Treatment of Intracranial Tumors by Systemic Transfer of ...Murine models have established that an...
8
[CANCER RESEARCH56. 4702-4708. October 15. 19961 phocytes have been identified in cancer-bearing patients, including peripheral blood (1—4),lymphoid tissue (5—7),and TILs3 (3, 8—10). Murine models have established that an abundant source of tumor sensitized T lymphocytes is present in LN-draining s.c. tumors (11, 12). T cells from tumor-bearing mice are largely incapable of mcdi ating tumor regression when immediately transferred into secondary tumor-bearing hosts (11, 12). However, these cells, when properly activated ex vivo, undergo a functional change such that they mediate regression of established tumors on adoptive transfer (12). Several ex vivo activation methods have been developed for tumor sensitized LN cells involving the use of tumor cells as well as T-cell-activating reagents. Tumor-reactive cells can be generated us ing mAbs directed against the € chain of the TCRCD3 complex (12, 13). This antigen-independent stimulation permits the activation of tumor-reactivecells in cases in which sufficienttumorsare unavail able or in which the relevant tumor antigens are not characterized. Recently, we have characterized the antitumor reactivity of superan tigen-activated tumor-draining LN cells (14). Bacterial superantigens are strong mitogens for T lymphocytes bearing certain TCR V@ regions (15). Treatment of tumor-draining LN cells with SEA or SEB led to the selective activation and expansion of certain TCR V/3 subsets. The adoptive transfer of SEB-activated LN cells resulted in the immunologically specific regression of established pulmonary metastases (14). To determine whether LN cells stimulated with SEs could effectively treat tumors in an immunologically privileged site, we used a model of experimentally induced IC tumor. The CNS has long been considered an immunologically privileged site. Several factors may contribute to this status, including an endo thelial structure that restricts passage of macromolecules, viruses, and cells; the absence of lymphatic drainage; and inadequate expression of MHC molecules (16, 17). Results from immunotherapy trials for malignant melanoma by either active immunization or adoptive trans fer of T cells suggest that the CNS may be relatively inaccessible to tumor-reactive cells, because some patients developed disease pro gression in the brain despite tumor regression at other sites (18). For this reason, patients with CNS metastases are usually excluded from immunotherapy trials. Attempts have been made to explore the po tential of adoptive immunotherapy for primary CNS malignancies, because a more favorable prognosis can be predicted by increased tumoral lymphocyte infiltration (19, 20). However, results from nu merous clinical trials of adoptive immunotherapy for brain tumors have thus far been disappointing (21, 22). Despite previous difficulties in generating an adequate immune response in the CNS, there are reasons to believe that T lymphocytes, under appropriate conditions, can penetrate the blood-brain barrier and mediate therapeutic effects. In experimental models, active im munization of animals with allogeneic cells or syngeneic melanoma cells resulted in the immunologically specific rejection of challenges in the brain with the allogeneic or tumor cells (23—25).Moreover, T-cell-mediated autoimmune responses exist in naturally occurring diseases such as multiple sclerosis and in experimental allergic en 3 The abbreviations used are: TIL, tumor-infiltrating lymphocyte; LN, lymph node; mAb, monoclonal antibody; TCR, T-cell receptor; SE, staphylococcal enterotoxin; CNS, central nervous system; IC, intracranial; ExF1', exfoliating toxin; CM, complete medium; IL-2, interleukin 2; WBI, whole-body irradiation; SAg, superantigen. ABSTRACT Adoptive transfer of tumor-sensitized T lymphocytes has demonstrated therapeutic efficacy in animal tumor models and in some patients with melanoma and renal cell cancers. In experimental settings, T lymphocytes derived from lymph nodes (LNs) draining progressively growing tumors can be activated cx vivo to generate tumor-reactive lymphocytes with therapeutic efficacy. Despite the theoretical concern regarding inaccessi bifity ofthe central nervous system to systemically transferred T cells, our recent experiments demonstrated that anti-CD3-activated tumor-draining LN cells are capable of mediating the regression of established intracere bral tumors. In this study, several staphylococcal enterotoxins (SEs), including SEA, SEC2, and SEE, and exfoliating toxin, known to be superantigens, were tested for their abffity to stimulate tumor-draining LN cells to acquire antitumor reactivity for the treatment of intracerebral tumors. SEa bind to the MHC class H molecule and provide an activating signal to T cells bearing particular T-cell receptor Vfi chains. Tumor draining LN celia activated with SEa demonstrated selective V@3T-cell expansion. In adoptive immunotherapy of intracranial (IC) tumors, SEA and SEC2-activated cells had the highest efficacy, whereas SEE-activated cells were not therapeutic. Despite the antigen independence of SE acti vation, the T cells retained immunological specificity for the tumor, which provided the initial in vivo sensitization of the LN. During the ex vivo stimulation with superantigens, both CD4@ and CD8@ T cells proliferated, and both subsets were required to mediate regression of IC tumors. In contrast to the adoptive immunotherapy of visceral tumors, the systemic administration of exogenous interleukin 2 failed to support the antitumor reactivity In mice depleted of CD4 cells, and, in fact, it inhibited the therapeutic efficacy. Furthermore, mice cured of intracerebral tumors by the adoptive transfer of T cells were resistant to an IC tumor rechallenge. However, in contrast to the immunological specificity demonstrated dur ing the primary adoptive transfer, cured mice were able to reject clad lenge with several immunologically distinct fibrosarcomas but not a mel anoma. These results indicate that superantigen-activated LN cells can circulate to and interact with intracerebral tumors mediating tumor regression in an immunologically specific manner. Although conditions that optimize the treatment of intracerebral tumors appear to be different from those for visceral tumors, analysis of T-cell receptor Vj3 expression among cells activated with several superantigens does not reflect a pref erential usage of Vfi gene segments in the immune response to autochth onous tumors. INTRODUCTION It is clearly evident that during progressive tumor growth, the host contains T lymphocytes sensitized to tumor antigens, but other im munological and physiological factors may have prevented an effec tive antitumor response from eradicating the existing tumor. However, under certain conditions, the intentional infusion of tumor-reactive T lymphocytes may result in the regression of tumors. The use of T lymphocytes for the treatment of cancers has been referred to as â€oeadoptive immunotherapy.― Several sources of tumor-sensitized lym Received 12/19/95; accepted 8/16/96. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. I This work was supported by NIH Grants ROl CA58927 and R37 CA67324 (S. S.) and K08 CA01580 (G. E. P.). 2 To whom requests for reprints should be addressed, at FF5, Center for Surgery Research, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195. 4702 Treatment of Intracranial Tumors by Systemic Transfer of Superantigen-activated Tumor-draining Lymph Node T Cells' Mamoru Lnoue, Gregory E. Plautz, and Suyu Shu2 Centerfor Surgery Research. The Cleveland Clinic Foundation. Cleveland, Ohio 44195 on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Treatment of Intracranial Tumors by Systemic Transfer of ...Murine models have established that an...

[CANCER RESEARCH56. 4702-4708. October 15. 19961
phocytes have been identified in cancer-bearing patients, includingperipheral blood (1—4),lymphoid tissue (5—7),and TILs3 (3, 8—10).Murine models have established that an abundant source of tumor
sensitized T lymphocytes is present in LN-draining s.c. tumors (11,12). T cells from tumor-bearing mice are largely incapable of mcdiating tumor regression when immediately transferred into secondarytumor-bearing hosts (11, 12). However, these cells, when properlyactivated ex vivo, undergo a functional change such that they mediateregression of established tumors on adoptive transfer (12).
Several ex vivo activation methods have been developed for tumorsensitized LN cells involving the use of tumor cells as well asT-cell-activating reagents. Tumor-reactive cells can be generated using mAbs directed against the €chain of the TCRCD3 complex (12,13). This antigen-independent stimulation permits the activation oftumor-reactivecells in cases in which sufficienttumorsare unavailable or in which the relevant tumor antigens are not characterized.Recently, we have characterized the antitumor reactivity of superantigen-activated tumor-draining LN cells (14). Bacterial superantigensare strong mitogens for T lymphocytes bearing certain TCR V@regions (15). Treatment of tumor-draining LN cells with SEA or SEBled to the selective activation and expansion of certain TCR V/3subsets. The adoptive transfer of SEB-activated LN cells resulted inthe immunologically specific regression of established pulmonarymetastases (14). To determine whether LN cells stimulated with SEscould effectively treat tumors in an immunologically privileged site,we used a model of experimentally induced IC tumor.
The CNS has long been considered an immunologically privilegedsite. Several factors may contribute to this status, including an endothelial structure that restricts passage of macromolecules, viruses, andcells; the absence of lymphatic drainage; and inadequate expression ofMHC molecules (16, 17). Results from immunotherapy trials formalignant melanoma by either active immunization or adoptive transfer of T cells suggest that the CNS may be relatively inaccessible totumor-reactive cells, because some patients developed disease progression in the brain despite tumor regression at other sites (18). Forthis reason, patients with CNS metastases are usually excluded fromimmunotherapy trials. Attempts have been made to explore the potential of adoptive immunotherapy for primary CNS malignancies,because a more favorable prognosis can be predicted by increasedtumoral lymphocyte infiltration (19, 20). However, results from numerous clinical trials of adoptive immunotherapy for brain tumorshave thus far been disappointing (21, 22).
Despite previous difficulties in generating an adequate immuneresponse in the CNS, there are reasons to believe that T lymphocytes,under appropriate conditions, can penetrate the blood-brain barrierand mediate therapeutic effects. In experimental models, active immunization of animals with allogeneic cells or syngeneic melanomacells resulted in the immunologically specific rejection of challengesin the brain with the allogeneic or tumor cells (23—25).Moreover,T-cell-mediated autoimmune responses exist in naturally occurringdiseases such as multiple sclerosis and in experimental allergic en
3 The abbreviations used are: TIL, tumor-infiltrating lymphocyte; LN, lymph node;
mAb, monoclonal antibody; TCR, T-cell receptor; SE, staphylococcal enterotoxin; CNS,central nervous system; IC, intracranial; ExF1', exfoliating toxin; CM, complete medium;IL-2, interleukin 2; WBI, whole-body irradiation; SAg, superantigen.
ABSTRACT
Adoptive transfer of tumor-sensitized T lymphocytes has demonstratedtherapeutic efficacy in animal tumor models and in some patients withmelanoma and renal cell cancers. In experimental settings, T lymphocytesderived from lymph nodes (LNs) draining progressively growing tumors
can be activated cx vivo to generate tumor-reactive lymphocytes withtherapeutic efficacy. Despite the theoretical concern regarding inaccessibifity ofthe central nervous system to systemically transferred T cells, ourrecent experiments demonstrated that anti-CD3-activated tumor-drainingLN cells are capable of mediating the regression of established intracerebral tumors. In this study, several staphylococcal enterotoxins (SEs),including SEA, SEC2, and SEE, and exfoliating toxin, known to besuperantigens, were tested for their abffity to stimulate tumor-drainingLN cells to acquire antitumor reactivity for the treatment of intracerebraltumors. SEa bind to the MHC class H molecule and provide an activatingsignal to T cells bearing particular T-cell receptor Vfi chains. Tumordraining LN celia activated with SEa demonstrated selective V@3T-cellexpansion. In adoptive immunotherapy of intracranial (IC) tumors, SEAand SEC2-activated cells had the highest efficacy, whereas SEE-activatedcells were not therapeutic. Despite the antigen independence of SE activation, the T cells retained immunological specificity for the tumor, whichprovided the initial in vivo sensitization of the LN. During the ex vivostimulation with superantigens, both CD4@ and CD8@ T cells proliferated,and both subsets were required to mediate regression of IC tumors. Incontrast to the adoptive immunotherapy of visceral tumors, the systemicadministration of exogenous interleukin 2 failed to support the antitumorreactivity In mice depleted of CD4 cells, and, in fact, it inhibited thetherapeutic efficacy. Furthermore, mice cured of intracerebral tumors bythe adoptive transfer of T cells were resistant to an IC tumor rechallenge.However, in contrast to the immunological specificity demonstrated during the primary adoptive transfer, cured mice were able to reject cladlenge with several immunologically distinct fibrosarcomas but not a melanoma. These results indicate that superantigen-activated LN cells cancirculate to and interact with intracerebral tumors mediating tumorregression in an immunologically specific manner. Although conditionsthat optimize the treatment of intracerebral tumors appear to be differentfrom those for visceral tumors, analysis of T-cell receptor Vj3expressionamong cells activated with several superantigens does not reflect a preferential usage of Vfi gene segments in the immune response to autochthonous tumors.
INTRODUCTION
It is clearly evident that during progressive tumor growth, the hostcontains T lymphocytes sensitized to tumor antigens, but other im
munological and physiological factors may have prevented an effective antitumor response from eradicating the existing tumor. However,under certain conditions, the intentional infusion of tumor-reactive Tlymphocytes may result in the regression of tumors. The use of Tlymphocytes for the treatment of cancers has been referred to as“adoptiveimmunotherapy.― Several sources of tumor-sensitized lym
Received 12/19/95; accepted 8/16/96.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I This work was supported by NIH Grants ROl CA58927 and R37 CA67324 (S. S.)
and K08 CA01580 (G. E. P.).2 To whom requests for reprints should be addressed, at FF5, Center for Surgery
Research, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195.
4702
Treatment of Intracranial Tumors by Systemic Transfer of Superantigen-activated
Tumor-draining Lymph Node T Cells'
Mamoru Lnoue, Gregory E. Plautz, and Suyu Shu2
Centerfor Surgery Research. The Cleveland Clinic Foundation. Cleveland, Ohio 44195
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

IMMUNOThERAPY OF BRAIN TUMORS WITH SAg.ACFIVATED T CELLS
cephalomyelitis (26, 27). To understand the factors that improveaccess and efficacy of T lymphocytes against IC tumors, we have useda murine model of IC inoculation of the weakly immunogenic fibrosarcomas MCA 205 and MCA 207.
The MCA 205 and MCA 207 tumors have been used to defineseveral parameters of the host immune response to syngeneic tumors(12, 14, 28). We use these tumors to develop methods that wouldallow the generation of tumor-reactive T lymphocytes during progres
sive tumor growth. Recently, we demonstrated that tumor-drainingLN cells activated ex vivo with the anti-CD3 antibody mediatedregression ofestablished IC tumors when systemically transferred (29,30). The anti-CD3 activation of T cells is polyclonal. Because theadoptive immunotherapy mediated by the activated cells is immunologically specific, it can be assumed that the anti-CD3-activated LNcells must contain a large proportion of T cells that lack the tumorspecificity but respond to the anti-CD3 stimulation. Theoretically,
immunologically specific T lymphocytes could be best activated andexpanded via stimulation with the interactions of TCR and tumorantigenic peptides presented in context with MHC molecules (3 1—33).In the absence of chemically and molecularly defined tumor antigens,this method of activation is not feasible. Alternatively, restricted
T-cell activation can be achieved with the use of superantigen molecules. Superantigens are a family of molecules that bind to MHC classII molecules to form ligands that interact with TCRs of distinct V@3regions regardless of other TCR components. As a result, each superantigen stimulates only a small fraction of T cells and, therefore, may
provide a means to preferentially activate tumor-reactive T cells. In aprevious publication, we defined conditions required for generatingimmune effector cells by some bacterial superantigens for treatmentof pulmonary metastases (14). In this study, tumor-draining LN cellsactivated with several staphylococcal superantigens were examinedfor the adoptive immunotherapy ofexperimentally induced IC tumors.Because of the V(3 specificity of the superantigen stimulation, anadditional goal was to determine whether there is overexpression ofthe TCR Vf3 regions in the immune response of LNs to syngeneictumors.
MATERIALS AND METHODS
Mice. Female C57BL/6J (hereafter called B6) mice were purchased fromThe JacksonLaboratory(Bar Harbor,ME), were at least 8 weeks of age, andweighed approximately 20 g at the time of experiments. Mice were housed ina specific pathogen-free environment and were fed food and water ad libitum.
Tumors. The 3-methylcholanthrene-induced fibrosarcomas MCA 205 andMCA207 originallyderivedin B6 mice were kindlyprovidedby Dr.JamesC.Yang (National Cancer Institute, NIH, Bethesda, MD; Ref. 34). These tumorshave been maintained in vivo by serial s.c. transplantation in syngeneic miceand were used at the third to eighth transplantation passages. Single-tumor cellsuspensions were prepared by digesting minced tumor in 40 ml HESS (LifeTechnologies, Inc., Grand Island, NY) containing 4 mg DNase I, 40 mgcollagenase type IV, and 100 units hyaluronidase type V (Sigma Chemical Co.,St. Louis, MO) for 3 h at room temperature. The tumor cells were filteredthrough a layer of Nytex 100 nylon mesh (Tetko, Inc., Briarcliff Manor, NY),washed three times with HESS, and suspended at the appropriate concentrations for IC or s.c. inoculations.
mAb. The anti-CD3 mAb (l45-2Cl 1) is a hamster IgG directed against theCD3€chainof the murineTCRCD3 complexandwas kindlyprovidedby Dr.J. Bluestone (Universityof Chicago;Ref. 35). Rat IgG2b anti-CD4(GK1.5,L3T4) and anti-CD8 (2.43, Lyt-2.2) hybridomas were obtained from theAmerican Type Culture Collection (Rockville, MD). The anti-V@3antibodylu 25(36)is a hamsterIgGlkindlyprovidedbyDr.P.Marrack(UniversityofColorado). The anti-V@5. 1 and 5.2 antibody MR9.4 (37), a mouse IgGi, and
anti-Vol 1 antibody RR3-l5 (38), a rat IgG, were kindly provided by Dr. 0.Kanagawa (Washington University, St. Louis, MO). The anti-Vj38.l-8.3 antibody F23.l and the V(38.2-specific antibody F23.2, mouse IgCi2a and IgG,
respectively, were kindly provided by Dr. R. J. Hodes (National CancerInstitute; Ref. 39). The mAbs used in this study were in ascites form producedby i.p. injection into sublethally irradiated, cyclophosphamide-treated DBA/2mice.
SEa. The enterotoxin SEA was purchased from Sigma. SEC2, SEE, andExFF were obtained from Toxin Technology, Inc. (Sarasota, FL).
fluorescence-activated Cell Sorting Analysis. Cells (5 X l0@) were in
cubated with appropriately diluted primary antibodies. F1TC-conjugatedmouse mAb to rat ,c chain (MRK-l; PharMingen, San Diego, CA), goatantihamster immunoglobulin (Kirkegand & Perry Laboratories, Gaithersburg,MD), or goat antimouse immunoglobulin (Cappel; Organon Teknika Corp.,Durham NC) was used depending on the species of the primary antibody.Stained cells (l0@) were analyzed on a FACScan (Becton Dickinson, Sunnyvale, CA). The percentage of positive cells was calculated by subtracting thebackground staining of the negative control and normalized based on thepercentage of CD3@ cells.
Tumor Inoculation. Mice were anesthetized with 0.6—0.8 mg pentobarbital i.p. Inoculation of 4 X 10―or 8 X 10―tumor cells (10 pi tumor cell
suspension of 4 or 8 X 106 cells/mi) was performed transcranially overapproximately 20 s, using a 27-gauge stainless steel needle and glass tuberculinsyringe (Perfectum; Popper & Sons, Inc., New Hyde Park, NY). The needleinsertion was perpendicular to the skull and in line with the anterior margin ofthe ear and the medial half of the right eye. The depth of insertion wascontrolled by placement of electric wire insulation as a collar over the needlewith exposure of the terminal 4 mm of the needle.
Activation of Tumor-draining LNs. s.c. tumors were established in B6mice by inoculation with 1.5 X 106tumor cells in 0.05 ml HESS in the flankregion bilaterally. Twelve days later, inguinal LNs draining the tumors wereresected under sterile conditions, teased apart with 20-gauge needles, andpressed with the blunt end of the plunger of a 10-mI plastic syringe. The cellsuspension from the combined LNs was filtered through a No. 100nylon mesh,washed, and resuspended in CM [RPM! 1640 supplemented with 10% heatinactivated FCS, 0.1 msi nonessential amino acids, 1 @tsodium pyruvate, 2mM glutamine, 100 pg/mi streptomycin, 100 units/mi penicillin, 50 pg/migentamicin, 0.5 .tg/ml amphotericin B, (all from Life Technologies), and5 x l0@ M 2-mercaptoethanol (Sigma)].
LN cells suspended at 4 X l0'@/mlwere stimulated by SEs at the followingconcentrations: SEA, 20 ng/ml; SEC2, 1 @g/m1;SEE, 1 @g/m1;and ExFT, 1iig/ml. Cells were cultured at 1 mI/well in 24-well plates in 5% CO2 at 37°Cfor 2 days.
Anti-CD3 was immobilized onto 24-well tissue culture plates, which hadbeen precoated overnight at 4°Cwith staphylococcus-protein A (Sigma) (0.3ml of a 100 ,.&g/mlsolution in PBS/well). Anti-CD3 (0.3 ml of a 2 pg/mi mAbsuspension in PBS) was incubated at 4°Cfor 4 h. Wells were washed twicewith PBS prior to the addition of 2 ml LN cells at a concentration of 2 X 106cells/mi. Cells were cultured for 2 days in 5% CO2 at 37°C.
Cells activated with either SEs or anti-CD3 were harvested, washed once,and resuspended in CM with 4 Cetus units/ml IL-2 (kindly supplied by ChironTherapeutics, Emeryville, CA; 1 Cetus unit = 6 IU) at a concentration of2 X 10@/ml in gas-permeable culture bags (Baxter/Fenwall, Deerfield, IL).After three additional days of incubation, the cells were harvested and resuspended in HESS for adoptive immunotherapy.
Adoptive Immunotherapy. Three days after IC inoculationwith tumorcells, mice received sublethal WBI, 500 cOy delivered from a ‘37Csirradiatorsource (Mark I irradiator; J. C. Shepard & Associates, Glendale, CA) beforeadoptive cell transfer. Previous experiments demonstrated that WBI augmented the efficacy of the adoptive transfer of IC tumors, although it hadminimal effects on tumor growth in the absence of cell transfer (30). Micereceived between 1 X 106 and 3 X l0@cx vivo-activated effector cells or1.2 X 108 freshly isolated tumor-draining LN cells in 1 ml through the tailvein. In some experiments, mice were also treated with IL-2 (10,000 units i.p.twice daily for eight doses). Mice were followed for survival or were euthanized by CO2 inhalation when death appeared imminent. The criteria used todetermine imminent death were palpable bulging of the skull and decreasedspontaneous and induced motor activity. These criteria were exhibited byanimals within 1—2days of spontaneous death.4
4 Unpublished observations.
4703
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 1Prol(fera:ion aml phenotype of activatedtumor-drainingSRcellsActivationProliferationThy
l.2@CD8@CD4@V@[email protected] [email protected]—[email protected]@I1Anti-CD3
SEASEC2SEEExF1'3.2
2.92.92.01.699
9298
1009763
2658714126
513326504
30>191710
<1<1<13122
1831317
<183<129
2825927
IMMUNOTHERAPYOF BRAIN TUMORS WITH SAg-ACTivATED T CELLS
T-Cell Subset Depletion. Treatmentof mice to deplete eitherthe CD4 orCD8 T-cell subset was performed immediately after adoptive transferofeffector cells. Either rat IgG, anti-CD4 mAb (L3T4, GK1.5), or anti-CD8 mAb(Lyt2, 2.43), was administered by iv. injection of 0.2 ml mAb ascites dilutedto 1.0 ml with HBSS. On imminent death of mice, spleens from two representative animals in each group were harvested, and flow cytometry wasperformed to confirm the success of T-cell subset depletion.
IC Tumor Rechallenge. Mice surviving for >60 days after adoptivetransfer of activated tumor-draining LN cells were rechallenged in the contralateral cerebral hemisphere with MCA 205 (4 X 10―cells), MCA 207(4 X 10―),MCA 203 (4 X l0@),or a clone of Bl6/BL6 melanoma (D5) cells(2 X 10@).Normal mice similarly inoculated served as controls.
Statistical Analysis. Analysis of survival was performed by the MannWhitney rank sum test.
RESULTS
Proliferation and Phenotype of SE-activated Tumor-drainingLN Cells. Single-cellsuspensionswerepreparedfromLN-drainings.c. MCA 205 tumors for 12 days. The LN cells were activated witheither immobilized anti-CD3 mAb or one of the SEs: SEA, SEC2,SEE, or ExFT. During the 2-day SE incubation, the total number ofcells did not increase; however, the percentage of T cells increasedfrom approximately 30 to 90%. The activated cells were washed and
resuspended in CM with IL-2 (4 units/mi) for an additional 3 daysprior to analysis or adoptive transfer. This sequence of culture inducesproliferation of cells but maintains their immunological specificity(14).
As shown in Table 1, there was adequate proliferation in all of thecultures, ranging from 1.6-fold expansion in the culture activated withExFT to 3.2-fold expansion in anti-CD3-activated cultures. Nearly allof the cells were T lymphocytes at the end of the culture period, andbecause the initial LN cell preparation contains approximately 35% Tlymphocytes, the expansion of T cells ranged from 4.7- to 9-fold. SEsbind to MHC class II molecules and interact with particular V@regions of the TCR. This V(3 specificity is the most notable phenotypic differences between cells activated with different SEs, whereasanti-CD3 activated T cells with a broad range of Vf3 types. The list ofVP subtypes tested for in Table 1 is not exhaustive but confirms theVP restriction of superantigen activation and is in accordance withpreviously published studies (36).
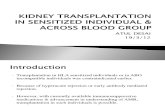
Therapeutic Efficacy of SE-activated LN Cells against IC Tumors. Mice bearing 3-day IC MCA 205 tumors were treated withsublethal WBI (500 cGy) prior to adoptive cell transfer. In an initialexperiment, 1.2 X 108 freshly isolated tumor-draining LN cells wereadministered i.v. Compared with mice that received no cell transfer,the median survival was not statistically different (17 versus 16 days;P > 0.05). This result, in which fresh tumor-draining LN cells werenot effective against IC tumors, is consistent with our previous experience in a lung metastases model (1 1, 12). Tumor-draining LN cellswere activated with SEs to determine whether they acquired therapeutic efficacy for IC tumors following ex vivo stimulation. As demonstrated in Fig. 1, adoptive transfer of 1.5 X l0@LN cells activatedwith SEA and SEC2 were highly effective, whereas anti CD3 andExFF were less effective against IC MCA 205 (P < 0.05 versuscontrols), and SEE-activated cells were ineffective. In addition, SEA-,
100 S NoCells0 AntJ-CD3
80 A SEC2.i@@ @A 0 SEE@ •EXFT
C,, 40
20
0
0 20 40 60 80 100Days PostTumorInoculation
Fig. 1. Survival of mice bearing IC tumors is mediated by activated tumor-draining LNcells. Mice (n = 5/treatment group; n 6 in no cell transfer group) were treated by theadoptive transfer iv. of 1.5 x iO@LN cells, activated with the indicated SE, on day 3 afterIC inoculationof tumors.
I 00
80
j6o
C,, 40
20
0
Days Post Tumor Inoculation
Fig. 2. Depletion of T-cell subsets abrogates the therapeutic efficacy of transferredcells. Mice (n = 5/treatment group; n = 6 in no cell transfer group) bearing 3-day ICtumors were treated by the adoptive transfer of 3 X iO@tumor-draining LN cells activatedwith SEC2. Immediately after cell transfer, mAbs directed against mouse CD4, CD8, orcontrol rat IgG were injected iv.
0 10 20 30 40 50 60
SEC2-, and anti-CD3-activated cells were superior to SEE-activatedcells (P < 0.05). An additional identically designed experiment confirmed the relative therapeutic efficacy of various SE-activated cells(data not shown). Interestingly, the survival time of mice that were notcured by ExFF or anti-CD3 treatment was similar to that of micefailing treatment with SEE.
Although there were some differences in ratios of CD4@:CD8@cells in various SE-activated cells (Table 1), this parameter did notcorrelate with therapeutic efficacy. For example, the CD4:CD8 ratioof the SEA-activated culture was 1.95, compared with 0.56 for theSEC2-activated cells. Therapeutic efficacy was also not correlatedwith the presence or absence of a particular Vf3 subset. SEC2-activated cultures were highly restricted to the [email protected] subset, whichwas minimally present in SEA-activated cultures. On the other hand,V@3 and Vf3ll subsets were amplified in cultures stimulated withSEA, which were therapeutic, and in SEE-activated cultures, whichwere not therapeutic.
TheRoleof CD4and CD8T Cellsin AdoptiveImmunotherapyand the Effects of Systemic Exogenous IL-2. Both CD4@ andCD8@ T-cell subsets were needed for the treatment of IC tumors.Depletion of either cell population in the SEC2-activated cell popu
4704
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

0
IMMUNOTHERAPYOF BRAIN TUMORS WITH SAg.ACTIvATED T CELLS
0 NoCeIls,HBSS
0 lL-2 D3-D6. IL-2 D4-D7. IL-2 D5-D8
@ lL-2D6-D9
NoCells,HBSSNo Cells,lL-2 80Cells, HBSSCells, IL-2 60
40
20
Fig. 3. Inhibitory effect oflL-2 on the treatment ofIC tumors bythe adoptivetransferof activatedtumor-drainingLN cells.Mice(n 5) were treated on day three (D3) after IC tumor inoculationby theadoptivetransferof 3 X [email protected], IL-2 (KY'units)or HBSSwasadministeredi.p. twicedaily for 4days staiting immediately after cell transfer. B, IL-2 treatment wasstarted at the indicated times after tumor inoculation and continued
for 4 days.
0
0 20 40 60 80 100 0 20 40 60 80 100
DaysPostTumorInoculation
lation after adoptive transfer abrogated the response (P = 0.0317; Fig.2). In addition, systemic IL-2 was found to inhibit the efficacy ofadoptively transferred cells against IC tumors, (P = 0.0317; Fig. 3A).The inhibitory effect of IL-2 could be demonstrated by delaying theinitiationof IL-2 treatmentfor up to 3 days after adoptivetransfer(Fig. 3B). Systemic IL-2 in the absence of cell transfer did not changethe median survival time of mice with IC tumors.
The activation protocol for these experiments includes culture inlow-dose IL-2 following superantigen activation. During the 3-dayculture in IL-2, T cells usually expand 6—10-fold in number. Therelative therapeutic activity of LN cells after 2-day SEC2 activation orafter an additional 3 days ofculture in IL-2 was compared by adoptivetransfer into mice bearing 3-day IC tumors. As shown in Fig. 4, allmice were cured by transfer of the highest cell dose studied, 9 X 106cells, activated with SEC2 alone or after an additional 3-day culture inlow-dose IL-2. Interestingly, at a dose of 3 X 106 cells, at whichintermediate efficacy was observed, there was not a statistically significant difference in the tumor regression rate (P > 0.05). Thisindicates that during expansion of T cells in IL-2, the antitumorreactivity per cell did not increase or decrease significantly.
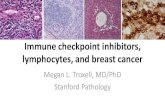
The Antitumor Response Is Initially Tumor Specific but Dinplays Cross-Reactivity on Tumor Rechallenge. The activationofTcells by SEs occurs indirectly through the presentation of SE molecules by MHC class II molecules and certain V@3elements ofthe TCR.Because this interaction is independent of the antigen-specific T-cellrecognition, the immunological specificity of the antitumor responsewas tested. In a crisscross experiment, cells derived from LN-drainingMCA 205 tumorsand activatedby SEC2 were found to be effectiveagainstIC MCA205 tumorsbut not againstthe antigenicallydistinctMCA 207 tumor (P = 0.0079; Fig. 5). Similarly, SEC2-activatedMCA 207 tumor-drainingLN cells were only active againstIC MCA
207 but not MCA 205 tumors (P = 0.0079). This result demonstrates,as have previous experiments, that the antitumor response mediatedby the activated LN cells is highly specific, and the specificity isdetermined during the in vivo sensitization of tumor-draining LNs.
Animals cured of MCA 205 IC tumors for more than 60 days wererechallenged with a second IC tumor inoculation. These animalsrejected the second inoculum of the same tumor (Fig. 6). Unexpectedly, mice cured of IC MCA 205 tumors often rejected secondarychallenges with antigenically distinct but histologically related tumors, including other weakly immunogenic fibrosarcomas, MCA 207,and MCA 203. The survival of mice cured of IC MCA 205 tumorschallenged with MCA 207 or MCA 203 tumors was not statisticallydifferent than that of mice rechallenged with MCA 205 tumors(P = 0.1049 and I, respectively). However, this cross-reactivity didnot extend to another tumor of a different histological type. The D5tumor, a subclone of the B16IBL6 melanoma, grew progressively,
with only a slight delay in most MCA 205-cured recipients in comparison to naive mice. There was also a statistically significant dif
ference in survival for MCA 205-cured mice rechallenged with MCA205 compared with D5 (P 0.0019). However, even for this histologically unrelated tumor, several animals demonstrated prolongedsurvival.
DISCUSSION
Tumor-draining LNs contain a mixture of cells, including MHCclass Il-positive, antigen-presenting cells such as macrophages, dendritic cells, and B cells that are capable of presenting SEs for T-cell
stimulation. During the first 2 days of superantigen stimulation, thetotal cell number did not increase; however, the percentage of T cells
increased from approximately 35% to greater than 90%, indicating
No Cell Transfer1X1@cells3X lOcells9X 10@cells
I00
80
60
40
20
0
Fig. 4. Comparison of the antitumor activity of tumor-draining@LN cells activated for 2 days with SEC2 or after expansion in@IL-2-containing medium for an additional 3 days. Graded doses ofactivated cells were infused iv. into mice(n = 5)bearing 3-day ICtumors. 0
0 102030405060 0 102030405060
DaysPostTumorInoculation
4705
A B100-___J@,. 100
Ic
@::‘,@,.
Two Day Activation Five Day Activation
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

IMMUNOTHERAPYOF BRAIN TUMORS WITH SAg-ACFIvATED I CELLS
I 00
80
•@60
(1@ 40
20
I00
80
60
40
20
0
0 No CellTransfer0 MCA2O5LNt@ MCA2O7LN
Fig. 5. Specificity ofthe antitumor response mediated by the adoptivetransfer of activated tumor-draining LN cells. Mice (n = 5) bearingeither IC MCA 205 or MCA 207 tumors were treated by the adoptivetransfer of 3 x io@SEC2-activated cells derived from LNs drainingeitherMCA205or MCA207tumors.
0
0 10 20 30 40 50 60 0 10 20 30 40 50 60
DaysPostTumorInoculation
selective T-cell proliferation. Vigorous T-cell proliferation becameclearly evident during the ensuing 3-day culture with IL-2. The totalexpansion of T lymphocytes ranged from 5- to 9-fold over the 5-dayculture period, and virtually all of the recovered cells were T lym
phocytes. Because the V3 subsets stimulated by the SEs were initiallya minority of the T-cell population, their relative expansion was evengreater than 5—9-fold.One of the critical requirements for the development of clinical adoptive immunotherapy is the ability to rapidlyexpand populations of T cells in vitro. The results from this studysuggest that supemantigen stimulation may afford a means to generatea large number of T cells for clinical use. However, because T-cellstimulation with supemantigens requires the presentation by MHCclass 11-positive accessory cells, additional stimulation of activated
cells may require the presence of these cells. In humans, activated Tlymphocytes often express MHC class 11molecules on their surface.Whether these induced molecules are sufficient to present superantigens remains to be confirmed.
The impetus for the current study using superantigen-stimulatedcells for immunotherapy came from numerous documented observations of restricted use of TCR gene segments that were selectivelyexpressed on T cells infiltrating solid tumors (40—43).Most of theseanalyses were carried out in patients without the simultaneous consideration of HLA alleles. Recently, a number of genes encodingmelanoma antigens, recognized as peptides presented by MHC classI molecules to CTLs, have been identified (44—50).In a patientpopulation matched for HLA-A2, TCR V(314 was demonstrated to be
MCA 205
100 -
80 -
60 -
40 -
20 -
0
I 00
80
60
40
20
0
—.—Naivemice—.--- MCA2O5 Cured
m>
(1)
I 00
80
60
40
20
I-I I I I I 0
0 102030405060 0 102030405060
MCA 203 D5
I00
80
60
40
20
0
0 10 20 30 40 50 60 0 10 20 30 40 50 60
Days After Tumor Rechallenge
Fig. 6. Cross-reactive antitumor response in mice cured of IC tumorsby the adoptive transfer of activated LN cells. Mice cured of IC MCA205 tumors by the adoptive transfer of 3 X iO@SEC2-activated LN cellswere rechallenged more than 60 days after the initial tumor inoculation.The fibrosarcomasMCA 207, MCA 203, and melanomaD5 wereinoculated in the contralateral hemisphere from the original MCA 205tumor (n = 8/group), and survival time after the secondary tumorchallenge was determined. Naive mice (n 5) were simultaneouslyinoculated with an identical dose of the indicated tumors.
4706
MCA 205 Tumor MCA 207 Tumor
MCA 207
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

IMMUNOTHERAPYOF BRAIN TUMORS WITH SAg-ACTIVATED I CELLS
overexpressed at the site of primary melanoma lesions (5 1). However,a lack of preferential TCR gene segment use has also been reported inmalignant melanoma (52).
if there is selection in TCR use in response to malignant tumorcells, it should be readily demonstrated with defined transplantabletumors in syngeneic animals. Such studies have been reported byseveral groups of investigators. For example, the immune response to
the MOPC-3.5 plasmacytoma appeared to be restricted to the CD8@TCR [email protected] (53). A preferentialuse of the TCR V(310gene wasreported to be the predominant T-cell immune response in spontaneous regression of the virally induced FBL-3 leukemia (54). In contrast, analysis of distribution of V@ usage by ilLs from progressivelygrowing methylcholanthrene-induced fibrosarcomas and a dimethylhydrazine-induced colon adenocarcinoma of B6 origin revealed abroad distribution of V@ phenotypes; although differences in frequency in comparison to spleen cells were observed (55). When TILswere examined for V@use after a period of in vitro culture, individualcultures rapidly became dominant for a single Vf3 phenotype. Therewas, however, no association of a specific V@ with tumor specificity.Although these data suggest the complexity of immune responses tosyngeneic tumors, it is also clear that different T-cell phenotypes canindependently mediate antitumor effects.
Our results are consistent with the conclusion that the selection oftumor-specific T cells is not reflected in any simple predominance ofVP use. The panel of SEs we tested induced the activation andproliferation of several Vj3 T cells, including V@33,Vf35, Vf38.2, andVj311. Antitumor efficacy did not seem to correspond to the prevalence of a particular V@ subset or its absence. For example, two V13species, V@3 and V31l, were amplified in cultures stimulated withSEA, which are therapeutically effective, as well as in cultures stimulated with SEE, which were ineffective. To further support thisconclusion, our recent study with the MCA 106 fibrosarcoma mdicates that at a clonal level, T cells with several V(3 phenotypes canequally mediate tumor regression (28).
Treatment of T lymphocytes with antibodies against CD3 or exposure to SEs has been reported to cause apoptosis in vivo and in vitro(56—58).Under the activation conditions used in these experiments,we observed continual proliferation through the duration of cultureand functional antitumor activity on adoptive transfer. One possibilityis that the T cells sensitized in vivo to tumor antigens were at a stageof differentiation that permitted proliferation and activation by SEexposure. However, the equivalent activity of cells after only 2-daySEC2 activation and cells after subsequent expansion in IL-2 for anadditional 3 days does not support this conclusion. Because 3-dayincubation with IL-2 resulted in an increase in net effector cellnumbers, we routinely include IL-2 expansion as part of the ex vivoactivation procedure. The presence of antigen-presenting cells in thelymph node culture during activation may have influenced proliferation of SE-stimulated cells, as has been observed in other systems (59,60).Theantitumorimmuneresponsepersistsin thehostandmediatesresistance to rechallenge.
Analogous to the adoptive immunotherapy of the same tumor,MCA 205, at a different histological site (e.g., lung), an effectiveantitumor response to IC tumors required both CD4@ and CD8@subsets. In a separate study, we have demonstrated by immunohistochemistry the presence of SEC2-activated [email protected]@T cells of bothCD4@ and CD8@ subsets infiltrating IC tumors following iv. adoptive transfer of SEC2-activated LN cells (61). In previous experimentsin which pulmonary MCA 205 metastases were treated with antiCD3- or SEB-activatedT cells, the administrationof systemic IL-2(15,000 units twice daily for eight doses) restored therapeutic efficacyin CD4@ cell-depleted animals, and in general, systemic IL-2 enhanced the function of mixed cultures consisting of both CD4@ and
CD8@ cells (11, 14). In contrast, for the treatment of IC tumors, IL-2inhibited the antitumor efficacy of transferred cells. This inhibition ofeffector cell function is apparent even if the IL-2 dose is delayed for48 h after cell transfer. The mechanism of inhibition by IL-2 has notyet been determined. Perhaps IL-2 affects the ability of effector cellsto migrate to the IC tumor site. IL-2 can cross the blood-brain barrierand induces vascular leak at the site of CNS tumors (62, 63). It maythus impose inhibitory effects in the local environment of the CNS.
The observation of considerable cross-reactivity between severalantigenically distinct tumors on rechallenge of cured animals wasinteresting but puzzling in light of the exquisite immunological specificity displayed by the transferred cells during the primary rejectionresponse. Cross-reactivity was not observed for all tumors tested; infact, followinginoculationof the B16IBL6melanomatumorline D5,there was only a slight prolongation in survival for most MCA205-cured mice compared with naive mice. It is possible that additional immune responses were generated during tumor rejectionagainst epitopes that are shared by other closely related malignanttumor lines, in particular, fibrosarcomas. T cells with a phenotype thatfacilitates their migration across the CNS vasculature may have beenselectively amplified during the primary rejection response. Altematively, the primary antitumor response may have induced long-termchanges in either the vasculature or the activity of nonspecific effectorcells within the CNS, which may facilitate the rejection of tumors withshared or closely related antigenic epitopes. Mice cured of IC tumorsdisplayed normal behavior during a prolonged observation periodafter tumor regression, suggesting that any of the possible changes inthe immunologically privileged status of the CNS did not significantlyaffect neurological function. Because the tumor cell lines used in these
studies are not derived from CNS tissue, the question of whetherimmune responses to cross-reactive neural epitopes develop in theregression of primary CNS neoplasms remains. Future studies withtumors derived from glial or neural elements will help address thesequestions and further define the criteria for successful adoptive immunotherapy of IC tumors.
REFERENCES
1. DeVries, J. E., and Spits, H. Cloned human cytotoxic lymphocyte lines reactive withautologous melanoma cells. J. Immunol., 132: 510—519, 1983.
2. Mukherji, B., and MacAlister, T. J. Clonal analysis of cytotoxic T cell responseagainst human melanomas. J. Exp. Med., 158: 240—245,1983.
3. Anichini, A., Mazzocchi, A., Fossati, 0., and Parmiani, G. Cytolytic T lymphocyteclones from peripheral blood and from tumor site detect intratumor heterogeneity ofmelanoma cells. J. Immunol., 142: 3692—3701, 1989.
4. Knuth, A., Wolfel, T., Klehmann, E., Boon, T., and Meyer Zum Buschenfelde, K. H.Cytolytic T-cell clones against an autologous human melanoma: specific study anddefinition of three antigens by immunoselection. Proc. Nail. Acad. Sci. USA, 86:2804—2808,1989.
5. Cozzolino, F., Torcia, M., Carossino, A., Giordani, R., Selli, C., Talini, 0., Realhi,E.,Novelli, A., Pistoia, V., and Ferrarmni,M. Characterization of cells from invadedlymph nodes in patients with solid tumors. J. Exp. Med., 166: 303—318,1987.
6. Barnd,D., Kerr,L., Metzgar,R., and Finn.0. Humantumor-specificT cell linesgenerated from invaded lymph nodes in patients with solid tumors. Transplant. Proc.,20: 339—341,1988.
7. Mukheiji, B., Guha, A., Chakrebarty, N., Sivandham, M., Nafted, A., Sporn, J., andErgin, M. Clonal analysis of cytotoxic and regulatory T cell responses against humanmelanoma. J. Exp. Med., 169: 1961—1967,1989.
8. Whiteside, T. L., Miescher, S., Hulimann, J., Moretta, L., and Von Hiedner, U. Clonalanalysis and in situ characterization of lymphocytes infiltrating human breast carcinomas. Cancer lmmunol. Immunother., 23: 169—178,1986.
9. Muul,L. M., Spiess,P. J., Director,E. P., and Rosenberg,S. A. Identificationofspecific cytolytic immune response against autologous tumor in humans bearingmalignant melanoma. J. Immunol., 138: 989—995,1987.
10. Topalian,S. L., Soloman,D., and Rosenberg,S. A. Tumor-specificcytolysisbylymphocytes infiltrating human melanomas. J. Immunol., 142: 3714—3725,1989.
11. Shu, S., Chou, T., and Rosenberg, S. A. Generation from tumor-bearing mice oflymphocytes with in vitro therapeutic efficacy. J. Immunol., 139: 295—304,1987.
12. Yoshizawa, H., Chang, A. E., and Shu, S. Specific adoptive immunotherapy mediatedby tumor-draining lymph node cells sequentially activated with anti-CD3 and IL-2.J. Immunol., 147: 729—737,1991.
13. Crossland, K. D., Lee, V. K., Chen, W., Riddell, S. R., Greenberg, P. D., and Cheever,
4707
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

IMMUNOTHERAPYOF BRAIN TUMORS WITH SAg.ACflVATED I CELLS
M. A. T cells from tumor-immunemice nonspecificallyexpandedin vitro withanti-CD3 plus IL-2 retain specific function in vitro and can eradicate disseminatedleukemia in vitro. J. Immunol., 146: 4414—4420,1991.
14. Shu, S., Krinock, R. A., Matsumura. T., Sussman, i. J., Fox, B. A., Chang, A. E., andTerman, D. S. Stimulation of tumor-draining lymph node cells with superantigenicstaphylococcal toxins leads to the generation of tumor-specific effector T cells.J. Immunol., 152: 1277—1288,1994.
15. Marrack, P., and Kappler, J. The staphylococcal enterotoxins and their relatives.Science (Washington DC), 248: 705—711, 1990.
16. Fontana, A., and Fierz, W. The endothelium-astrocyte immune control system of thebrain. Semin. Immunopathol., 8: 57—70,1985.
17. Lampson, L. A., and Hickey, W. F. Monoclonal antibody analysis of the MHCexpression in human brain biopsies. J. Immunol., 136: 4054—4062,1986.
18. Mitchell, M. S. Relapse in the central nervous system in melanoma patients successfully treated with biomodulators. J. Clin. Oncol., 7: 1701—1709,1989.
19. Di Lorenzo, N., Palma, L., and Nicole, S. Lymphocytic infiltration in long-survivalglioblastomas: possible host's resistance. Acts Neurochir., 39: 27—33,1977.
20. Palma, L., Di Lorenzo, N.. and Guidetti, B. Lymphocytic infiltrates in primaryglioblastomas and recidivous gliomas. Incidence, fate and relevance to prognosis in228 operated cases. J. Neurosurg., 49: 854—861,1978.
21. Sawamura, Y., and de Tribolet, N. Immunotherapy of brain tumors. J. Neurosurg.Sci., 34: 265—278,1990.
22. Lillihei, K. 0., Mitchell, D. H., Johnson, S. D., McCleary, E. L., and Kruse, C. A.Long-term follow-up of patients with recurrent malignant gliomas treated withadjuvant adoptive immunotherapy. Neurosurgery, 28: 16—23,1991.
23. Medawar, P. W. Immunity to homologous grafted skin. Ill. The fate of skin homogralts transplanted to the brain, to subcutaneous tissue, and to the anterior chamberof the eye. Br. J. Exp. Pathol., 29: 58—69,1948.
24. Takai, N., Tanaka, R., Yoshida, S., Ham, N., and Saito, T. in Vivaand in Vitroeffectof adoptive immunotherapy of experimental murine brain tumors using lymphokineactivated killer cells. Cancer Res., 48: 2047—2052,1988.
25. Staib, L., Hat-el,W., and Mitchell, M. S. Protection against experimental cerebralmetastases of murine melanoma B 16 by active immunization. Cancer Res., 53:1113—1121,1993.
26. Raine, C. S. Biology of disease. The analysis of autoimmune demyelination: itsimpact upon multiple sclerosis. Lab. Invest., 50: 608—635, 1984.
27. Hafler, D. A., and Weiner, H. L. T cells in multiple sclerosis and inflammatory centralnervous system disease. Immunol. Rev., 100: 307—332,1987.
28. Matsumura, T., Sussman. J. J., Krinock, R. A., Chang, A. E., and Shu, S. Characteristics and in Vivo homing of long-term T-cell lines and clones derived fromtumor-draining lymph nodes. Cancer Res., 54: 2744—2750,1994.
29. WahI, W. L., Sussman, J. J., Shu, S., and Chang, A. E. Adoptive immunotherapy ofmurine intracerebral tumors with anti-CD3/interleukin-2-activated tumor-draininglymph node cells. J. Immunother., 15: 242—250,1994.
30. Sussman, J. J., Wahl, W. L., Chang, A. E., and Shu, S. Unique characteristicsassociated with systemic adoptive immunotherapy of experimental intracerebral tumors. J. Immunother., 18: 35—44,1995.
31. Feltkamp, M. C. W., Smits, H. L., Vierboom, M. P. M., Minnaar, R. P., de Jongh,B. M., Drijfbout, J. W., Icr Schegget, J., Melief, C. J. M., and Kast, W. M.Vaccination with cytotoxic T lymphocyte epitope-containing peptide protects againsta tumor induced by human papillomavirus type 16-transfonned cells. Eur. J. Immunol., 23: 2242—2249,1993.
32. Irvine, K. R., McCabe, B. J., Rosenberg, S. A., and Restifo, N. P. Syntheticoligonucleotide expressed by a recombinant vaccinia virus elicits therapeutic Cl'L.J. Immunol., 154: 4651—4657,1995.
33. Mukheiji, B., Chakraborty, N. G., Yamasaki, S., Okino, T., Yamase, H.. Spom, J. R.,Kurtzman, S. K., Ergin, M. T., Ozols, J., Meehan, J., and Mauri, F. Induction ofantigen-specific cytolytic T cells in situ in human melanoma by immunization withsynthetic peptide-pulsed autologous antigen presenting cells. Proc. Natl. Acad. Sci.USA,92: 8078—8082,1995.
34. Barth,R. J., Jr., Bock,S. N., Mule,J. J., and Rosenberg,S. A. Uniquemurinetumor-associated antigens identified by tumor infiltrating lymphocytes. J. Immunol..144: 1531-1537, 1990.
35. Leo, 0., Foo, M., Sachs, D. H., Samelson, L. E., and Bluestone, J. A. Identificationofa monoclonal antibody specific for a murine T3 polypeptide. Proc. NatI. Acad. Sci.USA,84: 1374—1378,1987.
36. Pullen. A. M., Man-ack, P., and Kappler, J. W. The T cell repertoire is heavilyinfluenced by tolerance to polymorphic self-antigens. Nature (Lond.), 335: 796—801,1988.
37. Reich, E. P., Sherwin, R. S., Kanagawa, 0., and Janeway, C. A. J. An explanation forthe protective effect of MHC class II I-E molecule in murine diabetes. Nature (Lond.),341: 326—328,1989.
38. Bill, J., Kanagawa, 0., Woodland, D. L., and Palmer, E. The MHC molecule I-E isnecessary but not sufficient for the clonal deletion of V@3l1-bearing T cells. J. Exp.Med., 169: 1405—1419,1989.
39. Staerz, U., Rammansee, H., Benedeno, J., and Bevan, M. Characterization of amurine monoclonal antibody specific for an allotype determinant on T cell antigenreceptor. J. Immunol., 134: 3994—4000.1985.
40. Nina, T., Oksenberg, J. R., Rao, N. A., and Steinman, L. Prodominant expression of
T cell receptor Va7 in tumor-infiltrating lymphocytes in uveal melanoma. Science(Washington DC), 249: 672—674, 1990.
41. Weidman, E., Whiteside, T. L., Giorda, R., Herberman, R. B., and Truco, M. TheT-cell receptor V@3gene usage in tumor-infiltrating lymphocytes and blood of patientswith hepatocellular carcinoma. Cancer Res., 52: 5913—5920,1992.
42. Ikeda, H., Sato, N., Matsunnra, A., and Kikuchi, K. Analysis of T-cell receptor Vregion usage of cytotoxic T lymphocytes and tumor-infiltrating lymphocytes derivedfrom human autologous gastric signet ring cell carcinoma. Cancer Res., 53: 3078—3084, 1993.
43. thor Straten, P., Scholler, J., Hou-Jensen, K., and Zeuthen, J. Preferential usage ofT-cell receptor a@variable regions among tumor-infiltrating lymphocytes in primaryhuman malignant melanomas. Int. J. Cancer, 56: 78—86,1994.
44. Brichard, V., Van PcI, A., Wolfel, T., Wolfel, C., Dc Plaen, E., Lethe, B., Coulie, P.,and Boon, T. The tyrosinase gene codes for an antigen recognized by autologouscytolytic T lymphocytes on HLA-A2 melanomas. J. Exp. Med., 178: 489—495,1993.
45. Bakker, A. B., Schreurs, M. W., de Boer, A. J., Kawakami, Y., Rosenberg, S. A.,Adema, 0. J., and Figdor, C. G. Melanocyte lineage-specific antigen gplOO isrecognized by melanoma-derived tumor-infiltrating lymphocytes. J. Exp. Med., 179:1005—1009,1994.
46. Kawakami, Y., Eliyahu, S., Delgado, C. H., Robbins, P. F., Sakaguchi, K., Appella,E.. Yannelli, J. R., Adema, G. J., Miki, T., and Rosenberg, S. A. Identification of ahuman melanoma antigen recognized by tumor infiltrating lymphocytes associatedwith in vivo tumor rejection. Proc. Nail. Acad. Sci. USA, 91: 6458—6462,1994.
47. Coulie, P. G., Brichard, V., Van PcI, A., Wolfel, T., Schneider, J., Traversari, C.,Mattei, S., De Plaen, E., Lurquin, C.. Szikora, J., Renauld, J., and Boon, T. A newgene coding for a differentiation antigen recognized by autologous cytolytic Tlymphocytes on HLA-A2 melanomas. J. Exp. Med., 180: 35—42,1994.
48. Kawakami, Y., Eliyahu, S.. Delgado, C. H., Robbins, P. F., Rivoltini, L., Topalian,S. L., Miki. T., and Rosenberg, S. A. Cloning of the gene coding for a shared humanmelanoma antigen recognized by autologous T-cells infiltrating into tumor. Proc.NatI. Acad. Sci. USA, 91: 3515—3519,1994.
49. van der Bruggen. P., Bastin, J., Gajewski, T., Coulie, P. G., Boel, P., De Smet, C.,Traversari, C., Townsend, A., and Boon, T. A peptide encoded by human geneMAGE-3 and presented by HLA-A2 induces cytolytic T lymphocytic T lymphocytesthat recognize tumor cells expressing MAGE-3. Eur. J. Immunol., 12: 3038—3044,1994.
50. Darrow, T. L., Slingluff, C. L., and Seigler, H. F. The role of HLA class I antigensin recognition of melanoma cells by tumor-specific cytotoxic T lymphocytes: cvidence for shared tumor antigens. J. Immunol., 142: 3329—3335,1989.
51. Salvi, S., Segalla, F., Rao, S., Arianti, F., Sartori, M., Bratina, G., Caronni, E.,Anichini, A., Clemente, C., Parmiani, G., and Sensi, M. Overexpression of the T-cellreceptor @3-chainvariable region TCR@VI4 in HLA-A2-matched primary humanmelanoma. Cancer Res., 55: 3374—3379,1995.
52. Ferradini, L., Raman-Roman, S., Azocar, J., Avril, M., Viel, S., Triebel, F., andHercend. T. Analysis of T-cell receptor &@variability in lymphocytes infiltrating amelanoma metastasis. Cancer Res., 52: 4649—4654,1992.
53. Mokyr, M. B., Rubin, M., Newell, K. A., Prokhorova, A., and Bluestone, J. A.Involvement if TCR-VfJS.3+ cells in the cure of mice bearing a large MOPC-3l5tumor by low dose melphalan. J. Immunol.. 151: 4838—4846,1993.
54. Suzuki, M., Koseki, H., Mizutani, Y., Kuribayashi, K., Kanno, M., and Taniguchi, M.Expansion of murine T cells bearing a unique T cell receptor @3-chainin Friendvirus-induced tumor in situ. J. Immunol., 148: 2968—2974, 1992.
55. Karpati, R. M., Banks, S. M., Malissan, B., Rosenberg, S. A., Sheard, M. A., Weber,J. S., and Hodes, R. J. Phenotypic characterization of murine tumor-infiltrating Tlymphocytes. J. Immunol.. 146: 2043—2051,1991.
56. Dhein, J., Walczak, H., Baumier, C., Debatin, K., and Krammer, P. H. AutocrineT-cell suicide mediated by APO- l/(Fas/CD95). Nature (Lond.), 373: 438—441, 1995.
57. Schwartz, R. H. A cell culture model for T lymphocyte clonal anergy. Science(Washington DC), 248: 1349—1356,1990.
58. Kawabe, Y., and Ochi, A. Programmed cell death and extrathymic reduction of V@8@CD4@ T cells in mice tolerant to Staphylococcus aureus enterotoxin B. Nature(Lond.), 349: 245—248,1991.
59. Kabelitz, D., and Wesselborg, S. Life and death of a superantigen-reactive humanCD4@ T cell clone: staphylococcal enterotoxins induce death by apoptosis butsimultaneously trigger a proliferative response in the presence of HLA-DR@ antigenpresenting cells. Int. Immunol., 4: 1381—1388,1992.
60. Groux, H., Monte, D., Plouvier, B., Capron, A., and Ameisen, J-C. CD-3 mediatedapoptosis of human medullary thymocytes and activated peripheral T cells: respectiveroles of interleukin-l, interleukin-2, interferon-y, and accessory cells. Eur. J. Immunol.,23: 1623—1629,1993.
61. Plautz, G. E., Inoue, M., and Shu, S. Defining the synergistic effects of irradiation andT-cell immunotherapy for murine intracranial tumors. Cell. Immunol., 171: 277—284,1996.
62. Saris, S. C., Rosenberg, S. A., and Friedman, R. B. Penetration of recombinantinterleukin-2 across the blood-cerebrospinal fluid barrier. J. Neurosurg., 69: 29—34,1988.
63. Saris, S. C., Patronas, N. J., Rosenberg. S. A., Alexander, J. T., Frank, J., Schwartzentruber, D. J., Rubin, J. T., Barba, D., and Oldfield, E. H. The effect of intravenous
interleukin-2 on brain water content. J. Neurosurg., 71: 169—174,1989.
4708
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1996;56:4702-4708. Cancer Res Mamoru Inoue, Gregory E. Plautz and Suyu Shu Superantigen-activated Tumor-draining Lymph Node T CellsTreatment of Intracranial Tumors by Systemic Transfer of
Updated version
http://cancerres.aacrjournals.org/content/56/20/4702
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/56/20/4702To request permission to re-use all or part of this article, use this link
on May 20, 2020. © 1996 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from