Treatment of multiple sclerosis with Copolymer-1 (Copaxone®): implicating mechanisms of Th1 to...
9
Ž . Journal of Neuroimmunology 92 1998 113–121 ž w / Treatment of multiple sclerosis with Copolymer-1 Copaxone : implicating mechanisms of Th1 to Th2rTh3 immune-deviation Ariel Miller a,b,c, ) , Sarah Shapiro a,d , Rosa Gershtein a , Amalia Kinarty d , Hanna Rawashdeh a,b , Silvia Honigman b,c , Nitza Lahat d,c a Neuroimmunology Research Unit and Multiple Sclerosis Center, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israel b Department of Neurology, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israel c Faculty of Medicine and Rappaport Institute for Research in the Medical Sciences, Technion - Israel Institute of Technology, Haifa, Israel d Molecular Immunology Research Unit, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israel Received 19 May 1998; revised 28 July 1998; accepted 28 July 1998 Abstract Ž w . The synthetic polypeptide copolymer-1 Cop-1; Copaxone ; Glatiramer Acetate has been recently approved as an effective treatment Ž . in relapsing multiple sclerosis MS . A large body of evidence demonstrates that Cop-1 induces active suppression of CNS-inflammatory disease in animal models. However, Cop-1-mediated suppressor mechanisms have not yet been elucidated in humans. A 12-month open study following clinical and immunological parameters of ten relapsing MS patients treated with Cop-1 is presented. Relapse rates and Ž . disability scores EDSS were evaluated prior to and after 12 months of treatment. The immunological parameters assessed prior to and at Ž . 3 months’ interval during treatment included serum levels of soluble IL-2 receptor sIL-2R and IL-10 as well as leukocyte cytokine mRNA expression of TNFa , IL-4 and TGF-b. Copaxone treatment was found to lead to a significant reduction in the mean annual Ž . relapse rate from 1.4 prior to treatment to 0.6 during treatment and stabilization of disability in 90% of the patients. The treatment was accompanied by an elevation of serum IL-10 levels, suppression of the pro-inflammatory cytokine TNFa mRNA, and an elevation of the anti-inflammatory cytokines TGF-b and IL-4 mRNAs in PBLs. These results suggest that the beneficial clinical effects of Copaxone in MS patients may be attributed to changes in activation of T cell subsets and a shift from Th1 to Th2rTh3 cytokine profile, probably leading to Cop-1-driven mechanisms of bystander suppression. q 1998 Elsevier Science B.V. All rights reserved. Keywords: Multiple sclerosis; Immunomodulation; Copolymer-1; Th1rTh2; Cytokines; Bystander suppression 1. Introduction Ž . Multiple sclerosis MS is an inflammatory disease of Ž . the central nervous system CNS of suspected autoim- mune origin. Studies in MS and its animal model, experi- Ž . mental autoimmune encephalomyelitis EAE , suggest that MS results from immune-dysregulation and aberrant acti- vation, whereby CNS myelin proteins serve as autoanti- Abbreviations: CNS, central nervous system; Cop-1, Copolymer-1; EAE, experimental autoimmune encephalomyelitis; IL, interleukin; MS, multiple sclerosis; MBP, myelin basic protein; PBL, peripheral blood leukocytes; sIL-2R, soluble IL-2 receptor; TGF, transforming growth factor; Th, T helper cells; TNF, tumor necrosis factor ) Corresponding author. Tel.: q972 4 8250851; fax: q972 4 8250909; e-mail: [email protected] gens leading to a T cell-driven inflammatory and demyeli- Ž nating process Martin et al., 1992; Steinman et al., 1994; . Hafler and Weiner, 1995 . The immune-dysregulation in MS involves both cellular and humoral arms of the im- mune response and can be identified in the peripheral Ž . blood, cerebrospinal fluid CSF and CNS. These include: Ž . defective immune-suppressor responses Antel et al., 1986 ; elevated T cell reactivity against various myelin antigens, Ž . such as myelin basic protein MBP , proteolipid protein Ž . Ž . PLP or myelin oligodendrocyte glycoprotein MOG Ž . Steinman et al., 1995 ; increased expression of MHC Ž . class II molecules on antigen presenting cells APCs , monocytes, endothelial as well as glial cells; elevated Ž q levels of circulating memory T cells CD4 rIL- q q .Ž 2R rCD45RO Martin et al., 1992; Steinman et al., . 1994; Hafler and Weiner, 1995; Inobe et al., 1996 ; raised 0165-5728r98r$ - see front matter q 1998 Elsevier Science B.V. All rights reserved. Ž . PII: S0165-5728 98 00191-X
-
Upload
ariel-miller -
Category
Documents
-
view
214 -
download
0
Transcript of Treatment of multiple sclerosis with Copolymer-1 (Copaxone®): implicating mechanisms of Th1 to...

Ž .Journal of Neuroimmunology 92 1998 113–121
ž w /Treatment of multiple sclerosis with Copolymer-1 Copaxone :implicating mechanisms of Th1 to Th2rTh3 immune-deviation
Ariel Miller a,b,c,), Sarah Shapiro a,d, Rosa Gershtein a, Amalia Kinarty d,Hanna Rawashdeh a,b, Silvia Honigman b,c, Nitza Lahat d,c
a Neuroimmunology Research Unit and Multiple Sclerosis Center, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israelb Department of Neurology, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israel
c Faculty of Medicine and Rappaport Institute for Research in the Medical Sciences, Technion - Israel Institute of Technology, Haifa, Israeld Molecular Immunology Research Unit, Lady DaÕis Carmel Medical Center, 7 Michal Street, 34362 Haifa, Israel
Received 19 May 1998; revised 28 July 1998; accepted 28 July 1998
Abstract
Ž w .The synthetic polypeptide copolymer-1 Cop-1; Copaxone ; Glatiramer Acetate has been recently approved as an effective treatmentŽ .in relapsing multiple sclerosis MS . A large body of evidence demonstrates that Cop-1 induces active suppression of CNS-inflammatory
disease in animal models. However, Cop-1-mediated suppressor mechanisms have not yet been elucidated in humans. A 12-month openstudy following clinical and immunological parameters of ten relapsing MS patients treated with Cop-1 is presented. Relapse rates and
Ž .disability scores EDSS were evaluated prior to and after 12 months of treatment. The immunological parameters assessed prior to and atŽ .3 months’ interval during treatment included serum levels of soluble IL-2 receptor sIL-2R and IL-10 as well as leukocyte cytokine
mRNA expression of TNFa , IL-4 and TGF-b. Copaxone treatment was found to lead to a significant reduction in the mean annualŽ .relapse rate from 1.4 prior to treatment to 0.6 during treatment and stabilization of disability in 90% of the patients. The treatment was
accompanied by an elevation of serum IL-10 levels, suppression of the pro-inflammatory cytokine TNFa mRNA, and an elevation of theanti-inflammatory cytokines TGF-b and IL-4 mRNAs in PBLs. These results suggest that the beneficial clinical effects of Copaxone inMS patients may be attributed to changes in activation of T cell subsets and a shift from Th1 to Th2rTh3 cytokine profile, probablyleading to Cop-1-driven mechanisms of bystander suppression. q 1998 Elsevier Science B.V. All rights reserved.
Keywords: Multiple sclerosis; Immunomodulation; Copolymer-1; Th1rTh2; Cytokines; Bystander suppression
1. Introduction
Ž .Multiple sclerosis MS is an inflammatory disease ofŽ .the central nervous system CNS of suspected autoim-
mune origin. Studies in MS and its animal model, experi-Ž .mental autoimmune encephalomyelitis EAE , suggest that
MS results from immune-dysregulation and aberrant acti-vation, whereby CNS myelin proteins serve as autoanti-
Abbreviations: CNS, central nervous system; Cop-1, Copolymer-1;EAE, experimental autoimmune encephalomyelitis; IL, interleukin; MS,multiple sclerosis; MBP, myelin basic protein; PBL, peripheral bloodleukocytes; sIL-2R, soluble IL-2 receptor; TGF, transforming growthfactor; Th, T helper cells; TNF, tumor necrosis factor
) Corresponding author. Tel.: q972 4 8250851; fax: q972 4 8250909;e-mail: [email protected]
gens leading to a T cell-driven inflammatory and demyeli-Žnating process Martin et al., 1992; Steinman et al., 1994;
.Hafler and Weiner, 1995 . The immune-dysregulation inMS involves both cellular and humoral arms of the im-mune response and can be identified in the peripheral
Ž .blood, cerebrospinal fluid CSF and CNS. These include:Ž .defective immune-suppressor responses Antel et al., 1986 ;
elevated T cell reactivity against various myelin antigens,Ž .such as myelin basic protein MBP , proteolipid protein
Ž . Ž .PLP or myelin oligodendrocyte glycoprotein MOGŽ .Steinman et al., 1995 ; increased expression of MHC
Ž .class II molecules on antigen presenting cells APCs ,monocytes, endothelial as well as glial cells; elevated
Ž qlevels of circulating memory T cells CD4 rIL-q q. Ž2R rCD45RO Martin et al., 1992; Steinman et al.,
.1994; Hafler and Weiner, 1995; Inobe et al., 1996 ; raised
0165-5728r98r$ - see front matter q 1998 Elsevier Science B.V. All rights reserved.Ž .PII: S0165-5728 98 00191-X

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121114
levels of cell surface adhesion molecules on T cells andŽmacrophages Antel and Owens, 1993; Cannella and Raine,
.1995; Weller et al., 1996 . The elevated levels of adhesionmolecules correlate with the degree of blood brain barrierŽ . ŽBBB eruption Sharief et al., 1993; Rieckmann et al.,
.1994 . MS is also characterized by elevated levels ofpro-inflammatory cytokines such as tumor necrosis factor-aŽ . Ž . Ž .TNFa , interleukin IL -1, IL-2 and interferon IFN -g, in
Žthe peripheral blood Sharief and Hentges, 1991; Trotter et. Žal., 1991; Hartung et al., 1995 , CSF Hauser et al., 1990;. ŽRudick and Ransohoff, 1992 and in brain lesions Hof-
.mann et al., 1980 . The association of these inflammatoryŽcytokines with disease activity Hauser et al., 1990; Sharief
and Hentges, 1991; Rudick and Ransohoff, 1992; Hartung. qet al., 1995 implies that CD4 T cells of the T helper type
Ž . Ž .1 Th1 Voshuhl et al., 1993; Windhagen et al., 1996 andŽ .macrophages Cua et al., 1995; van der Laan et al., 1996 ,
play a pivotal role in the immunopathogenesis of the CNSdemyelinating disease. Moreover, the relative low levelsand defective production of IL-10, IL-4 and TGF-b in
Žpatients with active multiple sclerosis Mokhtarian et al.,. Ž1994 , and their protective role in EAE Johns et al., 1991;
Kuruvilla et al., 1991; Racke et al., 1991; Kennedy et al.,1992; Van der Veen and Stohlman, 1993; Fabry et al.,
.1995; Falcone and Bloom, 1997 , suggest that T cells ofthe Th2 and Th3 phenotypes, and their characteristic cy-tokine products may be involved in induction of remissionand in suppression of the disease process.
Increased understanding of the animal model and thehuman demyelinating disease has recently led to the imple-mentation of a number of immunomodulatory strategies in
Žthe treatment of MS. These include: IFN-b-1b IFNb
.multiple sclerosis study group, 1993; Paty, 1993 , IFN-b-1aŽ .Jacobs et al., 1994; Pozzilli et al., 1996 , as well as the
Ž wsynthetic polypeptide copolymer-1 Cop-1; Copaxone ;.Glatiramer Acetate , originally synthesized with the aim of
mimicking the myelin antigen MBP. Cop-1 treatment sup-Žpresses EAE induced in a variety of species Teitelbaum et
.al., 1997 , and has been demonstrated to reduce clinicaldisease activity in humans with relapsing–remitting MSŽAbramsky et al., 1977; Bornstein et al., 1987; Johnson et
. Ž .al., 1995 . The mechanism s of Cop-1 action are not fullyelucidated. It has been suggested that following binding to
Ž .MHC class II molecules on antigen presenting cells APCs ,Cop-1 competes with myelin antigens for presentation byAPC, thus preventing myelin-specific T cell activationŽRacke et al., 1992; Teitelbaum et al., 1992; Fridkis-Hareli
.et al., 1994; Teitelbaum et al., 1997 . An additional mech-anism suggested to be involved in Cop-1 immunomodula-tory activity is the induction of specific suppressor cellsŽ .Teitelbaum et al., 1997 . However, Cop-1-driven suppres-sor mechanisms have not yet been clarified in patients. Tofurther evaluate Cop-1 immunomodulatory activities, weconducted a clinical and immunological study in relapsingremitting MS patients treated with Copaxonew for 12months in an open trial.
2. Materials and methods
2.1. Patients and treatment
Ž .Ten patients nine female and one male , age rangeŽ .21–58 years mean, 37.5"11.94 years , with clinically
definite and laboratory supported relapsing remitting MSŽ .according to the criteria of Poser et al. Poser et al., 1983
were followed at the MS Center, Lady Davis CarmelHospital, Haifa, Israel, in an open trial. Mean diseaseduration was 9.4 years. Inclusion criteria included a historyof at least two clearly identified and documented relapsesin the 2 years prior to study entry; all patients wereambulatory, defined by an expanded disability status scaleŽ . Ž .EDSS Kurtzke, 1993 of 0 through 5.0; patients had notbeen corticosteroid treated for at least 3 months prior totrial. Patients were excluded if they had ever receivedimmunosuppressive therapy with cytotoxic activityŽ .azathiorine, cyclophosphamide or cyclosporine or lym-phoid irradiation. Additional exclusion criteria includedpregnancy or lactation, and all women were required to usean adequate contraceptive method. Signed informed con-sent was obtained from patients and the study was ap-proved by the Ethical Committee, Lady Davis Carmel
Ž .Medical Center. Age and sex matched controls ns6were included in all immunological assays. Copaxonew , 20
Žmg supplied by Teva Pharmaceutical Industries, Petach.Tiqva, Israel , was daily self administered, subcutaneously,
under a protocol approved by the Israeli Health Adminis-tration.
Clinical outcome measures were: annual relapse rate,the absolute changes in EDSS score and the proportion ofpatients with ‘improved’, ‘stable’ or ‘worsened’ clinicaldisability, by the end of the treatment. Relapse was definedas the appearance or reappearance of one or more neuro-logical abnormalities that persisted for at least 24 h, andhad been preceded by a stable or improving neurologicalstate of at least 30 days.
2.2. Serum leÕels of cytokines
Ž .The IFN-g, IL-2 Endogen, MA, USA , sIL-2R, IL-4Ž .and IL-10 high sensitivity, R&D Systems, CA serum
levels were determined by commercial ELISA kits. Datawas calculated from duplicate samples on the basis oftitration curves obtained from standards supplied by themanufactures.
2.3. Peripheral blood leukocytes
Ž .Peripheral blood 10 ml was collected in EDTA andŽ .immediately placed in ice. Red blood cells RBC wereŽ .spun down at 100=g, 48C and leukocytes PBL were
then pelleted from the plasma by centrifugation at 650=g,

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121 115
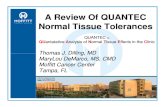
Fig. 1. Copolymer-1 treatment leads to reduced annual relapse rate in MSpatients. The number of relapses for each patient during the 2 years priorŽ . Žpre to treatment and during 1 year of treatment are presented figure on
.left; ≠ designates start of treatment . Figure on the right shows meanŽ .annual relapse rate prior to and after 1 year of treatment ps0.001 .
48C, for 10 min. Residual RBC were lysed with TE bufferŽ .10 mM Tris–HCl and 1 mM EDTA, pH 8.0 . RNA wasextracted from either fresh or liquid nitrogen frozen PBL.
2.4. RT-PCR
Total cellular RNA was isolated from PBL with Tri-Re-Ž .agent Medical Research Center, OH according to the
manufacturer’s instructions. RNA samples were washedtwice in 75% ethanol, air dried and suspended in 10 mlRNase free TE buffer. RNA quantity and quality weredetermined by spectrophotometric absorbance at 260r280nm. RNA samples were stored at y708C. Complementary
Ž .DNA cDNA was prepared by reverse transcription at378C for 60 min in 50 ml reaction mixture containing 2 mgRNA, 400 U Moloney Murine leukemia virus reverse
Ž .transcriptase Amersham, OH in the presence of RNA-Ž . Žguard Pharmacia, Germany and oligo-hexamers Phar-
.macia, NJ . The enzyme was than inactivated and theintegrity of the RNA was assessed by amplifying 1 ml
Ž .cDNA using G3PDH specific primers Clontech, CA . TheŽ . Ž .polymerase chain reaction PCR mix 25 ml volume
Žincluded reaction buffer 10 mM Tris–HCl, 50 mM KCl,.1.5 mM MgCl , 0.1% Triton X-100 0.2 mM each dNTP2
Fig. 2. Copolymer-1 treatment leads to stabilization of clinical disability.Disability of patients, assessed and graded according to Kurtzke’s ex-
Ž .tended disability status scale EDSS scores , were evaluated prior toŽ . Ž .treatment pre and after 1 year of Cop-1 treatment 12 m .
Fig. 3. Copolymer-1 treatment is associated with reduction in serum IL-2Ž .soluble receptor sIL-2R . Serum sIL-2R levels were determined by
ELISA in MS patients, prior to and during Cop-1 treatment, and inhealthy controls. The values presented were calculated using a standardtitration curve and represent mean values for each group"standard errorof mean.
Ž . X XSigma, MO , 0.4 mM 5 and 3 primers and 1U DNA TaqŽ .polymerase Appligene, France . Thirty-five cycles of PCR
amplification were performed, each consisting of denatura-tion at 948C, annealing at 688C, and extension at 728C in a
Ž .thermal cycler MJ Research, MA, USA . PCR productswere visualized by UV following electrophoresis of prod-
Ž .ucts in ethidium bromide stained 3% agarose gels Sigma .ŽStandard molecular size markers, negative controls PCR
. Žmix without sample cDNA and positive controls standard.cDNA supplied by manufacturer, Clontech were run with
each PCR assay.
2.5. Semi-quantitation of cytokine mRNA
ŽSemi-quantitative assessment of cytokine IL-4, TNFa ,.and TGF-b mRNA was performed by parallel PCR using
Ž .cytokine specific primers and G3PDH primers Clontech .To ensure that amplification was being performed at linear
Žphase, three different quantities of cDNA 2, 1, and 0.5 mlcDNA for G3PDH amplification; 4, 2, and 1 ml cDNA forTNFa and TGF-b amplification; 6, 4, and 2 ml for IL-4
.amplification, determined in preliminary experiments wereutilized in all assays. PCR was performed as above using
Fig. 4. Copolymer-1 treatment leads to elevation in serum IL-10. SerumIL-10 levels were determined in MS patients, prior to and during Cop-1treatment, and in healthy controls by ELISA. The values presented werecalculated using a standard titration curve and represent mean values foreach group"standard error of mean.

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121116
Ž .appropriate annealing temperatures 60–658C for eachcytokine. Resulting PCR products were visualized by UVfollowing electrophoresis, intensity of bands was measured
Žby video densitometry Bio Imaging Systems, Applitec,.Israel and the ratio between sample to G3PDH products
was calculated.
Fig. 5. Copolymer-1 treatment leads to modulation of cytokine mRNA expression in peripheral blood leukocytes. Semi-quantitative assessment of cytokineŽ . Ž .TNFa , A; IL-4, B; TGF-b, C mRNA from PBL was performed by RT-PCR using three concentrations of cDNA for each time period as described in
Ž . Ž .Section 2. Housekeeping gene, G3PDH, was amplified in parallel. Histogram upper panel shows mean ratio "standard error between densitometricintensity of specific cytokine to G3PDH PCR products for 10 treated MS patients at each time period examined and for four controls. Results of
Žrepresentative samples obtained at three different times presprior to treatment; 3 and 6 months; NCsnegative and PCspositive controls for PCR.amplification of Cop-1 treatment, are shown in bottom panel of figures.

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121 117
2.6. Statistical eÕaluation
Mean relapse rate and changes from baseline accordingto EDSS, were assessed using repeated-measures ANOVA.Statistical significance of data was determined using Stu-dent’s t-test for paired analysis of parameters with normaldistribution when comparing a single parameter at differ-ent times and Ranked Signed Wilcoxon for comparison ofgroups. P values of -0.05 were considered significant.
3. Results
3.1. Copolymer-1 treatment leads to reduced annual re-lapse rate
During the 1-year follow-up the Cop-1 treated patientsŽ .had six confirmed relapses Fig. 1 . The mean annual
relapse rates was 0.6 during the treatment as compared to1.4 prior to Cop-1 therapy, a 57% reduction, which was
Ž . Ž .statistically significant ps0.001 . Five 50% MS pa-tients receiving Cop-1 were relapse-free throughout thetrial.
3.2. Stabilization of neurological disability by Copolymer-1treatment
Among the 10 patients receiving Cop-1, neurologicaldisability improved in four, was stable in five, and wors-
Ž .ened in only one patient Fig. 2 . Thus, 90% of the patientstreated with Cop-1 were free of disease progression. Noclinically significant adverse event was noted. The mostcommonly recognized adverse event during treatment wasa localized injection-site reaction consisting of mild ery-themia and induration, which sometimes persisted for sev-eral days.
3.3. Modulation of serum sIL-2R and IL-10
ŽThe levels of sIL-2R in the sera were higher though.not of statistical significance, ps0.7 in pretreated MS
Ž .patients compared to healthy controls Fig. 3 . Slightchanges, including first a significant elevation at 3 monthsŽ .ps0.04 and eventually a slight decrease in the mean
Žvalue of this receptor at 12 months of treatment ps0.43;.pre vs. 12 months were observed. At all times a wide
variability in the level of sIL-2R was found amongst thepatients.
The mean level of serum IL-10 was slightly lower,though not significant, in pre-treated MS patients, com-
Ž . Ž .pared to healthy controls ps0.4 Fig. 4 . A 2-foldŽ .significant ps0.04 increase in the mean level of this
cytokine was observed at 3 months of treatment, as com-pared to baseline levels. However, the increment was
Ž .attenuated at 6 and 12 months of treatment ps0.16 . Itshould be noted that no detectable levels of IFN-g, IL-2and IL-4 were observed in these serum samples.
3.4. Cytokine mRNA expression of TNFa , IL-4 and TGF-bin PBL
Profound differences in baseline cytokine mRNAs ex-pression were observed in PBL derived from MS patientsas compared to controls and marked changes were identi-
Ž .fied in patients during Cop-1 treatment Fig. 5 . ElevatedmRNA expression levels of the pro-inflammatory cytokineTNFa were observed in all MS patients prior to treatment,whereas no detectable levels were observed in healthycontrols. The TNFa levels decreased in nine of the 10 MSpatients following Cop-1 treatment and after 12 months of
Žtreatment there was a 4-fold, statistically significant p-.0.004 , decrease in the mean mRNA level of this cytokine
Ž .compared to the mean level prior to treatment Fig. 5A .The changes in TNFa mRNA were accompanied by
enhanced mRNA expression of the anti-inflammatory cy-Ž .tokines IL-4 and TGF-b Fig. 5B–C . In 70% of patients
no mRNA expression for IL-4 was observed prior toCop-1 administration. After 12 months of treatment, sevenof the 10 patients showed IL-4 mRNA expression in PBLŽ .Fig. 5B . Following 3 and 6 months of treatment, theexpression of this cytokine was significantly elevated in
Žcomparison to pre-treatment levels ps0.05 and ps0.03,.respectively . Although still higher than baseline or control
levels, after 12 months of treatment the levels of IL-4mRNA were more attenuated. TGF-b mRNA expressionwas observed in 80% of MS patients prior to Cop-1
Ž .treatment Fig. 5C . However a 5-fold, statistically signifi-Ž .cant ps0.03 increase in the mean level of this cytokine
was observed after 6 months of treatment. At 12 months oftreatment, the differences between MS treated patients and
Žhealthy controls were still statistically significant ps. Ž .0.02 though they were not significant ps0.38 com-
pared to pre-treatment values.
4. Discussion
The immunological follow-up carried out in the presentstudy adds additional insight into the mechanisms of Cop-1immunomodulatory activities in MS patients and is, to thebest of our knowledge, the first report of regulatory mech-anisms of Cop-1 in humans. Although only 10 patientswere studied in an open trial, our results demonstratingthat Cop-1 treatment leads to a significant reduction of themean relapse rate as well as stabilization of disability,
Žconfirm previous published clinical studies Abramsky et.al., 1977; Bornstein et al., 1987; Johnson et al., 1995 . The
association of the clinical reduction of disease activity withthe shift of cytokine profile, observed in the present work,may contribute to our understanding of the immunomodu-latory effects mediated by Cop-1.
It has been proposed that the predominant mechanismunderlying the immunomodulatory activities of Cop-1 re-

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121118
sides in the immunological cross-reactivity of Cop-1 withMBP and its competition with MBP for MHC class IIpresentation. This may result in the inhibition of MBP-
Žspecific T cell activation Racke et al., 1992; Teitelbaum etal., 1992; Fridkis-Hareli et al., 1994; Teitelbaum et al.,
.1997 . Nevertheless, molecular mimicry to MBP andblocking of MBP-specific autoimmune T cells, does notexplain recent observations suggesting that the effect ofCop-1 in EAE is not restricted to a particular encephalito-gen, but rather suppresses disease induced by various
Ž .myelin antigens such as PLP Teitelbaum et al., 1996 andŽ .MOG Ben-Nun et al., 1996 . The suppressive activity of
Cop-1 has however, been shown to be organ-specific andlimited to inflammatory and autoimmune diseases involv-ing CNS-myelin, such as EAE, while no effect was
Ždemonstrated in SLE or other autoimmune diseases Arnon.et al., 1996 . Studies in experimental animals have indeed
suggested that the effectiveness of Cop-1 in preventingEAE results also from the induction of antigen-specific
Žsuppressor T cells that cross-react with MBP Teitelbaum.et al., 1997 . Cop-1 specific suppressor T cells isolated
form rodents showed polarized secretion of Th2 typeŽ .cytokines Aharoni et al., 1997 . However, active suppres-
sion as a possible mechanism for the beneficial effect ofCop-1 in humans with MS has not yet been described.
q Ž .CD4 T helper Th cells can be divided into subsetsbased on their characteristic cytokine secretion patterns
Žand effector functions Mosmann and Coffman, 1987;.Street et al., 1990 . Cytokines produced by Th1 cells
Ž .IL-12, IFN-g, IL-2 and TNFa are inflammatory media-tors of various autoimmune processes, including autoim-mune demyelinating diseases where oligodendrocytes are a
Žtarget for immune attack Voshuhl et al., 1993; Windhagen. Žet al., 1996 . Cytokines produced by Th2 cells IL-4 and
. Ž .IL-10 or Th3 cells TGF-b mediate antibody production,anti-inflammatory cascade and resolution of inflammatory
Žand autoimmune processes Johns et al., 1991; Kuruvilla etal., 1991; Racke et al., 1991; Kennedy et al., 1992; Vander Veen and Stohlman, 1993; Fabry et al., 1995; Falcone
.and Bloom, 1997 . Our present study demonstrates thattreatment of MS patients with Cop-1 leads to modulationin serum sIL-2R and in TNFa mRNA expression in PBL,and at the same time an elevation of serum IL-10 as wellas IL-4 and TGF-b mRNA expression. sIL-2R, generally amarker of T cell activation, binds secreted IL-2, thusprobably leading eventually to the inhibition of T cellactivation. This inhibition as well as the shift from Th1 to
Ž .Th2rTh3 type immune response implies that mechanism sof active suppression mediated by regulatory cytokinesmay be involved in suppression of MS by Cop-1. Of noteis the more prominent induction of Th2rTh3 cytokinesduring the first 6 months of Cop-1 treatment which waslater attenuated. This finding may be due to the stabiliza-tion of autoreactivity and maintained suppression of theTh1 response, manifested by the continued low levels ofTNFa during the treatment.
Modulation of an immune response from one dominatedby excessive Th1 activity to one dominated by the protec-tive cytokines produced by Th2rTh3 cells, has beendemonstrated as an effective immunomodulatory and ther-apeutic strategy in certain experimental autoimmune dis-eases. For example, IL-4 treatment in EAE resulted inamelioration of clinical disease, inhibition of the synthesisof inflammatory cytokines, the induction of MBP-specificTGF-b-producing Th2rTh3 cells, and diminished CNS
Ž .demyelination Van der Veen and Stohlman, 1993 . Simi-larly, induction of IL-10 mRNA expression was reportedto correlate with recovery in EAE. Although in some
Žreports IL-10 failed to suppress EAE Cannella et al.,.1996 , others have demonstrated that Th2 cells producing
IL-10 inhibit encephalitogenic Th1 cells and suppress EAEŽVan der Veen and Stohlman, 1993; Windhagen et al.,
.1996 . The induction of TGF-b demonstrated in our study,in association with the clinical efficacy of Cop-1 treatmentis in-line with recent reports regarding the importance ofthis cytokine in down-regulating autoimmunity. TGF-b, amultifunctional anti-inflammatory cytokine with immune-
Ž .suppressive effects on T cells in vitro Merrill et al., 1989 ,was successfully implemented as treatment of both acute
Žand chronic EAE Johns et al., 1991; Kuruvilla et al.,.1991; Racke et al., 1991 .
Reversal of the autoimmune response from Th1 to Th2appears to be a common denominator of a number of novelimmune-therapeutic strategies, both in EAE and in MS.
Ž .Cytokine-mediated immune-deviation Racke et al., 1994has been demonstrated also in humans during IFN-b treat-
Žment, the first treatment found to be effective in MS IFNb
.multiple sclerosis study group, 1993; Paty, 1993 . Cy-tokine switching was also demonstrated during vaccination
Ž .with naked DNA encoding T-cell receptor TCR Vb 8.2Ž .Waisman et al., 1996 , using Retinoid for the treatment of
Ž .EAE Racke et al., 1995 , Pentoxifilline in relapsing–re-Ž .mitting MS Rieckmann et al., 1996 and Linomide in
Ž .progressive MS Karussis et al., 1996 . It is of interest thatsome of the beneficial effects of glucocorticosteroids in thetreatment of acute exacerbation, appear to involve inhibi-tion of TNFa and lymphocyte adhesion as well as theinduction of anti-inflammatory Th2rTh3 cytokines such as
Ž .TGF-b Pitzalis et al., 1997 .Cop-1 is a prototype of antigen-driven immune-inter-
vention for the treatment of organ-specific autoimmunity.In addition to Cop-1, antigen-driven immune-modulationmay be elicited by other therapeutic strategies such as oraltolerance, altered peptide ligands, and vaccination with
Ž .T-cell receptor TCR peptides. In all these approaches,including Cop-1, as shown previously in the EAE modeland in the present study, there is evidence for the involve-ment of immune deviation and bystander suppression
Žmechanisms Miller et al., 1991; Karin et al., 1994; Van-denbark et al., 1996; Aharoni et al., 1997; Teitelbaum et
.al., 1997; Weiner, 1997 . Extensive studies in oral toler-Ž .ance Weiner, 1997 , have shown that it may not be

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121 119
necessary to identify the target autoantigen to suppress anorgan-specific autoimmune disease via antigen-driven tol-erance; it is necessary only to administer a protein capableof inducing regulatory cells that secrete suppressive cy-tokines upon encountering the autoantigen at the targetorgan. This characteristic phenomenon of suppressor cy-tokines, that may shut-down the inflammatory processindependently of the primary autoantigen or of theantigen-specificity of the autoimmune cells, has been de-
Žfined as antigen-driven bystander suppression Miller et.al., 1991 . Furthermore, therapeutic strategies implicating
mechanisms of bystander suppression may solve the prob-lem of spreading autoimmunity to additional autoantigens
Žduring the course of the ongoing disease Lehmann et al.,.1992 . Thus, the Th1 to Th2rTh3 immune-deviation
demonstrated in our study, implicating mechanisms ofbystander suppression, may explain the effects of Cop-1 on
ŽPLP and MOG-induced experimental diseases Ben-Nun et.al., 1996; Teitelbaum et al., 1996 . Immune-reactivity to
these myelin antigens as well as spreading autoimmunityto other putative neuro-antigens may be downregulated bythe anti-inflammatory mediators released at the microenvi-ronment of the target organ. It should be noted, however,that a shift from a Th1 to a Th2 cytokine productionphenotype may carry the risk of elicitation of the humoralarm of the immune response in a dysregulated mannerwith potential aggravation of the autoimmune process.
Ž .Lafaille et al. Lafaille et al., 1997 recently reported thatMBP-specific Th2 cells cause EAE in immune-deficienthosts rather than protect them from the disease. Similarly,Genain et al. have demonstrated that enhanced titers ofautoantibodies to MOG may mediate the late complica-
Žtions of immune-deviation therapy in EAE Genain et al.,.1996 . Hence, careful follow-up, both clinical as well as
immunological parameters may be required in patientstreated with therapeutic strategies implicating immune-de-viation, in order to identify such possible delayed compli-cations.
In conclusion, the beneficial clinical effects of Copa-xonew in MS patients, demonstrated also in the presentstudy, may be attributed to the induction of Cop-1-specific
Ž .regulatory Th2rTh3 cells cross-reactive with MBPwhich, upon encountering MBP at the target organ, secretanti-inflammatory cytokines, leading to bystander suppres-sion. Further understanding of the mechanisms implicatedin the immune-modulatory effects of Cop-1 as well asother immunoregulatory drugs, may contribute to the de-sign of future therapeutic cocktails and combination thera-
Ž .pies Milo and Panitch, 1995 .
Acknowledgements
We thank Drs. Rivka Riven-Kreitman and Nora Tarcicfor helpful discussions. This work was supported by a
Ž .grant from Teva Pharmaceutical Industries, Israel and the
combined research grant from the Ministry of Health,Carmel Medical Center and the Technion, Israel Instituteof Technology, Israel.
References
Abramsky, O., Teitelbaum, D., Arnon, R., 1977. Effect of a syntheticŽ .polypeptide Copolymer 1 on patients with multiple sclerosis and
acute disseminated encephalomyelitis: preliminary report. J. Neurol.Sci. 31, 433–438.
Aharoni, R., Teitelbaum, D., Sela, M., Arnon, R., 1997. Copolymer 1induces T cells of the T helper type 2 that crossreact with myelinbasic protein and suppress experimental autoimmune encephalomyeli-tis. Proc. Natl. Acad. Sci. USA 94, 10821–10826.
Antel, J.P., Owens, T., 1993. The attraction of adhesion molecules. Ann.w xNeurol. 34, 123–124, editorial .
Antel, J.P., Bania, M.B., Reder, A., Cashman, N., 1986. Activatedsuppressor cell dysfunction in progressive multiple sclerosis. J. Im-munol. 137, 137–141.
Arnon, R., Sela, M., Teitelbaum, D., 1996. New insights into themechanism of action of copolymer 1 in experimental allergic en-cephalomyelitis and multiple sclerosis. J. Neurol. 243, S8–13.
Ben-Nun, A., Mendel, I., Bakimer, R., Fridkis-Hareli, M., Teitelbaum,D., Arnon, R., Sela, M., Kerlero de Rosbo, N., 1996. The autoim-
Ž .mune reactivity to myelin oligodendrocyte glycoprotein MOG inmultiple sclerosis is potentially pathogenic: effect of copolymer 1 onMOG induced disease. J. Neurol. 243, S14–22.
Bornstein, M.B., Miller, A., Slagle, S., Weitzman, M., Crystal, H.,Drexler, Keilson, M., Merria, M., Wassertheil-Smollerer, S., Spada,V., Arnon, R., Jackobsohn, I., Teitelbaum, D., Sela, M., 1987. A pilottrial of Cop 1 in exacerbating-remitting multiple sclerosis. N. Engl. J.Med. 317, 408–414.
Cannella, B., Raine, C.S., 1995. The adhesion molecule and cytokineprofile of multiple sclerosis. Ann. Neurol. 37, 424–435.
Cannella, B., Gao, Y.L., Brosman, C., Raine, C.S., 1996. IL-10 fails toabrogate experimental autoimmune encephalomyelitis. J. Neurosci.Res. 45, 735–746.
Cua, D.J., Hinton, D.R., Kirkman, L., Stohlman, S.A., 1995. Macrophagesregulate induction of delayed-type hypersensitivity and experimentalallergic encephalomyelitis in SJL mice. Eur. J. Immunol. 25, 2318–2324.
Fabry, Z., Topham, D.J., Fee, D., Herlein, J., Carlino, J.A., Hart, M.N.,Sriram, S., 1995. TGF-b2 decreases migration of lymphocytes invitro and homing of cells into the central nervous system in vivo. J.Immunol. 155, 325–332.
Ž .Falcone, M., Bloom, B.R., 1997. A T helper cell 2 Th2 immuneresponse against non-self antigens modifies the cytokine profile ofautoimmune T cells and protects against experimental allergic en-cephalomyelitis. J. Exp. Med. 185, 901–907.
Fridkis-Hareli, M., Teitelbaum, D., Gurevitch, E., Pecht, I., Brautbar, C.,Kwon, O.J., Brenner, T., Arnon, R., Sela, M., 1994. Direct binding ofmyelin basic protein and synthetic copolymer 1 to class II majorhistocompatibility complex molecules on living antigen presentingcells—specificity and promiscuity. Proc. Natl. Acad. Sci. USA 91,4872–4876.
Genain, C.P., Abel, K., Belmar, N., Villinger, F., Rosenberg, D.P.,Linington, C., Raine, C.S., Hauser, S.L., 1996. Late complications ofimmune deviation therapy in a nonhuman primate. Science 274,2054–2057.
Hafler, D.A., Weiner, H.L., 1995. Immunologic mechanisms and therapyin multiple sclerosis. Immunol. Rev. 144, 75–107.
Hartung, H.P., Reiners, K., Archelos, J.J., Michels, M., Seeldrayers, P.,Heidenreich, F., Pflughaupt, K.W., Toyka, K.Y., 1995. Circulating

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121120
adhesion molecules and tumor necrosis factor receptor in multiplesclerosis: correlation with magnetic resonance imaging. Ann. Neurol.38, 186–193.
Hauser, S.L., Doolittle, T.H., Lincoln, R., Brown, R.H., Dinarello, C.A.,1990. Cytokine accumulation in CSF of multiple sclerosis patients:frequent detection of interleukin-1 and tumor necrosis factor but notinterleukin-6. Neurology 40, 1735–1739.
Hofmann, F.M., Hinton, D.R., Johnson, K., Merrill, J.E., 1980. Tumornecrosis factor identified in multiple sclerosis. J. Exp. Med. 170,607–612.
IFNb multiple sclerosis study group, 1993, 1993. Interferon beta-1b iseffective in relapsing–remitting multiple sclerosis. Clinical results ofmulticenter, randomized, double-blind, placebo-controlled trial. Neu-rology 43, 655–661.
Inobe, J.I., Chen, Y., Weiner, H.L., 1996. In vivo administration of IL-4induces TGF-beta-producing cells and protects animals from experi-mental autoimmune encephalomyelitis. Ann. N.Y. Acad. Sci. 778,390–392.
Jacobs, L., Cookfair, D., Rudick, R., Hemdon, R., Richert, J., Salazar, A.,1994. Results of phase III trial of intramuscular recombinant betainterferon as treatment of multiple sclerosis. Ann. Neurol. 36, 256–262.
Johns, L.D., Flanders, K.C., Ranges, G.E., Sriram, S., 1991. Successfultreatment of experimental allergic encephalomyelitis with transform-ing growth factor-beta 1. J. Immunol. 147, 1792–1796.
Johnson, K.P., Brooks, B.R., Cohen, J.A., Ford, C.C., Goldstein, J.,Lisak, R.P., Myers, L.W., Panitch, H.S., Rose, J.W., Schiffer, R.B.,Vollmer, T., Weiner, L.P., Wolinsky, J.S., 1995. Copolymer 1 re-duces relapse rate and improves disability in relapsing–remittingmultiple sclerosis: results of a phase III multicenter, double-blindplacebo-controlled trial. Neurology 45, 1268–1276.
Karin, N., Mitchell, D.J., Brocke, S., Ling, N., Steinman, L., 1994.Reversal of experimental autoimmune encephalomyelitis by a solublepeptide variant of a myelin basic protein epitope: T cell receptorantagonism and reduction of interferon gamma and tumor necrosisfactor alpha production. J. Exp. Med. 180, 2227–2237.
Karussis, D.M., Meiner, Z., Lehmann, D., Schwarz, A., Gomori, M.,Linde, A., Abramsky, O., 1996. Immunomodulation of experimental
Ž .autoimmune encephalomyelitis EAE and CR-EAE and of multiplesclerosis with quinoline-3-carboxamide. Neurology 47, 341–346.
Kennedy, J.K., Torrance, D.S., Picka, K.S., Mahler, K.M., 1992. Analy-sis of cytokine mRNA expression in the central nervous system ofmice with experimental autoimmune encephalomyelitis reveals thatIL-10 mRNA expression correlates with recovery. J. Immunol. 149,2496–2505.
Kurtzke, J.F., 1993. Rating neurologic impairment in multiple sclerosis:Ž .an expanded disability status scale EDSS . Neurology 33, 1444–1452.
Kuruvilla, A.P., Shah, R., Hochwald, G.M., Liggitt, H.D., Palladino,M.A., Thorbecke, G.J., 1991. Protective effect of transforming growthfactor beta 1 on experimental autoimmune diseases in mice. Proc.Natl. Acad. Sci. USA 88, 2918–2921.
Lafaille, J.J., Van de Keere, F., Hsa, A.L., Baron, J.L., Haas, W., Reine,C.S., Tanagawa, S., 1997. Myelin basic protein-specific T helper 2Ž .Th2 cells cause experimental autoimmune encephalomyelitis inimmunodeficient hosts rather than protect them from the disease. J.Exp. Med. 186, 307–312.
Lehmann, P.V., Forsthuber, T., Miller, A., Sercarz, E.E., 1992. Spreadingof T-cell autoimmunity to cryptic determinants of an autoantigen.Nature 358, 155–157.
Martin, R., McFarland, H.F., McFarlin, D.E., 1992. Immunological as-pects of demyelinating diseases. Annu. Rev. Immunol. 10, 153–187.
Merrill, J.E., Storm, S.R., Ellison, G.W., Myers, L.W., 1989. In vitrostudy of mediators of inflammation in multiple sclerosis. J. Clin.Immunol. 9, 84–96.
Miller, A., Lider, O., Weiner, L.H., 1991. Antigen driven bystandersuppression after oral administration of antigens. J. Exp. Med. 174,791–798.
Milo, R., Panitch, H.S., 1995. Additive effects of copolymer 1 andinterferon Beta-1b on the immune responses to myelin basic protein.J. Neuroimmunol. 61, 185–193.
Mokhtarian, F., Shi, Y., Shirazian, D., Morgante, L., Miller, A., Grob, D.,1994. Defective production of anti-inflammatory cytokine TGF-betaby T cell lines from patients with active multiple sclerosis. J. Im-munol. 152, 6003–6010.
Mosmann, T.R., Coffman, R.L., 1987. Two types of mouse helper T cellclone: implications for immune regulation. Immunol. Today 8, 223–227.
MSrMRI study group, Paty, D.W., 1993. The IFNb multiple sclerosisstudy group Interferon beta-1b is effective in relapsing–remittingmultiple sclerosis: II. MRI analysis of multicenter, randomized, dou-ble-blind, placebo-controlled trial. Neurology 43, 662–667.
Pitzalis, C., Sharrack, B., Gray, I.A., Lee, A., Hughes, R.A., 1997.Comparison of the effects of oral versus intravenous methylpred-nisolone regimens on peripheral blood T lymphocyte adhesionmolecule expression, T cell subsets distribution and TNF alpha con-centrations in multiple sclerosis. J. Neuroimmunol. 74, 62–68.
Poser, C.M., Paty, D.W., Scheinberg, L., McDonald, W.I., Davis, F.A.,Ebers, G.C., Johnson, K.P., Sibley, W.A., Silberberg, D.H.,Tourtelotte, W.W., 1983. New diagnostic criteria for multiple sclero-sis: guidelines for research protocols. Ann. Neurol. 13, 227–231.
Pozzilli, C., Bastianello, S., Koudriavtseva, T., Gasperini, C., Bozzao, A.,Millefiorini, E., Galgani, S., Buttinelli, C., Perciaccante, G., Piazza,G., Bozzao, L., Fieschi, C., 1996. Magnetic resonance imagingchanges with recombinant human interferon-beta-1a: a short termstudy in relapsing–remitting multiple sclerosis. J. Neurol. Neurosurg.Psychiatry 61, 251–258.
Racke, M.K., Dhib-Jalbut, S., Cannella, B., Albert, P.S., Raine, C.S.,McFarlin, D.E., 1991. Prevention and treatment of chronic relapsingexperimental allergic encephalomyelitis by transforming growth fac-tor-beta 1. J. Immunol. 146, 3012–3017.
Racke, M.K., Martin, R., McFarland, H., Fritz, R.B., 1992. Copolymer1-induced inhibition of antigen-specific T-cell activation: interferencewith antigen presentation. J. Neuroimmunol. 37, 75–84.
Racke, M.K., Bonomo, A., Scott, D.E., Cannella, B., Levine, A., Raine,C.S., Shevach, E.M., Rocken, M., 1994. Cytokine-induced immunedeviation as a therapy for inflammatory autoimmune disease. J. Exp.Med. 180, 1961–1966.
Racke, M.K., Burnett, D., Pak, S.H., Albert, P.S., Cannella, B., Raine,C.S., McFarlin, D.E., Scott, D.E., 1995. Retinoid treatment of experi-mental allergic encephalomyelitis. IL-4 production correlates withimproved disease course. J. Immunol. 154, 450–458.
Rieckmann, P., Martin, S., Weichselbraun, I., Albrechet, M., Kitze, B.,Weber, T., Tumani, H., Broocks, A., Luer, W., Helwig, A., 1994.Serial analysis of circulating adhesion molecules and TNF receptor inserum from patients with multiple sclerosis: sICAM-1 is an indicatorfor relapse. Neurology 44, 2367–2372.
Rieckmann, P., Weber, F., Gunther, A., Martin, S., Bitsch, A., Broocks,A., Kitze, B., Weber, T., Borner, T., Poser, S., 1996. Pentoxifylline, aphosphodiesterase inhibitor, induces immune deviation in patientswith multiple sclerosis. J. Neuroimmunol. 64, 193–200.
Rudick, R.A., Ransohoff, R.M., 1992. Cytokine secretion by multiplesclerosis monocytes. Relationship to disease activity. Arch. Neurol.49, 265–270.
Sharief, M.K., Hentges, R., 1991. Association between tumor necrosisfactor-a and disease progression in patients with multiple sclerosis.N. Engl. J. Med. 325, 467–472.
Sharief, M.K., Noori, M.A., Ciardi, M., Cirelli, A., Thompson, E.J.,1993. Increased levels of circulating ICAM-1 in serum and cere-brospinal fluid of patients with active multiple sclerosis: correlationwith TNF-a and blood-brain barrier damage. J. Neuroimmunol. 43,15–22.
Steinman, L., Miller, A., Bernard, C.C.A., Oxsenberg, J.R., 1994. Theepigenetics of multiple sclerosis: clues to etiology and a rationale forimmune therapy. Annu. Rev. Neurosci. 17, 247–265.

( )A. Miller et al.rJournal of Neuroimmunology 92 1998 113–121 121
Steinman, L., Waisman, A., Altmann, D., 1995. Major T-Cell responsesin multiple sclerosis. Molecular Medicine Today 1, 79–83.
Street, N.E., Schumacher, J.H., Fong, T.H., Bass, H., Fiorentino, D.F.,Leverah, J.A., Mosmann, T.R., 1990. Heterogeneity of mouse helperT cells: evidence from bulk culture and limiting dilution cloning forprecursors of Th1 and Th2 cells. J. Immunol. 144, 1629–1639.
Teitelbaum, D., Milo, R., Arnon, R., Sela, M., 1992. Synthetic copolymer1 inhibits human T-cell lines specific factor myelin basic protein.Proc. Natl. Acad. Sci. USA 898, 137–141.
Teitelbaum, D., Fridkis-Hareli, M., Arnon, R., Sela, M., 1996. Copoly-mer 1 inhibits chronic relapsing experimental allergic en-
Ž .cephalomyelitis induced by proteolipid protein PLP peptides in miceand interferes with PLP-specific T cell response. J. Neuroimmunol.64, 209–217.
Teitelbaum, D., Arnon, R., Sela, M., 1997. Copolymer 1: from basicresearch to clinical application. Cell Mol. Life Sci. 53, 24–28.
Trotter, J.L., Collins, K.G., van der Veen, R.C., 1991. Serum cytokinelevels in chronic progressive multiple sclerosis: interleukin-2 levelsparallel tumor necrosis factor-alpha levels. J. Neuroimmunol 33,29–36.
van der Laan, L.J., Ruuls, S.R., Weber, K.S., Lodder, I.J., Dopp, E.A.,Dijkstra, C.D., 1996. Macrophage phagocytosis of myelin in vitrodetermined by flow cytometry: phagocytosis is mediated by CR3 andinduces production of tumor necrosis factor-alpha and nitric oxide. J.Neuroimmunol. 70, 145–152.
Van der Veen, R.C., Stohlman, S.A., 1993. Encephalitogenic Th cells1
are inhibited by Th cells with related peptide specificity, relative2
roles of IL-4 and IL-10. J. Neuroimmunol. 48, 213–217.Vandenbark, A.A., Chou, Y.K., Whitham, R., Mass, M., Buenafe, A.,
Liefeld, D., Kavanagh, D., Cooper, S., Hashim, G.A., Offner, H.,Bourdette, D.N., 1996. Treatment of multiple sclerosis with T-cellreceptor peptides: results of a double-blind pilot trial. Nat. Med. 2,1109–1115.
Voshuhl, R.R., Martin, R., Bergman, C., Dalal, M., Ruddle, N.H.,Ž .McFarland, H.F., 1993. T helper Th1 functional phenotype of
human myelin basic protein-specific T lymphocytes. Autoimmunity15, 137–143.
Waisman, A., Ruiz, P.J., Hirschberg, D.L., Gelman, A., Oksenberg, J.R.,Brocke, S., Mor, F., Cohen, I.R., Steinman, L., 1996. Suppressivevaccination with DNA encoding a variable region gene of the T-cellreceptor prevents auto-immune encephalomyelitis and activates Th2immunity. Nat. Med. 8, 899–905.
Weiner, H.L., 1997. Oral tolerance: immune mechanisms and treatmentof autoimmune diseases. Immunol. Today 18, 335–343.
Weller, R.O., Engelhardt, B., Philips, M.J., 1996. Lymphocyte targetingof the central nervous system: a review of afferent and efferentCNS-immune pathways. Brain Pathology 6, 275–288.
Windhagen, A., Nicholson, L.B., Weiner, H.L., Kuchroo, V.K., Hafler,D.A., 1996. Role of Th1 and Th2 cells in neurologic disorders. Chem.Immunol. 63, 171–186.