical needs of minors.
• Basic medical needs have lexical priority over other interests and needs, both present and future-regarding.
• When efficacy of treatment is low (how low is a more complicated problem) or treatment is experimental, the state should be more hesitant to override the family’s refusal because it is ambiguous whether treatment promotes the minor’s basic interests.
• The evolving position by many courts, state legislatures, and health care providers to respect FAMILY REFUSALS in cases of life-threatening illness when an effective treatment exists is morally inconsistent with our obligation to protect and promote the basic medical needs of minors.
• Basic medical needs have lexical priority over other interests and needs, both present and future-regarding.
• When efficacy of treatment is low (how low is a more complicated problem) or treatment is experimental, the state should be more hesitant to override the family’s refusal because it is ambiguous whether treatment promotes the minor’s basic interests.


















