Psychiatry -Delirium, Dementia and Amnestic Disorders (Dr.sundiang)
Upload
victor-curtisCategory
view
216download
2
Treatment for Substance Use Disorders
and Co-Occurring MH Disorders:New Initiatives in the VA
James R. McKay, Ph.D.
Professor of Psychology in PsychiatryUniversity of Pennsylvania
Center of Excellence in Substance Abuse Treatment and Education
Philadelphia VA CESATE

Outline of the Presentation
• Treatment for substance use disorders (SUD) in the VA– Practice guidelines
– Evidence-based behavioral and pharmacological treatments
• Treatment for co-occurring SUD and PTSD– Numbers
– Practice guidelines
– Most recent research
• Treatment for co-occurring SUD and depression
• New initiatives to reorganize MH treatment in VA
• Examples of major rollouts of EBT for SUD in VA

Treatment

Uniform Services Handbookand
Practice Guidelines

Purpose of the Handbook
• Describe levels of care within VA system
• Specify SUD treatments that VA programs must be able to offer veterans
• Define the required features of programs at different levels in the continuum, including staffing, duration of care, and case loads
• Define standards for access

Practice Guidelines
• Provide step-by-step directions, presented in clinical algorithms, for every type of SUD treatment– Detoxifiation– Assessment and treatment planning– Residential treatment– Outpatient treatment– pharmacotherapy

MH screening in the VA
• All patients are screened once per year for alcohol problems, PTSD, and depression
• Vets who come up positive are supposed to be referred to either a brief intervention or to SUD/MH specialty care
• In practice, less than 50% of vets with a positive alcohol screen are referred
• Referral rates are higher for those with positive PTSD or depression screen
Evidence-Based Treatments for SUD:
Large-Scale Training Initiatives in the VA
Cognitive-Behavioral Therapy(CBT)
• CBT focuses on changing cognitions and behaviors thought to increase vulnerability to relapse– Cognitions:
• All or nothing thinking • Catastrophic thinking• Attributional biases
– Behaviors:• Spending time with other substance users• Going to “high risk” locations • Interpersonal conflict• Unstructured time
Contingency Management
• Provides rewards for drug negative urine samples or attendance at sessions
• Requires patient to provide urine samples 2-3x/week, and rapid analysis of samples
• Amount of reward can escalate with serial success and reset to lower amounts if substance use occurs
• Probably our most effective treatment for stimulant dependence

Motivational Enhancement Therapy • Many individuals with SUD are not ready for
abstinence oriented treatment• MET is designed to help people with SUD who are
relatively unmotivated • Techniques
– Compare patient’s substance use to normative data – Roll with resistance (non-confrontational)– Open ended questions combined with reflective listening– Express Empathy– Develop Discrepancies between behavior and goals
• Usually done in 3-4 sessions

Medications for the Treatment of SUD

Medications Approved in the US to Treat Alcohol Dependence
• Disulfiram (Antabuse): 1949
• Naltrexone (ReVia): 1994
• Acamprosate (Campral): 2004
• Long-acting Naltrexone (Vivitrol): 2006

Opiate Addiction
• Two agonist medications are effective for opiate dependence:– Methadone (dispensed daily in programs)
– Buprenorphine (can be dispensed by private physician in office)
• The antagonist medication naltrexone is highly effective, but very underused
• All must be used as long-term, maintenance medications in order to be effective

Are these meds used in the VA?
• Medications to reduce alcohol use:– Less than 10% of patients who might benefit
from these meds receive them– Reasons for low rate are being explored in a
number of research studies
• Medications to treat opiate use disorders– VA provides both methadone and
buprenorphine

Treatment of Co-Occurring PTSD and SUD
Epidemiology

VETERANS HEALTH ADMINISTRATION
Fiscal Year (FY) 2008 Prevalence of Co-Occurring Conditions in Veterans Seeking Treatment in Veterans Health Administration
(VHA)
PTSDN=351,708
Major Depressive Disorder
Schizophrenia Bipolar
SUDN=387,807
MDD & SUD23%
PTSD & SUD23%
N=80,588
Sch & SUD26%
BP & SUD33%

VETERANS HEALTH ADMINISTRATION
Fiscal Year (FY) 2013 Prevalence of Co-Occurring Conditions in Veterans Seeking Treatment in Veterans Health Administration
(VHA)
PTSDN=535,506 (up 52%)
Major Depressive Disorder (MDD)
Schizophrenia Bipolar(BP)
SUDN=516,095 (up 33%)
PTSD & SUD26.5%
N=142,163 (up 76%)

VETERANS HEALTH ADMINISTRATION
Mental Disorders1 among Veterans2
Returning from DeploymentCumulative from 1st Quarter FY 2002 through 1st Quarter FY 2014
Disease Category (ICD 9 code)Total O/O/O Veterans3
Change Q1FY11-FY12
Change since Q1FY12-FY13
Change since Q1FY13-FY14
PTSD (309.81) 311,688 22.5% 20.7% 19.0%
Depressive Disorders (311) 248,891 26.4% 24.5% 21.3%
Neurotic Disorders (300) 229,361 29.5% 27.4% 26.1%
Tobacco Use Disorder (305.1) 183,054 21.5% 19.7% 17.0%
Affective Psychoses (296) 152,587 27.7% 23.9% 23.2%
Alcohol Abuse (305.0) 73,029 26.6% 23.0% 19.2%
Alcohol Dependence (303) 72,055 29.8% 26.4% 22.0%
Drug Abuse (305.2-9) 53,839 33.7% 29.4% 26.4%
Drug Dependence (304) 40,630 34.7% 31.0% 26.3%
20
1 Includes provisional and confirmed diagnoses. http://www.publichealth.va.gov/epidemiology/reports/oefoifond/health-care-utilization/ 2 These are cumulative administrative data since FY 2002. 3 A total of 572,569 unique patients received one or more diagnoses of a possible mental disorder.
VETERANS HEALTH ADMINISTRATION
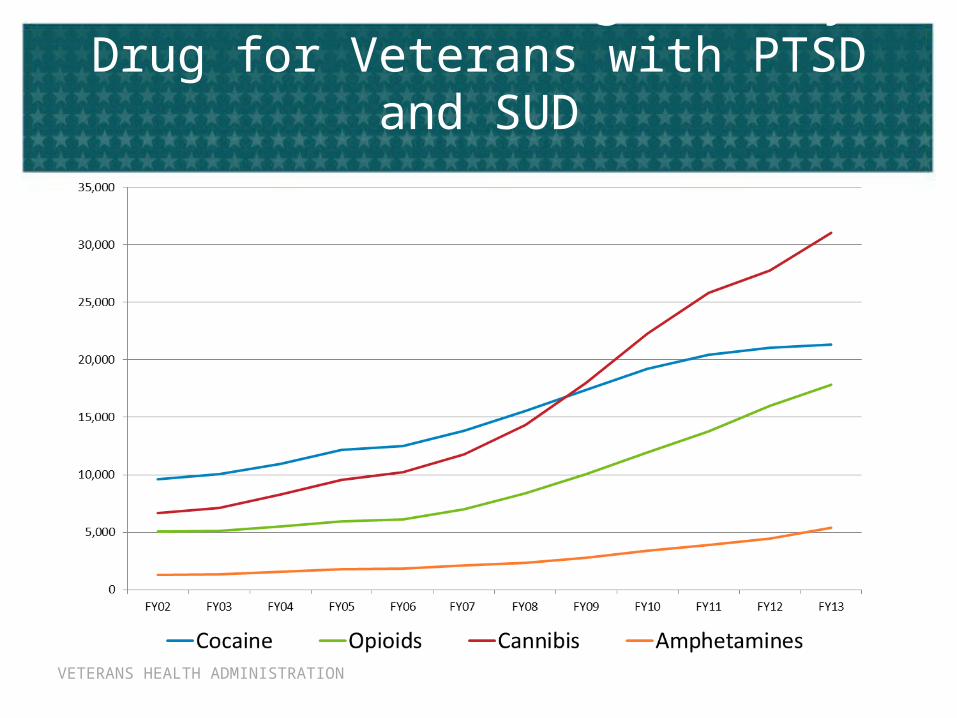
VHA Trends in Diagnoses by Drug for Veterans with PTSD and SUD

PTSD-SUD Treatment in the VA
VETERANS HEALTH ADMINISTRATION
Summary of VA/DoD PTSD Guideline Recommendations for Co-occurring
SUD
1. All patients diagnosed with PTSD should receive comprehensive assessment for SUD, including nicotine dependence
2. Recommend and offer cessation treatment to patients with nicotine dependence
3. Patients with SUD and PTSD should be educated about the relationships between PTSD and substance abuse. The patient’s prior treatment experience and preference should be considered since no single intervention approach for the co-morbidity has yet emerged as the treatment of choice.

VETERANS HEALTH ADMINISTRATION
Summary of VA/DoD PTSD Guideline Recommendations for Co-occurring
SUD
4. Treat other concurrent substance use disorders consistent with VA/DoD clinical practice guidelines for SUD including concurrent pharmacotherapy:a. Addiction-focused pharmacotherapy should be discussed, considered, available and offered, if indicated, for all patients with alcohol dependence and/or opioid dependenceb. Once initiated, addiction-focused pharmacotherapy should be monitored for adherence and treatment response.
Ravelski, Olivera-Figueroa & Petrakis (2014). PTSD and comorbid AUD: a review of pharmacological and alternative treatment options. Substance Abuse and Rehabilitation, 5, 25-36 http://dx.doi.org/10.2147/SAR.S37399
VETERANS HEALTH ADMINISTRATION
Summary of VA/DoD PTSD Guideline Recommendations for Co-occurring
SUD
5. Provide multiple services in the most accessible setting to promote engagement and coordination of care for both conditions.
6. Reassess response to treatment for SUD periodically and systematically, using standardized and valid self report instrument(s) and laboratory tests. Indicators of SUD treatment response include ongoing substance use, craving, side effects of medication, emerging symptoms, etc.
7. There is insufficient evidence to recommend for or against any specific psychosocial approach to addressing PTSD that is co-morbid with SUD.

Recent Research Findings

VETERANS HEALTH ADMINISTRATION
Cochrane Report on PTSD/SUD Treatment
- Roberts, Roberts, Jones, Bisson
Roberts NP, Roberts PA, Jones N, Bisson JI. Psychological interventions for post-traumatic stress disorder and comorbid substance use disorder. Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD010204. DOI: 10.1002/14651858.CD010204.pub2. Submitted for publication
• Searched up to Jan 10, 2014• RCT’s of individual or group psychotherapy with
PTSD/SUD participants, compared with waiting list, usual care, or other psychotherapy
• 14 studies included• Meta-analysis with over 1400 participants total

VETERANS HEALTH ADMINISTRATION
Cochrane Review Results
• Main comparison was CBT with trauma processing v. CBT without trauma focus (coping skills)
• Overall quality of evidence was low to very low – i.e., future research very likely to change estimate of effect

VETERANS HEALTH ADMINISTRATION
Results: Individual Trauma Focused
Interventionsw/Concurrent or Integrated SUD
Treatment
• PTSD symptoms– More effective than TAU or minimal intervention in
reduction in symptoms at post-treatment and follow-up
• Substance use– No effects at post-treatment, but more effective than
comparison conditions at 5-7 month follow-up
• Higher drop out rate than TAU

VETERANS HEALTH ADMINISTRATION
Results: Non-Trauma Focused Interventions
• Most studies looked at group-based interventions• No positive effect on PTSD symptoms or SUD
compared to TAU• Full course Seeking Safety more effective at end of
treatment than TAU, but not at follow-up• Drop out rate comparable to TAU
VETERANS HEALTH ADMINISTRATION
Other Findings
• High drop out rate across all studies• Review based on small number of studies, some
small or poorly designed• Need for further study given low to very low quality
of research• Need to interpret results with caution

VETERANS HEALTH ADMINISTRATION
Results
• Naltrexone produced better alcohol use outcomes than placebo (mean difference = -7.93 % days drinking)
• No significant effect for either naltrexone or prolonged exposure on PTSD outcomes
• Authors note that PE did not worsen drinking outcomes• Low PTSD severity <10 on PSS (exploratory analysis)
– 70% PE + nalrexone– 55% PE + placebo– 44% supportive + naltrexone– 37% supportive + placebo
33

VETERANS HEALTH ADMINISTRATION
Considerations
• Excluded substance dependence except for nicotine and cannabis
• Excluded for opiate use in past month prior to study entry
• Required abstinence prior to study participation


VETERANS HEALTH ADMINISTRATION
Design and Results
• Design– COPE (PE + CBT/RP) compared to TAU– 103 participants with PTSD and SUD dx– Followed for 9 months
• Results– COPE produced greater reductions in PTSD symptom
severity than TAU (mean difference -16.1)– No differences in substance use outcomes

VETERANS HEALTH ADMINISTRATION
Considerations
• Most participants polysubstance users– Median = 4 substances in past month
• The most common main drugs of concern were heroin (21%), cannabis (19%), amphetamines (17%), benzodiazepines (15%), alcohol (11%), cocaine (6%)
• Only 54% of COPE-assigned participants attended sessions with exposure– Most who did only attended one or two sessions
• Treatment took close to a year for some participants


VETERANS HEALTH ADMINISTRATION
Kaysen et al., 2014
• Method– Chart review of 536 Veterans receiving at least one
session of Cognitive Processing Therapy (CPT)– 90% male
• Looked at outcomes in three groups:– Current AUD (11% of sample)– Lifetime but not current AUD (39% of sample)– No AUD (50% of sample)
VETERANS HEALTH ADMINISTRATION
Results
• Comparable drop out rates in all 3 groups (m = 9 CPT sessions attended)
• Comparable symptom improvement in all 3 groups• Decrease in PTSD symptoms by all groups• Decrease in MDD symptoms by all groups

VETERANS HEALTH ADMINISTRATION
Considerations
• Chart review• No randomization• No alcohol use outcomes• No follow up
• But…– First study showing CPT works as well in those with AUD as
in those without AUD

VETERANS HEALTH ADMINISTRATION
Where Are We Now?
• Nothing to contradict PTSD Clinical Practice Guideline recommendations
• Treatment for alcohol use disorder or other SUD together with PTSD treatment
• Trauma focused (evidence based) PTSD treatments are tolerable and perform as well or better than other treatments
VETERANS HEALTH ADMINISTRATION
What do Vets Want?
• Pilot study by Back et al. (2014) looked at the treatment preferences of 35 veterans with SUD and PTSD
• Perceptions of SUD and PTSD– 94% perceived a relationship between SUD and PTSD symptoms– 85% perceived that increased PTSD symptoms led to increased SUD– 62% believed that improvement led to decrease in substance use
• Preferred sequence of treatments:– Integrated SUD/PTSD treatment: 66%– Treat SUD first: 20%– Treat PTSD first: 9%
43

Treatment of Co-Occurring SUD and Depression

New CBT-Based Interventions
• Building Recovery by Improving Goals, Habits, and Thoughts (BRIGHT)– Group based CBT for SUD patients with
depression– Delivered by SUD counselors, with little or no
formal training in mental health care– Well-suited to the VA, given reliance on group
counseling

Initial Research• Watkins et al. (2012)
– Quasi-experimental study compared residential TX to same plus BRIGHT groups
– Participants had SUD + major depression
– Results:• 3 months: Positive effect for BRIGHT over TAU on BDI
(p< .01) and SF-12 (p< .05)
• 6 months: Positive effect for BRIGHT over TAU on BDI (p= .08) and SF-12 (p< .05)
• Also, fewer days of substance use problems in BRIGHT, but no effect on alcohol use
Training Counselors to Provide BRIGHT
• VA Study (G. Curran, PI)• Developed a web-based, interactive training
program plus weekly telephone supervision• If successful, could replace more costly and time
consuming in-person training protocols• Pilot study produced very encouraging results• Three training products are now available on
TMS, and are being used by providers

Reorganization of VA SUD Services

Where services are provided
• Specialty SUD programs– Drug free– Opiate maintenance
• Behavioral Health Integrated Programs (BHIP)– panel model
• Primary care-based integrated teams

Where all this is going
• Greater management of SUD patients in BHIP or primary care programs
• Referral to SUD specialty care for more severe patients and those who keep relapsing
• Idea is to stabilize patient in SUD specialty care, and refer back to BHIP or primary care team.
VETERANS HEALTH ADMINISTRATION
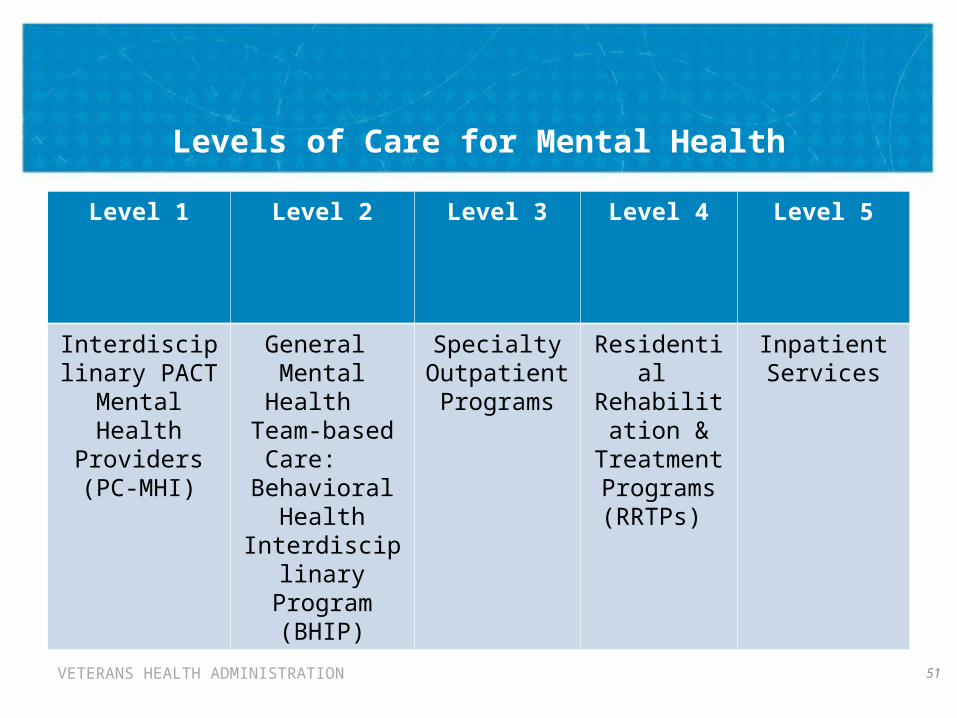
Levels of Care for Mental Health
51
Level 1 Level 2 Level 3 Level 4 Level 5
Interdisciplinary PACT Mental
Health Providers (PC-MHI)
General Mental Health
Team-based Care:
Behavioral Health
Interdisciplinary Program (BHIP)
Specialty Outpatient Programs
Residential Rehabilitation & Treatment
Programs (RRTPs)
Inpatient Services

VETERANS HEALTH ADMINISTRATION
The Behavioral Interdisciplinary Health Program (BHIP) Team
• What is a GMH team (BHIP team)?– Interdisciplinary team of mental health providers– Manages a specific panel of Veterans– Administrative support– Tracking patient visits and measures over time
• Each facility to develop one BHIP teamaccording to OMHO staffing model
VETERANS HEALTH ADMINISTRATION
Outpatient General Mental Health Staffing Model:
Behavioral Health Interdisciplinary Program (BHIP) Team Pilots
• This preliminary model is being piloted in VISNs 1, 4, 17, and 22. Teams with the staffing model clinical ratios have been launched, and it is expected that team size and panel composition may change over time with feedback from the pilots.
• The overarching goal for this staffing model is to build interdisciplinary teams who will provide the majority of mental health care necessary for a panel of assigned Veterans and thus open access to mental health care for all eligible Veterans.
• Teams leverage the expertise of individual members to provide recovery-oriented, evidence-based treatments for all mental health issues presented by Veterans.
• Adjustments will be made to the model and team formation on an ongoing basis as new data is obtained.
53

VETERANS HEALTH ADMINISTRATION
Mental Health Services Before and After BHIP Team Rollout
Before
Some providers may be practicing individually in discipline-specific or specialty-specific silos
Some providers may not be practicing at the top of their license/scope of practice
Clerical support varies widely across the system
Often there is limited or no dedicated time for indirect patient care activities
54
After
Interdisciplinary, team-based care
Practicing closer to top of license/scope
More consistent clerical support for teams
Dedicated time for indirect patient care activities

Initiatives in the VA to Disseminate Evidence-Based
Interventions:
Measurement-Based CareContingency Management

A 17-item measure of addiction problem severity that is designed to support measurement-based care (MBC) in SUD specialty care settings.
Retrospectively examines the patient's behavior in the past 30-
days.
Item selection based on research on predictors of relapse and outcome
Initial psychometric evaluation indicates the BAM items are reliable and sensitive to change (Cacciola et al., 2013).
Cacciola, J. S., Alterman, A. I., DePhilippis, D., Drapkin,M., Valades, C., Fala, N., et al. (2013). Development and initial evaluation of the Brief Addiction Monitor (BAM). Journal of Substance Abuse Treatment, 44, 256–263, http://dx.doi.org/10.1016/j.jsat.2012.07.013.

Substance Use Risk Factors Protective Factors
Any alcohol use Craving Self-efficacy
Heavy alcohol use Sleep problems Self-help
Drug use Mood Religion/spirituality
Risky situations Work, school
Family/social problems
Income
Physical health Social supports for recovery

The MBC perspective: The baseline data and feedback inform initial
treatment planning. The follow-up data and feedback inform treatment
changes. Follow-up BAMs also may be used in the context of
outreach to out-of-treatment veterans.
The POLICY perspective (MH Handbook): (k) Patients with substance use illness need to be
offered long-term management for substance use illness and any other coexisting psychiatric and general medical conditions. The patient's condition needs to be monitored in an ongoing manner, and care needs to be modified, as appropriate, in response to changes in their clinical status.

Four regional CM trainings were conducted in 2011 To support fidelity and competency in the delivery of
CM, the Philadelphia CESATE has been convening coaching teleconferences with CM providers.
Prior to enrolling patients in CM, providers participated in 2 CM Planning calls to review their CM implementation plan.
Once CM commences at their facility, providers participate in 4 Implementation calls in the first 6 months of implementation and ongoing calls every 6 months thereafter.
Providers submit Implementation Review forms which help identify departures from the proper protocol.
Since the final regional training in July 2011, 90 VA programs have begun delivering CM 82/90 (91%) are targeting abstinence 8/90 (9%) are targeting treatment attendance
…>80% Participation Rate on CM Coaching Calls
…>1200 veterans have received CM targeting abstinence.
…>90% of the nearly 15,000 urine specimens collected across all VHA CM programs have tested negative for the target drug.

Conclusions

Comorbidity is Common
• Over 140,000 vets with SUD and PTSD in FY13– up 76% from FY2008!!
• Between 23 and 35% of vets with major depression, schizophrenia, and bipolar disorder also have SUD

Pressing Questions• More information about individual treatments for
SUD and PTSD than about combined SUD/PTSD TX– Best combinations of psychotherapy and/or
pharmacotherapy?– Concurrent v. integrated?
• How to improve retention?– Shared decision making– Treatment matching?

When to Offer PE or CPT?
• No metric yet• Case by case decision with pts using collaborative
approach• Abstinent or willing to cut down?
– Willing not to use in a way that would disrupt treatment• Motivated for treatment• What supports are in place?

Strong emphasis on quality care
• Requirements for the kind of care vets can expect to receive are outlined in:– Uniform Services Handbook– Practice Guidelines
• Increased emphasis on evidence-based SUD treatments and measurement-based care
• Large-scale training initiatives within VA to disseminate evidence-based practices

Reorganization of MH services
• Introduction of BHIP and PACT models
• Attempt to manage patients more effectively across the continuum of care
• Concern about how to staff BHIP and still maintain adequate staffing for SUD specialty care

Thanks to Collaborators
• Penn and Phila VA– Donna Coviello
– Dom DePhilippis
– Michelle Drapkin
– Jessica Goodman
– Megan Ivey
– Kevin Lynch
– Dave Oslin
– Debbie Van Horn
• Other Institutions– Jon Morgenstern
(Columbia)
– Dan Kivlahan (U Wash)
– Susan Murphy (U Mich)
– Don Shepard (Brandeis)
– Mike French (U Miami)

Funding and Disclosures• Funding from NIAAA
– R01 AA10341 and R01 AA014850
– P01-AA016821
• Funding from NIDA– R01 DA020623
– K24-DA029062
• Funding from VHA• Caron Treatment Centers covers a portion of my
U Penn salary• No pharmaceutical company consultation
Contact Information
James R. McKay, Ph.D.
Center on the Continuum of Care in the Addictions
3440 Market St., Suite 370
Philadelphia, PA 19104
(215) 746-7704