Treatment and prognosis of patients with recurrent …Treatment and prognosis of patients with...
7
Page 1 of 7 Original research study Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) Competing interests: none declared. Conflict of interests: none declared. All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study T Jin 1 , H Lin 2,3 , HX Lin 2,3 , XY Cai 2,3 , HZ Wang 2,3 , WH Hu 2,3 , LB Guo 4 , JZ Zhao 5 * Abstract Introduction Although recurrent laryngeal carci- noma is a common clinical problem, the data regarding its natural history and prognostic factors are limited. The aims of this study were to evaluate the treatment outcomes of patients with recurrent laryngeal carcinoma and to identify the value of several prognostic factors. Methods A retrospective analysis of 224 con- secutive cases of recurrent laryngeal carcinoma, treated between 1996 and 2009, was performed. Overall survival was estimated using the Kaplan–Meier method. Log-rank test was employed to identify significant prognostic fac- tors for overall survival. The Cox pro- portional hazards model was applied to identify covariates significantly associated with the aforementioned endpoint. Results The estimated 3-, 5- and 10-year survival rates of the entire patient sample were 56.6%, 46.4% and 39.2%, respectively. On univariate analysis, the age, smoking index, grade, primary site, initial T stage, initial Union for International Cancer Control (UICC) stage and nodal status of the pri- mary tumour, as well as disease-free interval, extent of recurrence and suitability for surgery were all pow- erful prognostic factors for survival. On multivariate analysis, four varia- bles retained statistical significance: the initial T stage, nodal status, extent of recurrence and suitability for surgery. Conclusion Our results suggest that lower initial T stage, no initial cervical lymph node metastasis, only local recurrence and patients suitable for salvage surgery are favourable prognostic factors for overall survival of patients with recurrent laryngeal cancer. Introduction In the United States, it is estimated that about 49,260 new cases of oral cavity, pharyngeal and laryngeal can- cers occurred in 2010. An estimated 11,480 deaths from head and neck cancers occurred during the same time 1 . Of all head and neck tumours, 20% originate in the larynx. Recur- rences are common in laryngeal can- cer. The rate of recurrence in patients with T1 tumours of the larynx ranges from 5% to 13%, and in patients with T2 tumours, from 25% to 30% 2 . For patients with advanced laryngeal cancer, the rate of recurrence is approximately 30%–50% as reported by some studies 3–5 . The most frequent site of recurrence is the larynx itself, including the peristomal area fol- lowed by the regional lymph nodes and, less often, distant sites 6,7 . The options for patients who have failed definitive treatment for squa- mous cell carcinoma (SCC) of the larynx include (1) salvage surgery; (2) repeat radiation therapy (reirradiation), with or without chemotherapy; (3) palliative chemotherapy and (4) supportive care. Surgery is recommended for resectable recurrent locoregional disease. Surgi- cal treatment can either be endoscopic laser treatment or laryngectomy (partial or total), depending on the size and site of the tumour. Small recurrences can be treated by endo- scopic laser treatment. Larger tumours and those with subglottic extension are generally treated by total laryn- gectomy. Adjuvant therapy depends on the risk factors. If the recurrence is unresectable and the patient did not have prior radiotherapy, then radio- therapy with concurrent systemic therapy is recommended, depending on the performance status. For patients with recurrent disease not amenable to curative-intent radiation or surgery, the treatment approach is the same as that for patients with metastatic disease. Enrolment in a clinical trial is preferred. Choice of treatment also depends on age, general health and preference of the patient. The survival rate after local recurrence and salvage surgery varies greatly from 22% to 66% 8–11 . Some authors even report an overall 5-year survival rate of as low as 2% in this patient population 4 . This retrospective study reviews a series of 224 consecutive recurrent laryngeal carcinomas observed at our institutions and managed with the aforementioned therapeutic choices. The aim of this study was to report our results and try to identify, in a retrospective analysis, potential prog- nostic factors and possible guidelines in tailoring the most appropriate treatment for patients with recurrent laryngeal carcinoma. * Corresponding author Email: [email protected] 1 Department of Radiation Oncology, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China 2 Department of Radiation Oncology, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China 3 State Key Laboratory of Oncology in South China, Guangzhou, Guangdong, People’s Republic of China 4 Department of Oncology, Guangdong Second Provincial People’s Hospital, Guangzhou, Guangdong, People’s Republic of China 5 Department of Head and Neck Surgery, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China
Transcript of Treatment and prognosis of patients with recurrent …Treatment and prognosis of patients with...

Page 1 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study
T Jin1, H Lin2,3, HX Lin2,3, XY Cai2,3, HZ Wang2,3, WH Hu2,3, LB Guo4, JZ Zhao5*
AbstractIntroductionAlthough recurrent laryngeal carci-noma is a common clinical problem, the data regarding its natural history and prognostic factors are limited. The aims of this study were to evaluate the treatment outcomes of patients with recurrent laryngeal carcinoma and to identify the value of several prognostic factors.MethodsA retrospective analysis of 224 con-secutive cases of recurrent laryngeal carcinoma, treated between 1996 and 2009, was performed. Overall survival was estimated using the Kaplan–Meier method. Log-rank test was employed to identify significant prognostic fac-tors for overall survival. The Cox pro-portional hazards model was applied to identify covariates significantly associated with the aforementioned endpoint.ResultsThe estimated 3-, 5- and 10-year survival rates of the entire patient sample were 56.6%, 46.4% and 39.2%, respectively. On univariate analysis, the age, smoking index, grade, primary
site, initial T stage, initial Union for International Cancer Control (UICC) stage and nodal status of the pri-mary tumour, as well as disease-free interval, extent of recurrence and suitability for surgery were all pow-erful prognostic factors for survival. On multivariate analysis, four varia-bles retained statistical significance: the initial T stage, nodal status, extent of recurrence and suitability for surgery.ConclusionOur results suggest that lower initial T stage, no initial cervical lymph node metastasis, only local recurrence and patients suitable for salvage surgery are favourable prognostic factors for overall survival of patients with recurrent laryngeal cancer.
IntroductionIn the United States, it is estimated that about 49,260 new cases of oral cavity, pharyngeal and laryngeal can-cers occurred in 2010. An estimated 11,480 deaths from head and neck cancers occurred during the same time1. Of all head and neck tumours, 20% originate in the larynx. Recur-rences are common in laryngeal can-cer. The rate of recurrence in patients with T1 tumours of the larynx ranges from 5% to 13%, and in patients with T2 tumours, from 25% to 30%2. For patients with advanced laryngeal cancer, the rate of recurrence is approximately 30%–50% as reported by some studies3–5. The most frequent site of recurrence is the larynx itself, including the peristomal area fol-lowed by the regional lymph nodes and, less often, distant sites6,7.
The options for patients who have failed definitive treatment for squa-mous cell carcinoma (SCC) of the larynx
include (1) salvage surgery; (2) repeat radiation therapy (reirradiation), with or without chemotherapy; (3) palliative chemotherapy and (4) supportive care. Surgery is recommended for resectable recurrent locoregional disease. Surgi-cal treatment can either be endoscopic laser treatment or laryngectomy (partial or total), depending on the size and site of the tumour. Small recurrences can be treated by endo-scopic laser treatment. Larger tumours and those with subglottic extension are generally treated by total laryn-gectomy. Adjuvant therapy depends on the risk factors. If the recurrence is unresectable and the patient did not have prior radiotherapy, then radio-therapy with concurrent systemic therapy is recommended, depending on the performance status. For patients with recurrent disease not amenable to curative-intent radiation or surgery, the treatment approach is the same as that for patients with metastatic disease. Enrolment in a clinical trial is preferred. Choice of treatment also depends on age, general health and preference of the patient. The survival rate after local recurrence and salvage surgery varies greatly from 22% to 66%8–11. Some authors even report an overall 5-year survival rate of as low as 2% in this patient population4.
This retrospective study reviews a series of 224 consecutive recurrent laryngeal carcinomas observed at our institutions and managed with the aforementioned therapeutic choices. The aim of this study was to report our results and try to identify, in a retrospective analysis, potential prog-nostic factors and possible guidelines in tailoring the most appropriate treatment for patients with recurrent laryngeal carcinoma.
* Corresponding authorEmail: [email protected] Department of Radiation Oncology, Zhejiang
Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China
2 Department of Radiation Oncology, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China
3 State Key Laboratory of Oncology in South China, Guangzhou, Guangdong, People’s Republic of China
4 Department of Oncology, Guangdong Second Provincial People’s Hospital, Guangzhou, Guangdong, People’s Republic of China
5 Department of Head and Neck Surgery, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China

Page 2 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
Materials and methodsCharacteristics of patient enrolment criteriaBetween 1996 and 2009, 1621 con-secutive patients with neoplasms of the larynx were observed at the Sun Yat-sen University Cancer Center, China. Of these, 1556 patients had biopsy-proven SCC of the larynx. With a median follow-up time of 49.5 months (range, 7–176 months), recur-rent disease was diagnosed in 253 patients (16.3%). Among these 253 patients, the enrolment criteria were as follows: (a) each patient’s complete clinical and pathological data includ-ing age, gender, blood type, stage, smoking index, alcohol consumption, histological differentiation and treat-ment status; (b) patients were restaged according to the guidelines of the 2002 Union for International Cancer Control (UICC) by the cancer staging system; (c) no patient had distant metastasis at the time of initial staging and (d) patients were initially treated with the goal of a cure at our institution by one or a combination of three modali-ties: surgery, radiation therapy and chemotherapy. The study was approved by the Research Ethics Committee of the Sun Yat-sen University Cancer Center.
A total of 224 patients were evalu-ated in this analysis according to the above criteria. Patient characteristics are summarized in Table 1. There were 216 male (96.4%) and 8 female (3.6%) patients. The median age at diagnosis was 60 years (range, 16–83). There were 79 cases of T1, 67 cases of T2, 43 cases of T3 and 35 cases of T4. There were 105 cases of good differentiation, 94 cases of moderate differentiation and 25 cases of poor differentiation.
Treatment approaches for initial tumoursWhen selecting treatment approaches, a comprehensive consideration of each individual patient, their economic situ-ation and their treatment preferences was made by the multidisciplinary team at our cancer centre.
Table 1 Patient characteristics
Features No. of patients %
Gender
Female 8 3.6
Male 216 96.4
Age (years)a
<60 108 48.2
≥60 116 51.8
Histological grade
Well 105 46.9
Moderately 94 42.0
Poorly 25 11.1
Smoking indexb
<600 102 45.5
≥600 122 54.5
Alcohol consumption
No 146 65.2
Yes 78 34.8
Primary site
Glottic 155 69.2
Supraglottic 61 27.2
Subglottic 8 3.6
T Stage
1 and 2 146 65.2
3 and 4 78 34.8
Cervical lymph node metastasis
Positive 49 21.9
Negative 175 78.1
TNM Stage
I and II 133 59.4
III and IV 91 40.6
Blood type
A 66 29.5
B 54 24.1
AB 24 10.7
O 80 35.7aPatients were divided according to the median age.bSmoking index is defined as the number of cigarettes used per day × the total smoking time (years).

Page 3 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
For the treatment modality of the pri-mary site, 120 patients received surgery alone; 22 patients received 68–76 Gy radiation alone; 64 patients received surgery plus 60–66 Gy post-operative radiotherapy; 1 patient received 66 Gy radiotherapy plus surgery and 17 patients were treated with combined cisplatin-based chemotherapy, includ-ing 4 cases of neoadjuvant chemother-apy plus radiotherapy, 6 cases of surgery plus adjuvant chemotherapy, 1 case of concurrent chemoradiotherapy, 2 cases of surgery with concurrent chemora-diotherapy, 2 cases of neoadjuvant chemotherapy plus surgery plus 60 Gy post-operative radiotherapy and 2 cases of surgery plus adjuvant chem-otherapy plus 66 Gy post-operative radiotherapy.
In the surgical treatment of the neck, 72 patients were managed by neck dissection, including 27 cases with modified radical neck dissection (MRND) and 45 cases with selective neck dissection (SND). Further, 7 patients underwent 50–60 Gy neck radiation alone; 22 patients had com-bined neck dissection with 40–50 Gy post-operative radiotherapy; 3 patients were given cisplatin-based chemo-therapy alone; 106 patients received no active therapy and were observed; 14 patients had combined cisplatin-based chemotherapy, including 5 cases of neoadjuvant chemotherapy plus radiotherapy; 3 cases of surgery plus adjuvant chemotherapy; 1 case of con-current chemo-radiotherapy; 2 cases of surgery with concurrent chemo-radiotherapy; 2 cases of neoadjuvant chemotherapy plus surgery plus 54 Gy post-operative radiotherapy and 1 patient received surgery plus 60 Gy post-operative radiotherapy plus adjuvant chemotherapy.
Follow-up time and methodFollow-ups were conducted mainly via outpatient check-ups. The follow-up examination was started after treatment. Patients were seen every 2 months during the first year, every 3 months for the subsequent 2 years
and then every 6 months thereafter until death. All loco-regional tumours were diagnosed by clinical examina-tion, magnetic resonance imaging (MRI) or intensive computed tomog-raphy (CT), fiberoptic endoscopy and biopsy. Distant metastases were diag-nosed by clinical symptoms, physical examinations and imaging methods, including chest X-ray, bone scan, abdominal sonography, MRI, intensive CT or positron emission CT.
Statistical analysesSurvival was defined as the interval between the date of diagnosis of recur-rent disease and date of death or the last date on which the patient was known to be alive. Patients who died of no other documented cause were considered to have died from recur-rent laryngeal cancer. SPSS 13.0 statistical software was used (SPSS Inc., Chicago, IL) for analysis. The survival rate and univariate analysis were performed by the Kaplan–Meier method12 and log-rank test. Multivariate
analyses with the Cox proportional hazards model13 were used to test the independent significance by forward elimination of insignificant explana-tory variables of different parameters. A two-tailed P value of <0.05 was considered statistically significant.
ResultsSite of recurrenceAs many as 151 patients (67.4%) had local recurrence, either alone (140 patients) or with regional (11 patients) recurrence. In 57 patients (25.4%), there was a failure in the regional lymph nodes only, whereas 14 patients (6.3%) had isolated distant metasta-ses. However, 2 patients (0.9%) had regional lymph node recurrence and distant metastases. The median dis-ease free interval for all 224 patients was 11 months (range, 3–124).
Treatment for recurrent tumourThe treatments given at recurrence are summarized in Table 2. Surgery was performed in 142 patients (63.4%) for
Table 2 Treatment at recurrent tumour
No. of patients %
Surgery (n = 142)
Partial laryngectomy 62 27.7
Total laryngectomy 33 14.7
Unilateral neck node dissection 25 11.2
Bilateral neck node dissection 5 2.2
Laryngectomy and neck node dissection 17 7.6
Radiation (n = 26)
Radiation alone 12 5.4
Surgery plus post-operative radiotherapy 14 6.3
Chemotherapy (n = 39)
Chemotherapy alone 30 13.4
Radiotherapy plus adjuvant chemotherapy 6 2.7
Surgery plus adjuvant chemotherapy 1 0.4
Surgery plus post-operative radiotherapy plus adjuvant chemotherapy
2 0.9
No active therapy (n = 17)
No active therapy 17 7.6

Page 4 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
locoregional disease. Further, 62 and 33 patients were treated with partial and total laryngectomy, respec-tively. Unilateral neck node dissection was performed in 25 patients, whereas bilateral neck node dissection was performed in 5 patients. Further, 17 patients were treated with both lar-yngectomy and neck node dissection; 12 patients received 46–70 Gy radia-tion alone; 14 patients received surgery plus 44–60 Gy post-operative radio-therapy; 30 patients were given cisplatin-based chemotherapy alone; 9 patients were treated with combined cisplatin-based chemotherapy, includ-ing 1 case of radiotherapy plus adju-vant chemotherapy, 6 cases of surgery plus chemotherapy, 2 cases of surgery plus 60 Gy post-operative radiother-apy plus adjuvant chemotherapy and 17 patients refused active therapy and hence received only supportive care.
SurvivalThe last follow-up was on 31 December 2012, with a median follow-up time of 49.5 months (range, 7–176). No patients were lost during the follow-up. In total, 118 patients were alive and 106 patients died. The estimated 3-, 5- and 10-year survival rates of the entire patient sample were 56.6%, 46.4% and 39.2%, respectively.
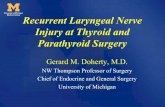
Univariate analysisAs shown in Table 3, survival after recurrence was significantly influ-enced by variables related to both primary and recurrent tumour. The age, smoking index, grade, primary site, initial T stage, initial UICC stage and nodal status of the primary tumour, as well as the disease-free interval, extent of the recurrence and suitable for surgery were powerful prognostic factors for survival (Figure 1).
Multivariate analysisMultivariate survival analysis was performed using the Cox regression model to calculate the odds ratio and 95% confidence intervals. Results of multivariate analysis are shown in
Table 3 Univariate analysis of prognostic factors for overall survival
Prognostic factor No. of patients 5-year OS χ2 P a
Gender 1.828 0.176
Female 8 62.5%
Male 216 45.7%
Ageb 7.910 0.005
<60 108 56.5%
≥60 116 37.4%
Smoking indexc 6.055 0.014
<600 102 52.2%
≥600 122 41.0%
Alcohol consumption 0.555 0.456
No 146 46.0%
Yes 78 49.9%
Grade 27.179 <0.001
Well 105 62.9%
Moderately 94 43.0%
Poorly 25 13.2%
Primary site 13.473 0.001
Glottic 155 51.1%
Supraglottic 61 29.7%
Subglottic 8 87.5%
Blood type 1.584 0.663
A 66 52.2%
B 54 46.6%
AB 24 49.6%
O 80 41.5%
Initial T stage 30.877 <0.001
1 and 2 146 60.9%
3 and 4 78 21.2%
Initial UICC stage 30.458 <0.001
I and II 133 61.9%
III and IV 91 23.8%
Initial nodal status 27.672 <0.001
Positive 49 21.8%
Negative 175 53.3%
Disease-free intervald 5.609 0.018
<11 months 105 40.9%
≥11 months 119 51.1%
Extent of recurrence 66.262 <0.001
Local only 140 55.8%
Regional (±local) 68 40.2%
(Continued)

Page 5 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
Table 4. Model A included variables related to both primary and recurrent tumour, while model B was composed of only the former and model C was composed of only the latter. Because the initial UICC stage depends on the initial T stage and nodal status, this variable was omitted from the analy-sis. According to model A, the initial T stage, nodal status and suitability for surgery strongly predicted patient out-come. When the analysis was limited
Figure 1: Survival curves of various groups of patients. (a) Overall survival by age. (b) Overall survival by smoking index. (c) Overall survival by grade. (d) Overall survival by primary site. (e) Overall survival by initial T stage. (f) Overall survival by initial nodal status. (g) Overall survival by disease-free interval. (h) Overall survival by extent of recurrence. (i) Overall survival by suitable for surgery.
Distant (±regional) 16 0%
Suitable for surgery 40.905 <0.001
No 65 17.4%
Yes 159 58.2%aLog-rank test.bPatients were divided into two groups according to the median age.cSmoking index is defined as the number of cigarettes smoked per day × the total smoking time (years).dPatients were divided into two groups according to the median duration of disease-free interval.
Table 3 (Continued)
Prognostic factor No. of patients 5-year OS χ2 P a

Page 6 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
to factors related with primary tumour (model B), initial T stage and nodal status were the only factors that pre-dicted survival. When the analysis was limited to recurrence-related fac-tors (model C), extent of recurrence and suitability for surgery were inde-pendent prognostic factors in recur-rent laryngeal SCC patients.
DiscussionDealing with recurrent laryngeal can-cer is arguably the greatest challenge faced by the physicians who treat these patients. This group of patients presents a unique set of dilemmas because the chance for a cure is low, and prior treatment generally has a negative impact on all current
therapeutic options. In this study, we retrospectively evaluated the signifi-cance of various prognostic factors related to both primary and recurrent tumour in 224 patients with recur-rent laryngeal cancer treated at the Sun Yat-sen University Cancer Center, China to gain a better understanding of the natural course of this entity and the factors predicting outcome.
The estimated 3-, 5- and 10-year survival rates of the entire patient sample were 56.6%, 46.4% and 39.2%, respectively. Our results are similar to those previously reported11,14. The estimated 5-year survival rate of the patients that had local recurrence was only 55.8%. When regional dis-ease was involved, the survival rate
decreased to 40.2%, with a further decline to 0% when distant metasta-ses were present.
On multivariate analysis, our results showed the 5-year overall survival (OS) was significantly related to the initial T stage, nodal status, extent of recurrence and operability of the recurrent tumour. Further, univariate analysis indicated that age ≥60 years, smoking index ≥600, poor degree of tumour differentiation (moderately or poorly), primary site (supraglottic cancer) and disease-free interval <11 months correlates with poor progno-sis. These results are partly similar to those previously reported11,14. In a similar research, Brenner et al.14 found that six prognostic factors related to survival of patients with recurrent laryngeal cancer on univar-iate analysis: T stage and nodal status of the primary tumour, primary tumour site, duration of disease-free interval, site of recurrence and operability of the recurrent tumour. Multivariate analysis only revealed that the initial site and site of recurrence retained statistical significance. When factors related to the primary disease were excluded from the analysis, the site of recurrence and its operability were the only predictors of survival. In addition, Lacy et al.15 found that the site of recurrence was a significant prognostic factor for survival, in addi-tion to the method of treatment of the primary tumour and original TNM stage. The operability of the recurrent tumour was also found to predict sur-vival, but only on univariate analysis. Goodwin et al.16 reported a prospective review of 109 consecutive patients (larynx with 46 patients) undergoing salvage surgery for recurrent SCC of the upper aerodigestive tract; they reported some contrasting results. They found that good prognosis was strongly dependent on the TNM stage of recurrent disease at the time of surgical salvage, weakly dependent on the site of disease and not depend-ent on the time to recurrence after initial therapy.
Table 4 Multivariate analysis of the effect of clinico-pathological factors on OS in recurrent laryngeal carcinoma patients
Variables OS
Odds ratio 95% CI P values
Model A
Age 1.306 0.859–1.986 0.212
Smoking index 1.118 0.731–1.709 0.607
Grade 1.235 0.903–1.690 0.186
Primary site 0.934 0.648–1.345 0.712
Initial T stage 1.821 1.154–2.875 0.010
Nodal status 1.599 1.005–2.542 0.047
Extent of the recurrence 1.310 0.946–1.812 0.104
Suitable for surgery 0.401 0.264–0.610 <0.001
Disease-free interval 0.806 0.540–1.203 0.292
Model B
Age 1.416 0.932–2.153 0.103
Smoking index 1.369 0.901–2.080 0.141
Grade 1.275 0.934–1.740 0.127
Primary site 0.871 0.598–1.268 0.471
Initial T stage 2.169 1.420–3.314 <0.001
Nodal status 2.060 1.317–3.223 0.002
Model C
Disease-free interval 0.699 0.473–1.033 0.073
Suitable for surgery 0.358 0.240–0.535 <0.001
Extent of the recurrence 1.868 1.399–2.495 <0.001

Page 7 of 7
Original research study
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Jin T, Lin H, Lin HX, Cai XY, Wang HZ, Hu WH, Guo LB, Zhao JZ. Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study. Head Neck Oncol. 2013 Feb 06;5(2):10.
Our results showed that 92.8% patients had a locoregional recur-rence, which accounted for the high rate (71.0%) of salvage surgery. Our rate of salvage surgery was compara-ble with that reported by Lacy et al. (rate of salvage surgery = 78%)15 and Brenner et al. (rate of salvage surgery = 69%)14. However, the rate was much higher than that reported by Yuen et al. (rate of salvage surgery = 21% only)4. Salvage surgery is generally considered to be the first option if the recurrent disease is resectable and the patient is able to undergo the required surgery. Fortunately, due to natural barriers to tumour spread, the ability to remove the entire larynx without threatening vital function and the relatively early onset of symptoms associated with recurrent disease, surgical salvage is highly successful17. The relationship between salvage surgery and OS has been examined in many patient series; this includes the results of studies conducted by Brenner et al.14 (76% patients who underwent salvage surgery were alive at the time of their analysis compared with 35% of those with inoperable recurrent disease, P < 0.05) and Yuen et al.4 (42% 5-year survival rate for patients who underwent surgery for recurrence compared with 2% of those who did not, P < 0.05). These results were substantially confirmed by our study, in which the estimated 5-year survival rate of the patients suitable for salvage surgery was 55.8%, which was much higher than those who were unsuitable for sal-vage surgery (17.4% only, P < 0.001).
The major criticism of retrospec-tive studies is that the data collected were not originally designed for a research application. Therefore, some factors responsible for the ultimate treatment outcome might be omitted in the analysis, thereby contributing to bias. Such censure correctly refers
to the present study, in which the data were heterogeneous and of lesser quality according to present stand-ards. Considering these factors, one should realize that conclusions from this study should be validated by future projects.
ConclusionAbove all, our data suggest that initial lower T stage, no initial cervical lymph node metastasis, only local recurrence and patients suitable for salvage sur-gery are favourable prognostic factors for OS of patients with recurrent laryn-geal cancer.
AcknowledgementsThis work was supported by the Excellent Talents Project of Zhejiang Cancer Hospital, P. R. China (To: T Jin, No. 2013).
References1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010 Sep–Oct;60:277–300.2. Barthel SW, Esclamado RM. Primary radiation therapy for early glottic cancer. Otolaryngol Head Neck Surg. 2001 Jan; 124(1):35–9.3. The Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med. 1991 Jun;324:1685–90.4. Yuen APW, Wei WI, Ho CM, Lam LK. Result of surgical treatment of advanced laryngeal carcinoma: patterns of failure. In: Smee R, Bridger GP, editors. Laryngeal cancer. Amsterdam: Elsevier Science BV; 1994. p.518–21.5. Lefebvre JL, Chevalier D, Luboinski B, Kirkpatrick A, Collette L, Sahmoud T. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organi-zation for Research and Treatment of Cancer phase III trial. EORTC Head and Neck Cancer Cooperative Group. J Natl Cancer Inst. 1996 Jul;88:890–9.
6. Marshak G, Brenner B, Shvero J, Shapira J, Ophir D, Hochman I, et al. Prognostic factors for local control of early glottic cancer: the Rabin Medical Center retrospective study on 207 patients. Int J Radiat Oncol Biol Phys. 1999;43(5):1009–13.7. Rübe C, Micke O, Grevers G, Rohloff R, Kaufmann H, Busch M, et al. Primary radi-otherapy of laryngeal carcinoma. An anal-ysis of the therapeutic results and of the relapse behavior in 283 patients. Strahl-enther Onkol. 1997 Feb;173(2):83–90.8. Soo KC, Shah FP, Gopinath KS, Gerold FP, Jaques DP, Strong EW. Analysis of prog-nostic variables and results after supraglot-tic partial laryngectomy. Am J Surg. 1988; 156:301–9.9. Bocca E, Pignataro O, Oldini C. Supraglot-tic laryngectomy: 30 years of experience. Ann Otol Rhinol Laryngol. 1983;92:14–21.10. Mittal B, Marks JE, Ogura JH. Trans-glottic carcinoma. Cancer. 1984 Jan;53(1): 151–9.11. Davidson J, Keane T, Brown D, Freeman J, Gullane P, Irish J, et al. Surgical salvage after radiotherapy for advanced laryngopharyngeal carcinoma. Arch Otolar-yngol Head Neck Surg. 1997 Apr;123(4): 420–4.12. Kaplan EL, Meier P. Non-parametric estimation from incomplete observations. J Am Statist Assoc. 1958;53:457–81.13. Cox DR. Regression models and life tables. JR Stat Soc Ser B. 1972;34:187–220.14. Brenner B, Marshak G, Sulkes A, Rakowsky E. Prognosis of patients with recurrent laryngeal carcinoma. Head Neck. 2001;23:531–5.15. Lacy PD, Piccirillo JF. Development of a new staging system for patients with recurrent laryngeal squamous cell carci-noma. Cancer. 1998 Sep;83(5):910–7.16. Goodwin WJ. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: When do the ends justify the means? Laryngoscope. 2000 Mar;110(93 Suppl): 1–18.17. Arnold DJ, Goodwin WJ, Weed DT, Civantos FJ. Treatment of recurrent and advanced stage squamous cell carcinoma of the head and neck. Semin Radiat Oncol. 2004;14:190–5.