Treatment of LS (Stage I-III) SCLC · The Christie NHS Foundation Trust Treatment of LS (Stage...
37
The Christie NHS Foundation Trust Treatment of LS (Stage I-III) SCLC Prof C Faivre-Finn Manchester Lung Cancer Group Manchester Radiation Related Research Group ESMO-The Christie Preceptorship programme on Lung Cancer 9 th March 2018 @finn_corinne
Transcript of Treatment of LS (Stage I-III) SCLC · The Christie NHS Foundation Trust Treatment of LS (Stage...

The Christie NHS Foundation Trust
Treatment of LS(Stage I-III) SCLC
Prof C Faivre-Finn
Manchester Lung Cancer Group
Manchester Radiation Related Research Group
ESMO-The Christie Preceptorship programme on Lung Cancer
9th March 2018
@finn_corinne
The Christie NHS Foundation Trust
DISCLOSURE OF INTEREST
I have no actual or potential conflict of interest in relation
to this presentation
The Christie NHS Foundation Trust
Introduction
• Incidence of SCLC is declining-less than 10-15% of all
lung cancer cases Govindan JCO 2006
• Majority (> 95%) are associated with tobacco exposure
• One third present with stage I-III disease
• Excellent responses to CT and RT but few patients will
be long term survivors
• High risk of local relapse
• High risk of distant spread (brain)
The Christie NHS Foundation Trust
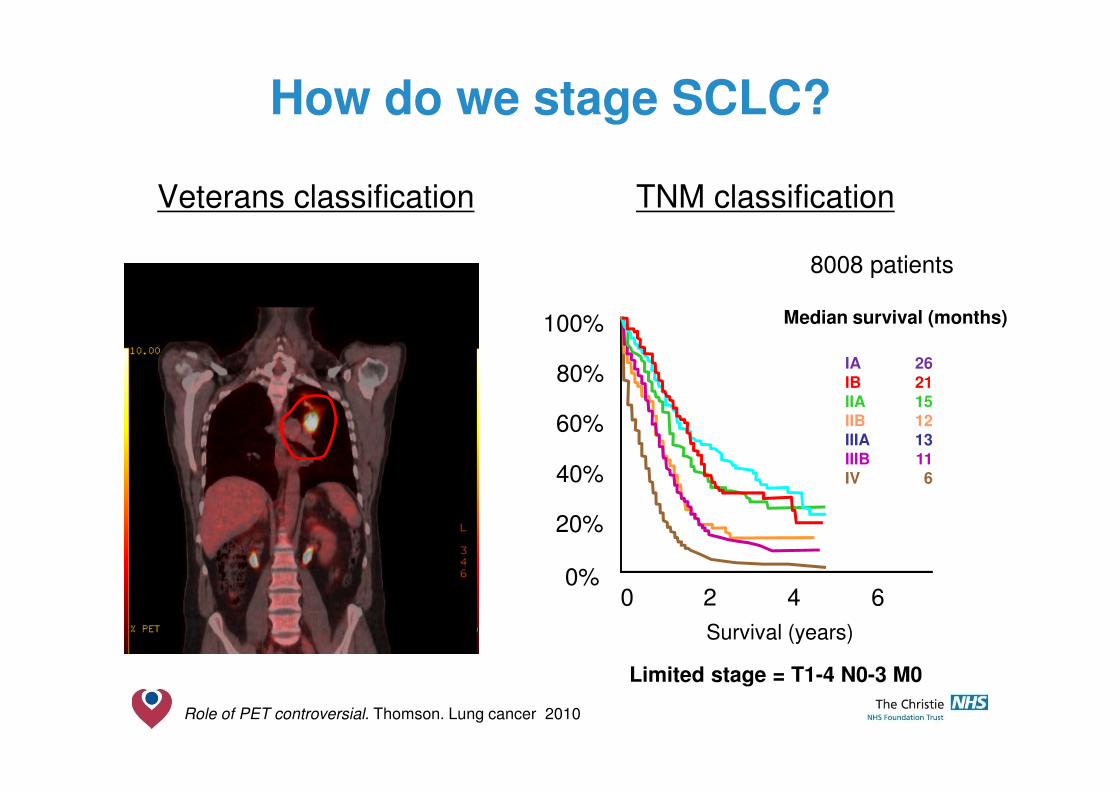
How do we stage SCLC?
Veterans classification TNM classification
0 2 4 6 8
Survival (years)
0%
20%
40%
60%
80%
100%
IAIBIIAIIBIIIAIIIBIV
2621151213116
Median survival (months)
8008 patients
Role of PET controversial. Thomson. Lung cancer 2010
Limited stage = T1-4 N0-3 M0

The Christie NHS Foundation Trust
• 76 year old male
• PMH HBP, mild COPD, ex smoker 30 PY
• PS1, MRC RS 1
• Presented with a cough and SOB on exertion
• FEV1 55% predicted, KCO 46% predicted
• Bronchoscopy-tumour obstructing the L main bronchus
• CT thorax&abdomenMass LUL
Station 4R, 4L, 5 and 7 lymph nodes
• CT brain clear
Stage I-III SCLC - Clinical case
Treatment options
• Sequential CTRT
• Concurrent CTRT
• Dose fractionation
– 40 Gy/15F
– 50-55 Gy/20F
– >60 Gy/30+F
• 3DRT or IMRT?
• PCI?

The Christie NHS Foundation Trust
• Cisplatin is the best radiosensitiser and has higher RR�Cisplatin plays a major role in the treatment of LS-SCLC
• Cisplatin-Etoposide can be delivered at full dose with thoracic RT with an acceptable toxicity profile
• No change in systemic therapy in last 20 years
� No role for anthracyclines/pemetrexed/irinotecan
� No role for chemotherapy dose intensification
� No role for targeted agents
Systemic treatment in stage I-III SCLC
The Christie NHS Foundation Trust
RadiotherapyCurrent evidence in stage I-III SCLC
• CTRT >CT (Pignon, Warde)
• Early RT >late RT (Fried , Cochrane review)
• Concurrent CTRT >sequential CTRT (Takada)
• Best survival results achieved with early BD concurrent CTRT(Turrisi, Jeremic, Faivre-Finn)
• PCI improves survival - 6% @ 3 years (Auperin)

The Christie NHS Foundation Trust
Role of thoracic radiotherapyMeta-analyses
• Pignon et al. N Engl J Med 1992
� 13 randomised trials
� 2140 patients
� 3 year survival
� 8.9 % CT alone
� 14.3% CT+RT
� Thoracic RT benefited more younger patients
RR of death in the CTRT as compared with CT group
� 0.72 for patients <55 years old (0.56-0.93)
� 1.07 (0.70-1.64) for patients over 70
• Warde et al. JCO 1992
• Limitations of the metaanalyses• Response to treatment assessed on CXR
• Dated RT techniques (2D)
14% reduction in risk of death, p = 0.001

The Christie NHS Foundation Trust
Timing of thoracic RT with chemotherapy
7 RCTsAdvantage of early (<9 weeks) radiotherapy
2 yr % NNT for benefit p
All (1524)
Platinum
Platinum+HART
+5.2 [0.6-9.7] 20 0.03
+9.8 [3.8-15.9] 10 0.001
+16.7 [9.4-26] 6 0.001
Fried et al. J Clin Oncol 2004
The Christie NHS Foundation Trust
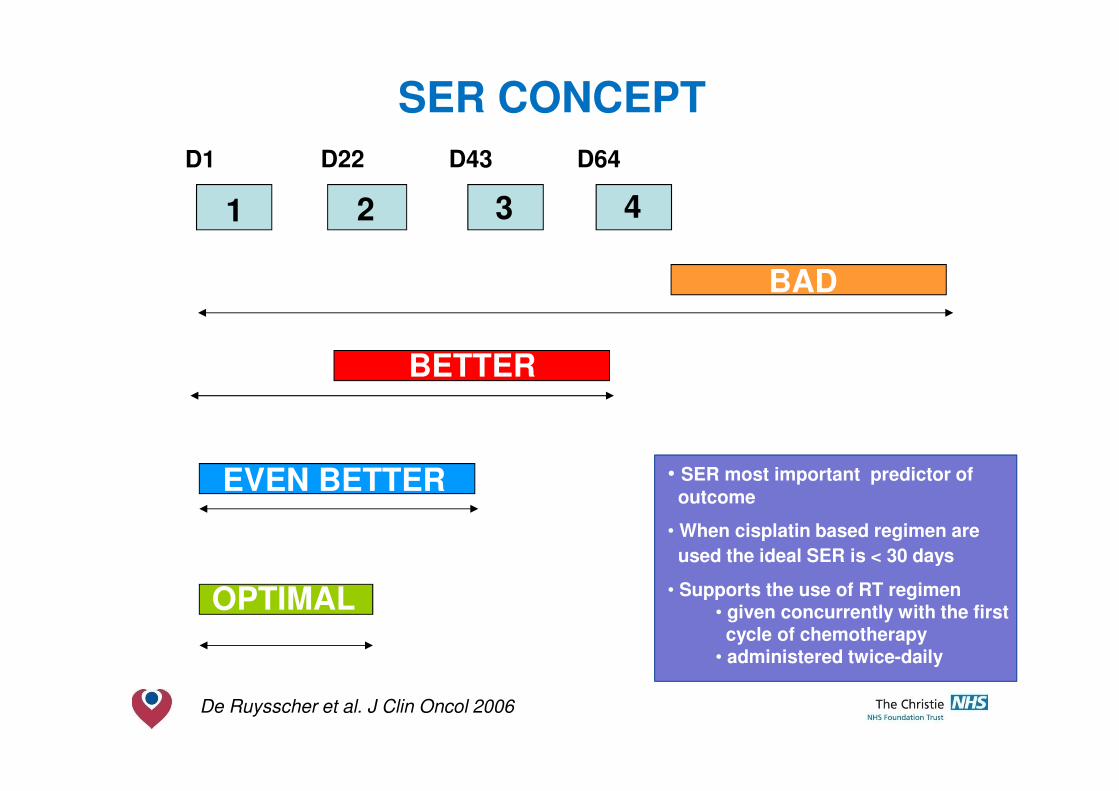
SER CONCEPT
EVEN BETTER
D1 D22 D43 D64
De Ruysscher et al. J Clin Oncol 2006
• SER most important predictor of
outcome
• When cisplatin based regimen are
used the ideal SER is < 30 days
• Supports the use of RT regimen • given concurrently with the first cycle of chemotherapy
• administered twice-daily
1 2 3 4
BAD
BETTER
OPTIMAL
EVEN BETTER

The Christie NHS Foundation Trust
Japan Clinical Oncology GroupConcurrent vs. sequential CTRT
n=231
Concurrent
4 weekly PE
Sequential
3 weekly PE
RT (45 Gy BD) Day 2 Post cycle 4
CR (%) 40 27
MST (months) 27 19
5 yr survival (%) 24 18
Takada et al. J Clin Oncol 2002
(p =0. 097)
The Christie NHS Foundation Trust
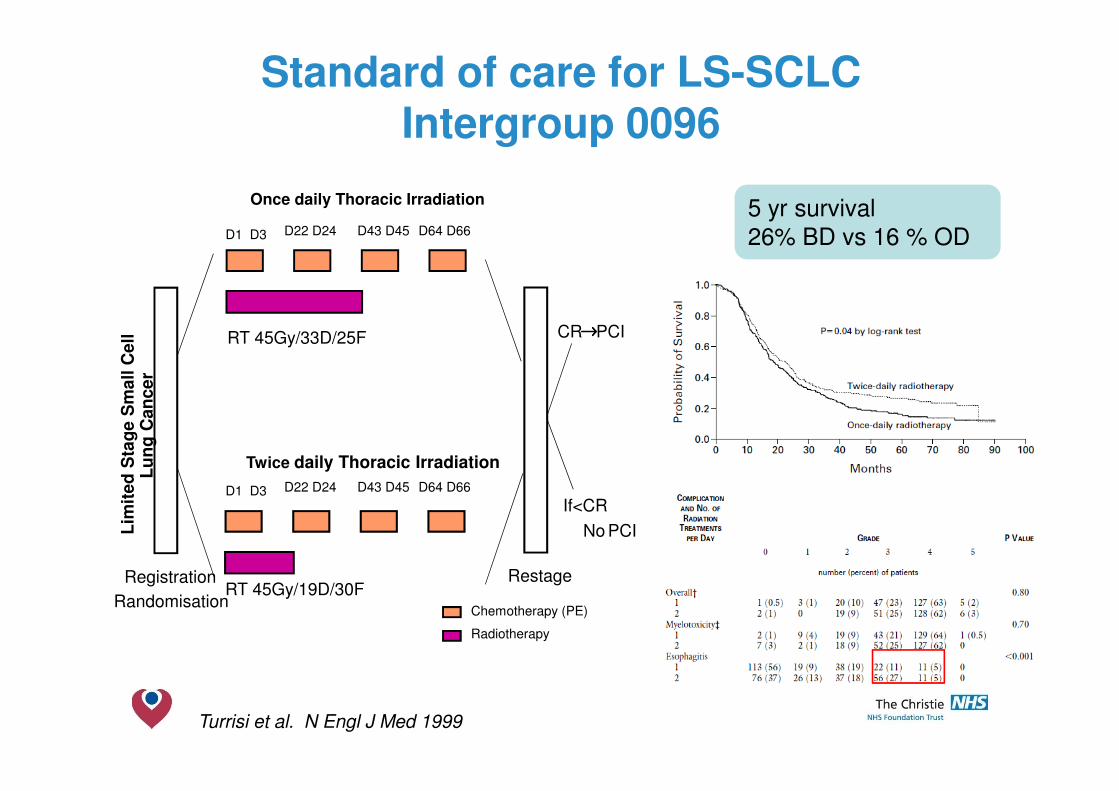
Standard of care for LS-SCLCIntergroup 0096
Turrisi et al. N Engl J Med 1999
Once daily Thoracic Irradiation
D1 D3
RT 45Gy/33D/25F
Twice daily Thoracic Irradiation
RT 45Gy/19D/30F
Lim
ited
Sta
ge S
mall C
ell
Lu
ng
Can
cer
CR→→→→PCI
If<CR
→→→→ No PCI
Registration
Randomisation
Restage
Chemotherapy (PE)
Radiotherapy
D22 D24 D43 D45 D64 D66
D1 D3 D22 D24 D43 D45 D64 D66
5 yr survival
26% BD vs 16 % OD

The Christie NHS Foundation Trust
Utilization of Hyperfractionated Radiation in SCLC and Its Impact on Survival
• National Cancer Database.1999-2012
• 25,045 patients diagnosed with non-
metastatic SCLC (22,626 had survival
data)
• The utilization of BD radiation overall was 11.3%
• Treatment at an academic centre was
associated with a higher likelihood of
receiving BD treatment (OR: 2.29, p <
0.001).
• Median survival was 22.1, 17.2, 18.3,
19.2, and 19.5 months for patients
receiving 45 Gy BD, 45 Gy OD , 46-
59.4 Gy OD, 60-61.2 Gy OD , and 62 -
72 Gy OD (p < 0.001 for pairwise
comparison to BD)
Schreiber. JTO 2015

The Christie NHS Foundation Trust
CTRT in the elderly
Subset analysis of Intergroup 0096
381 patients treated with BD vs OD CTRT
PS 0-1
age 30-82
31% ≥ 65 and 13% ≥ 70 years
Study not stratified per age groups
• Compliance to 4 cycles: 78% vs 90% for younger patients
• Toxicity (>70 vs. younger patients)• More severe hematologic toxicity (grade 4–5: 61% vs. 84%; p <0.01)
• More fatal toxicities (1% vs. 10%; p<0.01)
• No differences in non-hematologic toxicities
• Outcome according to age • No difference in event free survival rate, time to local failure, and duration of response
• Overall survival rates favored those younger than 70 years
(5 year 22% vs. 16%; p = 0.05)
Yuen et al. Cancer 2000
Once daily Thoracic Irradiation
D1 D3 D22 D24 D43 D45 D64 D66
RT 45Gy/33D/25F
Twice daily Thoracic Irradiation
D1 D3 D22 D24 D43 D45 D64 D66
RT 45Gy/19D/30F
Lim
ited
Sta
ge S
mall C
ell
Lu
ng
Can
cer
CR→→→→PCI
If<CR
→→→→NoPCI
RegistrationRandomisation
Restage
Chemotherapy (PE)
Radiotherapy
The Christie NHS Foundation Trust
How can we improve survival rates further with radiotherapy?
The Christie NHS Foundation Trust
Considerations for radiotherapy techniques
Modern techniques• 3D CRT/IMRT
• 4DCT and PETCT for RT planning
• IGRT
Better local control = Improved survival
Impact of advanced RT on outcome?

The Christie NHS Foundation Trust
Intensity modulated radiotherapy
V20 33.1%MLD 19.4GyMax SC 47.9 Gy
V20 35%MLD 20.1 GyMax SC 35.3 Gy
IMRT modulates the intensity profile of the radiation delivered to the
patient allowing improved targeting of the radiation dose

The Christie NHS Foundation Trust
3DCRT vs IMRT for stage I-III SCLC
• 223 patients treated at the MD Anderson between 2000-09 were retrospectively reviewed
• 119 receiving 3DCRT and 104 receiving IMRT
• Median age was 64 years (range 39-90 years)
• Radiation modality was not associated with differences in OS or DFS in either multivariable or propensity score-matched analyses
Shirvani. Int J Rad Oncol Biol Phys 2013

The Christie NHS Foundation Trust
CONVERT multinational, phase III randomised study
RT 45Gy/30F/19D
Lim
ited
Sta
ge S
mall C
ell
SD,PR,CR→→→→PCI
If<SD→→→→ no PCI
Registration
Randomisation
RestageChemotherapy
Radiotherapy
D1 D3 D22 D24 D43 D45 D64 D66
Twice-daily (BD) thoracic RT
D1 D3 D22 D24 D43 D45 D64 D66
RT 66Gy/33F/45D
Once-daily (OD) thoracic RT
Stratification factorsCentreNo. of cycles chemo: 4 vs.6 PS: 0,1 vs. 2
RTP after randomisationRT started on D22 cycle 13DCRT or IMRTNo ENIQA programme
Chemotherapy4 to 6 cycles Cisplatin 25mg/m2 D1-3 or75mg/m2 D1Etoposide 100mg/m2 D1-3
547 patients
8 countries
75 centres
PS 0-2
No age limit

The Christie NHS Foundation Trust
Overall survival
Median follow-up: 45 months
Overall survival(n=543)
BD OD Log-rank
Median(months)
30 (24-34) 25 (21-31)
p=0.14
1-year 83% (78-87) 76% (71-81)
2-year 56% (50-62) 51% (45-57)
3-year 43% (37-49) 39% (33-45)
5-year 34% (27-41) 31% (25-37)
Primary objective-overall survival Trial hypothesis
Expected survival BD arm 44%Projected survival OD arm 56%
(5) (1) (17) (30) (22) (13) (3)(3) (1) (27) (29) (25) (19) (3)
HR=1.18 with 95% CI 0.95-1.45 p=0.14
0
20
40
60
80
100
Aliv
e (
%)
273 224 151 92 54 25 6 2BD270 202 134 88 46 21 7 3OD
Number at risk
0 1 2 3 4 5 6 7Years from randomisation
OD
BD
Overall survival
Faivre-Finn. Lancet Oncol 2017

The Christie NHS Foundation Trust
Acute Toxicity
•1 patient in each arm not assessable for oesophagitis, 6 patients for pneumonitis
•*1 patient in BD arm and 2 patients in OD arm (1 received sequential CTRT) died
from radiation pneumonitis
Organ at risk Arm N Median (Range)
Lung V5 (%) BDOD
246234
56.2 (7.2-88.5)60.8 (7.0-91.6)
Lung V20 (%) BDOD
252240
23.2 (0.1-35.4)28.8 (8.0-40.5)
Heart (% total dose)
BDOD
240229
2.0 (0-45.3)1.4 (0-36.2)
Spinal cord (max dose, Gy)
BDOD
251241
32.0 (1.3-45.8)41.7 (1.3-52.6)
Oesophagus (max dose, Gy)
BDOD
248236
45.7 (0.7-64.4)65.9 (2.2-71.7)
Oesophagus V35 (%)
BDOD
246230
34.0 (0-76.5)38.8 (0-82.8)
ARM BD (n=254) OD (n=256) p
AE (grade) 1-2
n (%)
3
n (%)
4
n (%)
5
n (%)
1-2
n (%)
3
n (%)
4
n (%)
5
n (%)
Oesophagitis 159
(62·6)
46
(18·1)
1
(0·4)
- 135
(52·7)
47
(18·4)
- - 0·85
Pneumonitis 51
(20·1)
3
(1·2)
1
(0·4)
1
(0·4)*
49
(19·1)
3
(1·2)
1
(0·4)
2
(0·8)*
0·70
Faivre-Finn. Lancet Oncol 2017
The Christie NHS Foundation Trust
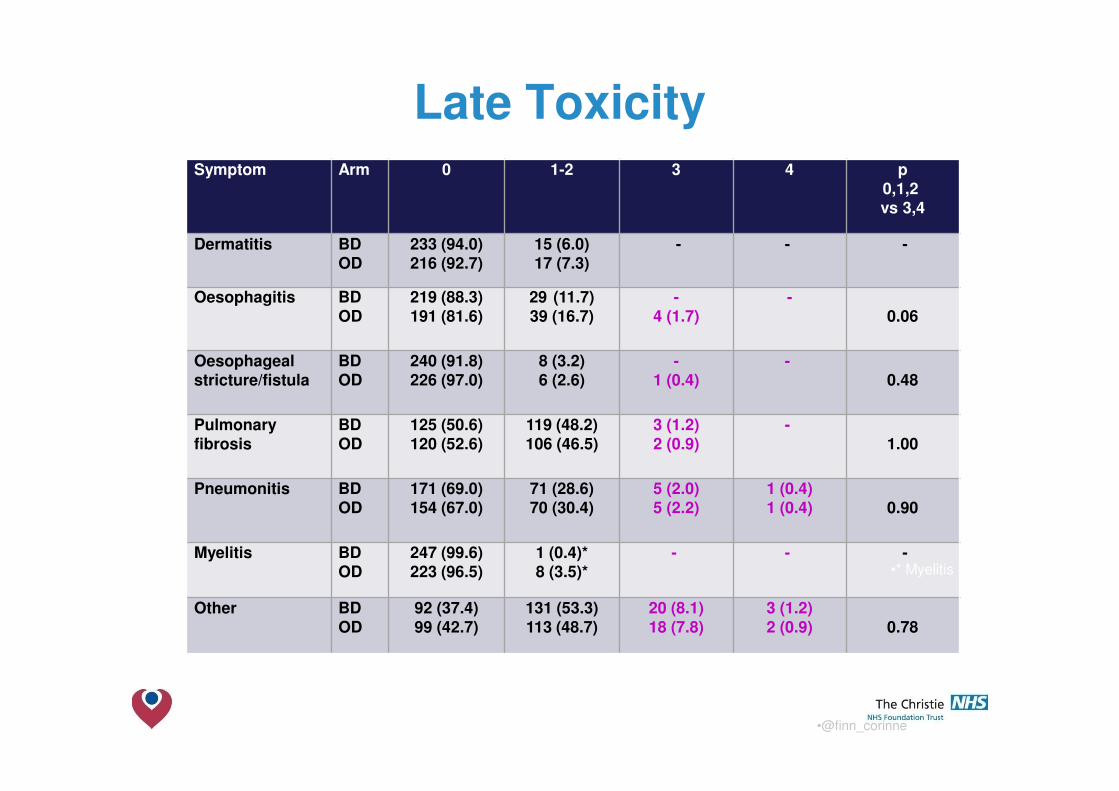
Symptom Arm 0 1-2 3 4 p0,1,2vs 3,4
Dermatitis BDOD
233 (94.0)216 (92.7)
15 (6.0)17 (7.3)
- - -
Oesophagitis BDOD
219 (88.3)191 (81.6)
29 (11.7)39 (16.7)
-4 (1.7)
-0.06
Oesophagealstricture/fistula
BDOD
240 (91.8)226 (97.0)
8 (3.2)6 (2.6)
-1 (0.4)
-0.48
Pulmonaryfibrosis
BDOD
125 (50.6)120 (52.6)
119 (48.2)106 (46.5)
3 (1.2)2 (0.9)
-1.00
Pneumonitis BDOD
171 (69.0)154 (67.0)
71 (28.6)70 (30.4)
5 (2.0)5 (2.2)
1 (0.4)1 (0.4) 0.90
Myelitis BDOD
247 (99.6)223 (96.5)
1 (0.4)*8 (3.5)*
- - -
Other BDOD
92 (37.4)99 (42.7)
131 (53.3)113 (48.7)
20 (8.1)18 (7.8)
3 (1.2)2 (0.9) 0.78
•* Myelitis all grade 1
•@finn_corinne
Late Toxicity

The Christie NHS Foundation Trust
CONVERT- CTC - Multivariate AnalysisAt-Risk Group PFS OS
Models Positive Negative P HR 95% CI P HR 95% CI
With 2-CTCs threshold
2 CTCs at baseline ≥ 2 < 2 0.021 1.85 1.10 to 3.12 0.006 2.15 1.25 to 3.70
ECOG PS 1 0 0.011 2.20 1.19 to 4.07 0.009 2.39 1.25 to 4.60
2 0 0.184 2.15 0.70 to 6.63 0.148 2.32 0.74 to 7.29
With 15-CTCs threshold
15 CTCs at baseline
≥ 15 < 15 <.001 6.03 3.00 to 12.08 <.001 6.19 3.08 to 12.42
ECOG PS 1 0 0.157 1.60 0.84 to 3.05 0.168 1.63 0.81 to 3.25
2 0 0.439 1.58 0.50 to 5.03 0.223 2.05 0.64 to 6.56
With 50-CTCs threshold
50 CTCs at baseline
≥ 50 < 50 0.002 3.59 1.58 to 8.18 0.003 3.42 1.52 to 7.67
ECOG PS 1 0 0.034 1.96 1.05 to 3.65 0.034 2.05 1.05 to 3.97
2 0 0.298 1.85 0.58 to 5.89 0.148 2.35 0.74 to 7.47
• CTC count is highly prognostic for survival
• Independent from other clinical factors (eg PET staging)
•15 CTCs predicted ≤ 2 years survival in 100% and ≤ 1
year survival in 70% of the patients
• Provides a hypothesis to stratify patients prospectively for
CTC count in future clinical trials
Fernandez-Guiterrez. World Lung 2016
The Christie NHS Foundation Trust
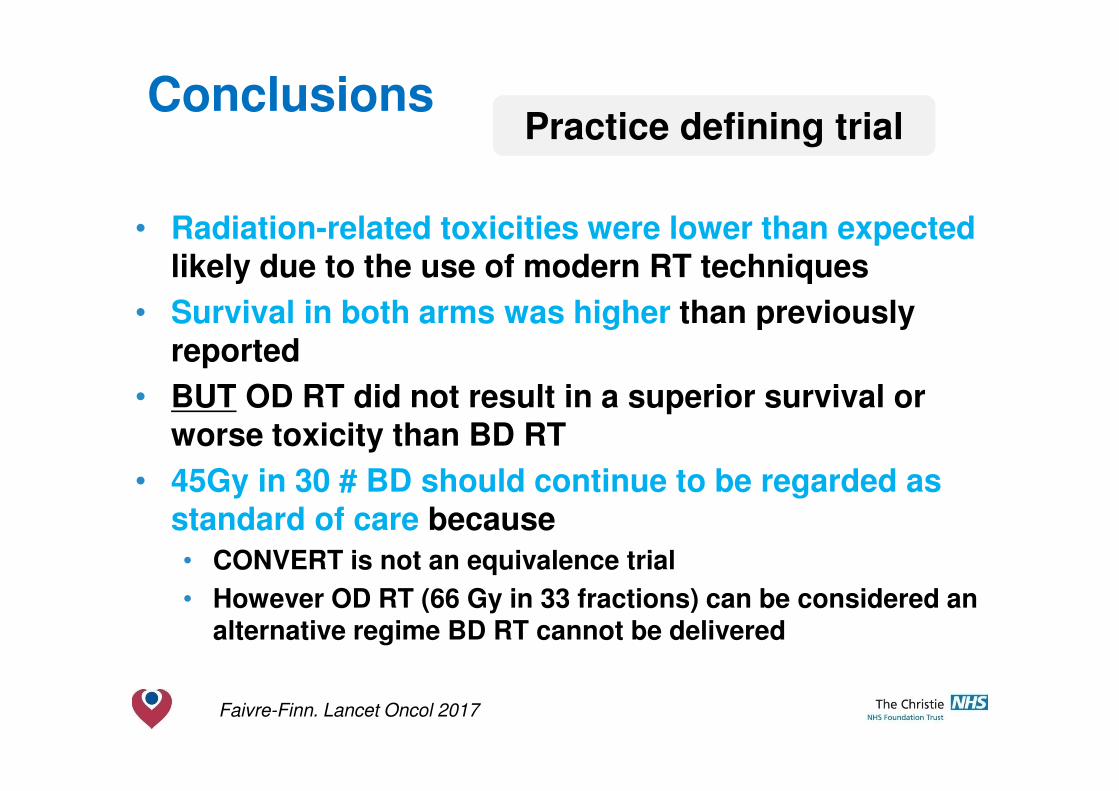
Conclusions
• Radiation-related toxicities were lower than expected likely due to the use of modern RT techniques
• Survival in both arms was higher than previously reported
• BUT OD RT did not result in a superior survival or worse toxicity than BD RT
• 45Gy in 30 # BD should continue to be regarded as standard of care because
• CONVERT is not an equivalence trial
• However OD RT (66 Gy in 33 fractions) can be considered an alternative regime BD RT cannot be delivered
Faivre-Finn. Lancet Oncol 2017
Practice defining trial

The Christie NHS Foundation Trust
Intergroup studyCALGB 30610-RTOG 0538
Limited
SCLC
45 Gy BID/
3 weeks
61.2 Gy CB/
5 weeks
70 Gy QD/
7 weeks
45 Gy BID/
3 weeks
Experimental TRT arm
PS 0-1
PE X 4 → PCI
Cycle 1 or 2 TRT
Re-assess
VS.
Primary endpoints = OS

The Christie NHS Foundation Trust
Can we improve survival rates further with systemic treatment?
The Christie NHS Foundation Trust
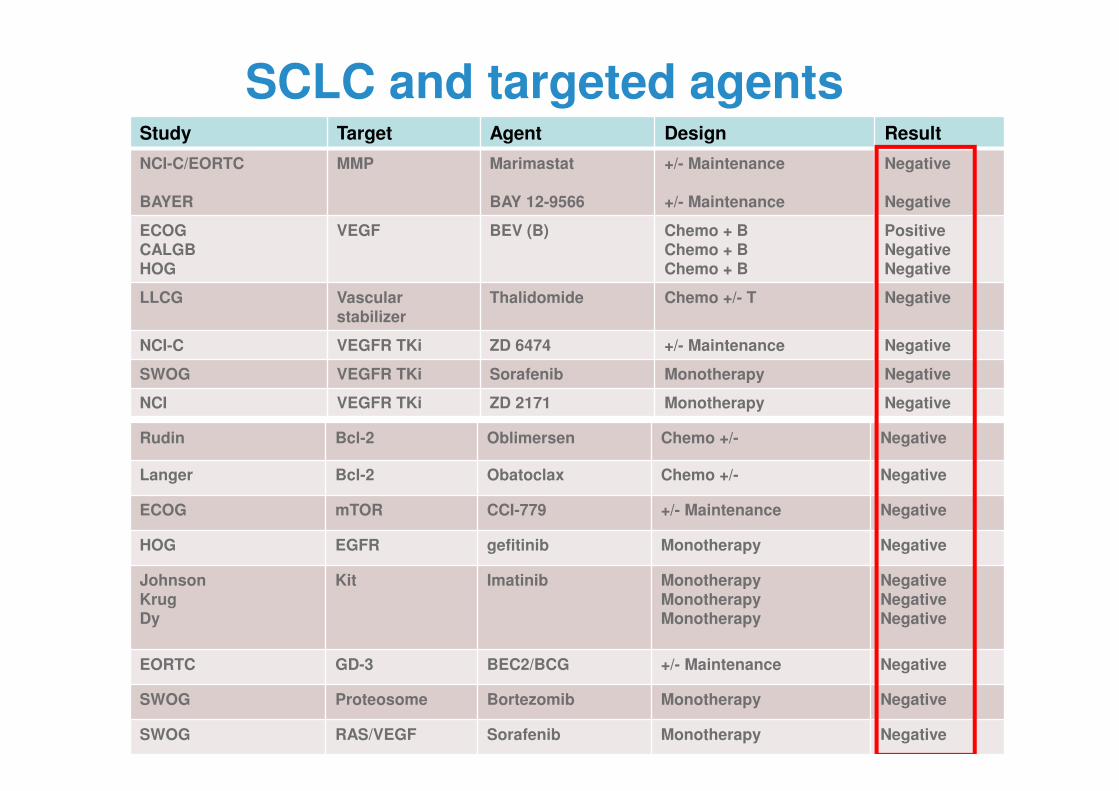
SCLC and targeted agentsStudy Target Agent Design Result
NCI-C/EORTC
BAYER
MMP Marimastat
BAY 12-9566
+/- Maintenance
+/- Maintenance
Negative
Negative
ECOGCALGBHOG
VEGF BEV (B) Chemo + BChemo + BChemo + B
PositiveNegativeNegative
LLCG Vascular stabilizer
Thalidomide Chemo +/- T Negative
NCI-C VEGFR TKi ZD 6474 +/- Maintenance Negative
SWOG VEGFR TKi Sorafenib Monotherapy Negative
NCI VEGFR TKi ZD 2171 Monotherapy Negative
Rudin Bcl-2 Oblimersen Chemo +/- Negative
Langer Bcl-2 Obatoclax Chemo +/- Negative
ECOG mTOR CCI-779 +/- Maintenance Negative
HOG EGFR gefitinib Monotherapy Negative
JohnsonKrugDy
Kit Imatinib MonotherapyMonotherapyMonotherapy
NegativeNegativeNegative
EORTC GD-3 BEC2/BCG +/- Maintenance Negative
SWOG Proteosome Bortezomib Monotherapy Negative
SWOG RAS/VEGF Sorafenib Monotherapy Negative

The Christie NHS Foundation Trust
Targeted agents and RT
Spigel et al. J Clin Oncol 2010
Phase II -29 LS-SCLC patients recruited
Early trial closure
Two patients developed tracheoesophageal fistulae
One patient died from an aerodigestive hemorrhage

The Christie NHS Foundation Trust
Chemo-Radiotherapy:
cis-/carboplatin + etoposide
4 cycles
Biomaterial for translationalresearch:
Consolidation vs observation:
induction maintenance
max 1 year
combination nivolumab
nivolumab/ipilimumab
observation
Screening:
LD SCLCPCI
Tumour
evaluation:
PD
off
Voluntaryre-biopsy:
? FFPE block
yes
noR
•••• •••• ••••
3 6 9 3 6 9 1812
after randomisation
RT (Thoracic Radiotherapy): CT scans for tumourassessment
accelerated schedule preferred - up to 18 months: every 9 weeks
start: day 1 of chemo cycle 1 or - up to 2 years: every 12 weeks
day 1 of chemo cycle 2 - years 3 & 4: every 6 months
- at 5 years
0Week
Serum
At progression:
Whole blood Whole bloodWhole blood
RT
RT
from startof chemotherapy
-2
CT
Serum SerumSerum
FDG-PET-CT
or CT
Brain MRI
or CT
Biopsy:
FFPE block
or slides
27
CT •••• •••• ••••
14 16
STIMULI

The Christie NHS Foundation Trust
Progress in stage I-III SCLC
SWO
G 9
713
SWO
G 0
222
NC
CTG
892
052
CA
LGB
923
5R
TOG
960
9EC
OG
259
6IN
T0096
QD
INT00
96B
ID
CO
NVER
T QD
CO
NVER
T BID
0
10
20
30
40
Me
dia
n S
urv
iva
l (m
on
ths
)
CT alone
Seq CTRT
ConCTRT
BD CTRT
CONVERT BD
5 year survival (%)
<10
10-15
20-25
25
34
The Christie NHS Foundation Trust
Surgery for very limited SCLC?
The Christie NHS Foundation Trust
Facts
• Stage I SCLC is diagnosed in ~5% of patients
• Paucity of prospective evidence in very early stage SCLC
• Staging, surgery and RT techniques have evolved dramatically in last decade

The Christie NHS Foundation Trust
Surgery vs RT
MRC trial. 144 patients with ‘no evidence of metastatic disease, operable and fit enough for resection’
Surgery . ‘Patients allocated to surgery were to undergo thoracotomy with the
intention of performing a total resection of all growth’
Radical radiotherapy. ‘Patients allocated to radical RT were to be treated by the
technique customarily used by the radiotherapists’ (11% pall RT, 4% no RT)
R
Fox et al. Lancet 1973 No chemotherapy, no details on TNM

The Christie NHS Foundation Trust
Surgery vs RT
Lad et al. Chest 1994
50 Gy/25#
Actuarial 2 year survival 20%
ECOG-EORTC 328 pts registered, 146 pts randomised, 13 pts stage I

The Christie NHS Foundation Trust
NCI recommendationsRole of surgery
• The role of surgery in the management of patients with SCLC is unproven
• Evidence:
� Small case series and population studies have reported favourable outcomes for the minority of LD patients with very limited disease (level of evidence 3)
� A randomized study evaluating the role of surgery in addition to CTRT found no OS benefit with the addition of pulmonary resection [Lad et al] (level of evidence 1)
• Given the absence of data from randomized trials, the role of surgery in the management of individual patients with SCLC must be considered, both in terms of potential benefit and riskfrom the surgical procedure
http://www.cancer.gov/cancertopics/pdq/treatment/small-cell-lung

The Christie NHS Foundation Trust
Early
Locally-advanced
p=0.001
EarlyLocally-
advanced
Log
rank
Median 50 months95%CI 35,-
25 months95% CI 21, 29
p=0.0011-year 83% 79%
2-year 64% 50%
513 patients eligible for this sub-group analysis and 87 (17%) had early disease:
• 4 patients (4.6%) ���� TNM stage I
• 83 patient (95.4%) ���� TNM stage II
Toxicity
(number evaluated early/ locally-advanced)
Grade Early Locally-advanced
Chi-sq
(p-value)
Oesophagitis
(82/ 393)
0
1-2
≥3
32 (39%)
41 (50%)
9 (11%)
72 (18.3%)
237 (60.3%)
84 (21.4%)<0.005
Pneumonitis
(82/ 389)
0
1-2
≥3
59 (72%)
21 (25.6%)
2 (2.4%)
307 (78.9%)
74 (19%)
8 (2.1%) 0.52
CONVERT EARLY STAGE

The Christie NHS Foundation Trust
SUMMARY
• For clinical guidelines : ESMO Ann Oncol 2010, 2013
NCCN Thorax 2016
NCI recommendations
• Cisplatin etoposide is still standard in combination with RT
• Progress has been made with RT!! We should all CONVERT to BDRT
• Role of surgery for stage I-II SCLC not well defined
• We need to increase our understanding of the biology and individualise treatment