TREATMENT NEUROSYPHILIS - Postgraduate Medical...
7
January 1953 C. S. NICOL: The Treatment of Neurosyphilis 27 i. The age incidence is lower. 2. The pouches' are often solitary. 3. The pouches are peculiarly liable to cause acute symptoms. Acute diverticulitis of the caecum, which closely resembles acute appendi- citis in its clinical features, may, in fact, be the first indication of the presence of a pouch. Rarely, chronic inflammation of a diverticulum causes a mass in the right iliac fossa which is liable to be mistaken for cancer and the true nature of which only comes to light after excision. The management of a case of acute diverticulitis revealed at operation undertaken on a diagnosis of acute appendicitis will vary according to the find- ings. There have been cases recorded in which the inflamed diverticulum was readily seen and was excised. In others there is found a mass of inflammatory tissue and the wall of the caecum itself is acutely inflamed. The best procedure for the latter condition is to exteriorize the bowel, with subsequent excision and, finally, closure. This is a protracted and irksome experience for the patient, but there appears to be no alternative. Diverticula of the Appendix Diverticula of the appendix may be demon- strated in about t per cent. of appendices removed at operation. They may be associated with generalized diverticulosis of the colon or may result from disorganization of the appendix mus- culature as a result of chronic fibrosis. They are not in themselves of any notable clinical significance. BIBLIOGRAPHY EDWARDS, H. C. (I939), Diverticula of the Small and Large Intestine, John Wright & Sons, Bristol. KRON, S. D., and SPECTER, J. (I95o), Gastroenterology, is, 62. MAYFIELD, L. H., and WAUGH, J. M. (I949), Ann. Surg., x29, I98. MAYFIELD, L. H., and WAUGH, J. M. (I949), Ibid., 130, i86. ORR, I. M., and RUSSELL, J. Y. W. (i95x), Brit. 7. Surg., 39, I39. WALKER, R. M. (I945), Brit. J. Surg., 32, 457. THE TREATMENT OF NEUROSYPHILIS By C. S. NICOL, M.D., M.R.C.P. Medical Officer in Charge, Special Treatment Centre, St. Bartholomew's Hospital: Assistant Physician. Whitechapel Clinic, London Hospital In a paper dealing with the treatment of neuro- syphilis, it is first necessary to discuss briefly the incidence, clinical classification and natural history of the condition. It is almost certain that 'invasion' of the nervous system by the treponema pallidum occurs during the primary stage of the disease in all cases, but in the majority these organisms do not survive to produce an inflammatory process, thus 'in- volvement ' may occur in 25 to 35 per cent. of cases. This involvement is first manifested by a pleo- cytosis and increased protein content of the spinal fluid in the secondary stage of the disease as demonstrated by the pioneer work of Ravaut (I903). Even after involvement of the nervous system at this stage spontaneous regression occurs in a number of cases so that Bruusgaard's (1929) analysis of patients with untreated syphilis seen many years later, gave a figure of 9.5 per cent. for those with neurosyphilis, while Rosahn's (1946) analysis of autopsy findings in 77 patients with untreated syphilis showed pathological evidence of neurosyphilis in 7.6 per cent. A classification of neurosyphilis is always difficult as the involvement of meninges, vessels and parenchyma never occurs alone, but one or other type usually predominates. I. Early syphilis (within first four years of infection): (a) Asymptomatic neurosyphilis. (b) Acute syphilitic meningitis (may occur in secondary stage or later). 2. Late syphilis (after fourth year of infection): (a) Asymptomatic neurosyphilis. (b) Meningeal syphilis of brain or spinal cord (often termed meningo-vascular as there is also involvement of smaller vessels). (c) Vascular syphilis of brain or spinal cord (involvement of medium-sized vessels). (d) Parenchymatous: (i) General paresis.. (ii) Tabes dorsalis. (iii) Optic atrophy. (e) Gumma of brain or spinal cord. It is important to know something of the natural history of neurosyphilis and realize that reversal copyright. on 23 April 2018 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. Downloaded from
Transcript of TREATMENT NEUROSYPHILIS - Postgraduate Medical...

January 1953 C. S. NICOL: The Treatment of Neurosyphilis 27
i. The age incidence is lower.2. The pouches' are often solitary.3. The pouches are peculiarly liable to cause
acute symptoms. Acute diverticulitis of thecaecum, which closely resembles acute appendi-citis in its clinical features, may, in fact, be thefirst indication of the presence of a pouch. Rarely,chronic inflammation of a diverticulum causes amass in the right iliac fossa which is liable to bemistaken for cancer and the true nature of whichonly comes to light after excision.The management of a case of acute diverticulitis
revealed at operation undertaken on a diagnosis ofacute appendicitis will vary according to the find-ings. There have been cases recorded in whichthe inflamed diverticulum was readily seen andwas excised. In others there is found a mass ofinflammatory tissue and the wall of the caecumitself is acutely inflamed. The best procedure forthe latter condition is to exteriorize the bowel, with
subsequent excision and, finally, closure. This isa protracted and irksome experience for thepatient, but there appears to be no alternative.
Diverticula of the AppendixDiverticula of the appendix may be demon-
strated in about t per cent. of appendices removedat operation. They may be associated withgeneralized diverticulosis of the colon or mayresult from disorganization of the appendix mus-culature as a result of chronic fibrosis. They are notin themselves of any notable clinical significance.
BIBLIOGRAPHYEDWARDS, H. C. (I939), Diverticula of the Small and Large
Intestine, John Wright & Sons, Bristol.KRON, S. D., and SPECTER, J. (I95o), Gastroenterology, is, 62.MAYFIELD, L. H., and WAUGH, J. M. (I949), Ann. Surg.,
x29, I98.MAYFIELD, L. H., and WAUGH, J. M. (I949), Ibid., 130, i86.ORR, I. M., and RUSSELL, J. Y. W. (i95x), Brit. 7. Surg., 39,
I39.WALKER, R. M. (I945), Brit. J. Surg., 32, 457.
THE TREATMENT OF NEUROSYPHILISBy C. S. NICOL, M.D., M.R.C.P.
Medical Officer in Charge, Special Treatment Centre, St. Bartholomew's Hospital:Assistant Physician. Whitechapel Clinic, London Hospital
In a paper dealing with the treatment of neuro-syphilis, it is first necessary to discuss briefly theincidence, clinical classification and natural historyof the condition.
It is almost certain that 'invasion' of thenervous system by the treponema pallidum occursduring the primary stage of the disease in all cases,but in the majority these organisms do not surviveto produce an inflammatory process, thus 'in-volvement ' may occur in 25 to 35 per cent. of cases.This involvement is first manifested by a pleo-cytosis and increased protein content of the spinalfluid in the secondary stage of the disease asdemonstrated by the pioneer work of Ravaut(I903). Even after involvement of the nervoussystem at this stage spontaneous regression occursin a number of cases so that Bruusgaard's (1929)analysis of patients with untreated syphilis seenmany years later, gave a figure of 9.5 per cent. forthose with neurosyphilis, while Rosahn's (1946)analysis of autopsy findings in 77 patients withuntreated syphilis showed pathological evidenceof neurosyphilis in 7.6 per cent.
A classification of neurosyphilis is alwaysdifficult as the involvement of meninges, vesselsand parenchyma never occurs alone, but one orother type usually predominates.
I. Early syphilis (within first four years ofinfection):
(a) Asymptomatic neurosyphilis.(b) Acute syphilitic meningitis (may occur in
secondary stage or later).2. Late syphilis (after fourth year of infection):
(a) Asymptomatic neurosyphilis.(b) Meningeal syphilis of brain or spinal cord
(often termed meningo-vascular as there is alsoinvolvement of smaller vessels).
(c) Vascular syphilis of brain or spinal cord(involvement of medium-sized vessels).
(d) Parenchymatous:(i) General paresis..(ii) Tabes dorsalis.(iii) Optic atrophy.
(e) Gumma of brain or spinal cord.It is important to know something of the natural
history of neurosyphilis and realize that reversal
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

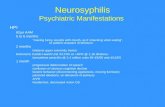
28 POSTGRADUATE MEDICAL JOURNAL January 1953Early, Syphilis Late Syphilis
Asymptomatic Asymptomatic Tabes DorsalisNeurosyphilis- Neurosyphilis
Tabo-paresisAcute Syphilitic Meningeal Syphilis General Paresisx
Meningitis (meningo-vascular) )
of the spinal fluid to normal can occur in bothsymptomatic and asymptomatic conditions. Pro-gression is the rule with involvement of theparenchyma of the brain or spinal cord. This isindicated in Table I.
In considering the curative effect of any drug inneurosyphilis it is most important to realize thatthis is very different in inflammatory (meningeal)and degenerative (parenchymatous) lesions. Theremay be complete resolution of inflammatorylesions with treatment as one sees in asympto-matic and meningo-vascular neurosyphilis, on theother hand if a degenerative lesion predominatesas in tabes dorsalis, signs and symptoms mayremain unchanged.
In some conditions, such as general paresis orErb's spastic paraplegia, both types of lesions maybe present. Gummatous lesions are of the in-flammatory type, while the results of vascularneurosyphilis are mainly degenerative. If thesefacts are realized it is easier to assess the responseto treatment in the various types of neurosyphilis.It is also a general rule that inflammatory lesionsoccur -earlier in the course of the disease thandegenerative lesions, and thus early treatment(ideally in the asymptomatic phase) will give thebest results.
Examination of the cerebro-spinal fluid isessential in neurosyphilis, both in diagnosis andin order to assess the results of treatment. Thisinvolves four tests: (a) the cell count; (b) theestimation of total proteins; (c) the spinal fluidWassermann reaction; (d) Lange's colloidal goldcurve. A test for increase in globulin (Pandytest) is not essential as the colloidal gold test is anindication of the albumen globulin ratio in thespinal fluid.
(a) An increase in the cell count above 3 to 5per cu.mm. is the earliest indication of involvementof the nervous system by the treponema pallidum,and equally it is the first test to revert to normalas a result of treatment.
(b) An increase in the total protein above 40mgm. per cent. follows an increased cell count, andit also is the next test to revert to normal withtreatment.
(c) The Wassermann reaction takes longer tobecome positive and is slow to reverse with treat-ment; it may take several years to revert tonegative. Thus retreatment is not necessarily
indicated if this test remains positive provided thecell count and protein revert to normal. Aquantitative Wassermann test is helpful as itindicates the gradual fall in titre. False positivereactions of the Wassermann test in the spinal fluidare rare, except in the presence of bacterialmeningitis, when the ' reagin ' from the blood maypass through the choroid plexus provided, ofcourse, that the patient already has latent syphilis.
(d) The colloidal gold test parallels the Wasser-mann test in the rate of appearance of abnormalcurves and their modification and reversal tonormal with treatment. Dattner (i944) has em-phasized that the so-called paretic, luetic andmeningitic curves do not necessarily indicate theconditions named. They may all occur inasymptomatic neurosyphilis, and a paretic patientmay have a luetic curve and vice versa. It isprobable, however, that the presence of a pareticcurve in a patient with asymptomatic neuro-syphilis suggests that that patient, if untreated,would develop general paresis. In 1944 Langeand Harris introduced a new method for thecolloidal gold test by which the colour changeswere constant and the numerical value given toeach would be totalled so as to produce a quantita-tive as well as a qualitative test.
Using these basic tests, spinal fluid findings inneurosyphilis are usually classified in three groups.Group I. Cases with abnormal cell count and
total protein with a negative colloidal gold andWassermann test.Group 2. All cases not included in Group I or
Group 3.Group 3. Cases with abnormal cell count and
total protein, positive Wassermann test and aparetic type of colloidal curve.
Dattner Thomas ConceptDattner and Thomas (I942) believe that the
cure of a patient with neurosyphilis is assured ifall the tests in the spinal fluid become and remainnegative. They assume that this indicates resolu-tion of the meningeal inflammatory process andbelieve that while any degenerative process cannotbe reversed, it will not progress. On the otherhand in tabes dorsalis and optic atrophy this is notalways the case.
In contrast to the reversal of an abnormal spinalfluid produced by adequate therapy, the blood
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

January 1953 C. S. NICOL: The Treatment of Neurosyphilis
serological tests (Wassermann and Kahn re-actions) remain positive in the majority of cases.Quantitive tests will demonstrate variations intitre according to certain patterns (Redmond,Nicol and Shooter, I952). ' Seroresistance' isof no prognostic significance and does not indicatefurther treatment of the neurosyphilis.
General Considerations of TherapyBefore the discovery of penicillin, neurosyphilis
was treated with various combinations of neo-arsphenamine, 'bismuth, tryparsamide and fevertherapy (benign tertian malaria or mechanicalfever). Since the introduction of penicillin allare agreed that this is the drug of choice. Thereare still, however, a number of controversialpoints to be decided.
I. The type of penicillin, dosage and duration ofcourse. In most clinics at present the procainesalt of penicillin is used. This saves multiple in-jections and' may be given once daily intra-muscularly in dosage ranging from o.s to I.o megaunit. A course of injections may last for io to15 days, giving a range of from 5.0 to 15.0 megaunits total dosage.
2. The mechanism of the Jarisch Herxheimerreaction and possible means of preventing it.Heyman, Sheldon and Evans (I952) now considerthe Herxheimer reaction to be a hypersensitivityphenomenon of the delayed type. This reaction,as manifested by a rise in rectal temperatureabove 00oo F. following the first injection ofpenicillin, is not uncommon in all types of neuro-syphilis and may occur in about half the cases -ofgeneral paresis treated. It is uncommon, how-ever, to get a severe reaction with exacerbation ofsymptoms or the appearance of new symptoms.In this country the present policy is to give 6 to 12weeks preparatory treatment with intramuscularbismuth (0.2 to 0.4 g. each injection) in the hopeof preventing a reaction. While the resultant delayin giving the penicillin is not important in mostcases of neurosyphilis, it may be thought advisablethat acute syphilitic meningitis or general paresisof acute onset should be treated immediately withpenicillin and the small risk of a serious Herx-heimer reaction accepted. The evidence from thework of Farmer (1948) suggests that giving initialsmall doses of penicillin in no way prevents aHerxheimer reaction, thus when a course ofpenicillin is started initially or after bismuththerapy it may be given in full dosage.
3. The indications for adjuvant fever therapy.In I946 the situation was summarized by Mooreas follows:
Penicillin alone is indicated in early asympto-matic neurosyphilis, meningo-vascular neuro-
syphilis, vascular neurosyphilis and gumma of thebrain and cord.
Penicillin plus fever therapy is indicated ingeneral paresis, tabo paresis, primary opticatrophy, eighth nerve deafness, syphilitic epilepsyand Erb's spastic paraplegia.The best type of fever therapy is induced
malaria, 8 to I2 paroxysms (40o to 6o or more hoursof fever over 104° F.).Hahn (1951) summarizes the present trend as
follows:Although opinions to the contrary are expressed
the consensus appears to be that in all forms -ofneurosyphilis, with the exception of primary opticatrophy, the clinical and spinal fluid results oftreatment with penicillin alone are comparable tothose with penicillin plus fever therapy.
Early Syphilis (First Four Years of Infection)(a) Asymptomatic neurosyphilis. Excellent re-
sults as judged by spinal fluid reversal are obtainedwith penicillin alone. Hahn (I95i) reports Iooper cent. entirely satisfactory of 25 patients treatedby this method.
(b) Acute syphilitic meningitis. Moore (1946)reported on i o cases treated with intramuscularpenicillin in total dosage ranging from 6o0,ooounits to 4,000,000 units given in 71 to i i days.The follow-up was from 287 to 667 days. Theimmediate symptomatic response was dramatic-ally favourable in every case. Headache and stiffneck disappeared in 24 to 48 hours. Cranial nerveparalysis disappeared in all cases except one inwhich a slight residuum remained after 98 days.Of four patients with eighth nerve deafness, oneshowed no improvement (tested by audiometer)after 104 days. Two patients with convulsionshad no further attacks after therapy. Threepatients had mild febrile Herxheimer reactionswithout any -clinical exacerbation. The spinalfluid response was entirely satisfactory at the lastobservation in nine cases, in the tenth case thecells had been reduced from I,450 c.mm. to 9c.mm. 383 days after treatment, other spinal fluidfindings were negative in this case.
In one of the io cases there was a muco-cutaneous relapse 287 days after treatment, whichhad consisted of only 6oo,ooo units of penicillin in71 days.The results reported in this group are dramatic
when the small dosage of penicillin given in somecases is considered. There is every reason toexpect excellent results with present dosageschedules.Late Syphilis (More Than Four Years AfterOriginal Infection)
(a) Asymptomatic neurosyphilis. Penicillin alone
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

30 POSTGRADUATE MEDICAL JOURNAL January I953
is used. Hahn (I95I) reports in I8o cases with94.5 per cent. entirely satisfactory response, 5 percent. unknown and only 0.5 per cent. failure asjudged by spinal fluid examination.
(b) Meningeal syphilis (including Erb's spasticparaplegia). In cases in which there is a pre-dominant meningeal reaction, results with peni-cillin should be adequate except in Erb's paraplegia.Hahn (I95 ) reports results in nine cases ofmeningeal involvement of the brain with cranialnerve lesions (excluding optic atrophy and eighthnerve deafness), II.I per cent. were entirely satis-factory, 44-4 per cent. significantly improved,Ix.x per cent. results unknown and 44-4 per cent.treatment failures. He also reports I8 cases ofspinal cord involvement (including Erb's para-plegia) giving II.I per cent. entirely satisfactory,22.2 per cent. significantly improved, I6.7 per cent.results unknown and 50 per cent. treatmentfailures; when he used malaria in addition topenicillin in three cases there were two failures andone success.
Jones et al. (I95I) in a study of i9 patientswith non-tabetic spinal cord syphilis observed thebest clinical results in five patients with meningomyelitis with a duration of symptoms of less thanfive months. They stated that the outcome inthree patients with Erb's spastic paraplegia orsyphilitic amyotrophic lateral sclerosis was dis-couraging. The duration of symptoms in thesepatients was of more than one year's duration, andthey concluded that considerable degenerativechanges had taken place before the onset oftherapy. The spinal fluid response in all the casesthey reported was comparable to that occurringin other types of neurosyphilis.
(c) Vascular syphilis. Following the occlusionof a medium-sized cerebral or spinal vessel thereis always some degree of myelomalacia. As aresult of this there is usually little clinical responseto therapy.
Jones et al. (I95i) describe six patients withacute transverse myelitis as the result of anteriorspinal artery thrombosis. None obtained com-plete clinical recovery after treatment with peni-cillin. Two of them, however, showed someimprovement in motor function and became am-bulatory in spite of severe spasticity, they also hadfair control of the bladder' and anal sphincters.Two patients showed a poor clinical response withbut slight improvement of motor function. Twopatients showed no recovery and died two monthsand two and a half years after treatment respec-tively.Hahn (I95i) reports the results of penicillin
therapy in 20 patients with cerebral and spinalvascular syphilis, 20 per cent. were entirely satis-factory, 60 per cent. were significantly improved,
in I5 per cent. the results were unknown and 5per cent. were treatment failures.
(d) General paresis. In this condition, whetheroccurring as a single entity or combined with tabesdorsalis (tabo-paresis), there remains a differenceof opinion as to the necessity of fever therapy inaddition to penicillin. Analysis of reported re-sults should be assessed both in relation to spinalfluid reversal and in relation to clinical results interms of the degree of social recuperation. Itmay be interesting to compare clinical resultsobtained by different workers in different countriesin the last few years.
CLINICALLY CURED OR GREATLY IMPROVED(a) Combined penicillin and malaria therapyCurtis, Kruse and Norton (I949) . 42% of 77 casesLereboullet and Brisset (I949) · 50% ,, 31 ,,Nicol and Whelen (I95I) .... 65% ,, I4x ,,Lescher and Richards (I947) .. 66% ,, ,,Hahn (1951) . .. 67% ,, 43 ,,Kopp, Rose and Solomon (1948) .. 67% ,, 446 ,,Kierland, O'Leary and Underwood
(1948) ........ 70% ,, 76 ,,(b) Penicillin therapy aloneCurtis, Kruse and Norton (I949) · · 47% of I55 casesHahn (I95I) .. 55% ,, 70 ,,Lescher and Richards (1947) * 70% ,, ,,Delay, Desclaux and Stevenin (x947) 8o ,, 95 ,,
No biostatistical conclusions can be drawn fromthis type of comparison. Perlo, Rose, Carmenand Solomon (I95I) were able to compare twosimilar groups of patients with advanced simpledementia treated with penicillin only and peni-cillin plus malaria therapy respectively. Theysummarize the results in three tables, which arereproduced overleaf.They concluded that 'clinical results with
penicillin alone proved slightly more favourablethan those obtained with combined therapy.'
It must be remembered that malarial therapynecessitates admission to a special hospital withskilled medical and nursing care, as there arerisks of grave complications and fatalities havebeen reported. Such a centre exists in thiscountry-The Mott Clinic, Epsom.
Penicillin therapy gives varying results accord-ing to the type of psychosis present in paresis.Kopp, Rose and Solomon (1948) report 85 percent. improvement in patients with slight psychicdisturbances, 66 per cent. improvement in affectivedementia, but only 25 per cent. improvement inpatients with a paranoid psychosis.
Bruetsch considers that total dosage of peni-cillin in paresis should be more than Io mega units,as he found treponema pallidum still present in thecerebral cortex of patients who came to autopsyafter having received this dosage.
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

January 1953 C. S. NICOL: The Treatment of Neurosyphilis 3'
122 PATIENTS WITH ADVANCED SIMPLE DEMENTIA(after Perlo, Rose, Carmen and Solomon)
CLINICAL STATUSImproved Arrested Worse
Penicillin alone, 30 patients .... I9 (63%) 8 (27%) 3 (Io%)Combined therapy, 92 patients .... 48 (52%) 25 (27%) I9 (21%)
SOCIAL ADJUSTMENTGood Fair Poor Not known
Penicillin alone, 30 patients . 5 (7%) 9 (30%) I. (50%) I (3%)Combined therapy, 92 patients .. 13 (I4%) 26 (28%) 48 (52%) 5 (6%)
WoRK LEVELWorking Not Working Hospitalized
Penicillin alone, 30 patients....
II (37%) 6 (20%) I3 (43%)Combined therapy, 92 patients .... 38 (41%) x6 (I8%) 38 (41%)
Lastly, there is the problem of the Herxheimerreaction in patients with paresis. Heyman,Sheldon and Evans (95z2) reported this in 23 (52per cent.) of 44 patients with paresis. Six of these23 patients showed a transient intensification oftheir psychotic manifestations. Putkonen andRehtijarvi (1950) studied the Herxheimer reactionin 223 patients with neurosyphilis. All 21 patientsin this series with paresis previously untreatedshowed a febrile response. They stated thatprevious therapy with arsenic and/or bismuthseemed to reduce this to some extent, while pre-vious malarial or penicillin treatment made thereaction impossible. They also stated that themore active was the spinal fluid the more likelywas the febrile response to occur. It usually tookplace 12 to I6 hours after the first injection ofpenicillin. They did not experience any seriousclinical exacerbations. In a few patients there wasincreased confusion during the febrile responseand in one patient who had previously had fits, afurther convulsion occurred at the fever peak.Lereboullet and Sapin Jalloustre (x947) record apatient with paresis who died in status epilepticusafter penicillin therapy had been begun and theauthor has seen a similar case.
(e) Tabes dorsalis. In this condition the problemagain arises as to whether penicillin therapy aloneis adequate. Hahn (I95I) tabulates the results in70 patients treated with penicillin and 31 withpenicillin and malaria. The results in the firstgroup were 41.4 per cent. entirely satisfactory,I8.6 per cent. significantly improved, II.4 percent. results unknown and 28.6 per cent. treatmentfailures. In the second group there were 48.4 percent. entirely satisfactory, I9.4 per cent. signifi-cantly improved, I2.9 per cent. results unknownand I9.4 per cent. treatment failures. He con-
cludes the effects of penicillin plus malaria therapyon tabetic symptoms are essentially the same asthose of penicillin alone. Asjudged also by overallclinical results the addition of malaria therapyaffords no definite benefit. He also states that in afew patients development or progression of symp-toms occurs after treatment. Koteen (1949) re-ported on 403 patients with tabes including 49treated with penicillin alone. There was im-provement of symptoms and signs such as im-potence (40 per cent.), ataxia (54 per cent.),lightening pains (50 per cent.), urinary com-plications (33 per cent.) and paresthesiae (66 percent.) as indicated. Gastric and other crises,pupillary abnormalities and deep sensibility dis-orders remained unaffected. The appearance of anew clinical sign such as a Charcot's joint mightoccur after treatment. Herxheimer reactions areuncommon in tabes according to Putkonen andRehtijarvi (1950).
(f) Optic atrophy. This serious complication isoften associated with tabes dorsalis. If un-treated the patient may become blind in three tofive years from the onset of symptoms, but theprogression of the condition is very variable. Onemust emphasize the importance of early diagnosisby the examination of the optic discs, visual acuityand visual fields (the earliest change). Klauderand Gross (1949) reported in 56 patients givenpenicillin and malarial therapy, that there were32 stabilizations, io aggravations and eight becameblind. Hahn (195i) reported progression in six of17 patients with primary optic atrophy after treat-ment with penicillin alone, and in three of i6 aftertreatment with penicillin plus malaria. Blindnessoccurred in four of the former and two of the lattergroup. The total period of observation in bothgroups was only 15 months. Similar types of
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

32 POSTGRADUATE MEDICAL JOURNAL January 1953
patient composed both treatment groups. Heconcludes that penicillin alone cannot yet beevaluated, and penicillin plus malaria remains thetreatment of choice.
(g) Gumma of brain or cord. This condition is aclinical rarity and may only be diagnosed at opera-tion as in the case of a gumma of the cord describedby Thompson and Preston (I950); their case re-ponded favourably to penicillin therapy. It hasbeen stated in the past that a serious clinicalHerxheimer reaction might occur, especially if thelesion were in the brain below the tentorium cere-belli and that a pressure cone of the medulla mightresult in a fatality. Premedication with bismuthshould always be given as a prophylaxis against thisevent.
Spinal Fluid RelapseDattner (I949) reported on the spinal fluid out-
come of 388 patients with various types of neuro-syphilis observed for 6 to 56 months, and recordedonly 43 failures to a first course of penicillin. Ofthese 43 patients, 24 responded favourably to asecond course of higher dosage, of the other I9failures only three showed a continuous active pro-cess indicated by persistent abnormal cell countand protein. In I95o Dattner reported concern-ing further treatment of these three patients (allcases of asymptomatic neurosyphilis). Two hadreached an inactive state following treatment withfour courses of penicillin totalling 49.8 and 59mega units respectively. The third case had notbeen followed long enough to evaluate treatment.In Hahn's (I95I) whole series of 589 patients withall types of neurosyphilis, the spinal fluid relapserate was I.25 per cent. for the penicillin group and0.93 per cent. for the penicillin plus malaria group.These relapses only occurred in patients whoseinitial spinal fluid contained io or more cells andwho received less than 5 mega. units of penicillin.No patient suffered more than one spinal fluidrelapse.Antibiotics Other Than PenicillinThere is as yet no evidence that these prepara-
tions are more efficient than penicillin in the treat-ment of syphilis, and they remain considerablymore expensive. They have been used experi-mentally for the treatment of neurosyphilis in alimited number of cases. Kierland and O'Leary'I950) treated I2 patients with neurosyphilis bygiving oral aureomycin and reported satisfactoryclinical and spinal fluid reversal. Romansky et al.(I95) treated five patients who had neurosyphiliswith chloramphenicol for i5 days. They reportedreversal of abnormal spinal fluid cell counts. Therewas no clinical improvement in a case of tabesdorsalis or in a case of optic atrophy. Robinson
(I952) mentioned an investigation which he wasundertaking with Mohr to study the effect ofaureomycin and chloramphenicol in I patientswith late asymptomatic neurosyphilis (Group 3spinal fluid changes). The dosage given for bothdrugs was 6o g. in 15 days. In a graph he showedthe return to normal of spinal fluid cell counts inI8o days with a slow improvement in the colloidalgold curve. The total protein and complementfixation test remained essentially unchanged duringthis time. He concluded that the treatment ofchoice for neurosyphilis remained procaine peni-cillin, 600,000 units daily or every other day to anapproximate total of io million units.
SummaryI. In a summary of the present status of treat-
ment in the various types of neurosyphilis therecent literature concerning clinical and spinalfluid results has been reviewed.
2. Penicillin appears to be the drug of choice forneurosyphilis; the newer antibiotics have not beenproved more effective.The total amount of penicillin given should not
be less than 6 mega units administered in not lessthan io days. Dosage up to 15 mega units in I5days is employed in many clinics. The procainesalt of penicillin is generally used with an injectiongiven intramuscularly once in every 24 hours.This makes ambulatory treatment possible.
3. Penicillin alone will give as satisfactory spinalfluid reversal and clinical outcome as when com-bined with malarial therapy except in optic atrophy.
4. Where malaria therapy is indicated thepatient should be sent, if possible, to a specialcentre where expert medical and nursing care willreduce the risk of a fatality to a minimum.
5. Spinal fluid relapse rate is low with penicillintherapy and retreatment with a larger dosage isusually successful.
6. The Jarisch-Herxheimer reaction as mani-fested by a febrile response is not uncommonespecially in general paresis, but serious newclinical symptoms or exacerbation of existingsymptoms are rare. In this country, however, itis still considered prudent to give 6 to I2 weekspreparatory treatment with intramuscular bismuthbefore the administration of penicillin in caseswhere there is no urgency. In cases of acutesyphilitic meningitis or in general paresis of acuteonset it may be considered best to give penicillininitially accepting the risk of a clinical Herxheimerreaction.
7. Giving penicillin in initial small dosage,which is gradually increased, in no way modifiesthe incidence or severity of a Herxheimer reaction.Thus when penicillin is administered for neuro-syphilis it may be given in full dosage.
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from

January 1953 A. W. LIPMANN KESSEL: Fractures Around the Elbow Joint 33
BIBLIOGRAPHYBRUUSGAARD, E. (I929), Arch. f. Derm. u. Syph., 157, 309.CURTIS, A. C., KRUSE, W. T., and NORTON, D. H. (I949),
Am. J. of Syph. Gonor. &f Ven. Dis., 33, 527.DATTNER, B. (I944), 'The Management of Neurosyphilis,'
Grune & Stratton, New York.DATTNER, B. (1949), Am. Y. Syph. Gonor. & Ven. Dis., 33, 571.DATTNER, B. (I950), Am. Y. Syph. Gonor. & Ven. Dis., 34, 373.DATTNER, B., and THOMAS, E. W. (I942), Am. J. Syph. Gonor.
& Ven. Dis., 26, 21.DELAY, DESCLAUX and STEVENIN (I947), Rev. Neur.,
July, 515.FARMER, T. W. (I948), Y.A.M.A., 138, 48.HAHN, R. D. with assistance of LEWIS, B., WIGGALL, R. H.,
and CROSS, E. S. (x95s), Am. Y. Syph. Gonor.& Ven. Dis.,35, 433-
HEYMAN, A., SHELDON, W. A., and EVANS, L. D. (1952),Brit. J. Ven. Dis., 28, 50.
JONES, R. W., HEYMAN, A., SMITH, W. A., and WILSON, R.(x95I), Am. Y. Syph. Gonor. & Ven. Dis., 35, 72.
KIERLAND, R. R., and O'LEARY, P. A. (I950), Am. J. Syph.Gonor. & Ven. Dis., 34, 443.
KIERLAND, R. R., O'LEARY, P. A., and UNDERWOOD,L. J. (I948), Am. Y. Syph. Gonor. & Ven. Dis., 32, 470.
KLAUDER,J. V., and GROSS, B. A. (x949), Am. . Syph. Gonor.& Ven. Dis., 33, 234.
KOPP, T., ROSE, A. S., and SOLOMON, H. C. (1948), Am. J.Syph. Gonor. & Ven. Dis., 32, 509.
KOTEEN, H. (i949), Am. J. Syph. Gonor. & Ven. Dis., 33, 364.LANGE, C., and HARRIS, A. H. (i944), Am. _. Pub. Health,
34, 1087.LEREBOULLET, ]., and BRISSET (I949), Rev. Neur., 8, 646.LEREBOULLET, J., and JALLOUSTRE, S. (I947), Bull. Soc.
Med. Hop., 26, 775.LESCHER, G., and RICHARDS (x947), Brit. Med. J., ii, 565.MOORE, J. E. (1946), 'Penicillin in Syphilis,' Blackwell, Oxford.NICOL, W. D., and WHELEN, M. (I9s5), Brit. J. Ven. Dis.,
27, 132.PERLO, V. P., ROSE, A. S., CARMEN, L. R., and SOLOMON,
H. C. (i95x), Am. J. Syph. Gonor. & Ven. 12is., 35, 559-PUTKONEN, T., and REHTIJARVI, K. (I95i), Acta. Dermat-
Venereol., 31, 120.RAVAUT, P. A. (I903), An. de Dermat et Syph., 4, 537.REDMOND, A., NICOL, C. S., and SHOOTER, R. A. (1952),
Brit. J. Ven. Dis., 28, 13.ROBINSON, R. C. V. (I952), Brit. J. Ven. Dis., 28, 8o.ROMANSKY, M. J., OLANSKY, S., TAGGART, S. R., LAWD-
MAN, G. S., and ROBIN, E. D. (I95I), Am. J. Syph. Gonor.& Ven. Dis., 35, 234.
ROSAHN, P. (1946), gournal of V.D. Information Supplement 21.THOMPSON, R. G., and PRESTON, R. H. (I950), Am. J. Syph.
Gonor. & Ven. Dis., 34, 356.
VFRACTURES AROUND THE ELBOW JOINT
IN CHILDRENBy A. W. LIPMANN KESSEL
London
The swings and slides of public parks provideour hospitals with a regular week-end clientele ofsmall boys who have sustained fractures about theelbow joint. The diagnosis of many such frac-tures calls for nice judgment and a meticulousattention to the general principles as well as thedetails of treatment. The I935 Report of theB.M.A. Committee on Fractures did not analyzefractures in children, but if it is true that theaverage incapacity period for a simple fracture ofthe clavicle in adults who were not treated in anorganized clinic was 22 weeks, as compared to fiveweeks for those treated in organized clinics, itwould be a fair assumption that a similar analysisfor the group of more serious and difficult fractureswe are now considering would reveal an evengreater difference.
Diagnosis and classification. The precise diag-nosis of the type of fracture is essential, but byno means always easy because of the complexityof the ossification of the lower end of the growinghumerus. Leaving aside for the moment thequestion of soft tissue damage, this group offractures may be broadly classified into five radio-logical types. Intermediate as well as complextypes will, of course, occur. In cases of doubt the
opposite elbow must always be X-rayed forcomparison:
Supracondylar fractures-extension and flexionvarieties.
Transcondylar-simple and' T '-shaped.Epicondylar avulsion, with or without disloca-
tion.Fracture-separation of the external condyle
epiphysis.Fracture of the head or neck of the radius.Treatment. Each type of fracture will be con-
sidered separately, but there are certain generalprinciples applicable to the treatment of all thesefractures.
I. Manipulative reduction must always begentle. Only too often does a complication arisefrom the violence of attempted reduction ratherthan from the original injury itself.
2. Wherever possible a 'single attack' shouldbe made to achieve reduction by closed manipula-tion. It should be carried out under generalanaesthesia with X-ray control (not screening), andthe several attempts that may be necessary toachieve satisfactory alignment should be carriedout at the same session. An examination of someof the disasters which have occurred shows only
copyright. on 23 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.327.27 on 1 January 1953. D
ownloaded from