Congenitally Missing Upper Laterals. Clinical Considerations: Orthodontic Space Closure
Upload
nguyenxuyenCategory
view
216download
0
Carmine Di StasiRadiology and Interventional Radiology Department
Catholic University – Rome
Fond. Policlinico Universitario A. Gemelli
Treatment of abscesses and hepatic cysts

Cysts - classification
• Simple cysts
• Echinococcosis
• Cystadenoma and cystadenocarcinoma
• Polycystic liver disease (PLD)

Simple Cysts
• Arise congenitally from
aberrant bile duct
• Inner layer cuboidal biliary epithelial cells
• Clear, bile-like, fluid
• Without connection to the biliary tree

Cysts - epidemiology
• Estimated prevalence of benign
non-parasitic lesions is 3-18 %
in the general population
• 15% of these patients are symptomatic (abdominalpain and distention, dyspnea, early satiety, nausea)
Benzimra J et al Eur Radiol 2014

Simple Cysts - Treatment
• “Wait-and-see” policy
If there are symptoms:
• Percutaneus treatment
• Laparoscopic or open surgical fenestration techniques

Simple Cysts - Treatment
Percutaneus treatment
vs
Laparoscopic fenestration

Simple Cysts - Treatment
• Percutaneous sclerotherapy as effective as laparoscopicunroofing, with a lower incidence of complications, shorterhospital stays and lower recurrence rates
• Cyst fenestration (review of 43 studies): reduction of symptoms was found in 92 % of treated patients
• 22 % of laparoscopic procedures were converted to open fenestration ; overall morbidity of cyst fenestration: 11-23%
Titus F. M. Wijnands et al Eur Radiol 2016

Percutaneus treatment
• Percutaneus aspirationmere aspiration of cystic fluid leads to complete recurrence of the cyst
• Percutaneus drainage- no fluid reaccumulation compared to aspiration- only principal option when the cysts comunicates with vital structures
(biliary system, pancreatic duct) because sclerotherapy is contraindicated- occasionally, suction drainage leads to a chronically collapsed cyst and the
ultimate goal of cyst obliteration
(infection risk; patient discomfort; occasionally successful)
• Sclerotherapytetracycline, bleomycin, n-butyl cyanoacrylate with iodizedoil, sodium tetradecyl, hypertonic saline, ethanolamineoleate, acetic acid, ethanol

Sclerotherapy : technicque
• Typically 6-8 F pigtail catheter is inserted into the cyst via the Seldinger or Trocar technique
• All of the fluid is aspirated (culture , cytology mucinous fluid on needle aspirationindicates an underlying cystadenoma)
• Diluted contrast is injected through the catheter under fluoroscopic guidance or CT scan can be performed after injection to exclude leakage of fluid into the peritoneum or communication with blood vessels or biliary system
• After ethanol has been injected into the cyst, the patient should be rotated from prone to supine to right and left lateral decubitus positioning so the alcohol can contact the entire cyst wall. The patient should spend 5 to 10 minutes in each position, and the alcohol should be left in the cyst cavity for a minimum of 20minutes. The alcoholshould then be completely aspirated

Sclerotherapy: Ethanol
• Ethanol causes protein denaturation, cell death, and inflammatory fibrosis after contacting the cyst wall
• 10-50% (more often 25-30%) of the aspirated cyst volume is replaced with 95% ethanol
• The maximum volume of ethanol should be limited to 100-200mL in adults to avoid alcoholtoxicity from systemically absorbed alcohol
• In the literature, the duration of alcohol dwell time within the cystic cavity differs 10 min to 4 h
• Blood ethanol concentration related with alcohol volume injected into the cystic cavity duringprocedure (do not exceed toxic levels in sclerotherapy with duration of 4 h and alcohol volumesless than 200 cc)
Okan Akhan et al Cardiovasc Intervent Radiol 2015

Efficacy and safety of sclerotherapy
• 89.6% of patients had either disappearance (54.7%) or reduction of symptoms. No patients reportedaggravation of symptoms. Symptomatic reduction in 72–100% of patients; complete symptomdisappearance from 56% to 100%
• patients with lower diameter reduction at one month or with haemorrhagic cysts had higher risk of having a suboptimal technical response at six months
• strong hepatic cyst reduction following aspiration sclerotherapy predicts complete clinical response
• haemorrhagic cyst / limited cyst size reduction at one month predicted suboptimal long-term cystreduction but did not affect clinical response
• prolonged exposure of the sclerosing agent to the cyst wall seems to improve efficacy of treatment butthe impact of duration of sclerotherapy on treatment efficacy remains to be tested
• The most common adverse event was pain. This was reported in 8 of 13 studies with a range between 5% and 90%
Titus F.M. Wijnands AJR 2017 (review)
Titus F.M. Wijnands et al Eur Radiol 2016
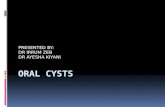
Hydatid cysts
Morphologic evolution
CE 1Fine back echoesVisible cyst wall
CE 2 a-b-cMultiseptated cyst(daughter cysts)“wheel-like”“rosette-like”“honeycomb-like”
CE 3 a-bDetachement of membrane Degenerating daughter cysts“water-lily” appearance
CE 4 a-bNo liquid component“ball of wool”Degenerating membranes
CE 5Thick calcified wallDegree of calcification from partial to complete
ACTIVE TRANSITIONAL INACTIVE
Medical and percutaneous, or surgical treatment No treatment
Gharbi 1 Gharbi 3 Gharbi 2 Gharbi 4 Gharbi 5
Caremani M et al Giornale Italiano di Ecografia 2005WHO Informal Working Group Acta Tropica 2003

Hydatid cystis -treatment-
Percutaneous t. + chemotherapy > Surgical treatment
• greater clinical efficacy• lower rates of morbidity, mortality, disease recurrence
• PAIR (Puncture, Aspiration, Injection, Re-Aspiration ): ethanol / 20% hypertonic saline
• > 6 cm drainage (8 F) placement after puncture (Single Puncture Catheterization)
• MoCAT (modified catheterization-14F-) daughter vesicles disrupted and removed from the cavitybefore sclerotherapy with alcohol
- technical success rate 99.5%- major complications (anaphylaxis) < 1% - minor) complications (bil fistula, abscess) 10.3%- mean hospital stay 1.55 ± 2.3 days (range: 0-23 days)- recurrences 5.4%
Suleyman Bakdik et al Radiol Med 2017
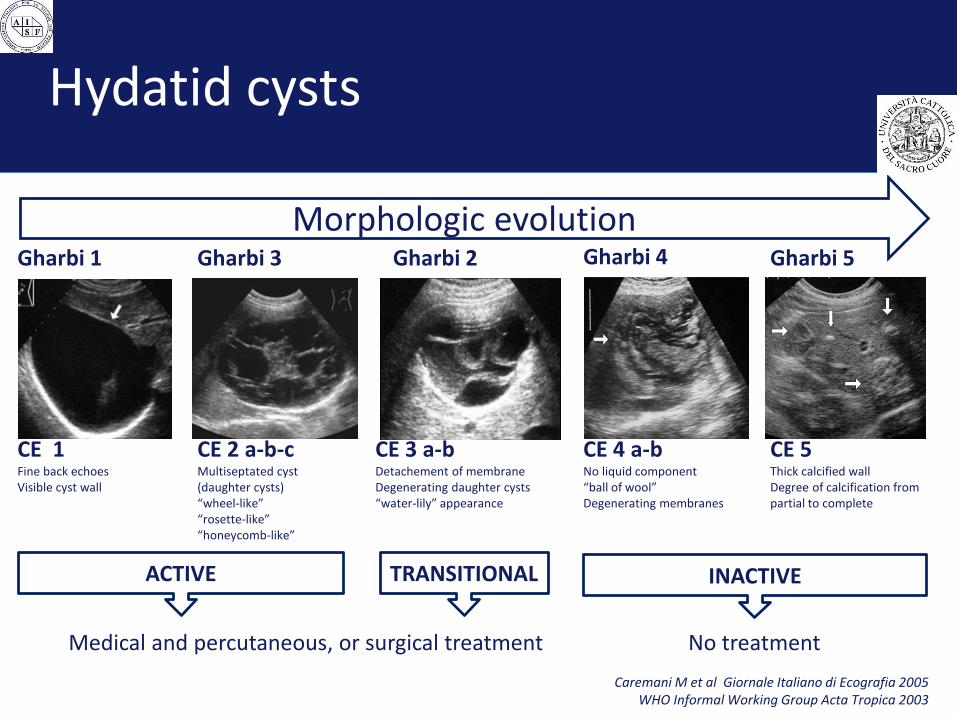
Sclerotherapy
05/2014
• Diagnosis of hepatic cysts (S6)
• CT performed for other reason
• 8.5 cm diameter
10/2014
• Abdominal Pain
• Dimensional increase (+2,5cm)
• Signs of bleeding
• 11 cm diameter
01/2015
• Sclerotherapy
• minocyclinehydrochloride (400 mg)
01/2016
• residual cysts of 2.5 cm
A.S. -female- 78 y.o.

Sclerotherapy
• Abdominal pain and distention
• Diagnosis of hepatic cysts in US and CT
• Max diameter 14.7 cm
• 1 month after sclerotherapy
• minocycline hydrochloride(500mg)
• 6 months after
• residual cysts of 6.4 cm
• (- 92% in vol)
M.B. -female- 52 y.o.

Hepatic abscesses: generalities
• Suppurated cavity caused by the invasion and multiplication of microorganisms within healthy or diseased liverparenchyma
• 2 - 45 cases per 100,000 hospital admissions each year
• Microbes can invade the liver parenchyma by way of the bile ducts, blood stream (hematogenic, most oftenportal), or by contiguous spread, especially via the gallbladder bed
• Incidence of HA seems to increase with age and co-morbidities (diabetes, denutrition, immunosuppression)
• etiology of HA can be bacterial, parasitic (amebic essentially), mixed (pyogenic superinfection of parasiticabscess) or more rarely fungal
• South-East Asia/Africa, amebic contamination is the most frequent cause; Western countries 80% of HA are bacterial
Kuang-Chi L et al Am J Surg 2013

Hepatic abscesses: etiologies
• Biliary disease (cholecystitis, cholangitis)
• Intra-abdominal collections (appendicitis, sigmoid diverticulitis, Crohn’s disease)
• Secondary to pancreatoduodenectomy
• Liver transplantation
• Interventional techniques (radio-frequency ablation, intra-arterial chemo-embolization)
• Liver trauma
• More rarely in the wake of septicemia either on healthy or preexisting liver diseases(biliary cysts, hydatid cyst, cystic or necrotic metastases)

Hepatic abscesses: biliary
• 50-60% of HA
• rarely the presenting complication of cholelithiasis
• cholangitis (biliary obstruction or underlying disease - intrahepatic stones, inflammatory and/or ischemic
cholangitis or Caroli’s disease) biliary obstruction must be resolved (endoscopic sphincterotomy or
percutaneous biliary drainage)
• cholecystitis: contiguous septic spread perforation of an infected gallbladder (< 1%)
Lardiere-Deguelte S et al J Visc Surg 2015

Hepatic abscesses: “non biliary”
• Portal origin (diveritculitis, appendicitis, chronic inflammatory bowel disease) 10-20% of HA
• Arterial origin (Gram-positive: staphylococcus or steptococcus / fungal:Candida albicans / Klebsiella pn.)
• more likely in pateints with co-morbidities such as diabetes or immunosuppression
• Preexisting hepatic disease• Superinfection of biliary cysts < 2%
• Superinfection of primary and metastatic liver malignancy (prognosis less favorable)
• Superinfection of hydatid cysts (fistul. biliary tree)
• Complicating pancreatoduodenectomy• stenosis or obstruction of the hepatic artery
• stricture of the choledocho-enterostomy
• biliary reflux
Lardiere-Deguelte S et al J Visc Surg 2015

Hepatic abscesses: “non biliary”
• After chemo-embolization/radio-frequency ablation (choledocho-enterostomy/history
of sphincterotomy or biliary drainage -ascending colonization-)
• After liver trauma • extent of liver necrosis
• after intra-arterial embolization to con-trol trauma-related hepatic bleeding
• superinfection of a biloma
• Post-transplantation• HA 0.5 - 1%
• mortality can reach 45% (risk of graft loss)
• Risk of HA secondary to ERCP (endoscopic stent placement for strictures or leaks) can attain 26%
• Percutaneous maneuvers (biliary opacification/drainage, liver biopsy) bacteremia 12 times more often in bilio-enterostomy compared with choledocho-choledochostomy
Lardiere-Deguelte S et al J Visc Surg 2015

Hepatic abscesses: mortality
• mortality reaching 15%
• circumstances of onset
• signs of severity related to co-morbidity
• underlying biliary disease
• delays in management
Lardiere-Deguelte S et al J Visc Surg 2015

Hepatic abscesses: treatment
• Antibiotics
• Started promptly, before drainage procedures, to limit the systemiceffects of septicemia
• Less than 3-5 cm, especially when multiple, antibiotics alone, no drainage (no general consensus) 80-100% success rate
• Empirical antibiotic choice/ selection based on culture and sensitivities
• between 2 and 6 weeks
Lardiere-Deguelte S et al J Visc Surg 2015

Hepatic abscesses: percutaneous treatment
• PNA percutaneous needle aspiration
• PCD percutaneous catheter drainage

Hepatic abscesses: percutaneous treatment
PNA
77.8%
=
=
=
low
Success rate
Duration of hospital stay
Procedure-related complications
Days to achieve clinical improvement
Days to achieve a50% reduction in the size of the abscess cavity
Days total or near total resolution of the abscess cavity
Mortality (co-morbidities)
PCD
96.1%
=
=
>
>
=
low
Yu-Long-Cal et al HPB 2014 (meta-analysis 5 RCT)

Hepatic abscesses: percutaneous treatment
PCD > PNA
• number of aspiration attempts (do not limit the number of attempts highest rate of success)
• volume of the abscess
Yu-Long-Cal et al HPB 2014 (meta-analysis 5 RCT)

Hepatic abscesses : PCD
Reported failure rate of primary PCD ranges widely from 0% to 30%(exchange or repositioning of an existing catheter to optimize catheter drainage)
Salvage drainage performed during follow-up if a patient hadsymptoms and imaging confirmed an undrained abscess
Overall success rate > 90%
Haider Steffen J et al AJR 2017
Hepatic abscesses : PCD
Associations With Primary Clinical Failure• unresectable hepatopancreatobiliary malignancy (x 2.4 risk of primary failure: overall
success 79%)
• presence of multiple abscesses (x 2.5 risk of primary failure: overall success > 95%)
• catheter removal despite daily output ≥ 15 mL/d (x 4.1 risk of primary failure: overallsuccess > 95%)
Cavity closure mean of 30 days (>150 ml)
Cavity closure mean of 20 days (<150 ml)Patients with large abscesses needed more catheter adjustments and had longerdrainage duration, but this did not compromise the success rate
Haider Steffen J et al AJR 2017

Hepatic amebic abscesses
• Conservative (Metronidazole)
• Percutaneous needle aspiration
• Percutaneous catheter drainage
• Surgical drainage
Needle aspiration successful in 70%
Catheter drainage successful in 100%
Needle aspiration successful in 80%
Catheter drainage sussessful in 90%
Jha AK et al J Indian Med Assoc 2012
Gupta SS et al ANZ J Surg 2011
Most believe that abscesses of less than 5 cm can be managed medically and abscesses larger than 10cm must undergo ultrasound guided percutaneous needle aspiration along with medical management.
5-10 cm abscesses?percutaneous needle aspiration + metronidazole not superior to metronidazole alone uncomplicated, solitary amoebic liver abscesses of size 5 to 10 cm
Bammigatti c et al Trop Doc 2013

02/09/2013
• Fever
• Abdominal pain
• 6 cm diameter
03/09/2013
• US+Fluo Percutaneous Drainage
• 12 Fr catheter
• No comunication with biliary system
14/09/2013
• 10 days after drainage: catheter removal
20/09/2013
• 6 days after catheter removal
B.R. -male- 40 y.o.
20/10/2013
• 1 month after catheter removal
Hepatic abscesses : PCD

02/03/2008
• Fever
• Abdominal pain
• PCD
14/03/2008
• 12 days after drainage
(Catheter removal after 34 days)
W.W. -male- 35 y.o. chronic pancreatitis + alcoholic cirrhosis
20/05/2010
• 2 years after catheter removal
Hepatic abscesses : PCD

Hepatic abscesses: surgical treatment
• Failed percutaneous drainage
• (Inaccessibility/multilocular abscesses)
• Surgical treatment of the underlying cause of HA

Treatment of abscesses and hepatic cysts
Thank you