Treatment as Prevention - WHO
64
British Columbia Centre for Excellence in HIV/AIDS Julio Montaner MD, FRCPC, FCCP, FRSC Director, BC-Centre for Excellence on HIV/AIDS, Providence Health Care Professor of Medicine and Head, Division of AIDS, University of British Columbia President, International AIDS Society UNAIDS, Geneva, March 24th 2010 Treatment as Prevention: HAART Expansion - A Powerful Strategy to Reduce AIDS Morbidity and Mortality and HIV Incidence
Transcript of Treatment as Prevention - WHO

British ColumbiaCentre for Excellencein HIV/AIDS
Julio Montaner MD, FRCPC, FCCP, FRSCDirector, BC-Centre for Excellence on HIV/AIDS, Providence Health Care
Professor of Medicine and Head, Division of AIDS, University of British ColumbiaPresident, International AIDS Society
UNAIDS, Geneva, March 24th 2010
Treatment as Prevention:HAART Expansion - A Powerful Strategy to Reduce
AIDS Morbidity and Mortality and HIV Incidence

05
10152025303540
82 84 86 88 90 92 94Year
Dea
ths
per 1
00,0
00 P
opul
atio
n UnintentionalinjuryCancer
HeartdiseaseSuicide
HIV infection
Homicide
Chronic liverdiseaseStroke
Diabetes
USA - Trends in Annual Rates of DeathAges 25 to 44

Announced Oct 6th 2008
Harald zur Hausen Harald zur Hausen Françoise Françoise Barré-Sinoussi Barré-Sinoussi Luc Luc MontagnierMontagnier

Vancouver 1996“One World One Hope”

J Mellors et al. Annals 1997
00
20
40
60
80
100> 750501-750351-500201-350< 200
> 30 10-30 3-10 0.5-3 < 0.5
CD4+cells/µL
Plasma HIV RNA (thousand copies/mL)
% Progression to AIDS in 3 yrs
Vancouver 1996“One World One Hope”
Plasma Viral Load, a strong Predictor of outcome in HIV Infected Individuals
High Plasma Viral Load: Poor PrognosisLow Plasma Viral Load: Good Prognosis

Montaner et al JAMA, March 25th 1998
Triple Therapy: AZT + ddI + NVP
AZT + ddI
AZT + NVP
Study Weeks0
0
-1
-2
-3
Dual Therapy Regimens
Triple Therapy: AZT+3TC+IDV
Gulick et al; JAMA, July 1, 1998
52
J Mellors et al. Annals 1997
00
20
40
60
80
100> 750501-750351-500201-350< 200
> 30 10-30 3-10 0.5-3 < 0.5
CD4+cells/µL
Plasma HIV RNA (thousand copies/mL)
% Progression to AIDS in 3 yrs
Vancouver 1996“One World One Hope”
Cha
nge
in V
iral L
oad

Impact of HAART in BC-CfE
0
20
40
60
80
100
120
140
1993-94 1995-96 1997-98 1999-00 2001-02 2003-04
Death Rate per 1000
Modified from Hogg et al, Lancet. 2009
Greater than 85% reduction in death rate among those
engaged in care

Impact of HAART in BC-CfE
0
20
40
60
80
100
120
140
1993-94 1995-96 1997-98 1999-00 2001-02 2003-04
Death Rate per 1000
0
5
10
15
20
25
30
35
1993-94 1995-96 1997-98 1999-00 2001-02 2003-04
Life Expectancy at age 20
Modified from Hogg et al, Lancet. 2009


HAART Can Reduce HIV Transmission
HAART stops HIV replication↓
HIV levels fall to undetectable in blood
as well as in sexual fluids↓
Sharp reduction in HIV transmission
Prevention Strategies
- Education- Change in behavoir- Harm reduction- New strategies/technology- Vaccines
Existing strategies have failedto contain the global HIV pandemic

Modified from Alimenti et al CAHR, 2009
VerticalTransmission
Canada, 1990 to 2008

Discordant Couples
S Attia, M Egger, M Muller, M Zwahlen and N Lowa. AIDS. 2009 Jul 17;23(11):1397-404

Discordant Couples
S Attia, M Egger, M Muller, M Zwahlen and N Lowa. AIDS. 2009 Jul 17;23(11):1397-404
Studies of heterosexual discordant couples observed notransmission in patients treated with ART and with viral load
below 400 c/ml, but data were compatible with onetransmission per 79 person-years.

B&M Gates Fdn: HIV Transmission Risk inHeterosexual Serodiscordant Couples
3,400 couples In 7 African countries
All counseled and given free condoms
HAART initiated based on CD4 count eligibility
Over the next 1 to 3 years, 103 new HIV infections
All but 1 infection occurred in the untreated couples Estimated 92% reduction of HIV transmission by HAART
Unadjusted relative risk: 0.17 (95% CI: 0.004-0.94; P = .037)
Adjusted relative risk: 0.08 (95% CI: 0.002-0.57; P = .004)
Adjusted for visit and CD4+ cell count at initiation
Donnell D, et al. CROI 2010. Abstract 136.

B&M Gates Fdn: HIV Transmission Risk inHeterosexual Serodiscordant Couples
3,400 couples In 7 African countries
All counseled and given free condoms
HAART initiated based on CD4 count eligibility
Over the next 1 to 3 years, 103 new HIV infections
All but 1 infection occurred in the untreated couples Estimated 92% reduction of HIV transmission by HAART
Unadjusted relative risk: 0.17 (95% CI: 0.004-0.94; P = .037)
Adjusted relative risk: 0.08 (95% CI: 0.002-0.57; P = .004)
Adjusted for visit and CD4+ cell count at initiation
Donnell D, et al. CROI 2010. Abstract 136.
More recently an email has been circulated saying that: More recently an email has been circulated saying that: ““The single case of transmission involved a man The single case of transmission involved a man who initiated who initiated ARVs ARVs 18 days before his 12-month 18 days before his 12-month
study visit. At this visit his partner tested positive for HIV, study visit. At this visit his partner tested positive for HIV, having been negative at month 9.having been negative at month 9.””


Wood et al, BMJ, 2009

Wood et al, BMJ, 2009
Whiskers represent 95% confidence intervals.

Wood et al, BMJ, 2009
Whiskers represent 95% confidence intervals.

Wood et al, BMJ, May 16, 2009

6 months Baseline
Plasma Viral Load (log10 copies/mL) Distribution
Modified from Anema et al. EIDJ 2009
Impact of HAART in BC-CfEFr
eque
ncy
of p
eopl
e

24 months Baseline
Plasma Viral Load (log10 copies/mL) Distribution
Impact of HAART in BC-CfEFr
eque
ncy
of p
eopl
e
Modified from Anema et al. EIDJ 2009

New HIV and Syphilis in BC
M REKART, BC-CDC, 2006
Rat
e pe
r 100
,000
pop
ulat
ion

New HIV and Syphilis in BCR
ate
per 1
00,0
00 p
opul
atio
n
M REKART, BC-CDC, 2006

Cost of Medical Management of 1 HIV infection over alifetime = $250,000
“HIV deficit” in BC in 2005: 400
Cost-Effectiveness of HAARTBC-DTP
Averted lifetime Rx cost up to 2001 US $96.4MA total of 3,963 pts were on HAART in BC in 2005
Total actual drug cost (using patented drugs) in 2005 $49 million US
800 cases per year
400 cases per year

Cost of Medical Management of 1 HIV infection over alifetime = $250,000
“HIV deficit” in BC in 2005: 400
Cost-Effectiveness of HAARTBC-DTP
Averted lifetime Rx cost up to U$A 100MA total of 3,963 pts were on HAART in BC in 2005
Total actual drug cost (using patented drugs) in 2005
U$A 50M
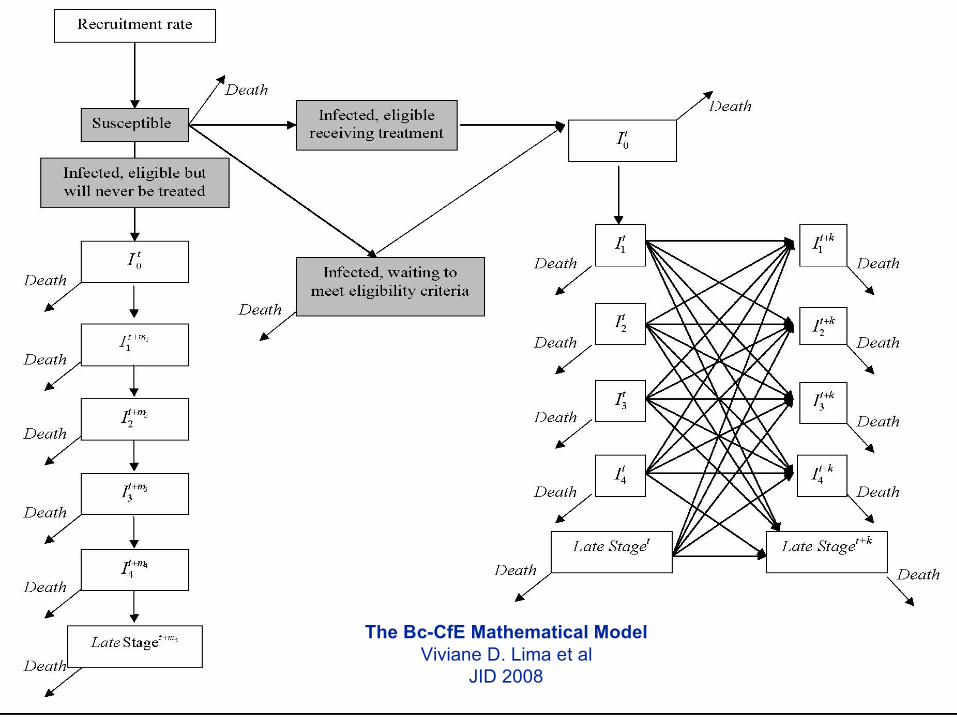
The Bc-CfE Mathematical ModelViviane D. Lima et al
JID 2008

Adherence: 0% - <40%
Guideline: !200 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Current Adherence: 78.5%
Guideline: !200 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Adherence: 80% - <95%
Guideline: !200 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Adherence: 95% - 100%
Guideline: !200 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Adherence: 0% - <40%
Guideline: !350 cells /mm 3
100
150
200
250
300
350
400
450
500
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Current Adherence: 78.5%
Guideline: !350 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Adherence: 80% - <95%
Guideline: !350 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
Adherence: 95% - 100%
Guideline: !350 cells /mm 3
100
150
200
250
300
350
400
450
500
550
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Num
ber
of N
ew I
nfec
tions
50% 75% 90% 100%Coverage:
CD4 200/mm3Adh <40%
CD4 200/mm3Adh 40 - 80%
CD4 200/mm3Adh 80 - 95%
CD4 200/mm3Adh 95 - 100%
CD4 350/mm3Adh <40%
CD4 350/mm3Adh 40 - 80%
CD4 350/mm3Adh 80 - 95%
CD4 350/mm3Adh 95 - 100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%
50%75%90%
100%V D Lima et al
JID 2008

Incremental net benefit (Millionsof CDN $) over 30 years
K Johnston et al, submitted, 2010
0 5 10 15 20 25 30
020
040
060
080
0
Time (years)
Net
Ben
efit
(milli
on $
Can
200
5)
Overall PopulationPatient-Centered
Overall population and
patient-centered
incremental net benefit of
increasing uptake of
HAART from 50% to 75%
over 30 years, based on a
willingness-to-pay
thresholds of $50,000 per
quality-adjusted life year.
Summary
HAART is widely regarded as a cost effective, life-saving strategy
↓ Mortality of treated HIV/AIDS patients↓ Morbidity of treated HIV/AIDS patients↓ Health Resource utilization↓ Vertical Transmission of HIV infection
Furthermore, when the impact of HAART on HIVtransmission is considered, HAART expansionbecomes a cost-averting strategy

The third approach, though, is the most intriguing. This is to do nothingmore than press ahead faster with the treatment program. Since treatmentreduces viral load, it should, in theory, make those being treated lessinfectious. Of course, theory is one thing and practice another. But studiesin Taiwan and British Columbia (the latter by Julio Montaner, the incomingpresident of the International AIDS Society, which organizes the conference)have shown big falls in transmission rates as ARVs have been rolled out.

HIV prevalence
Montaner et al, Lancet 2006
Number of infectionsprevented
Treat all
Treat 30%
Cost of treatment
Treat all
Treat 30%
The Power of HAART: Demographic Model

R Granich, C Gilks, C Dye, K De Cock, B Williams. The Lancet Nov 26th 2008

AIDS Nov 27th 2008, The EconomistDeploying the drugs used to treat AIDS may be the way to limit its spread
Illustration by Peter Schrank
Thank you
AIDS Nov 27th 2008, The EconomistDeploying the drugs used to treat AIDS may be the way to limit its spread
Illustration by Peter Schrank
Thank you


An Alternative Approach
Preliminary Results

Methods Prospective ecological study in BC, Canada
Used administrative records to evaluate the associationbetween expansion of HAART coverage, population levelplasma HIV-1-viral load and new HIV diagnoses
HIV testing, CD4 & viral load testing and HAARTdistribution are centralized and free in BC
Data for second half of 2009 is preliminary due to delayedreporting, therefore only the first half of 2009 was used forstatistical analyses
Montaner et al, CROI 2010

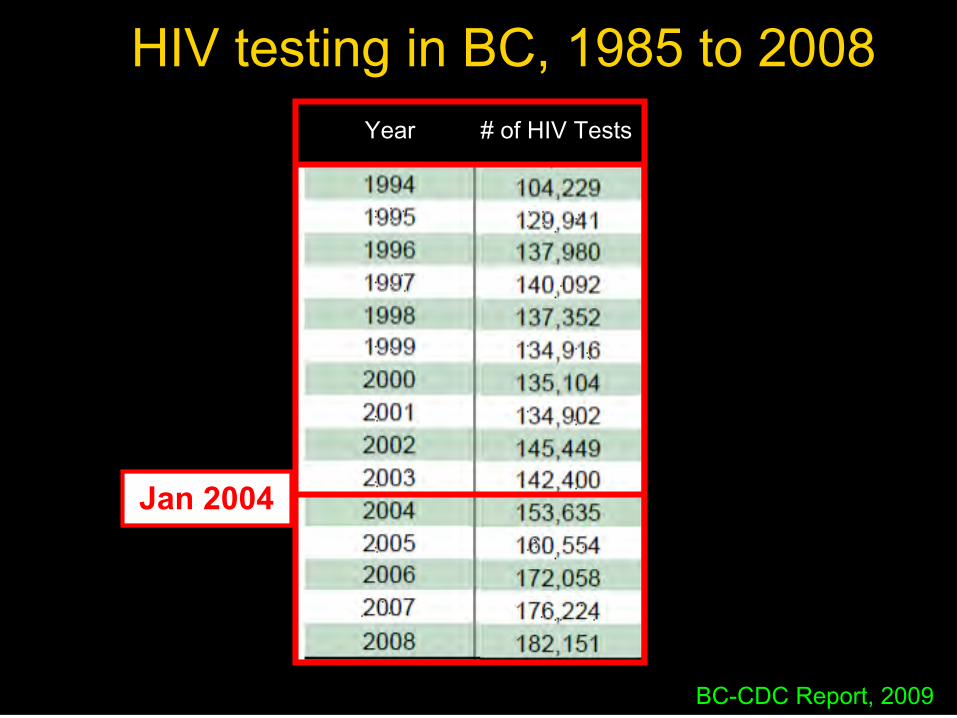
January 2004
The second expansion of HAARToccurred prior to the new 2008
IAS-USA Guidelines, which wereadopted in BC at the end of 2008
The first expansion of HAARToccurred as a result of the new 1996
IAS-USA Guidelines, which wereadopted in BC in the summer of
1996
Summer of 1996
Year Montaner et al, CROI 2010


0.01
0.10
1.00
1995 2000 2005 2010
0.20
0.02
0.04
0.01
0.10
1.00
1995 2000 2005 2010
0.20
0.02
0.04
90
80
70
60
Inci
denc
e/yr
Vira
l loa
d <
50/
mL
(%)
Acquired resistancefalling
Plasma viral loadsuppression rising

Num
ber of New
HIV+ D
iagnosesNum
ber o
f Act
ive
HA
AR
T Pa
rtic
ipan
ts
Year
New HIV+ Diagnoses (All)
New HIV+ Diagnoses (IDU)
Active on HAART
Number of Active HAARTParticipants and Number of New
HIV+ Diagnoses per Year
p=0.015
Montaner et al, CROI 2010

Number of Active HAARTParticipants and Number of New
HIV+ Diagnoses per Year
New HIV+ Diagnoses (All)
New HIV+ Diagnoses (IDU)
Active on HAART
Num
ber of New
HIV+ D
iagnoses
Year
Num
ber o
f Act
ive
HA
AR
T Pa
rtic
ipan
ts
p=0.015
p=0.085
p=0.026
Montaner et al, CROI 2010

“True” New Yearly HIV Diagnoses in BC
BC-CDC Updated March 2010
Jan 2004
Year Year # of HIV Tests # of HIV Tests
BC-CDC Report, 2009
HIV testing in BC, 1985 to 2008

Hepatitis C, 1999-2008 Infectious Syphilis, 1999-2008
Genital Chlamydia, 1999-2008 Gonorrhea, 1999-2008
• BC
x Canada
• BC
x Canada
• BC
x Canada• BC
x Canada
2004
2004 2004
2004

HighestHIV-1- PlasmaViral load per
Year
Ever on Treatment&
Censoring at the time ofDeath or Move
IDUIDU
The proportion of HIV infected IDUs engaged in care in BC with plasma viralload >1500 c/mL, as a surrogate for “high” community HIV-1-viral load,
decreased from ~50% in 2000-04 to ~20% in 2009 (p<0.001)
Non IDUNon IDU
Montaner et al, CROI 2010

“Provincial Viral Load”All Patients Ever Tested for Plasma HIV-1-Viral Load in BC
Censoring at the time of Death or MoveCensoring at the time of Death or Move

New Data: Pre HAART CD4 Count
Montaner et al, 2010, Preliminary Data

Community pVL and New HIV DiagnosesSan Francisco
Das-Douglas M, et al. CROI 2010. Abstract 33.
Mean CVL
0
5000
10,000
15,000
20,000
25,000
30,000
2004 2005 2006 2007 2008
Mea
n C
omm
unity
Vira
l Loa
d (c
opie
s/m
L)
Newly diagnosed andreported HIV cases
0
200
400
600
800
1000
1200
Num
ber of New
ly Diagnosed H
IV Cases
P = .005 forassociation*
798
642523 518
434
*Data insufficient to prove significant association with reduced HIV incidence.
A Formidable Challenge
A Unique Opportunity

When to Start HAART?A matter of Perspective
years
Viral Load
CD4 Count

When to Start HAART?A matter of Perspective
years
years
Viral Load
CD4 Count

When to Start HAART?A matter of Perspective
years
years
years
Viral Load
CD4 Count

When to Start HAART?A matter of Perspective
years
years
years
Viral Load
CD4 Count
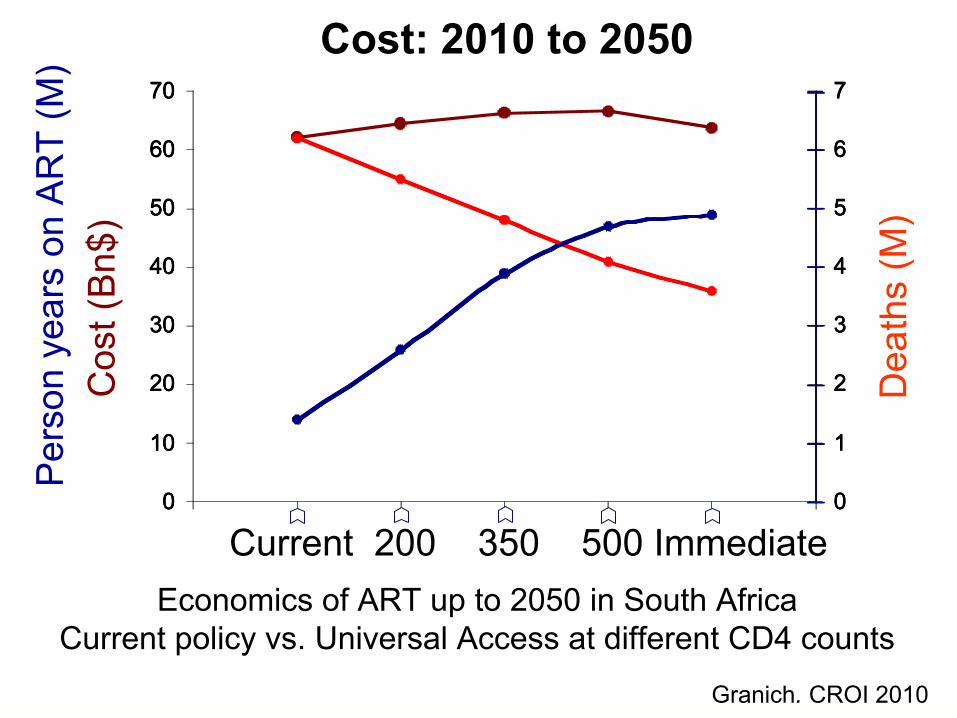
Cost: 2010 to 2050
Granich. CROI 2010
0
10
20
30
40
50
60
70
0 1 2 3 4 5 60
1
2
3
4
5
6
7
0
10
20
30
40
50
60
70
0 1 2 3 4 5 60
1
2
3
4
5
6
7
0
10
20
30
40
50
60
70
0 1 2 3 4 5 60
1
2
3
4
5
6
7
Pers
on y
ears
on
ART
(M)
Dea
ths
(M)
Cos
t (B
n$)
Economics of ART up to 2050 in South AfricaCurrent policy vs. Universal Access at different CD4 counts
Current 200 350 500 Immediate

STOP HIV & AIDSSTOP HIV & AIDS: Seek and Treat toOptimally Prevent HIV & AIDS*
* Supported through a $2.5M five year Avant Garde Award by theNational Institute for Drug Abuse (NIDA) at the NIH in 2008 and$48M (+ drugs) four year outreach grant by BC Govt in 2010

Prospectively Evaluate the Impact of HAART Expansionon AIDS Morbidity and Mortality and HIV Incidence in BC
Intervention Primary Endpoint HAART Expansion HIV Incidence within medical guidelines at years 3 to 5
Secondary Endpoints:
MORBIDITY AND MORTALITY, CD4 COUNTS, HIV-1-RNA LEVELS,
RESISTANCE, ADVERSE EVENTS, SAFETY, ADHERENCE,
HOSPITALIZATIONS, RESOURCE UTILIZATION
STOP HIV & AIDSSTOP HIV & AIDS: Seek and Treat toOptimally Prevent HIV & AIDS*
* Supported through a $2.5M five year Avant Garde Award by theNational Institute for Drug Abuse (NIDA) at the NIH in 2008 and$48M (+ drugs) four year outreach grant by BC Govt in 2010

HAART has a substantial added preventive value
The magnitude of this effect is not yet fully characterized, and
may well vary in different settings
Seek and Treat among those who have a medical indication for
HAART cannot wait for the above to be resolved
Many lives will be saved and much insight will be gained from
closely monitoring a more “aggressive”roll out of HAART within Rx
Guidelines
Seek and Treat outside the range where treatment is medically
indicated remains a research question
However, Rx Guidelines leave few outside the “treatment
envelope”
TAP should serve to re-energize Universal Access
HAART Expansion to Reduce AIDSMorbidity & Mortality, and HIV Incidence

Combination prevention
CommunityInterventions
BiomedicalInterventions
StructuralInterventions
HIV testing,linkage to careand expanded
HAARTcoverage
Individualand small
groupbehavioral
interventions
HIVHIVPreventionPrevention
Modified from T. Coates

All scientific work is incomplete - whether it beobservational or experimental. All scientific work isliable to be upset or modified by advancingknowledge. That does not confer upon us a freedomto ignore the knowledge we already have, or topostpone the action that it appears to demand at agiven time.
Bradford-Hill, A. 1965 The environment and disease: Association orCausation? President address at January 14 meeting. Proceedings of the
Royal Society of Medicine 163 (seriesB): 295-300
A Statistician’s Opinion

British ColumbiaCentre for Excellencein HIV/AIDS
Seek and Treat to OptimallyPrevent HIV & AIDS
STOP HIV & AIDSSTOP HIV & AIDS
R Hogg, E Wood, T Kerr, M Tyndall, A Levy, PR Harrigan,Viviane Lima, Aranka Anema, Stephen Smith, Warren O’Brien
Pedro Cahn, Jose Esparza, Craig Mc Clure, Robin GornaJacques Normand, Nora Volkow
IAS - USA ART Guidelines Panel, IAS, WHO and UNAIDS
BC-MoH and MHL&SSPH Foundation
Merck, Gilead, ViiVMSHRF, CIHR, NIDA and NIH
H&W, Ottawa
Research Staff and Study Participants

Thank You
British ColumbiaCentre for Excellencein HIV/AIDS