
Treatment for scoliosis | curvature of the spine | thoracic kyphosis | Spine Surgeon in Colorado

Revised version 10.03.2007
TREATMENT OF SCOLIOSIS. F.E.D. METHOD
The Results of 400 cases
Santos Sastre (1) ; Pedro Lapuente (2); M. Merçe Roca (3); Alicia Trallero (4);
Gustavo Pseiro (5); Paolo Raimondi (6); Natalia Sastre (7)
(1) Professor at the Univerdad de Barcelona. Director of the Centro de Rehabilitación y Medicina Fisica in
Barcelona. Consultant in the CAPs Eaixemple de Barcelona – ICS. España
(2) Medical Manager of the Centro de Medicina Correctiva in Sabadell Barcelona. España
(3) Assistant-Manager of the Centro de Rehabilitación y Medicina Física in Barcelona. España
(4) Manager of the Centro Coras in Madrid. España
(5) Professor at the Universidad in la Coruña. España
(6) Professor in Departimento di Ingegneria – Facoltà di Scienze Motorie – Universitat di L’Aquila – Italia
(7) Biologist. Universidad Autonoma de Barcelona. España
Correspondence:
Prof. Santos Sastre
Centro de Rehabilitación y Medicina Física
Aribau, 300
08006 Barcelona
Spain
Tel. + 34 93 2021366
Fax: + 34 93 2096260
e-mail: [email protected]
____________________________________________________________________
Study design. To find the value of the radiological changes to the spine of 400 children
suffering from scoliosis who were treated with a special physiotherapy treatment for a
year.
Objectives. To evaluate the reduction of the Cobb angle and the vertebra rotation, the
averages, and the improvement percentage of 400 scoliosis cases who were treated with
the F.E.D method for 12 months.
Background. The conservative treatment of spine deviations is often met with little
enthusiasm and conviction. We have recently finished this study which started at the
end of 1989, after having been encouraged by the results of our investigations which
consisted in applying the conservative treatment to scoliosis- first in animals (rabbits),
then in humans, during their growth period.
Material and Methods. Four hundred scoliosis cases aged between 4 and 42. The
average age at the start was 13,5 and the Risser was 1,805. 13% were under 10 years of
age; 63% between 10 and 15 and 24% were over-15 years. 64% were girls/women and
36% boys/men.
Progressive Idiopathic Scoliosis 368 cases (92%); 9 Congenital (2,25%); 8 Neurogenics
(2%); 5 Myogenics (1,25%); 4 Osteogenics (1%); 3 Post Traumatics (0,75%); 2
Postural Acquired (0,50%) and 1 Post Surgery (0,25%).
The rachis alterations were measured by physical and functional tests and by an antero-
posterior X-ray, in standing position, of the general spine with vision of the Iliac crests
and femoral heads. An X-ray was taken of them every 6 months. The curves ranged
between 10º and 66º, with an average Cobb angle of 20º, and a vertebra rotation of 12º
in 117 cases. 248 cases had curves under 20º Cobb. 94 cases had between 20º and 30º
Cobb. 31 cases had 31º to 40º Cobb. 27 cases had curves above 41º Cobb.

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
2
All patients had special physiotherapy treatment for 12 months. The treatment
consisted in preparing the thoracic-lumbar back area, using electrotherapy and thermo
therapy; then applying external corrective forces on the scoliosis curves. These were
generated by a designed, experimented and patented system (F.E.D.) This system allows
the rachis to be elongated and set three-dimensionally while applying a pressure (of
between 1 and 100 kg) to the apex of the scoliosis curve, de-rotating and inflecting it
intermittently (15 seconds of pressure and 10 of relaxation) for 30 minutes. Every
session ended with analytical kinesitherapy and PNF.
Results. At the end of 12 months, the radiological study showed a significant reduction
in the average Cobb angle, from 20º to 9º, with a relative recuperation percentage of
67%. The vertebra rotation was reduced from 12º to 4º, with a relative recuperation
percentage of 74%. There was a significant improvement as a result of this treatment.
The scoliosis curve and the vertebra rotation were significantly less after 12 months of
F.E.D treatment.
Conclusions. The results blatantly contradict the negative concept that many
specialists have of the effectiveness of physiotherapy in treating scoliosis. These
experiments and results prove the effectiveness and value of physiotherapy and its
therapeutic effects. It should be a top option for treating spinal curves.
Key words. idiopathic scoliosis; conservative treatment; scoliosis correction; the value
of physiotherapy; spine; spinal deformities; spinal curvatures; physical therapy
techniques; vertebra de-rotation; inflection of the scoliosis curve; three-dimensional
setting of the rachis; orthopaedic procedures; F.E.D.
______________________________________________________________________
Introduction
The dynamic forces generated by the daily activities of the individual suffering from
scoliosis, kyphoses or lordosis exert a continual unilateral pressure on the hemi
vertebrae, discs and cartilages which are subjected to greater compression, leading to
alterations in their trophism and their imbibition system. Studies on the effects
generated by a derangement of the imbibition mechanism of the vertebrae and cartilage,
have shown that they can cause a de-stabilization effect to the spine and cause
scoliosis. (1,5,7,11,46,47,48,52,61,63). Through similar mechanisms, the vertebral
growth nuclei and the neurocentral cartilages may also be affected (28,31,46,47,61).
Compression of the neurocentral cartilage in pigs and rabbits caused scoliosis (16,38).
Surgical interventions in animals affecting the vertebral growth nuclei also caused
scoliosis (13,15,21,33,34,35). Unilateral epiphysiodesis of the epifhysis cartilage, in
dogs and rabbits, caused wedging with vertebral deformation and scoliosis (1,38).
The lesion of several epiphyseal cartilage plates of the vertebrae in young pups of 2 to 3
months caused scoliosis and kyphosis (20). The resection of the sacrospinatus and
interspinatus muscles and ligaments in animals resulted in an asymmetrical
chondrogenesis due to unequal compression, causing kyphosis and scoliosis (3,43,57).
Alterations in the transport of calcium to the cellular membrane in the back muscles
have been pinpointed as a cause of scoliosis as well. (69).
From these experiments, we’ve learned that unilateral and asymmetrical pinching,
cutting and chearing cause repeated micro trauma to the cartilaginous tissues and bone,
resulting in ischemic disorders and morphological changes which enhance the curves.
(2,11,39,46,49,66). Nutritional imbalances of the spine were studied. The coagulation of
the proximal segments of the intercostal arteries in rabbits induced scoliosis (12).
Unilateral, vascular alterations of the metameric artery nourishing hemi vertebra, the

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
3
growth cartilages and the neurocentral cartilages caused scoliosis in rabbits during their
growth period (6). The unilateral intervertebra compressive factors worsen the curves;
without these compressive factors, scoliosis wouldn’t form (30,34,46,49,59,60,68).
The FED system of tridimensional spine Fixation, in Elongation with graded corrective
and De-rotating pressure and postural self-control by the patient was postulated on the
basis of our daily practice experience, which led us to the following hypothesis: “If asymmetrical, dynamic compressive forces are able to cause and worsen a deformation of the
bone during the period of bone growth, then other greater forces applied in the contrary direction
should stop the primary deforming effects and normalize the situation »
Our research started more than 20 years ago based on this hypothesis. It consisted in
creating experimental scoliosis in forty 25-day old rabbits. Twenty animals had
physiotherapy treatment. Compressive, dynamic and asymmetric forces generated by
adequate manual techniques were applied to oppose the causes aggravating the
deformity. The other twenty rabbits were not interfered with. After the four-month
experiment, the results were significant when comparing the treated and non-treated
animals. The miotendinous-ligamentous forces elicited by vertebral manipulation, with
their mechanical effects on the scoliotic incurvation, achieved a remodelling of the
bone, cartilaginous and muscular tissues of the treated rabbits. The study showed, with a
99.99% certainty, the effectiveness of therapy in those treated when compared to the
non-treated. The significant difference between the two groups could only be attributed
to the techniques of the treatment used in our research (46,62). In December 1989, we
designed an experiment prototype of the FED system to achieve the same therapeutic
effects in humans as in the rabbits. For about 15 years, we’ve been treating patients, as
much as possible during their growth period, who have spinal curvature, mainly
idiopathic scoliosis. Our results are compiled below.
Material and Methods
Four hundred patients suffering from scoliosis, aged between 4 and 42.
The initial average age was 13,5; the initial Risser average was of 1,805 and at the end
of twelve months, of 2,359 . The distribution in function of the age gap for 280 cases
was: < 10 years old, 13%; [10-15 years old], 63%; > 15 years old, 24%.
64% of the patients were girls/women 36% were boys/men. Table 1.
Before starting the treatment, all the patients underwent a physical and functional test
and a measurement of the spine alteration by X-ray, antero posterior, in standing
position, of the spine with vision of the Iliac crests and femoral heads.
There were clinical, physical and functional tests done every 6 weeks and X-rays done
every 6 months.
The initial X-ray showed curves ranging from 10º to 66º, with an initial average Cobb
angle of 20º and the Raimondi (40,41) vertebra rotation of 12º in 117 of the cases, .
The characteristics and frequency distribution of the curve size is given in Table 1.
During 12 months, all the patients regularly had special physiotherapy, which consisted
in preparing the thoracic-lumbar back area using electrotherapy and thermoterapy.
This was followed by applying external corrective forces to the scoliosis curve using the
FED system, to achieve the same therapeutic results that were achieved with the rabbits.
Figure 1.
The FED system is fundamentally a chassis formed by profile members. These can be
adjusted vertically and horizontally and support the means for holding up the patient as
well as other therapeutic means to immobilise the patient. This system allows the
tridimensional fixation of the spine in elongation, with a de-rotary corrective pressure

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
4
which is adjustable and exerts between 1 and 100 kg to an area of 2.000mm2 on the
apex of the scoliotic curve, de-rotating and inflecting it intermittently (15 seconds of
pressure and 10 of relaxation). These traction-elongation forces, de-rotating, inflecting
and/or reversing the scoliosis curve with the patient’s posture auto control, while in an
ortostatic position, is done repeatedly during 30 minutes.
The correction of the deformity is thus possible due to the therapeutic effects on the
various tissues from the traction, elongation, pressure, detraction and de-rotation forces
as well as the control of correction by the patient himself. All this stimulates the
propioceptive system – the interoceptors of the capsules, tendons and muscles -, which,
when placed under stress, begin transmitting afferences to the upper centres that register
the correct position and improves the postural self-control.
Each session ends with a half hour of analytical kinessitherapy and PNF.
Results
Effectiveness of the treatment
Scoliosis according to King-moe I, II, III, IV and V
Table 2.
In scoliosis patients with more than one curve, only the most pronounced curve
was taken into account. If the two curves were the same, we elected the dorsal scoliosis,
which is, in double scoliosis cases, the one with the least relative recuperation. Figures
2, 3 and 4.
Statistical comparison of two observational means in large populations (n = 400) with
paired data.
1. A change of variables is made. We define a new variable yxz −= , where
:x initial curve; :y curve at the end of the 12 months; :z each individual’s
difference.
2. 52,11=Z 83,272=ZS
3. :0H the treatment has not produced significant improvement; the curve
before and after the treatment is the same, 0=Z
:1H the treatment has produced significant improvement; the curve after the
treatment is less 0>Z
(This is a comparison test of an observed average 400
∑ −=
yxZ , with a
theoretic average 0=m ).
4. 6555,43
400
83,27
52,11
2===
n
S
ZZ
n
If 01.0ZZ ≤ , we accept the 0H

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
5
If 01.0ZZ > , we reject the 0H
As 6555,43576.201.0 <=Z , we reject the 0H (with a 01.0=x risk).
The treatment produces a significant improvement. The scoliosis curve is
significantly less after the 12-month treatment. Table 2.
Rotation
Statistical comparison of two observational means in a large population (n =
117) with paired data.
1. yxz −= , where :x initial rotation; :y rotation after 12 months; :z each
individual’s difference.
2. 25,8=Z 007,292=ZS
3. :0H the treatment has not produced significant improvement; the rotation
after the treatment is the same, 0=Z
:1H the treatment has produced significant improvement; the rotation after the
treatment is less. 0>Z
(This is a comparison test of an observed average 117
∑ −=
yxZ , with a
theoretic average of 0=m ).
4. 5758,16
117
007,29
25,8
2===
n
S
ZZ
n
If 01.0ZZ ≤ , 0H is accepted
If 01.0ZZ > , 0H is rejected
As 5758,16576.201.0 <=Z , we reject 0H (with a 01.0=x risk).
Figure 4.
The treatment produces a significant improvement. The scoliosis curve
rotation is significantly less after the 12-month treatment. Table 2.
Locating the post treatment improvement.

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
6
Test to determine whether the treatment has a different effect on the lumbar
scoliosis and the dorsal scoliosis.
Analysis of the variance: factorial plan of two unrepeated factors.
Factor A: Type of scoliosis, dorsal or lumbar in patients with scoliosis King-
Moe I, II and V.
- Factor B: Patients (factor not relevant)
According to the F distribution:
89,3)05.0,161,1( =F
79,6)01.0,161,1( =F
the factor is significant at the 1% level.
There it is. There are differences in the results of treating dorsal scoliosis and lumbar
scoliosis in patients with double scoliosis: lumbar scoliosis recuperates better. This
significant difference is due to the obstacle of the ribs to the other scoliosis curve.
The average recuperation degree of scoliosis King-Moe I dorsal is of º10=X ,
and the lumbar is of º13=X .
The average recuperation degree of scoliosis King-Moe II dorsal is of º9=X ,
and the lumbar is of º10=X .
The average recuperation degree of scoliosis King-Moe V dorsal is of º12=X ,
and of the lumbar is of º11=X .
Table 3.
Recuperation percentage in relation to the degree of bone maturity
1. The value of the Risser. The average value of Risser for the 12 months was
calculated; the equivalences can be found in Table 4.
2. The recuperation percentage. Since all the individuals improved, the
measurement of relative improvement was recorded.
100.)()(
.. ×⋅
⋅⋅⋅⋅−⋅=
inicialCurvatura
tratmesesntrasCurvainicialCurvaP cobbr
100.)()(
.. ×⋅
⋅⋅⋅⋅−⋅=
inicialRotación
tratmesesntrasRotacióninicialRotaciónP rotr
The average Risser at the start was of 1,805 and at the end, was of 2,359. Table 5
shows the total averages of recuperation of Cobb and the rotation in function of the

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
7
average Risser after 12 months of treatment. In individuals with double scoliosis, the
Cobb was only taken for the bigger scoliosis curve. If the curves were the same, the
recuperation percentage of the dorsal scoliosis curve was taken, since it is the one of
less relative recuperation.
Correlation
Variables:
=x Average Risser of the 12-month treatment.
=y Recuperation percentage after the 12-month treatment.
6689,0−=
⋅−
=
∑
yx
xySS
yxN
xy
r
Test of independence between the variables x and y
:0H Independence between the variables x and y , if )01.0,398(rrxy ≤ .
The hypothesis of independence between variables with 01.0=x risk is
rejected; the variables x and y are related.
Regression line
Variables:
=x Average Risser of the 12-month treatment.
=y Recuperation percentage after the 12-month treatment. Figure 5.
We can conclude that:
- The variables :x [average Risser of the 12-month treatment] and :y [recuperation
percentage after the 12-month treatment], are independent variables, with a correlation
coefficient = - 0,6689.
- The negative coefficient indicates that they are proportional inverse variables
(regression lines with a negative gradient): when the variable :x [average Risser of the
12 month treatment] increases, the variable :y [recuperation percentage after the 12
month treatment] decreases.
Discussion
The results clearly show, beyond any doubt, the therapeutic effects of the FED system
on the bone, cartilage, disc, ligaments, muscles, vascular system sensorimotor network,
neuromuscular system and orthostatic postural control of the patient with spine
deformity. There is a logical, rational and scientific explanation for this. In fact, there

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
8
was no reason apart from the technical difficulty to think that we would not be able to
obtain the same results with humans as we got some years earlier in rabbits treated
exclusively with physiotherapy (46,62).
These results from 15 years of evaluating, treating and following scoliosis patients,
blatantly contradict the negative concept that many specialists have of the effectiveness
of physiotherapy in treating spinal curves. (8,9,19,22). It is probable that the results of
the conservative treatment, as Willers states (67), have not been clearly documented in
the past. Now, however, more therapeutic preponderance must be conceded to
physiotherapy when it comes to spinal curvatures since the results from the experiments
prove its efficiency and therapeutic effects (4,10,23,29,46,47,49,50,51,55,56,62,65).
Cotrel (10) and Stagnara (56) have combined systematic exercise programmes, which
have reduced the seriousness of idiopathic scoliosis.
In the USA, however, they have opted for the “benefits” of surgery and braces, namely
the Milwaukee brace and the lumbosacral orthosis. They have openly spoken out
against physiotherapy. Today, we know that the Milwaukee brace is only
recommended for kyphose and scoliosis cervico-thoracic, which represent
approximately 1% of all scoliosis cases. On the other hand, there are also questions
over the long-term effects and complications of surgery on curvature of the spine. More
and more specialists are choosing the conservative treatment and applying the new
active and effective methods early on. (4,10,13,23,25,26,32,42,46,47,49,50,51,54,
55,56,62,64,65).
We know that spinal deformities have their genesis, independently of the etiology, in
alterations of the vertebra or of the systems and elements of the rachis called extra
vertebral alterations.
All these alterations become apparent through morphological and anatomopathological
changes of the bone and cartilage. They can vary in seriousness if they are not treated
and can even start to be noticed by the naked eye. These structural changes will end up
unbalancing the perfect symmetry of the spine and chest, which in turn, will accelerate
the deformation, especially in scoliosis cases with a Cobb angle above 30º and a high
rotation component (36,53,58). In order to reduce the deformation once it is structured
in the spine, external forces are needed to achieve the orthostatic position of the spine.
The most important factor, which also conditions the others, is that the rachis has not
yet finished growing. The recuperation percentage is always higher, the younger the
patient. The younger the patient, with Risser at around zero, the higher the recuperation
percentage when using the FED method, and fewer are the difficulties that could arise
when rectifying the pathological curves of the spine.
Mccarthy (26) states that early diagnosis and treatment at an early age is the best way to
prevent later scoliosis complications. According to Viladot (64) the best scoliosis
treatment is early diagnosis.
In fact, some authors pinpoint the risk of scoliosis progression at puberty and associate
it to the menarche presence and the secondary sexual characteristics (14,24,37,56,70).
This is the reason for the insistence on early diagnosis and treatment, before the growth
spurt. There has been enough research made to know the risk of scoliosis progression.
(14,17,24,26,27,45,54,56,70).
The FED method is a global treatment which mainly corrects the pathological curves of
the spine during the growth period. It reduces and appeases the painful symptomology
in children and adults (4), showing an effectiveness index (IE) (8,18) significant and
superior to all existing conservative methods (23,50,65). Figures 6 and 7.
The FED method, although investigated and put into practice from another angle, with
methodology and different techniques of applying non-comparable external forces, is

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
9
similar to Cotrel and Morell’s (10) “E.D.F” technique. Although the abbreviations FED
– EDF, are in a different order, they mean the same :F = Fixation (Setting); E =
Elongation, and D = De-rotation and inflecting or inverting the scoliosis curves. The
Cotrel and Morell technique consists of a system similar to a rectangular stretcher which
elongates, rotates and finally sets the spine in plaster cast.
The FED system sets the spine three dimensionally. It then elongates and rotates it at
the same time as it inflects it, which in many cases, reverses the scoliosis curves in a
dynamic and active way rather than passively. The monitored forces applied are
generated by an electro-pneumo-mechanic system to rectify the rachis curves. The
intensity and intermittence is regulated by a computer which guarantees efficiency and
security. The FED unit is a very versatile system that can be applied to any type of
spinal deformities, be it scoliosis kypohses or lordoses.
Conclusion. The benefits of the F.E.D Method.
1.- The early diagnosis and treatment by FED Method during the child’s growing spurt
are logical and rational interventions which can correct spinal deformities and avoid
personal, social, and economic problems which she or he may experience in the future.
2.- The F.E.D. method structurally shapes and rectifies wholly or partially the
alterations of the vertebrocostals, discs, cartilages, muscles, vascularisation, the
propioception and the awareness of the orthostatic position, normalising and improving
posture. All this is done during the patient’s growth period.
3.- The external forces applied by the FED method firmly push on the growing spinal
structures inhibiting the hyperactive asymmetric bone generation, as well as soft tissue
alterations and sensorimotor network. At the same time, it stimulates and favours the
tissue activity in the hypoactive side which is the cause of asymmetry.
4.- The FED method, accelerates the awareness and volitive correction process of the
spinal curves of people suffering from scoliosis, kiphoses or lordoses.
5.-The FED method avoids the slave-like assistance of the physiotherapist in teaching
and correcting patients’ spinal curvature. .
6.- Through F.E.D, we are able to monitor the control the amount of force applied in
the opposite direction to the one causing the deformation on the spine of the patient. It
has an efficiency very rarely obtained by other procedures.
7.- The F.E.D. method is easy to apply when compared to other procedures such as
plasters, tractions, stretchers, braces...
8.- In serious, advanced spinal curvature, the F.E.D method allows the use of
orthopaedic systems, out of treatment hours, which compliment and improve the
achieved results.
9.- In symptomatic spinal curvature, applying the F.E.D method reduces and/or
appeases the symptomatology, mainly the pain, the stiffness and the instability...both in
children and adults, given that it avoids medicine (51), (which is inefficient since it does
not solve the cause of the symptomology).
10.- The F.E.D method, when applied early on, rectifies the rachis during the growth
spurt making the need for surgery, really very exceptional. In the worst of the cases, it
makes the surgeon’s intervention easier when there is no other option, as long as the
criteria of the specialists are met. (9,22,44).
A conservative method such as the F.E.D method, is extraordinarily good value, as
much for the individual as for the society because it avoids any further suffering, health
problems and absences from work of those suffering from spinal deformities. More

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
10
importantly, it improves their potential life span and their quality of life as well as
avoiding the aggression and implants of foreign material that surgery entails.
References
1. ALGARA LAMAGNIERE, C.(1976). Alteraciones experimentales de los
cartílagos de crecimiento epifisarios del cuerpo vertebral . Tesis doctoral. Universidad de Barcelona.
2. AMATO. V. P. y BOMBELLI. R. (1959). The normal vascular sopply of vertebral column in the growing rabbit. J. Bone and Joint Surg. 41-B. págs. 782-795.
3. ARNO. C. 1903. Experimentelle Beiträge zur Lehre der Skoliose. Archiv. für Orthepädie, Mechanoherapie and unfallchirurgie. 1. págs. 145-166.
4. BARRIOS, C.; J.P. LAPUENTE y S. SASTRE (2002) Treatment of chronic pain in adult scoliosis. Research into Spinal Deformities, 3, 290-303. Amsterdam. Ios Press (A. Tanguy and B. Peuchot).
5. BEGUIRISTAIN GURPIDE, J.L. (1973). Escoliosis experimental en ratas bípedas. Tesis doctoral. Universidad de Navarra.
6. BERLANGA, J.L. y colab. (1986). Estudio de la alteración vascular en la etiopatogenia de las desviaciones laterales experimentales . I Jornadas Internacionales sobre Investigación en la Columna Vertebral. Valencia.
7. BOUILLET, R. Y A. VINCENT (1967). La scoliose idiopathique . Acta. Orthop. Belg., 33, págs. 93-388.
8. BLOUNT, W. And J. MOE (1980). The Milwauke brace. Baltimore. Williams and Wilkins.
9. BRADFORD, D.S.; B. TAY and S. HU (1999) Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine, 24, 2617-2629.
10. COTREL, Y. et R. MOREL (1964) La technique de l’EDF dans les correction des scolioses. Rev. Chir. Orthop., 50, 59-75
11. CROCK, H.V. y H. YOSHIZAWA (1977). The blood supply of the vertebral column and spinal cercl in man . New York. Springer Verlag.
12. DE SALIS AMARAL C. (1977). Escoliosis experimental por lesión vascular . Tesis doctoal. Universidad de Navarra.
13. DIKSON, R.A. (1985). Conservative treatment for idiophatic scoliosis Jour. Bone Joint. Surg., 67 B. págs. 176-181.
14. DUVAL-BEAUPÈRE, G.; J. DUBOUSSET et P. QUENEAU (1970) Pour une théorie unique de l’evolution des scolioses. Nouv. Press Med., 78, 1141-1145.
15. FARFAN, H.F. (1973). Mechanical Disorders of the Low Back . Philadelphia. Lea and Febiger.
16. GILI, R.J. (1975). Influencia de la fisis neurocentral en la patogenia de la escoliosis experimental . Tesis doctoral. Universidad de Navarra.
17. GOLDBER, C.J.; F.E. DOWLING and E.E.FOGARTY (1994). Left toracic scoliosis configurations. Why so different? Spine, 19, 1385-1389
18. GONZÁLEZ-VIEJO, M.A. y M.J. CATALÁN ESPARDUCER (1999). Índice de efectividad del tratamiento de la escoliosis idiopática mediante el protocolo de ortetización de un servicio de rehabilitación. TOI (Bcn), 12, 83-98.
19. GONZÁLEZ-VIEJO, M.A.; O.COHÍ y F. SALINAS (2001). Escoliosis. Realidad tridimensional. Brcelona. Masson.
20. HAAS, S.L. (1939) Growth in length of the vetebrae’. Arch. Surg., 38. 21. HAAS, S.L. (1939) Experimental production of scoliosis . J. Bone Joint Surg., 22,
págs. 963-968. 22. JAMES, J.I.P. (1975). The management of infants with scoliosis. J. Bone Joint
Surg., 57B., 4, 422-429. 23. LAPUENTE, J.P.; S. SASTRE and C. BARRIOS (2002). Idiopathic scoliosis
under 30º in growing patients. Acomparative study of the F.E.D. Methode and other conservative treatments. Amsterdam. Research into Spinal Deformities, 3,

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
11
258-278. IOS Press (A. Tangay and B. Peuchot). 24. LONSTEIN, J.E. and J.M. CARLSON (1984). The predition of curve progresion
in untreated idiopathic scoliosis during growth. J. Bone Joint Surg., 66A, 1601-1671.
25. MAUROY, J.C. (1996). La escoliose. Traitement orthopédique conservateur. Montpellier. Sauramps Medical, 15-19.
26. MCCARTHY, R.E. (1987). Prevention of the complications of scoliosis by early detection. Clinical Orthopaedics and Related Research, 222, 73-78.
27. METHA, M.H. (1972). The rib-vertebra angle in the early diagnosis between resolving and progressive infantil scoliosis. J. Bone Joint Surg., 54B, 230-243.
28. MICHELSSON, J. E. (1965). The developement of spinal deformity in experimental scoliosis . Acta Orth. Scandinavica, 81
29. MOLLON, G.; J.C. RODOT et M. OLLIER (1986). Scoliosis structurales mineurs et kinésithérapie. Étude statistique comparative des résultats. Ponencia aal III Congreso Nacional de Fisioterapia. Valencia.
30. MÜLLER, (1928) Slcoliose in Tierversuch . Bruns’ Beiträge zurKlinischen Chirurgie, 42, págs. 343-379.
31. NACHEMSON, A.L. and T. SAHLSTRAND (1977). Etiologic factors in adolescent idiopathic scoliosis. Spine, 2, 176-181.
32. NACHEMSON, A.L.and L.E. PETERSON (1995). Members of the brace study group of the Scoliosis Research Society. Effectiveness of the treatment with a brace in girls who have adolescent idiopathic scoliosis. J. Bone Joint Surg., 77A, 815-822.
33. NACHLAS, I.W. y J.N. BORDEN (1950). Experimental scoliosis. The role of the epiphisis . Surg. Ginec. Obstetr., 90, págs. 672-679.
34. OTTANDER, H.G.(1963). ‘Experimental progressive scoliosis in a pig . Acta Orthop. Scand., 33.pág.91.
35. PACHER, W. (1928). Operative Erzengung einer skoliose im Tierversuch . Zeitschrift für Orthopäedie, 69, pág. 140.
36. PERDRIOLLE, R. et J. VIDAL (1981). Étude de la coubure scoliotique. Importance de l’extension et de la rotation vertèbrale. Rev. Chir. Orthop., 67, 25-34.
37. PERDRIOLLE, R. and J. VIDAL (1987). Morphology of scoliosis: Three-Dimensional evolution. Orthopedics, 10, 909-915.
38. PIQUÉ. C. (1976). Tesis Doctoral . Universidad de Barcelona. 39. PITZEN, P. (1927) Experimentalle Erzengong von skoliosen . Zeitscrift fiir
Orlhopädische Chirurgie. págs. 49-58. 40. RAIMONDI, P. (1985). La rotazione vertebrale-proposta di un nuovo metodo di
misurazione. L’Aquila: Anali ISBF 1985, 81-84. 41. RAIMONDI, P. (1986) L’evaluation de la rotation vertebrale avec la methode
Raimondi . Extrait de la relation du 3ème Congres International I.C.H.P.E.R. 42. RAIMONDI, P.; O.VINCENZINI e collab. (2003). Teoria Metodologia e
Didactica del movimento – Compensativo Rieducativo Preventivo. Perugia. Margiacchi-Galeno Editrice.
43. RIGGINS, R.S.; U.K. ABBOTT; C.R. ASHMORE; R.B. RUCKER y J.R. ACCARREY (1977). Escoliosis in chickens . J.Bone Joint Surg., 59A. págs. 1.020-1.025.
44. RISSER, J.C. (1966). Treatment of scoliosis during the past 50 years. Clin. Orthop., 44, 109-113.
45. ROAF, R. (1971). Growth of the spinal articular process and their clinical significance. En: “Scoliosis and growth”. Ed. P. Zorab. Londres. Cchurchill Livingstone.
46. SASTRE, S. y COL. (1989) Fisioterapia experimental en Escoliosis . Fisioterapia, 39, págs. 7-26.
47. SASTRE, S.; A. MORENO; F. GÓMEZ; A. ESTRADA; CH. PEGOLO; G.G. HERRERA y A. CARRERA. (1993) Tratamiento de la escoliosis Método F.E.D.(Fijación tridimensional de la c.v. en Elongación, por suspensión, con presión correctora y Desrotatoria) . Fisioterapia. 15,1, págs. 3-18.

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
12
48. SASTRE, S. (1994). Scientific Basis of the F.E.D. Methode. European Spinal Resonance-Medical, 3, 3, 7-17.
49. SASTRE, S. (1995). Método de tratamiento de las escoliosis, cifósis y lordosis. Barcelona. Universidad de Barcelona.
50. SASTRE, S.; J.P. LAPUENTE; C. SANTAPAU y M. BUENO (1999). Dynamic Treatment of Scoliosis. (The Results of 174 Cases). Research into Spinal Deformities. Amsterdam. IOS Press. (I.A.F. Stokes).
51. SASTRE, S.; J.P. LAPUENTE and C. BARRIOS (2002). Benefits of F.E.D. Treatment in Scheuerman’s Disease. Research into Spinal Deformities. Amsterdam. IOS Press (A. Tanguy and B. Peuchot).
52. SEVASTIK, J.; S. ARO and H. NORMELLI (1984). Experimental and clinical scoliosis. Clin. Orthop. Rel. Res., 191, 27-34.
53. SEVASTIK, J.; M. AGADIR and B. SEVASTIK (1990). Effects of the rib elongation on the spine. I. Distorsion of the vertebral aligment in the rabit. Spine, 15, 822-825.
54. SEVASTIK, J. (1997). Priorities and Long Term Task in Research of Idiopathic Scoliosis. Research into Spinal Deformities.1, 503-505 Amsterdam. IOS Press (J.A. Sevastik and K.M. Diab).
55. SOHIER, R et P. HEUREUX (1979). Kinésithérapie des rachis scoliotiques. Bruxelles. Mecaprint.
56. STAGNARA, P. (1953). Scolioses évolutives en période de croissance. Aspects cliniques et radiologiques. Propositions thérapeutiques. Rev. Chir. Orthop., 39, 378-449.
57. STIWELL, D.L. y M.D. STANFORD (1962) Structural Defomities of vertebrae Bone adaptation and Modeling in Experimental Scoliosis and Kyphosis .J. Bone Joint Surg. 44 A, págs. 611-634.
58. STOKES, I.A.F. (1989). Axial rotation component of thoracic scoliosis. J. Orthop. Res., 7, 702-708.
59. STOKES, I.A.F.; H. SPENCE; D.D.AROUSSON and N. KILMER (1996). Mechanical modulation of vertebral body growth: implication for scolikosis progression. Spine, 21, (10), 1162-1167.
60. STOKES, I.A.F. (1997). Analysis of symetry of vertebral body loading consequent to lateral spinal curvature. Research into Spinal Deformities, 1, 97-101. Amsterdam. IOS Press (J.A. Sevastik and K.M. Diab).
61. TAYLOR, T.K.F. (1975). The disc factor in scoliosis (proceedings and reports of universities) . J. Bone Joint Surg., 57B, pág. 121.
62. TRESERRA, J. y S.. SASTRE (1989) Acción de la fisioterapia en la escoliosis experimental . Rev. Ortop. Traum., 33B.l.págs. 117-124.
63. TRUETA, J. (1975). La estructura del cuerpo humano. Estudio sobre su desarrollo y decadencia . Barcelona. Labor.
64. VILADOT, R.; O. COHÍ y S. CLAVEL (1995).Ortesis y prótesis del aparato locomotor. Columna vertebral. Barcelona. Masson.
65. WEISS, H.R.; I. HECKEL and C. STEPHAN (2002). Application of passive transverse forces in the rehabilitation of spinal deformities. A randomized controlled study. Research into Spinal Deformities. Amsterdam. IOS Press (A. Tanguy and B. Peuchot).
66. WILEY, A.M. y J. TRUETA (1959) The vascular anatomy of the spina and its relationship to piogenic vertebral osteomielitis . J. Bone Joint Surg.. 41. pág. 796.
67. WILLERS, U. (1994). Clinical and experimental studies on the thoracospinal deformity in scoliosis. Stockholm. Kongl Carolinska Medico Chirurgiska Institutet.
68. WULLSTEIN, L. (1902) Die skoliose in ihrer Behandloug und Entstehung nach Klinischen und ex-perimentellen Stadien . Zeitschrift für Qrtopädische Chirurgie, 10. pág. 177.
69. WONG, Y.C.and al. (1977). Ultraestructural changes in the back muscles of idiopathic scoliosis. Spine, 2, 251-257.
70. ZORAB, P.A. (1971). Escoliosis and growth. London. Churchil Livingtone.

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
13
Table1. Classification, seriousness and distribution of the scoliosis curves
Type of curve Average Cobb Distribution of the Curves
(400 cases)
Average rotation
(117 cases)
n cases Initial Grade <20º [20º-30º] [31º-40º] >40º n cases Initial
Grade
King-Moe I 112 18 72 31 6 3 49 13
King-Moe II 100 25 37 39 14 9 23 13
King-Moe III 64 17 52 5 3 4 10 9
King-Moe IV 117 19 87 18 5 8 29 9
King-Moe V 7 42 1 3 3 6 20
Total of the general table
400 20 248 94 31 27 117 12
Table 2. Percentage improvement of the Cobb and Rotation.
Type of curve Average Cobb Average PR in function of the curve Average rotation
Final
Grade Average PR <20º [20º-30º] [31º-40º] >40º
Final
Grade Average PR
King-Moe I 5 75 84 61 52 50 4 76
King-Moe II 16 45 65 39 30 18 5 63
King-Moe III 6 76 85 35 35 36 3 86
King-Moe IV 7 74 84 56 28 34 2 84
King-Moe V 27 37 63 33 32 13 41
Total of the general table
9 67 81 50 35 31 4 74
PR: Relative recuperation percentage
Table 3. Analysis of the variance with a 1% level of significance
Origino f the variations
Sum of the squares
Grades of =freedom=
Average of the cuadrados
F Probability Critical value of F
=Filas= 8170 161 50,7469 3,1950 0,0000 1,4453
Columns 185 1 185,2623 11,6639 0,0008 6,7949
=Error= 2557 161 15,8835
Total 10913 323

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
14
Figure 1. FED system. A Manual techniques used in research with animals to correct the experimental scoliosis.
(46,47,48,49,62)
B The FED unit inspired the research and experiments. C Sketch of the overall corrective forces on the rachis generated in the FED unit.
D Sketch –detail of the incidente of the corrective forces on the anatomical enclaves
rib-vertebrae, neurcentral and epiphyseal cartilages -
A B C D
Table 4. Value of the average Risser throughout the 12
month treatment.
Risser X Initial Risser Risser 12
months
0 0 0
0,5 0 1
1 1 1
1,5 1 2
2 2 2
2,5 2 3
3 3 3
3,5 3 4
4 4 4
4,5 4 5
5 5 5
Table 5. Average Risser and recuperation percentages (PR) of the Cobb and the rotation.
Risser X PR average of the Cobb at
12 months
PR average of the rotation at
12 months
0 88,56 88,41
0,5 74,03 76,62
1 74,99 100,00
1,5 57,27 70,83
2 66,31 33,33
2,5 46,77 67,44
3 66,49 74,05
3,5 60,37 70,50
4 40,95 60,21
4,5 64,56 70,08
5 56,09 83,88

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
15
Figure 2. Average of the percentage of recuperation of the
Cobb in function of the initial curve. Figure 3. Average of the percentage of recuperation of the
Cobb in function of the initial King-Moe
Figure 4. Average of the percentage of recuperation of the rotation in function of the initial King-Moe (n=117 patients)
Figure 5. Regression line. We note a dependence between the recuperation average and the average Risser after
12 months of treatment using the FED method.
81
50
3531
0
50
100
<20º [20º-30º] [31º-40º] >40º
%
75
45
76 74
37
0
50
100
I II III IV V
King-Moe%
76
63
86 84
41
0
50
100
I II III IV V
King-Moe
%

Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
16
.
y = -5,3819x + 76,763
R2 = 0,4474
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6
AVERAGE RISSER
%
Figure 6. X-ray of a 12 year old girl with progressive idiopathic scoliosis. She had two sessions a week of the FED method
and the rest of the week analytical kinesitherapy at home. Evolution :
A B C
X-ray: A 06/2003: T11-L4 26º Risser 0 Raimondi L2 10º
B 01/2004: T11-L4 19º Risser 1,5 Raimondi L2 8º
C 11/2004: T11-L4 15º Risser 2,5 Raimondi L2 3º
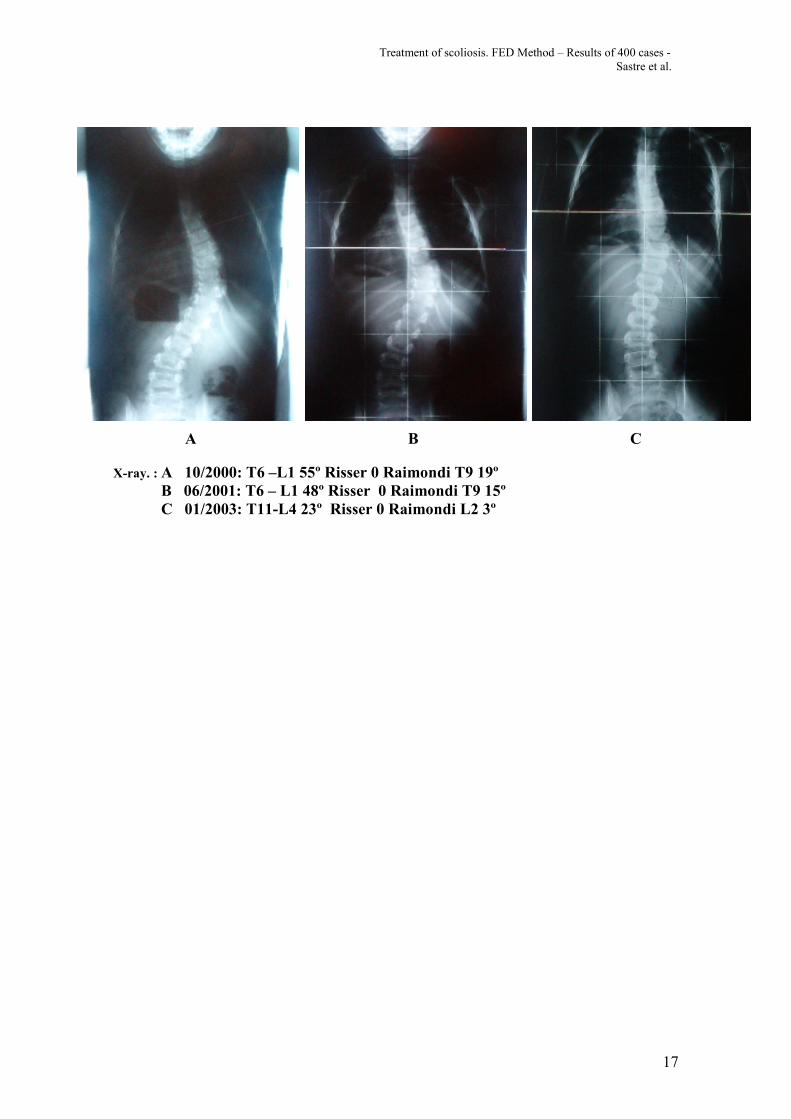
Figure 7. X-ray of a 5 year old boy with progressive idiopathic scoliosis. Sessions from Monday to Friday using FED
method. Weekends he had analytical kinesitherapy at home. Evolution:
Treatment of scoliosis. FED Method – Results of 400 cases -
Sastre et al.
17
A B C
X-ray. : A 10/2000: T6 –L1 55º Risser 0 Raimondi T9 19º
B 06/2001: T6 – L1 48º Risser 0 Raimondi T9 15º
C 01/2003: T11-L4 23º Risser 0 Raimondi L2 3º


















