
Trends in Susceptibility of Vancomycin-resistant...
21
Trends in Susceptibility of Vancomycin-resistant Enterococcus 1 faecium to Tigecycline, Daptomycin, and Linezolid and 2 Molecular Epidemiology of the Isolates: Results from the 3 Tigecycline In Vitro Surveillance in Taiwan (TIST) Study, 4 2006-2010 5 6 7 Hsih-Yeh Tsai 1 , Chun-Hsing Liao 1 , Yen-Hsu Chen 2 , Po-Liang Lu 2 , Cheng-Hua 8 Huang 3 , Chin-Te Lu 4 , Yin-Ching Chuang 5 , Shih-Ming Tsao 6 , Yao-Shen Chen 7 , 9 Yung-Ching Liu 7 , Wei-Yu Chen 8 , Tsrang-Neng Jang 8 , Hsiu-Chen Lin 9 , Chih-Ming 10 Chen 10 , Zhi-Yuan Shi 11 , Sung-Ching Pan 12 , Jia-Ling Yang 12 , Hsiang-Chi Kung 12 , 11 Chun-Eng Liu 13 ,Yu-Jen Cheng 13 , Jien-Wei Liu 14 , Wu Sun 15 , Lih-Shinn Wang 16 , 12 Wen-Chien Ko 17 , Kwok-Woon Yu 18 , Ping-Cherng Chiang 19 , Ming-Hsun Lee 19 , 13 Chun-Ming Lee 20 , Gwo-Jong Hsu 21 , Po-Ren Hsueh 1, 22 * 14 15 1 Section of Infectious Diseases, Department of Internal Medicine, Far Eastern 16 Memorial Hospital, Taiwan; 2 Division of Infectious Diseases, Department of Internal 17 Medicine, Kaohsiung Medical University Hospital; Graduate Institute of Medicine, 18 College of Medicine, Kaohsiung Medical University, Taiwan; 3 Division of Infectious 19 Diseases, Department of Internal Medicine, Cathay General Hospital, Taiwan 20 4 Section of Infectious Diseases, Department of Internal Medicine, Lotung Poh-Ai 21 Hospital, Taiwan; 5 Department of Internal Medicine, Chi-Mei Medical Center, 22 Taiwan; 6 Infectious Section, Internal Medicine Department, Institute Microbiology 23 and Immunology, Chung Shan Medical University, and University Hospital, Taiwan 24 7 Section of Infectious Diseases, Shuang Ho Hospital, Taipei Medical University and 25 Copyright © 2012, American Society for Microbiology. All Rights Reserved. Antimicrob. Agents Chemother. doi:10.1128/AAC.00533-12 AAC Accepts, published online ahead of print on 9 April 2012 on June 2, 2018 by guest http://aac.asm.org/ Downloaded from
Transcript of Trends in Susceptibility of Vancomycin-resistant...
Trends in Susceptibility of Vancomycin-resistant Enterococcus 1
faecium to Tigecycline, Daptomycin, and Linezolid and 2
Molecular Epidemiology of the Isolates: Results from the 3
Tigecycline In Vitro Surveillance in Taiwan (TIST) Study, 4
2006-2010 5
6
7
Hsih-Yeh Tsai1, Chun-Hsing Liao1, Yen-Hsu Chen2, Po-Liang Lu2, Cheng-Hua 8
Huang3, Chin-Te Lu4, Yin-Ching Chuang5, Shih-Ming Tsao6, Yao-Shen Chen7, 9
Yung-Ching Liu7, Wei-Yu Chen8, Tsrang-Neng Jang8, Hsiu-Chen Lin9, Chih-Ming 10
Chen10, Zhi-Yuan Shi11, Sung-Ching Pan12, Jia-Ling Yang12, Hsiang-Chi Kung12, 11
Chun-Eng Liu13,Yu-Jen Cheng13, Jien-Wei Liu14, Wu Sun15, Lih-Shinn Wang16, 12
Wen-Chien Ko17, Kwok-Woon Yu18, Ping-Cherng Chiang19, Ming-Hsun Lee19, 13
Chun-Ming Lee20, Gwo-Jong Hsu21, Po-Ren Hsueh1, 22* 14
15
1Section of Infectious Diseases, Department of Internal Medicine, Far Eastern 16
Memorial Hospital, Taiwan; 2Division of Infectious Diseases, Department of Internal 17
Medicine, Kaohsiung Medical University Hospital; Graduate Institute of Medicine, 18
College of Medicine, Kaohsiung Medical University, Taiwan; 3Division of Infectious 19
Diseases, Department of Internal Medicine, Cathay General Hospital, Taiwan 20
4Section of Infectious Diseases, Department of Internal Medicine, Lotung Poh-Ai 21
Hospital, Taiwan; 5Department of Internal Medicine, Chi-Mei Medical Center, 22
Taiwan; 6Infectious Section, Internal Medicine Department, Institute Microbiology 23
and Immunology, Chung Shan Medical University, and University Hospital, Taiwan 24
7Section of Infectious Diseases, Shuang Ho Hospital, Taipei Medical University and 25
Copyright © 2012, American Society for Microbiology. All Rights Reserved.Antimicrob. Agents Chemother. doi:10.1128/AAC.00533-12 AAC Accepts, published online ahead of print on 9 April 2012
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

School of Medicine, Taipei Medical University, Taipei; and Section of Infectious 26
Diseases, Department of Internal Medicine, Kaohsiung Veterans General Hospital, 27
Kaohsiung, Taiwan; 8Section of Infectious Diseases, Department of Internal Medicine, 28
Shin Kong Wu Ho-Su Memorial Hospital, Taiwan; 9Department of Pediatrics, School 29
of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 30
10Section of Infectious Diseases, Department of Internal Medicine, Tungs' Taichung 31
MetroHarbor Hospital, Taiwan; 11Section of Infectious Diseases, Department of 32
Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 33
12Department of Internal Medicine, National Taiwan University Hospital, Taipei, 34
Taiwan; 13Section of Infectious Diseases, Department of Internal Medicine, 35
Changhua Christian Hospital, Taiwan; 14Division of Infectious Diseases, Department 36
of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Chang Gung 37
University Medical College, Taiwan; 15Department of Infection Control, Pao-Chien 38
Hospital, Taiwan; 16Section of Infectious Diseases, Department of Internal Medicine, 39
Buddhist Tzu Chi General Hospital, Taiwan; 40
17Department of Medicine, National Cheng Kung University Medical College and 41
Hospital, Taiwan; 18Division of Infectious Diseases, Department of Internal Medicine, 42
Pathology and Laboratory Medicine, Taipei Veterans General Hospital, Taiwan; 43
19Division of Infectious Diseases, Department of Internal Medicine, Chang Gung 44
Medical Foundation Linkou Branch, Taiwan; 20Section of Infectious Diseases, 45
Department of Internal Medicine, Mackay Memorial Hospital 46
21Division of Infectious Diseases, Department of Internal Medicine, Ditmanson 47
Medical Foundation Chiayi Christian Hospital, Taiwan; 22Departments of Laboratory 48
Medicine and Internal Medicine, National Taiwan University Hospital, National 49
Taiwan University College of Medicine, Taipei, Taiwan 50
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
*Corresponding author. Mailing address: Departments of Laboratory Medicine and 51
Internal Medicine, National Taiwan University Hospital, No.7, Chung-Shan South 52
Road, Taipei 100, Taiwan. Phone: 886-2-23123456, ext. 65355. Fax: 886-2-23224263. 53
E-mail: [email protected]. 54
55
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
Among the 219 vancomycin-resistant Enterococcus faecium isolates collected in 56
20 Taiwanese hospitals from 2006 to 2010, all were susceptible to linezolid and 57
daptomycin, and 98.6% were susceptible to tigecycline. There was a shift 58
towards higher tigecycline MIC values (MIC90s) from 2006-2007 (0.06 μg/ml) to 59
2008-2010 (0.12 μg/ml). The MIC90s of daptomycin and linezolid remained 60
stationary. Although pulsotypes among the isolates from the 20 hospitals varied, 61
intra-hospital spreading of several clones was identified in 13 hospitals. 62
63
64
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
65
Enterococcus species were first isolated in a patient with endocarditis in the early 66
1900s (15) and have been recognized as an important cause of nosocomial urinary 67
tract infection and bacteremia since the mid 1970s (4). Penicillin, ampicillin and 68
aminoglycosides are the drug of first-line choice of choice for the treatment of 69
enterococcal infection. Glycopeptides are effective antibiotics for the treatment of 70
infections due to beta-lactam-resistant enterococci beginning in the 1980s (7). 71
However, the rate of isolation of vancomycin-resistant enterococci (VRE) strains is on 72
the rise in North America (17), Europe (2), and Asia (4). In Taiwan, a nationwide 73
surveillance study of antimicrobial resistance in patients admitted to intensive care 74
units clearly demonstrated a significant rise in VRE among regional hospitals and 75
medical centers during the period 2003 to 2009 (5). Specifically, at the National 76
Taiwan University Hospital, rates of VRE among all enterococci species causing 77
healthcare-associated infection significantly increased from 1.7% (0.007 per 100 78
inpatient-days) in 2000 to 25.1% (0.188 per 100 inpatient-days) in 2009 (14). Clonal 79
dissemination and the presence of multiple clones of VRE have also been reported in 80
hospitals in Taiwan (8, 9). Tigecycline, daptomycin, and linezolid are now the drugs 81
of choice for the treatment of infections due to VRE. However, the in vitro 82
susceptibilities of VRE species to these agents have been shown to vary with time and 83
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
between countries. Herein, we report the trends in in vitro susceptibility of 84
vancomycin-resistant E. faecium to tigecycline, daptomycin, and linezolid in Taiwan 85
during the period 2006 to 2010. 86
Clinical isolates of VRE were collected as part of the Tigecycline In Vitro 87
Surveillance in Taiwan (TIST) study, a nationwide, multi-center prospective 88
surveillance study conducted in 20 medical centers and regional hospitals throughout 89
Taiwan during the period January 2006 to December 2010 (5). Duplicate isolates from 90
the same patients were excluded (one isolate per patient). Consecutive VRE isolates 91
during a three-month period per year from each participating hospital were collected 92
with a maximal number of isolates of 10 per hospital per year. These VRE isolates 93
were identified and vancomycin resistance was determined by the disk diffusion 94
method at each hospital and reconfirmed by the central laboratory at the National 95
Taiwan University Hospital (NTUH). Minimum inhibitory concentrations (MICs) of 96
three antimicrobial agents, namely tigecycline, daptomycin, and linezolid, were 97
determined using the broth microdilution method according to the guidelines of the 98
Clinical and Laboratory Standards Institute (CLSI) (6). Susceptibility testing for the 99
three agents was performed at the same central laboratory at NTUH using same type 100
of media, Mueller-Hinton broth (BBL Microbiology Systems, Cockeysville, MD), 101
and the same protocol every year. Susceptibilities to the three agents were classified 102
based on the U.S. Food and Drug Administration (FDA), the European Committee on 103
Antimicrobial Susceptibility Testing (EUCAST-2012; www.eucast.org), and CLSI 104
2012 breakpoints (6). 105
In order to understand the genetic relatedness of vancomycin-resistant E. faecium 106
isolates, particularly those with daptomycin MICs of 4 μg/ml, pulsed-field gel 107
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
electrophoresis (PFGE) profiles of SmaI-digested genomic DNAs of these isolates 108
were determined as previously described (9). 109
A total of 219 clinical isolates of vancomycin-resistant E. faecium were collected 110
from 20 hospitals during the five-year study period (Table 1). Numbers of clinical 111
isolates obtained from 2006 to 2010 were 13 in 2006, 15 in 2007, 41 in 2008, 78 in 112
2009, and 72 in 2010 (5). Susceptibility of vancomycin-resistant E. faecium to 113
tigecycline was 98.6% according to US FDA and EUCAST-2012 breakpoints (22). 114
The three VRE isolates that were less susceptible to tigecycline had tigecycline MICs 115
of 0.5, 0.5, and 1 μg/ml. All isolates were susceptible to daptomycin and linezolid 116
according to CLSI-2012 and EUCAST-2012 criteria (6). The MICs of daptomycin 117
were 2 μg/ml and the MICs of linezolid were 1-2 μg/ml for the three tigecycline 118
non-susceptible isolates. 119
The distributions of MIC values of the three agents against the 120
vancomycin-resistant E. faecium strains are shown in Table 2. MIC50 and MIC90 121
values of tigecycline, daptomycin, and linezolid against the clinical isolates were 122
≤0.03 μg/ml and 0.12 μg/ml (range, ≤0.03-1 μg/ml), 2 μg/ml and 2 μg/ml (range, 123
0.12-4 μg/ml), and 1 μg/ml and 2 μg/ml (range, 0.25-2 μg/ml), respectively. There 124
was a shift towards higher tigecycline MIC values from 2006-2007 (MIC90 of 0.06 125
μg/ml) to 2008-2010 (MIC90 of 0.12 μg/ml) (Figure 1A). The MIC values of 126
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
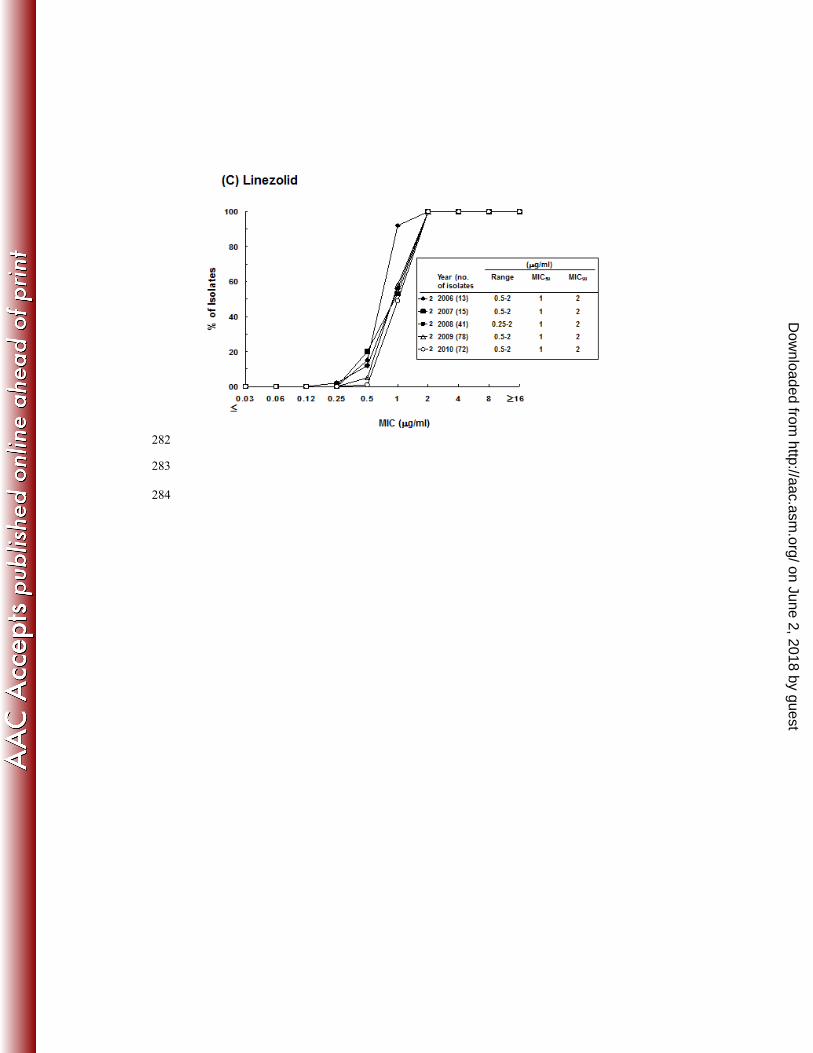
daptomycin and linezolid against the isolates remained stationary during the study 127
period (Figure 1B and 1C). 128
A total of 14 vancomycin-resistant E. faecium isolates were susceptible to 129
daptomycin with MICs of 4 μg/ml (Table 3). Those isolates were also susceptible to 130
tigecycline and linezolid. All of the isolates were susceptible to tigecycline at a 131
concentration of 0.06 μg/ml, and nine of the 14 clinical isolates were susceptible to 132
linezolid at a concentration of 2 μg/ml. 133
Even though the pulsotypes of the isolates varied among the 20 hospitals, 13 134
hospitals in Taiwan showed evidence of intra-hospital spreading of VRE isolates with 135
the same pulsotypes (Table 3). Thirteen pulsotypes were found among the 14 isolates 136
of vancomycin-resistant E. faecium with daptomycin MICs of 4 μg/ml, indicating the 137
absence of inter-hospital spreading of these strains among Taiwanese hospitals (Figure 138
2). 139
Although the incidence of infection due to VRE has risen in recent years in many 140
countries (1, 15), the incidence of VRE in Taiwan remains relatively low (3-7%) (15), 141
especially compared to the incidence of hospital-acquired VRE infection in the United 142
States (28%).VRE species are recovered from colonized rather than infected patients 143
in many institutions (24), but VRE infection is associated with higher recurrence and 144
mortality (21). In addition, the treatment regimens for VRE infections are limited to 145
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
tigecycline, daptomycin, and linezolid. However, only a few reports regarding the 146
antimicrobial susceptibility of VRE isolates to these antibiotics in certain hospitals in 147
Taiwan have been published (10, 11), and no nationwide surveillance studies of 148
susceptibility of VRE species to the above-mentioned antimicrobial agents have been 149
conducted. 150
In this study, we found that all clinical isolates of VRE were susceptible to 151
daptomycin and linezolid, and that almost all VRE isolates (98.6%) were susceptible 152
to tigecycline. Studies conducted in Europe and the United States demonstrated 153
similar findings (3, 18-20). Daptomycin non-susceptible enterococci may be an 154
emerging clinical problem in other countries (12), but they were not identified in our 155
study. In this study, the reason why the VRE isolates with daptomycin MICs of 4 156
μg/ml were selected for molecular typing to elucidate the possible clonal spreads 157
because there are concerns about achieving adequate concentrations of daptomycin 158
using standard doses (≤ 6 mg/kg) when the MICs of the isolates approach the upper 159
end (4 μg/ml) of the susceptible range (13). Higher doses of daptomycin may be 160
needed to treat infections caused by VRE isolates with higher MICs (3-4 μg/ml), 161
although there was no significant difference in time to microbiological cure between 162
MIC subgroups of ≤ 2 μg/ml versus >2 and ≤4 μg/ml of VRE isolates causing 163
bacteremia (13). We found that there was no marked increase in the trend of resistance 164
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
to daptomycin and linezolid; however, we did find that there was an increase in 165
resistance to tigecycline during the study period relative to the trend in resistance rates 166
reported previously in Taiwan (10, 11). 167
In conclusion, tigecycline, daptomycin, and linezolid remain active against VRE 168
isolates. Nonetheless, the emerging resistance of VRE to these agents should be 169
monitored. Inter-hospital spreads of VRE among Taiwanese hospitals were not 170
evident, however, intra-hospital dissemination of several VRE clones was found in 171
several hospitals. 172
173
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
References 174
1. Ben, R. J., J. J. Lu, T. G. Young, W. M. Chi, C. C. Wang, M. L. Chu, and J. 175
C. Wang. 1996. Clinical isolation of vancomycin-resistant Enterococcus 176
faecalis in Taiwan. J Formos Med Assoc 95:946-949. 177
2. Bonten, M. J. M., R. Willems, and R. A. Weinstein. 2001. 178
Vancomycin-resistant enterococci: why are they here, and where do they come 179
from? Lancet Infect. Dis. 1:314-325. 180
3. Bourdon, N., M. Fines-Guyon, J. M. Thiolet, S. Maugat, B. Coignard, R. 181
Leclercq, and V. Cattoir. 2011. Changing trends in vancomycin-resistant 182
enterococci in French hospitals, 2001-08. J. Antimicrob. Chemother. 183
66:713-721. 184
4. Cetinkaya Y, F. P., and C. G. Mayhall. 2000. Vancomycin-resistant 185
enterococci. Clin. Microbiol. Rev. 13:686-707. 186
5. Chen, Y. H., P. L. Lu, C. H. Huang, C. H. Liao, C. T. Lu, Y. C. Chuang, S. 187
M. Tsao, Y. S. Chen, Y. C. Liu, W. Y. Chen, T. N. Jang, H. C. Lin, C. M. 188
Chen, Z. Y. Shi, S. C. Pan, C. L. Yang, H. C. Kung, C. E. Liu, Y. J. Cheng, 189
J. W. Liu, W. Sun, L. S. Wang, W. C. Ko, K. W. Yu, P. C. Chiang, M. H. 190
Lee, C. M. Lee, G. J. Hsu, and P. R. Hsueh. 2011. Trends in the 191
Susceptibility of Clinically Important Resistant Bacteria to Tigecycline: 192
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
Results from the Tigecycline In-vitro Surveillance in Taiwan (TIST), 193
2006-2010. Antimicrob. Agents Chemother. [Epub ahead of print]. 194
6. Clinical and Laboratory Standards Institute. 2012. Performance standards 195
for antimicrobial susceptibility testing; 22nd informational supplement. CLSI 196
document M100-S20. Clinical and Laboratory Standards Institute, Wayne, PA. 197
7. Grayson, M. L., G. M. Eliopoulos, C. B. Wennersten, K. L. Ruoff, P. C. De 198
Girolami, M. J. Ferraro, R. C. Moellering Jr. 1991. Increasing resistance to 199
beta-lactam antibiotics among clinical isolates of Enterococcus faecium: a 200
22-year review at one institution. Antimicrob. Agents Chemother. 201
35:2180-2184. 202
8. Hsieh, Y. C., W. S. Lee, T. Y. Ou, and P. R. Hsueh. 2010. Clonal spread of 203
CC17 vancomycin-resistant Enterococcus faecium with multilocus sequence 204
type 78 (ST78) and a novel ST444 in Taiwan. Eur. J. Clin. Microbiol. Infect. 205
Dis. 29:25-30. 206
9. Hsueh, P. R., L. J. Teng, H. J. Pan, Y. C. Chen, L. H. Wang, S. C. Chang, S. 207
W. Ho, and K. T. Luh. 1999. Emergence of vancomycin-resistant enterococci 208
at a university hospital in Taiwan: persistence of multiple species and multiple 209
clones. Infect. Control Hosp. Epidemiol. 20:828-833. 210
10. Hsueh, P. R., W. H. Chen, L. J. Teng, and K. T. Luh. 2005. Nosocomial 211
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
infections due to methicillin-resistant Staphylococcus aureus and 212
vancomycin-resistant enterococci at a university hospital in Taiwan from 1991 213
to 2003: resistance trends, antibiotic usage and in vitro activities of newer 214
antimicrobial agents. Int. J. Antimicrob. Agents 26:43-49. 215
11. Huang, Y. T., C. H. Liao, L. J. Teng, and P. R. Hsueh. 2008. Comparative 216
bactericidal activities of daptomycin, glycopeptides, linezolid and tigecycline 217
against blood isolates of Gram-positive bacteria in Taiwan. Clin. Microbiol. 218
Infect. 14:124-129. 219
12. Kelesidis, T., R. Humphries, D. Z. Uslan, and D. A. Pegues. 2010. 220
Daptomycin nonsusceptible enterococci: an emerging challenge for clinicians. 221
Clin. Infect. Dis. 52:228-234. 222
13. King, E. A., D. McCoy, S. Desai, T. Nyirenda, and K. Bicking K. 2011. 223
Vancomycin-resistant enterococcal bacteraemia and daptomycin: are higher 224
doses necessary? J. Antimicrob. Chemother. 66:2112-2118. 225
14. Lai, C. C., C. Y. Wang, C. C. Chu, C. K. Tan, C. L. Lu, Y. L. Lee, Y. T. 226
Huang , P. I. Lee, and P. R. Hsueh. 2011. Correlation between antimicrobial 227
consumption and resistance among Staphylococcus aureus and enterococci 228
causing healthcare-associated infections at a university hospital in Taiwan 229
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
from 2000 to 2009. Eur. J. Clin. Microbiol. Infect. Dis. 30:265-271. 230
15. Lo, W. T., W.-J. Lin, T. S. Chiueh, S. Y. Lee, C. C. Wang, and J. J. Lu. 231
2011. Changing trends in antimicrobial resistance of major bacterial pathogens, 232
1985–2005: A study from a medical center in northern Taiwan. J. Microbiol. 233
Immunol. Infect. 44:131-138. 234
16. Murray, B. E. 1990. The life and times of the Enterococcus. Clin. Microbiol. 235
Rev. 3:46-65. 236
17. Murry, B. E. 2000. Vancomycin-resistant enterococcal infections. N. Engl. J. 237
Med. 342:710-721. 238
18. Rathe, M., L. Kristensen, S. Ellermann-Eriksen, M. K. Thomsen, and H. 239
Schumacher. 2010. Vancomycin-resistant Enterococcus spp.: validation of 240
susceptibility testing and in vitro activity of vancomycin, linezolid, tigecycline 241
and daptomycin. APMIS 118:66-73. 242
19. Sader, H. S., G. J. Moet, D. J. Farrell, and R. N. Jones. 2011. Antimicrobial 243
susceptibility of daptomycin and comparator agents tested against 244
methicillin-resistant Staphylococcus aureus and vancomycin-resistant 245
enterococci: trend analysis of a 6-year period in US medical centers 246
(2005–2010). Diagn. Microbiol. Infect. Dis. 70:412-416. 247
20. Sader, H. S., J. M. Streit, T. R. Fritsche, and R. N. Jones. 2006. 248
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
Antimicrobial susceptibility of gram-positive bacteria isolated from European 249
medical centres: results of the Daptomycin Surveillance Programme 250
(2002-2004). Clin. Microbiol. Infect. 12:844-852. 251
21. Salgado, C. D., and B. M. Farr. 2003. Outcomes associated with 252
vancomycin-resistant enterococci: a meta-analysis. Infect. Control Hosp. 253
Epidemiol. 24:690-698. 254
22. Tseng, S. H., C. M. Lee, T. Y. Lin, S. C. Chang, F. Y. Chang. 2010. 255
Emergence and spread of multi-drug resistant organisms: think globally and 256
act locally. J. Microbiol. Immunol. Infect. 44:157-165. 257
23. Uttley, A. H., C. H. Collins, J. Naidoo, and R. C. George. 1988. 258
Vancomycin-resistant enterococci. Lancet 1:57-8. 259
24. Wang, J. L., and P. R. Hsueh. 2009. Therapeutic options for infections due to 260
vancomycin-resistant enterococci. Expert Opin. Pharmacother. 10:785-796. 261
262
263
264
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
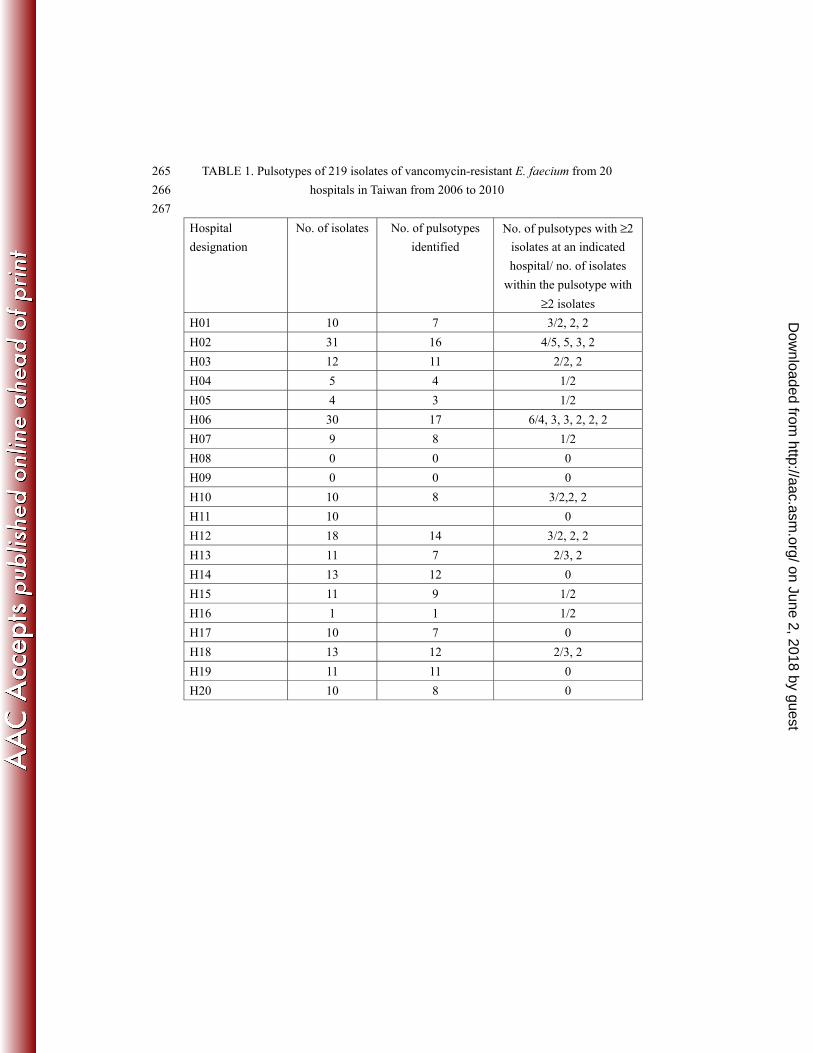
TABLE 1. Pulsotypes of 219 isolates of vancomycin-resistant E. faecium from 20 265
hospitals in Taiwan from 2006 to 2010 266
267
Hospital
designation
No. of isolates No. of pulsotypes
identified
No. of pulsotypes with ≥2
isolates at an indicated
hospital/ no. of isolates
within the pulsotype with
≥2 isolates
H01 10 7 3/2, 2, 2
H02 31 16 4/5, 5, 3, 2
H03 12 11 2/2, 2
H04 5 4 1/2
H05 4 3 1/2
H06 30 17 6/4, 3, 3, 2, 2, 2
H07 9 8 1/2
H08 0 0 0
H09 0 0 0
H10 10 8 3/2,2, 2
H11 10 0
H12 18 14 3/2, 2, 2
H13 11 7 2/3, 2
H14 13 12 0
H15 11 9 1/2
H16 1 1 1/2
H17 10 7 0
H18 13 12 2/3, 2
H19 11 11 0
H20 10 8 0
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
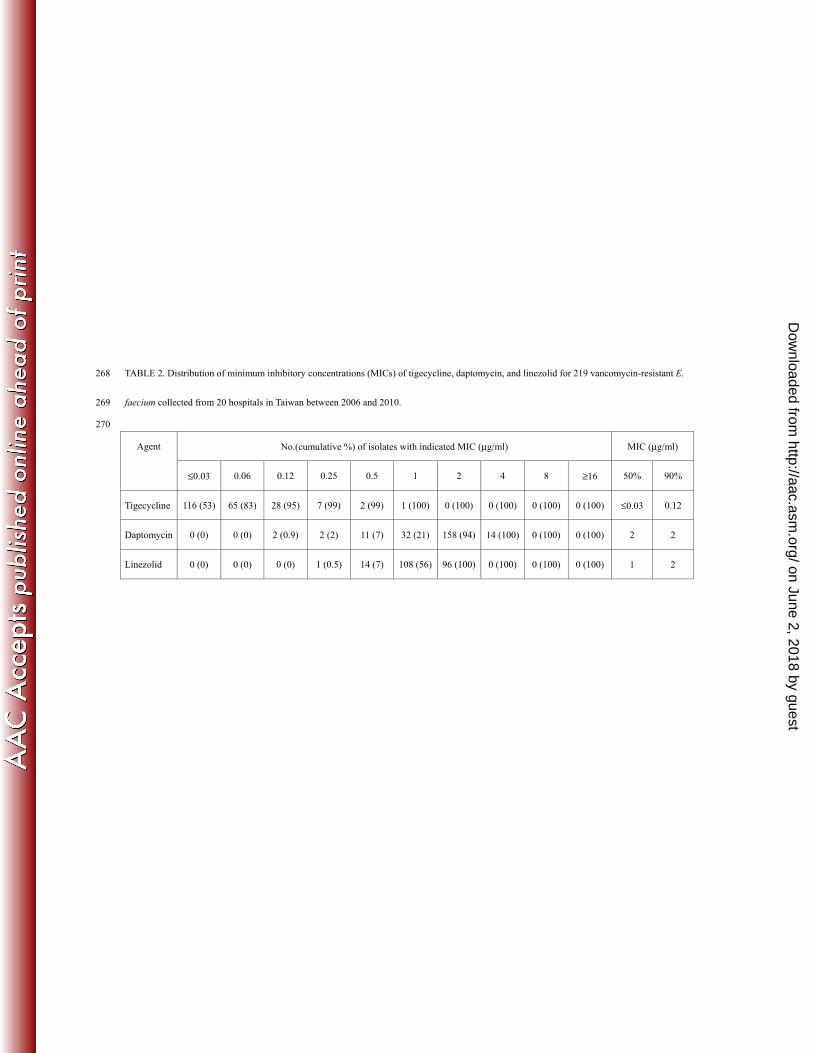
TABLE 2. Distribution of minimum inhibitory concentrations (MICs) of tigecycline, daptomycin, and linezolid for 219 vancomycin-resistant E. 268
faecium collected from 20 hospitals in Taiwan between 2006 and 2010. 269
270
Agent No.(cumulative %) of isolates with indicated MIC (μg/ml) MIC (μg/ml)
≤0.03 0.06 0.12 0.25 0.5 1 2 4 8 ≥16 50% 90%
Tigecycline 116 (53) 65 (83) 28 (95) 7 (99) 2 (99) 1 (100) 0 (100) 0 (100) 0 (100) 0 (100) ≤0.03 0.12
Daptomycin 0 (0) 0 (0) 2 (0.9) 2 (2) 11 (7) 32 (21) 158 (94) 14 (100) 0 (100) 0 (100) 2 2
Linezolid 0 (0) 0 (0) 0 (0) 1 (0.5) 14 (7) 108 (56) 96 (100) 0 (100) 0 (100) 0 (100) 1 2
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
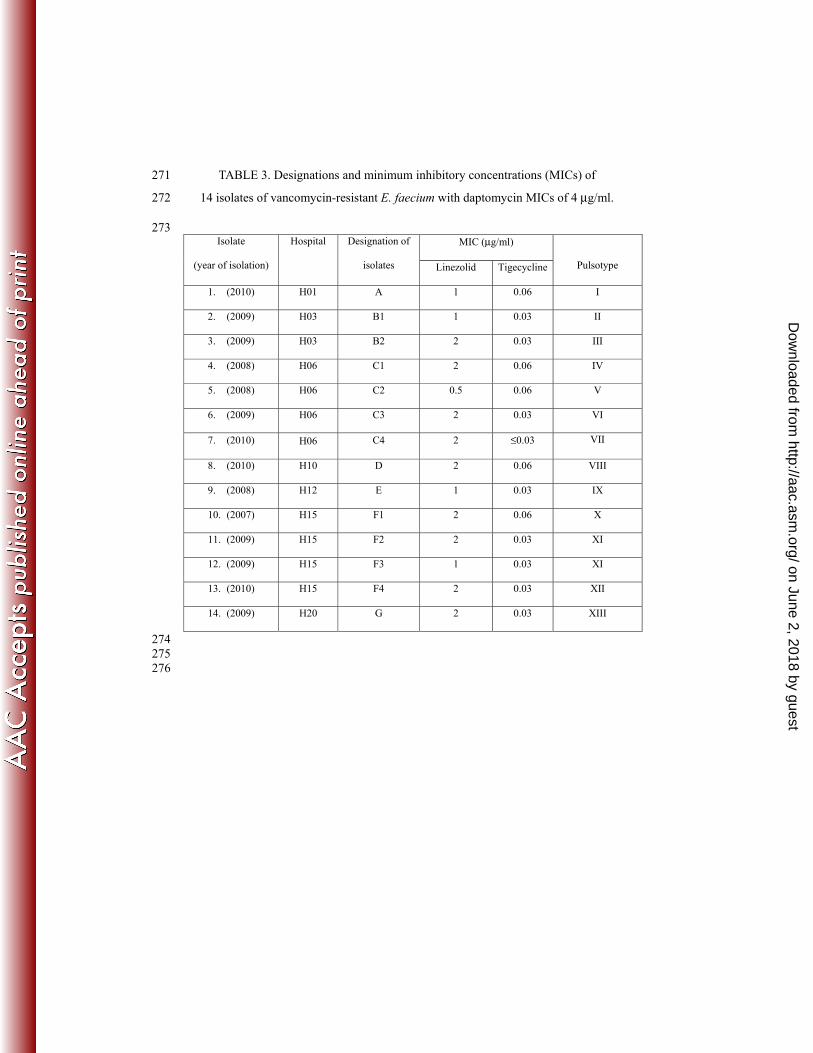
TABLE 3. Designations and minimum inhibitory concentrations (MICs) of 271
14 isolates of vancomycin-resistant E. faecium with daptomycin MICs of 4 μg/ml. 272
273 Isolate
(year of isolation)
Hospital Designation of
isolates
MIC (μg/ml)
Pulsotype Linezolid Tigecycline
1. (2010) H01 A 1 0.06 I
2. (2009) H03 B1 1 0.03 II
3. (2009) H03 B2 2 0.03 III
4. (2008) H06 C1 2 0.06 IV
5. (2008) H06 C2 0.5 0.06 V
6. (2009) H06 C3 2 0.03 VI
7. (2010) H06 C4 2 ≤0.03 VII
8. (2010) H10 D 2 0.06 VIII
9. (2008) H12 E 1 0.03 IX
10. (2007) H15 F1 2 0.06 X
11. (2009) H15 F2 2 0.03 XI
12. (2009) H15 F3 1 0.03 XI
13. (2010) H15 F4 2 0.03 XII
14. (2009) H20 G 2 0.03 XIII
274 275
276
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
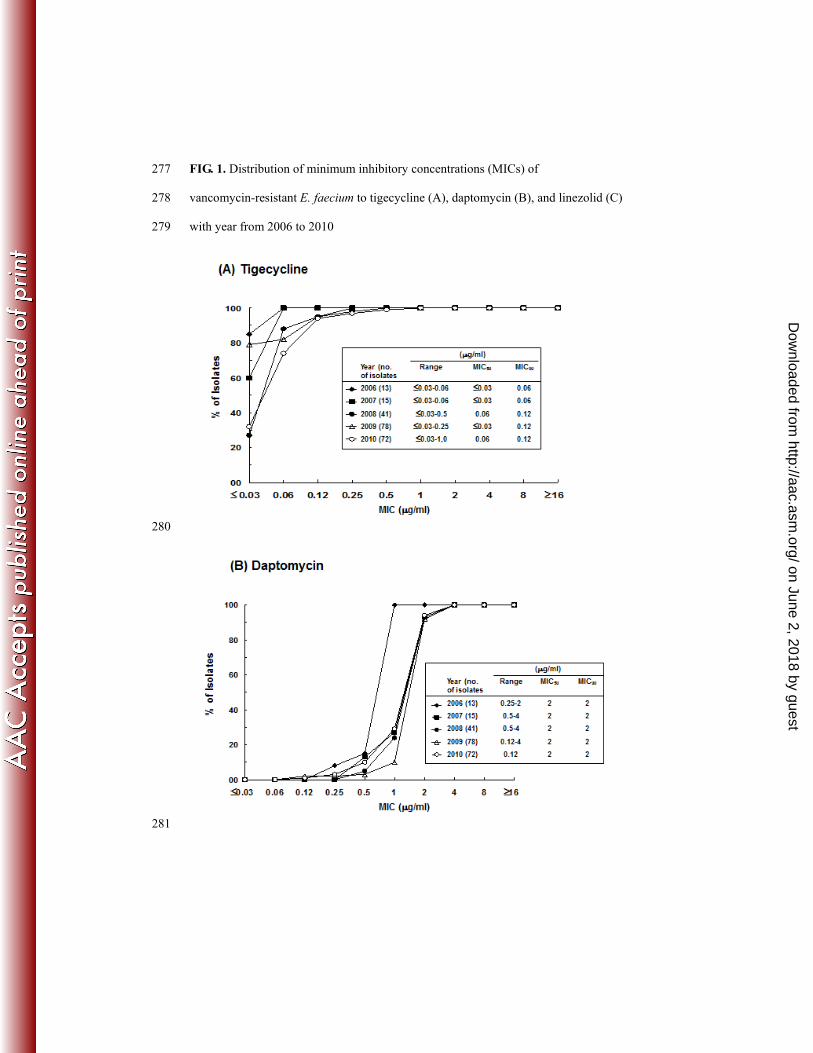
FIG. 1. Distribution of minimum inhibitory concentrations (MICs) of 277
vancomycin-resistant E. faecium to tigecycline (A), daptomycin (B), and linezolid (C) 278
with year from 2006 to 2010 279
280
281
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
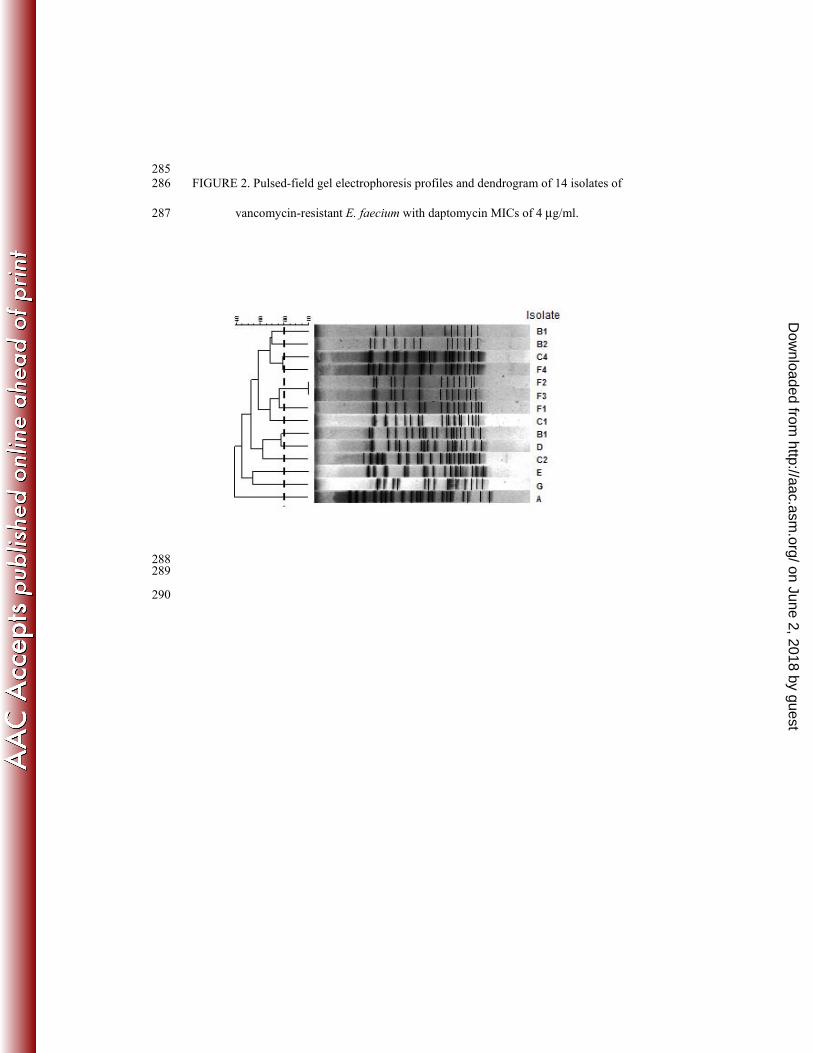
285 FIGURE 2. Pulsed-field gel electrophoresis profiles and dendrogram of 14 isolates of 286
vancomycin-resistant E. faecium with daptomycin MICs of 4 μg/ml. 287
288 289
290
on June 2, 2018 by guesthttp://aac.asm
.org/D
ownloaded from


















