Treatment with 131I - · PDF fileEnforcement Action Example 1 ... of 88 patients with GO...
102
-
Upload
trinhnguyet -
Category
Documents
-
view
216 -
download
0
Transcript of Treatment with 131I - · PDF fileEnforcement Action Example 1 ... of 88 patients with GO...

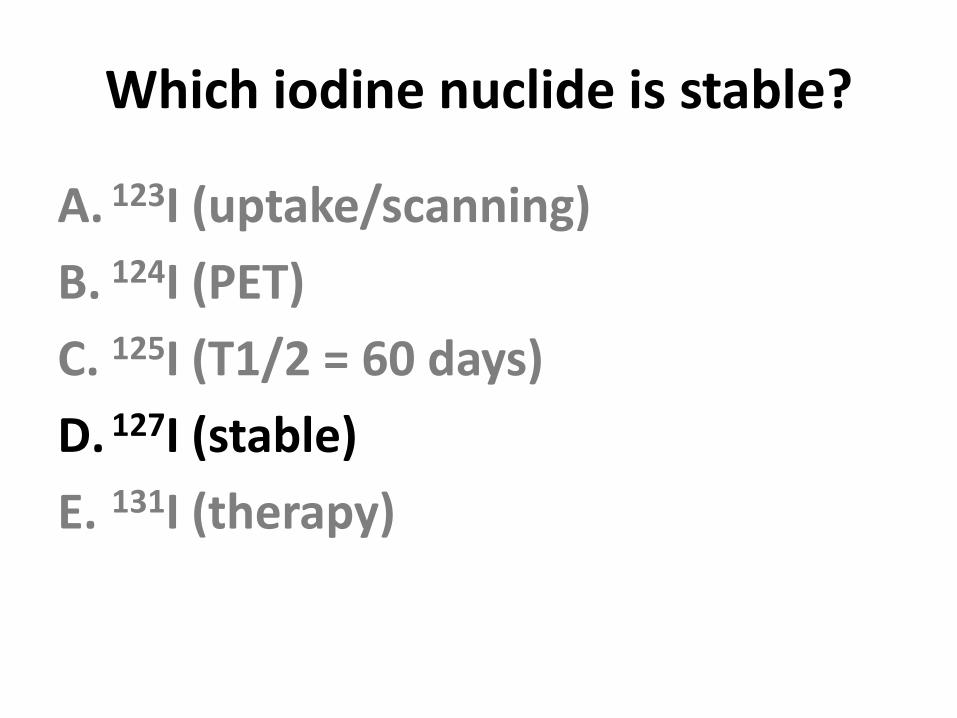
Which iodine nuclide is stable?
A. 123I
B. 124I
C. 125I
D. 127I
E. 131I
Which iodine nuclide is stable?
A. 123I (uptake/scanning)
B. 124I (PET)
C. 125I (T1/2 = 60 days)
D. 127I (stable)
E. 131I (therapy)

124I PET/CT
Clin Nucl Med 2013;38: 770-777
Nodular goiter

124I PET/CT
Clin Nucl Med 2013;38: 770-777
Toxic nodular goiter

124I PET/CT
Clin Nucl Med 2013;38: 770-777
Toxic multinodular goiter

What percent of 131I is typically absorbed from the GI tract?
A. 25%
B. 50%
C. 75%
D. 100%

What percent of 131I is typically absorbed from the GI tract?
A. 25%
B. 50%
C. 75%
D. 100%
Must assume that 100% of 131I is absorbed in order for thyroid uptakes to make sense without correcting for % absorption.

When the Radiologic Health Branch visits your practice, what 131I
documentation do they ask for?
A. Informed consents
B. Patients’ mR/min @ 1 m
C. Pregnancy test results
D. Written directives

When the Radiologic Health Branch visits your practice, what 131I
documentation do they ask for?
A. Informed consents
B. Patients’ mR/min @ 1 m
C. Pregnancy test results
D. Written directives

What is the cut-off dose for the requirement for a written directive?
A. 30 µCi
B. 5 mCi
C. 30 mCi
D. 33 mCi

What is the cut-off dose for the requirement for a written directive?
A. 30 µCi
B. 5 mCi
C. 30 mCi
D. 33 mCi
§ 35.40 Written Directives The AU must sign and date the WD before administering: • 131I > 30 uCi • Any therapeutic dosage of
unsealed radioactive material • Any therapeutic dose of
radiation from solid or sealed radioactive material

Violations Associated with Written Directives
• Most common violations pertain to Procedures for Administrations Requiring a Written Directive (§35.41)

How long must written directive records be maintained?
A. 1 year
B. 3 years
C. 7 years
D. Indefinitely

How long must written directive records be maintained?
A. 1 year
B. 3 years
C. 7 years
D. Indefinitely
All written directives must be kept on file for 3 years (10 CFR 35.2040) Licensee must retain a copy of the WD procedures for 3 years (10 CFR 35.2041)

Enforcement Action Example 1 • On May 12, 2008, a Notice of Violation
issued for a Severity Level III violation, involved two written directives not dated and signed by an authorized user before the administration of 131I >30 uCi.
• Specifically, on April 30, 2007, two nuclear medicine technologists administered 131I to two patients, without a dated and signed written directive.
www.nrc.gov/reading-rm/doc-collections/enforcement/actions/materials/

Enforcement Action Example 2
• On June 2, 2010, the NRC issued a Notice of Violation and Proposed Imposition of Civil Penalty in the amount of $14,000 to the Department of Veterans Affairs for two Severity Level III violations identified as a result of a medical event that occurred at the San Diego Healthcare System facility

• The medical event resulted when 131I was injected into the wrong port of the g-tube resulting in an underdose to the patient’s thyroid and an unintended dose to the patient’s stomach.
• Specifically, the licensee’s written procedures did not include directions for administering byproduct material through a g-tube to ensure that the administered dose was in accordance with the written directive as required by 10 CFR 35.41(a)(2).
www.nrc.gov/reading-rm/doc-collections/enforcement/actions/materials/

Inject here
Not here!
X
Administering liquid Na131I via g-tube

How long after receiving 100 mCi of 131I might a patient trigger an airport alarm?
A. 8 days
B. 30 days
C. 80 days
D. 95 days

How long after receiving 100 mCi of 131I might a patient trigger an airport alarm?
A. 8 days
B. 30 days
C. 80 days
D. 95 days
Zuckier L, et al. Sensitivity of personal homeland security radiation detectors to medical radionuclides and implications for counseling of nuclear medicine patients. Radiological Society of North America (RSNA) (Abstract). 2004. 2011
Radionuclide Days
Fluorine-18 1
Technetium-99m 3
Iodine-123 3
Indium-111 14
Gallium-67 30
Thallium-201 30
Iodine-131 95

Assuming T1/2 = 8 days, what fraction of 131I remains at 95 days?
A. 8/95
B. 98/95)2
C. (0.5)8/95
D. (0.5)95/8

Assuming T1/2 = 8 days, what fraction of 131I remains at 95 days?
A. 8/95
B. 98/95)2
C. (0.5)8/95
D. (0.5)95/8
• A(t) = Aoe – (0.693/T½) * time
• A(t)/Ao = e – (0.693/8) * 95
• A(t) = ?
• Or;
• A(t)/Ao = (0.5) time/T½
• A(t)/Ao = (0.5)95/8
• A(t)/Ao = ?

Assuming T1/2 = 8 days, what fraction of 131I remains at 95 days?
A. 8/95
B. 98/95)2
C. (0.5)8/95
D. (0.5)95/8
• A(t)/Ao = (0.5) time/T½
• A(t)/Ao = (0.5)95/8
• A(t)/Ao = ?
Hint: In Google, type in .5^(95/8)=

Assuming T1/2 = 8 days, what fraction of 131I remains at 95 days?
A. 8/95
B. 98/95)2
C. (0.5)8/95
D. (0.5)95/8
• A(t) = Aoe – (0.693/T½) * time
• A(t)/Ao = e – (0.693/8) * 95
• A(t) = 0.000266
• Or;
• A(t)/Ao = (0.5) time/T½
• A(t)/Ao = (0.5)95/8
• A(t)/Ao = 0.000266
Airport security detects < 30 uCi !

Detection of 131I in a patient with thyroid cancer by internal radiation exposure screening using a whole
body counter in Fukushima
• Woman 78yr in Soma City, 40km north of the Fukushima Daiichi nuclear power plant, 1st 131I+ case at 2 years post.
Clinical Nuclear Medicine. 39(3):281-282, March 2014.

Patient is unable to swallow solids. How should 131I be administered?
A. Aerosolized
B. Intravenous
C. Liquid
D. MiniCaps

Patient is unable to swallow solids. How should 131I be administered?
A. Aerosolized
B. Intravenous
C. Liquid
D. MiniCaps
Depending on the patient and product availability, either liquid 131I or “MiniCaps 131I may be considered.
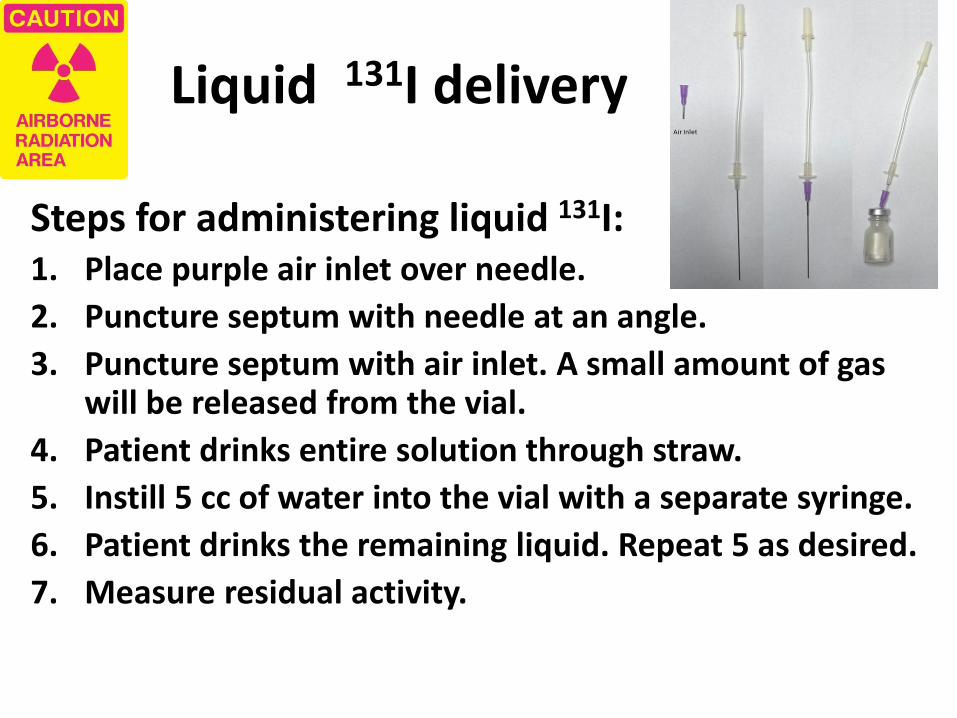
Liquid 131I delivery
Steps for administering liquid 131I: 1. Place purple air inlet over needle.
2. Puncture septum with needle at an angle.
3. Puncture septum with air inlet. A small amount of gas will be released from the vial.
4. Patient drinks entire solution through straw.
5. Instill 5 cc of water into the vial with a separate syringe.
6. Patient drinks the remaining liquid. Repeat 5 as desired.
7. Measure residual activity.

131I MiniCaps • MiniCaps are 25% of the volume
of traditional 131I capsules. (#3 capsule- 1/8” by 5/8”)
• May contain up to 200 mCi.
• Compounded to USP standards.

Hyperthyroidism: Causes • Graves
• Autonomous nodule
• Hashimoto
• Subacute thyroiditis
• Postpartum thyroiditis
• Pituitary TSH adenoma
• Stroma ovarii
• Jod-Basedow (Contrast agents, amiodarone)
• Fictitious Hyperthyroidism. The American Thyroid Association. http://www.thyroid.org/what-is-hyperthyroidism

Stroma Ovarii
36 year old hyperthyroid woman with a right adnexal mass

Hyperthyroidism: Treatments Medical therapy
• Beta blockers: Propranolol, 20–40 mg qid or Atenolol, 25–50 mg qd
• Thionamides (Agranulocytosis < 1%)
– Methimazole preferred over propylthiouracil (lower hepatotoxicity).
– Dosages depend on hyperthyroidism severity.
Radioiodine 131I
Surgery

Graves
• Hyperthyroidism
• Goiter
• Ophthalmopathy
• Pretibial myxedema
• Anti-TSH Receptor Antibody (TRAb)
“Thyroid Inferno”

RIA for Hyperthyroidism
• Dose = D
• D = V x (100/U) x C
• D= I-131 activity (MBq) to be administered
• V= thyroid gland volume (ml)
• U= 24-h I-131 uptake (%)
• C= 3.7 or 7.4 MBq (1 or 2 mCi) /ml of thyroid

131I activity/gm vs mass
Willegaignon J, et al. Clin Nuc Med. 38:231-236, April 2013.

131I T1/2 effective
Willegaignon J, et al. Clin Nuc Med. In press.

Graves 131I Rx Outcomes
Santos RB, et al. Clin Nucl Med 2012;37: 241–244
10 mCi, n = 76
15 mCi, n = 52
• Thyroids >60 g had a 2.4 x less chance of remission (OR -2.4; 1.18–4.96).
• 11/128 had significant GO; none progressed on 1 month of 0.5 mg/kg prednisone.
p = 0.54
GO = Grave Opthalmopathy

Autonomous nodule
• Typically > 3 cm (15 g), may be 5+ cm (60 gm)
• Eventually necrose centrally
• Can be excised for cure
• Usually treat with 131I, 25+ mCi
Henry D Plummer

TSH Stimulation Test Autonomous Nodule
TSH stimulates only the normal thyroid
+TSH

Toxic Multinodular
Goiter
• Usually treat with 131I, 25+ mCi
• Surgery can treat hyperthyroidism and decompress neck structures.

Ronga G, et al. Clin Nucl Med. 2013;38: 349-353
Treatment of autonomous toxic nodules: 50 years of experience

Progressive Graves
Ophthalmopathy
• 15% of GO Rx’ed with 131I show progression
• Factors: cigarette smoking, severe hyperthyroidism (T3 >5 nmol/L), high TRAb, and uncontrolled hypothyroidism.
• po prednisone (0.3 to 0.5 mg/kg 1 to 3 days post-RAI, with tapering of the dose until withdrawal 3 months later)
NEJM 2009;360:994

Graves Ophthalmology Recommendations
• Ophthalmopathy worsened in 26 patients out of 88 patients with GO after RAI alone.
• None of 96 patients with GO plus prednisolone prophylaxis developed worsening of GO (RR 0·03; 95% CI 0·00–0·24).
• Additional precautions:
– Smoking cessation
– Correct thyroid function
Clinical Endocrinology (2008) 69, 943–950.

A woman, 36 with Graves disease and hyperthyroidism poorly controlled with carbimazole. Rx I-131 (20 mCi) 3 days later, she had a choking sensation, SOB, dysphagia, neck discomfort and swelling.
Full Title: Acute Neck Edema Following Iodine-131 Ablation of the Thyroid Clin Nucl Med. 2013;38:278-279.

Fetal Thyroid
47
20 week pregnancy
25 mCi 131I for autonomous nodule
Day 8
At 5 months, the fetal thyroid is significantly developed and the ratio of thyroid/body size is maximal.
http://doseinfo-radar.com/RADAR-INT-NM.html

Man 46, TSH 0.04, RIU 22%/30%:
A. Autonomous toxic nodule
B. Differentiated thyroid cancer
C. Hurthle cell tumor
D. Parathyroid adenoma

Man 46, TSH 0.04, RIU 22%/30%:
A. Autonomous toxic nodule
B. Differentiated thyroid cancer
C. Hurthle cell tumor
D. Parathyroid adenoma

What is the most important factor that affects the outcome of radioiodine therapy for Graves disease with hyperthyroidism?
1. 24 hour radioiodine uptake
2. Gland mass in grams
3. Presence of nodules
4. Ratio of 4 hour to 24 hour uptakes

What is the most important factor that affects the outcome of radioiodine therapy for Graves disease with hyperthyroidism?
1. 24 hour radioiodine uptake
2. Gland mass in grams
3. Presence of nodules
4. Ratio of 4 hour to 24 hour uptakes

53 year old hyperthyroid woman with large thyroid: Most likely diagnosis?
A. Grave disease B. Marine-Lenhart syndrome C. Plummer disease D. Toxic multinodular goiter
6 hr 59% 28 hr 66%
7 mo later, 6 hr 44% 22 hr 55%
Rx 131I 30 mCi

53 year old hyperthyroid woman with large thyroid: Most likely diagnosis?
A. Grave disease B. Marine-Lenhart syndrome C. Plummer disease D. Toxic multinodular goiter
6 hr 59% 28 hr 66%
7 mo later, 6 hr 44% 22 hr 55%
Rx 131I 30 mCi

53 year old hyperthyroid woman with large thyroid: Most likely diagnosis?
A. Grave disease B. Marine-Lenhart syndrome C. Plummer disease D. Toxic multinodular goiter
6 hr 59% 28 hr 66%
7 mo later, 6 hr 44% 22 hr 55%
Rx 131I 30 mCi
Marine –Lenhart syndrome is Graves plus autonomous hyper-functioning goiter

4 hyperthyroid patients
A. Amiodarone
B. Toxic nodule
C. Grave Disease
D. Marine-Lenhart

RIA for Hyperthyroidism: Summary
• Hyperthyroidism with Graves is effectively treated with 15 mCi of 131I.
• Toxic nodules are effectively treated with 16 to 30 mCi of 131I. 25+ mCi is favored in the US.
• While 131I retention is important, hyperthyroid tissue mass has the most impact on outcomes.
• Risks of 131I (15%) and benefits of steroid coverage for prevention of GO progression are debatable. GO patients must stop smoking.

“Current Concepts in Radio-Iodine Therapy for
Differentiated Thyroid Cancer”
Patrick M Colletti MD
Disclosures: None

What is the level of evidence supporting Rx of DCT with 131I?
A Strongly recommends based on good evidence that RAI can improve important health
outcomes. Evidence includes consistent results from well-designed, well-conducted
studies in representative populations that directly assess effects on health outcomes.
B Recommends based on fair evidence that RAI can improve important health outcomes.
The evidence is sufficient to determine effects on health outcomes, but the strength of the
evidence is limited by the number, quality, or consistency of the individual studies;
generalizability to routine practice; or indirect nature of the evidence on health outcomes.
C Recommends based on expert opinion.
D Recommends against based on expert opinion.
E Recommends against. Recommendation is based on fair evidence that RAI does not
improve important health outcomes or that harms outweigh benefits.
F Strongly recommends against based on good evidence that RAI does not improve
important health outcomes or that harms outweigh benefits.
I Recommends neither for nor against because evidence is insufficient to recommend
for or against RIA because evidence is lacking RAI improves important health outcomes,
the evidence is of poor quality, or the evidence is conflicting. The balance of benefits and
harms cannot be determined.

Expected benefit with radioiodine ablation
Factors Description
Decreased risk
of death
Decreased risk of
recurrence
May facilitate
initial staging
and follow-up
RAI ablation
usually
recommended
Strength
of
evidence
T1 1 cm or less, intrathyroidal
or microscopic multifocal
No No Yes No E
1–2 cm, intrathyroidal No Conflicting data Yes Selective use I
T2 >2–4 cm, intrathyroidal No Conflicting data Yes Selective use C
T3 >4 cm
<45 years old No Conflicting data Yes 100-150 mCi B
≥45 years old Yes Yes Yes 100-150 mCi B
Any size, any age, minimal
extrathyroidal extension
No Inadequate data Yes Selective use I
T4 Any size with gross
extrathyroidal extension
Yes Yes Yes 150-200 mCi B
Nx,N0 No nodal metastases No No Yes No I
N1 <45 years old No Conflicting data Yes Selective use C
>45 years old Conflicting data Conflicting data Yes Selective use C
M1 Distant metastasis Yes Yes Yes 150-250 mCi A
http://www.thyroidguidelines.org/revised/differentiated

What is the level of evidence supporting Rx of DCT with 131I?
Randolph GW, Daniels GH 2002 Radioactive iodine lobe ablation as an alternative to completion thyroidectomy for follicular carcinoma of the thyroid. Thyroid 12:989–996.
§RECOMMENDATION 30 Ablation of the remaining lobe with radioactive iodine has been used as an alternative to completion thyroidectomy. It is unknown whether this approach results in similar long-term outcomes. Consequently, routine radioactive iodine ablation in lieu of completion thyroidectomy is not recommended. Recommendation rating: D

Residual thyroid obscures mets

• Bleeding: 2.5%
• RLN palsy: temp 7% (0-22%),
perm 1.7% (0-18%)
• Hypo PTH: temp 36% (0.6-39%)
perm: 3.3% (0-7.6%)

Woman, 35 with thyroidectomy 8 years previously (for nodular hyperplasia) has a new thyroid nodule:
Clin Nucl Med 2014
30 mCi 131I
TSH- 49.5 μIU/mL Tg- 19.5 ng/mL TgAb- 20.3 U/mL.

What are the active foci? A. Artifact B. Thyroid mets C. Normal thyroid
Clin Nucl Med 2014

What are the active foci? A. Artifact B. Thyroid mets C. Normal thyroid
Clin Nucl Med 2014
Transaxillary endoscopic thyroidectomy

Survival Disease Free Survival
log rank = 7.16 P = 0.007
log rank = 11.1 P < 0.001
93%
62%
89%
78%
N = 100
T1-T3 100 mCi T4-N1 150 mCi M1 200 mCi

• RAI did not improve survival of surgery vs surgery + RIA for clinically detected recurrent DTC.
• The probability of dying or living with persistent disease after treatment of recurrent thyroid cancer is less for 131I detected recurrences compared to clinically diagnosed recurrences.

Am J Med. Volume 97, Issue 5, Pages 418-428 (November 1994) Long-term impact of initial surgical and medical therapy on
papillary and follicular thyroid cancer Ernest L. Mazzaferri, MD, FACP, Sissy M. Jhiang, PhD
• 1355 papillary and follicular cancer patients
• After 30 years, the survival rate was 76%, recurrence rate was 30%, and cancer death rate was 8%.
• When patients with distant metastases at diagnosis were excluded, follicular and papillary cancer mortality rates were similar (10% versus 6%, P = NS).

Am J Med. Volume 97, Issue 5, Pages 418-428 (November 1994) Long-term impact of initial surgical and medical therapy on
papillary and follicular thyroid cancer Ernest L. Mazzaferri, MD, FACP, Sissy M. Jhiang, PhD
• 131I to ablate normal thyroid remnants: recurrence rate was <1/3 the rate after thyroid hormone therapy alone (P <0.001).
• Low 131I doses (29 to 50 mCi) were as effective as high doses (51 to 200 mCi) in controlling tumor recurrence (7% versus 9%, P = NS).
• 131I for remnant ablation or cancer therapy, recurrence and the likelihood of cancer death were reduced by at least 50%, despite more adverse prognostic factors in patients given 131I.

Am J Med. Volume 97, Issue 5, Pages 418-428 (November 1994) Long-term impact of initial surgical and medical therapy on
papillary and follicular thyroid cancer Ernest L. Mazzaferri, MD, FACP, Sissy M. Jhiang, PhD
• At 30 years, cumulative cancer
mortality rate following 131I therapy for any reason, was 1/3 that in patients not so treated (P = 0.03).

2 patients with DTC lung mets; which is higher risk for cancer death?
Patient A Patient B

2 patients with DTC lung mets; which is higher risk for cancer death?
Patient A, with lung mets >1 cm is at greater risk for DTC related death.
< 1 cm
1 cm+
Survival

Significance of DTC lung mets?
• 24/369 (6%) had lung mets
• Followed for mean of 13 years
• 21% death / 46% “good response to 131I”
• RAI dose of 457.3 (300-600) mCi 131I) for “good responders”.
• Extra-thyroidal invasion, 18F-FDG uptake, and lung mets > 1cm predicted death.
Clin Nucl Med 2014

131I beta radiation
What is the maximum beta tissue range for 131I
A. 0.5 mm
B. 2.4 mm
C. 5.2 mm
D. 7.8 mm

131I beta radiation
What is the maximum beta tissue range for 131I
A. 0.5 mm
B. 2.4 mm
C. 5.2 mm
D. 7.8 mm
• The mean beta tissue range for 131I is 0.5 mm

2 patients with DTC lung mets; which is higher risk for fibrosis?
Patient A Patient B

2 patients with DTC lung mets; which is higher risk for fibrosis?
Patient B has a higher risk of post 131I ablation pulmonary fibrosis.
That typical risk is <1%
Radiation fibrosis is more likely after 80 mCi to the lungs.

Side effects of DTC treatment with 131I
• Radiation thyroiditis 10–20%
• Sialadenitis (dry mouth) 30%
• Gastritis 30%
• Radiation pulmonary fibrosis (patients with lung metastases) <1%
• Second primary malignancy <1%

Results: In both groups, bilateral involvement of the parotid gland was the most frequently seen and was followed by bilateral involvement of the submandibular gland. Conclusion: An early start of sucking lemon candy may induce a significant increase in salivary gland damage. Lemon candy should not be given until 24 h RAI. J Nucl Med 2005; 46:261–266
Lemon candy given Immediate
(n=116)
At 24 hours
(n=139)
Sialoadenitis 63.8% 36.8% P = 0.001
Taste loss 39.0% 25.6% P = 0.01
Dry mouth 23.8% 11.2% P = 0.005
Permanent xerostomia 14.3% 5.6% P = 0.05

Time in hours 4 24 48
Rad
ioio
din
e U
pta
ke
Salivary Gland Radioiodine Uptake
Liu et al. Influence of vitamin C on salivary absorbed dose of 131I in thyroid cancer patients: a prospective, randomized, single-blind, controlled trial. J Nucl Med 2010;4:618-23.
Conclusion: Salivary stimulation with vitamin C at any
time after 131I administration has only a limited effect on salivary absorbed dose in thyroid cancer patients.

1. What is the total accumulated 131I dose for differentiated thyroid cancer above which second primary neoplasms have
been shown to occur?
A. 10 GBq (270 mCi)
B. 20 GBq (540 mCi)
C. 30 GBq (810 mCi)
D. 40 GBq (1.08 Ci)

1. What is the total accumulated 131I dose for differentiated thyroid cancer above which second primary neoplasms have
been shown to occur?
A. 10 GBq (270 mCi)
B. 20 GBq (540 mCi)
C. 30 GBq (810 mCi)
D. 40 GBq (1.08 Ci)
The correct answer is “D”, 40 GBq (1.08 Ci). “The cumulative dose of I-131 more than 40 GBq (1.08 Ci) was the sole factor associated with increased odds of SPM after adjusting for age, follow-up duration, histology of DTC, presence of metastasis and history of external radiotherapy ” (Odds ratio: 113; 95% CI: 8.6-1495.6; p<0.0001). Reference: Fallahi et al, Clin Nucl Med 2011

Incidence of second primary malignancies during a long-term surveillance of patients with differentiated thyroid carcinoma in relation to radioiodine treatment
“The cumulative dose of I-131 more than 40 GBq (1.08 Ci) was the sole factor associated with increased odds of SPM after adjusting for age, follow-up duration, histology of DTC, presence of metastasis and history of external radiotherapy
(Odds ratio: 113; 95% CI: 8.6-1495.6; p<0.0001).”
Fallahi et al, Clin Nucl Med 2011

2. What 131I dose adjustment is appropriate in an athyroid patient with differentiated thyroid cancer and end-stage renal failure?
A. Increase dose x2
B. No adjustment required
C. Reduce dose by 50%
D. 5-fold reduction

2. What 131I dose adjustment is appropriate in an athyroid patient with differentiated thyroid cancer and end-stage renal failure?
A. Increase dose x2
B. No adjustment required
C. Reduce dose by 50%
D. 5-fold reduction
The correct answer is D. 5-fold reduction. According to Kaptein et al, “…in patients receiving continuous ambulatory peritoneal dialysis therapy, 5-fold reductions in radioiodine clearance rates require 5-fold decreases in Na131I dosages to avoid excessive radiation to total body and red marrow.” Kaptein EM, et al. Radioiodine dosimetry in patients with end-stage renal disease receiving continuous ambulatory peritoneal dialysis therapy. J Clin Endocrinol Metab. 2000 Sep;85(9):3058-64.

3. What is the typical exposure to household members living with patients treated as outpatients with up to 200 mCi of 131I for differentiated thyroid cancer?
A. <35 days BRET
B. 100 days BRET
C. 365 days BRET
D. 1000 days BRET
• BRET = Background radiation equivalent time

3. What is the typical exposure to household members living with patients treated as outpatients with up to 200 mCi of 131I for differentiated thyroid cancer?
A. <35 days BRET
B. 100 days BRET
C. 365 days BRET
D. 1000 days BRET
• BRET = Background radiation equivalent time
Willegaignon J, et al. Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure. Clin Nucl Med. 2011 Jun;36(6):440-5.
The correct answer is A. <35 days BRET

Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure
• “100 DTC selected outpatients treated with 131I and their caregivers were monitored at home for radiation dose by using thermoluminescent dosimeters. Surface contamination and contaminated solid wastes were identified and measured with a Geiger-Müller detector.”
Willegaignon J, et al. Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure. Clin Nucl Med. 2011 Jun;36(6):440-5.

Willegaignon J, et al. Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure. Clin Nucl Med. 2011 Jun;36(6):440-5.

Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure
• “90 monitored individuals received a mean dose of 0.27 (±0.28) mSv, and the maximum dose registered was 1.6 mSv.” Assuming a mean annual background exposure of 3 mSv, daily background is 0.0082 mSv. Thus, mean participant exposure was 33 day BRET.
• No participant received more than 200 days BRET.
Willegaignon J, et al. Outpatient radioiodine therapy for thyroid cancer: a safe nuclear medicine procedure. Clin Nucl Med. 2011 Jun;36(6):440-5.

Besides the USA, where is outpatient RAI > 30 mCi lawfully performed?
A. China
B. France
C. Israel
D. Italy
E. United Kingdom

Besides the USA, where is outpatient RAI > 30 mCi lawfully performed?
A. China
B. France
C. Israel (MOH Circ 0064/2002 File 4/3/200H)
D. Italy
E. United Kingdom

1 / 12
131I治疗甲亢专家共识(2010年) 前言 甲状腺功能亢进症,简称甲亢)以甲亢最多见,
我国人群患病率约1.2% 。甲亢的主要治疗方法为抗甲状腺药物和治疗。近年来,用治疗 甲亢的患者呈增多趋势,为了进一步规范治疗,由多位核医学专家经多次共同商讨,数易其稿,历时2年,就有关治疗甲亢临床相关问题形成此共识。 [1] 131 I 131 I 131 I 131 I
本共识立足甲状腺核医学,参考相关文献和临床应用情况,遵循先进性、实用性、公认性和时效性原则,重点阐述治疗甲亢相关问题,对甲亢的临床表现、实验室检查、甲亢
危象处理和抗甲状腺药物治疗等内容予以简述[2,3]。 131 I
Local 131I regulations sent by colleagues in China:


Clin Nucl Med 2014;39: 977-979
What is the greatest risk in RIA for this patient with DTC? A. Edema B. Headache C. Hemorrhage D. Necrosis E. Stunning
2 mCi 131I 200 mCi 131I

Clin Nucl Med 2014;39: 977-979
What is the greatest risk in RIA for this patient with DTC? A. Edema B. Headache C. Hemorrhage D. Necrosis E. Stunning
2 mCi 131I 200 mCi 131I
DTC brain mets: • 0.3-1.3% of DTC patients • Mean survival 4.7 months

FDG-PET/CT in differentiated thyroid cancer
18F-FDG

FDG-PET/CT in differentiated thyroid cancer
18F-FDG
131I

FDG-PET/CT in DTC
Clin Nucl Med 2014

How will the patient be followed up?
Whole body scan - (1 week) Resume T4 - (24 hours) Endocrine appointment
How to advise regarding radiation safety?
Verbal instructions Teach back instructions Printed instructions
Release to home or admit to the hospital?
Suitable discharge isolation Local radiation safety requirements
What medical preparation is required?
Medications to stop Medications to start Diet Modifications Additional tests ~ PFT
What dose is appropriate? (Written Directive) Remnant Ablation
30-100 mCi
+ Nodes, vascular invasion
100-150 mCi
Metastases
150-250 mCi
Patient for 131I Treatment
History/Physical LABS: Tg, TgAB,TSH,CBC, pregnancy test Pre-treatment imaging
SUMMARY

“Treatment with 131I”

Presentation Evaluations
• Too much
• Too little
• Too fast
• Too slow
• More food
• Too technical
• Too cold