Traumatic Brain Injuries: Pathophysiology, Treatment and Prevention
42
Traumatic Brain Injuries: Pathophysiology, Treatment and Prevention
-
Upload
medicineandhealthneurolog -
Category
Health & Medicine
-
view
11.753 -
download
0
description
Transcript of Traumatic Brain Injuries: Pathophysiology, Treatment and Prevention

Traumatic Brain Injuries: Pathophysiology, Treatment and
Prevention

2
Disclaimer
The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of the Army, Department of Defense, or U.S. Government.

3
Defense and Veterans Brain Injury Center (DVBIC)
• DVBIC, founded in 1991 as the Defense and Veterans Head Injury Program (DVHIP), a congressionally funded DoD-VA Disease Management Program.
• The DVBIC mission:– conduct clinical research– ensure optimal clinical care– education for military, veterans, and their families.
• Military Sites: WRAMC, NMCSD, WH-BAMC• VAMC’s – Richmond, Minn, Palo Alto, Tampa• civilian community reentry programs – Virginia Neurocare and
Laurel Highlands (Western Penna)

4
Mechanisms of Injury
Traumatic Brain Injury
Blunt(Closed) Penetrating
Explosion Fall GSW Stab Blast Fragment
Motor vehicle crashes (MVC)

5
Traumatic Brain InjuryDescription
Severity GCS LOC PTAMild 13–15 <20 min-1 hr <24 hr
Moderate 9–12 1 – 24 hrs. > 24 hrs. - <7days
Severe 3–8 >24 hrs. >7 days
GCS = Glasgow Coma ScaleLOC = Loss of consciousnessPTA = Posttraumatic amnesia

6
American Congress of Rehabilitation Medicine: Mild Traumatic Brain Injury
(MTBI) Definition
A traumatically induced physiological disruption of brain function manifested by at least one of these symptoms:• Loss of consciousness < 30 minutes• Loss of memory for events immediately before
(retrograde amnesia) or after the accident (Post Traumatic Amnesia <24 hours)
• Any alteration in mental state at the time of the injury (dazed, disoriented, confused)
• Presence of focal neurological deficits • If given, GCS score > 13
Kay, et al., 1993

7
Relative Proportion of Levels of Care for TBISource: CDC: Traumatic Brain Injury in the United States, October 2004
50,000 Deaths
235,000Hospitalizations
1,111,000Emergency Department Visits
???Other Medical Care or No Care

8
Head Injury in the U.S. Military
0
50
100
150
200
250
15-17 18-24 25-34 35-44
Males (Active Duty)
Males (Otherbeneficiaries)Females (Active Duty)
Females (Otherbeneficiaries)
Ommaya AK, Ommaya AK, Dannenberg AL, Salazar AM. Causation, incidence, and costs of traumatic brain injury in the U.S. Military Medical System. J Trauma. 1996

9
Traumatic Brain Injury (TBI) Epidemiology: Incidence
From D. Hovda, UCLA BIRC Program (modified from Kraus JF, et. al. 1996 and Durkin MS, et. al. 1998)
Age (years)
Incid
ence
(cas
es/1
00,0
00)
0
50
100
150
200
250
300
350
400
450
0 10 20 30 40 50 60 70
San Diego, 1981Rhode Island, 1979-80Bronx, 1980-81Virginia, 1978Manhattan, 1998

10
0
50
100
150
200
250
300
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Fiscal Year
Inci
denc
e R
ate/
100,
000
Pers
onne
lIncidence of TBI-Related HospitalizationsAmong Active Duty US Army Personnel
(Ivins, et al, Neuroepidemiology, 2006)

11
Mechanisms of Injury
Diffuse Axonal Contra coupPenetrating Gun Shot Wound
From the Centre for Neuro Skills

12

13

14

15
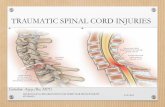
Pathophysiology of Injury
• Primary Injury: Function of energy transmitted to brain– Very little can be done by health care providers to influence– Command enforcement of personal protection
• Helmets, Seatbelts
• Secondary Injury: Function of damage to brain from systemic physiology– Systemic
• Hypotension: Acute and easily treatable• Hypoxia: Acute and easily treatable• Fever and Electrolyte Imbalances
– Seizures– Intracranial Pressure Can Lead to Herniation

16
Neuropathology of Closed TBI
Primary Injury: Contusions/HemorrhagesDiffuse Axonal Injury (DAI)
Secondary Injury (Intracranial): Blood Flow and Metabolic Changes Traumatic HematomasCerebral EdemaHydrocephalusIncreased Intracranial Pressure

17
Severe and Penetrating Brain Injury: Clinical
Challenges• Craniectomy• Vascular Complications
• 47.4% had traumatic cerebral vasospasm. Majority were blast related injury (Armonda, R., Bell, R., Vo,A., et al 2006. Wartime traumatic cerebral vasospasm: Recent review of combat casualties. Neurosurgery, 59(6), 1215 -1225.)
• Autonomic Instability/Sympathetic Storms• Infectious Complications
Archives of Physical Medicine and Rehab (Invited Manuscript) R. Riechers, et al.

18

19
Brain-Behavior Relationshipsand Regional Cortical Vulnerability to TBIFigure adapted from Arciniegas and Beresford 2001)
Dorsolateral prefrontal cortex(executive function, including sustained and complex attention, memory retrieval, abstraction, judgement, insight, problem solving)
Amygdala (emotional learning and conditioning, including fear/anxiety)
Anterior temporal cortex(memory retrieval, sensory-limbic integration)
Ventral brainstem (arousal, ascending activation of diencephalic, subcortical, and cortical structures)
Hippocampal-Entorhinal Complex (declarative memory)
Viewed on coronal MRI
Orbitofrontal cortex(emotional and social responding)
(

20
Postconcussion Symptoms (PCS)
SOMATIC• Headache• Dizziness• Fatigue – for physical
and mental• Visual Disturbances• Sensitivity to Noise and Light
COGNITIVE• Decreased Concentration• Memory ProblemsNEUROPSYCHIATRIC• Anxiety• Depression• Irritability• Mood Swings• Sleep Disturbances

21
Post Concussive Symptoms in Mild TBI
• Natural history is recovery within weeks/months (Levin 1987)
• A small percentage will have persistent symptoms (Alexander, Neurology 1995)
• Repeat concussions – more morbidity (Collins, et al, Neurosurgery 2002)
• Educational interventions effective in reducing symptoms (Ponsford, et al. 2002)

22
Cognitive Changes
Attention/Concentration
Speed of Mental Processing
Learning/Information Retrieval
Executive Functions (e. g., Planning, Problem Solving, Self Monitoring) May see judgment problems, apathy, inappropriate behaviors

23
fMRI study of MTBI and Memory (McAllister, et
al, 2000)

24
Neurometabolic Changes and Concussion (Hovda et al, 1998)

25
Simple Reaction Time Warden D, Bleiberg J, Cameron K, et al, Neurology, 2001
200
220
240
260
280
300
320
340
360
Baseline 1 hour post 4 days post
p < 0.05

26
Concussion:Time to Recovery
Math Scores Percent Change from Baseline
-20-15-10-505
10152025303540
Baseline 0-23 Hours 1-2 days 3-7 days 8-14 days
Intervals
Perc
ent C
hang
e
Controls
Concussed
p=.05
Bleiberg J., et al. Neurosurgery, 2004.

27
Post Deployment TBI Questions
Did you have any injury(ies) during your deployment from any of the following? (check all that apply):
1. Fragment2. Bullet3. Vehicular (any type of vehicle, including airplane)4. Fall5. Blast (Improvised Explosive Device, RPG, Land mine, Grenade, etc.)6. Other specify: Did any injury received while you were deployed result in any of the following? (check all that apply):1. Being dazed, confused or “seeing stars”2. Not remembering the injury3. Losing consciousness (knocked out) for less than a minute4. Losing consciousness for 1-20 minutes5. Losing consciousness for longer than 20 minutes6. Having any symptoms of concussion afterward (such as headache, dizziness, irritability, etc.)7. Head Injury8. None of the above (any of 1-5 suggest a MTBI diagnosis)

28
Post-Deployment TBI Screening
• DVBIC has worked with multiple sites screening returning war fighters
• Approximately 10-20% war fighters had a TBI while in theater (Army Times-Sept 5, 2005)
• Virtually all were mild TBI
• Most are now asymptomatic

29
Involved in/exposed to/experienced:
Blast, vehicular crash, fall, GSW to head/face and/or neck, (including superficial
wounds): Yes
TBI Symptom Screening/Interview:Any LOC, AOC, PTA and symptoms endorsed on the Post Concussive
Symptom Checklist
Cognitive, physical, and/or emotional symptoms or findings thought to be due to TBI
Cognitive, physical, and/or emotional symtoms or findings thought to be due to PTSD or other psychiatric disorder
Medical Evaluation
Yes
WRAMC TBI Screening Flow Chart
Note: Both may be present at this level

30
Walter Reed OIF/OEF
TBI Experience (1/03 to 4/05) N=433 Hospitalized patients with TBI• 68% of injuries were due to
explosion/blast
• 88.5% were closed TBI
• Post Traumatic Amnesia (PTA) < 24 hours: 43%
Warden et al., Journal of Neurotrauma 2005; 22:1178

31
Walter Reed OIF/OEF TBI Experience (cont.)
• Complications - 14% shock; 9.5% hypoxia; 25% skull fracture; 18.7% subdural hematoma; and 1.5% epidurals
• 6% had seizures• 19% had limb amputations; lower extremity most common• 91 % reported post concussive symptoms:
– headache (47%)– memory deficits (46%)– irritability/aggression (45%)– attention/concentration difficulties (41%)
• Of 43% with a psychiatric symptoms noted, depression was the most common (27%).
Warden et al., Journal of Neurotrauma 2005; 22:1178

32
Military Context

33
Blast Wave Physics
Courtesy of Keith Prusaczyk, Ph.D.

34
Evaluation of MTBI in the field
• Medic obtains history using• Military Acute Concussion Evaluation
(MACE)• New Clinical Practice Guideline drawing
on sports concussion and operational experts released 22 Dec 06– includes the SAC – Standard Assessment of Concussion (McCrea 2000)

35
Conclusions Regarding PTSD
in TBI Patients
• Studies suggest that PTSD following TBI does occur, but may be modified by the brain injury.
• Intrusive memories are less common in individuals; when present, highly predictive of PTSD
• PTSD is more likely in mild TBI than severe TBI
(Bombardier, C., et al. 2006. J Neuropsychiatry Clin Neurosci: Posttraumatic Stress Disorder Symptoms During the First Six Months After Traumatic Brain Injury: 18:4:501-508)

36
Treatment Areas
• Education and support for the patient’s family
• Rest and avoidance of another injury• Individual and group therapies• Medication including symptom mgt• Rehab (acute, sub-acute, community re-
entry)

37
Guidelines for the Pharmacologic Treatment of Neurobehavioral
Sequelae of TBI
• Symptom Management • Addresses 3 topic areas
– Aggression– Cognitive disorders– Affective disorder/Anxiety/Psychotic disorders Warden D., Gordon B., McAllister T., et al (2006). Guidelines for the
pharmacologic treatment of neurobehavioral sequelae of traumatic brain injury. Journal of Neurotrauma, 10(23), 1468-1501.

38
Guidelines for the Pharmacologic Treatment of Neurobehavioral Sequelae of TBI
• Despite reviewing a significant number of studies on drug treatment of neurobehavioral sequelae after TBI, the quality of evidence did not support any treatment standards and few guidelines due to a number of recurrent methodological problems.
• Guidelines were established for the use of methylphenidate in the treatment of deficits in attention and speed of information processing, as well as for the use of beta-blockers for the treatment of aggression following TBI.
• Options were recommended in the treatment of depression, bipolar disorder/mania, psychosis, aggression, general cognitive functions, and deficits in attention, speed of processing, and memory after TBI.

39
Prevention Areas
• Rest to prevent re-injury• Education regarding risk taking behaviors• Neurometabolic changes and concussion • Helmets

40
Questions?

41
Referral to Defense and Veterans Brain Injury Center (DVBIC)
Toll Free Referral and Information Line: 1-800-870-9244 DSN 662-6345
Web Site: www.DVBIC.org

42
DVBIC Headquarters, WRAMC
• Amy Craig, MBA• Pannakal David, MD• COL James Ecklund, MC• Jamie Fraser, MPH• Louis French, PsyD• Phil Girard, MS• Kathy Helmick, RN, CRNP• Maraquita Hollman, BA• Ronnell Iandolo, RN• Angela Ibrahim, MPA, CRA• Brian Ivins, MA • COL Robert Labutta, MC• COL Geoff Ling, MC
• Wei Lu, RN• Lisa Moy Martin, RNC• Silvia Massetti, MSW • Kathryn Misner, PA-C• Sonal Pancholi, PhD• Glenn Parkinson, MSW, MA• CPT Ron Riechers, MC• Karen Schwab, PhD • Alice Marie Stevens, MA• Katie Sullivan, MS• Jose Valls, LPN• Jehue Wilkinson, LPN• Michael Wilmore, PA-C• Cecilie Witt, BA