
Traumatic Aortic Disruption SVS Clinical Practice · PDF file27 comparative observational...
5
1 UCSF Vascular Symposium 2012 April 27, 2012 W. Anthony Lee, MD, FACS Director of Endovascular Services Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures Cook Medical: research grant support, consulting, honorarium, travel stipend Bolton Medical: consulting, honorarium This presentation will discuss off-label use of medical devices Traumatic Aortic Disruption Mechanism: Acceleration/deceleration injury Intimal tear Transmural disruption Location: Ligamentum arteriosum Associated poly-trauma (long bone, pelvic fractures, solid organ injury, closed head injury, pulmonary contusion) Outcome associated with early hemodynamic (in)stability SVS Clinical Practice Guidelines Systematic review and meta-analysis (Knowledge and Encounter Research Unit, Mayo Clinic) 7768 patients in 139 studies 112 case series (>10 cases): median 15 cases 27 comparative observational nonrandomized studies 77% males Mean f/u: 2 years Non-operative Open Endovascular Age (yrs) 39 36 39 ISS 36 34 40 Time interval to tx(hrs) --- 16 19 LSA coverage (%) --- --- 30
Transcript of Traumatic Aortic Disruption SVS Clinical Practice · PDF file27 comparative observational...
1
UCSF Vascular Symposium 2012April 27, 2012
W. Anthony Lee, MD, FACSDirector of Endovascular Services
Christine E. Lynn Heart and Vascular InstituteBoca Raton, Florida
Disclosures� Cook Medical: research grant support,
consulting, honorarium, travel stipend� Bolton Medical: consulting, honorarium� This presentation will discuss off-label use
of medical devices
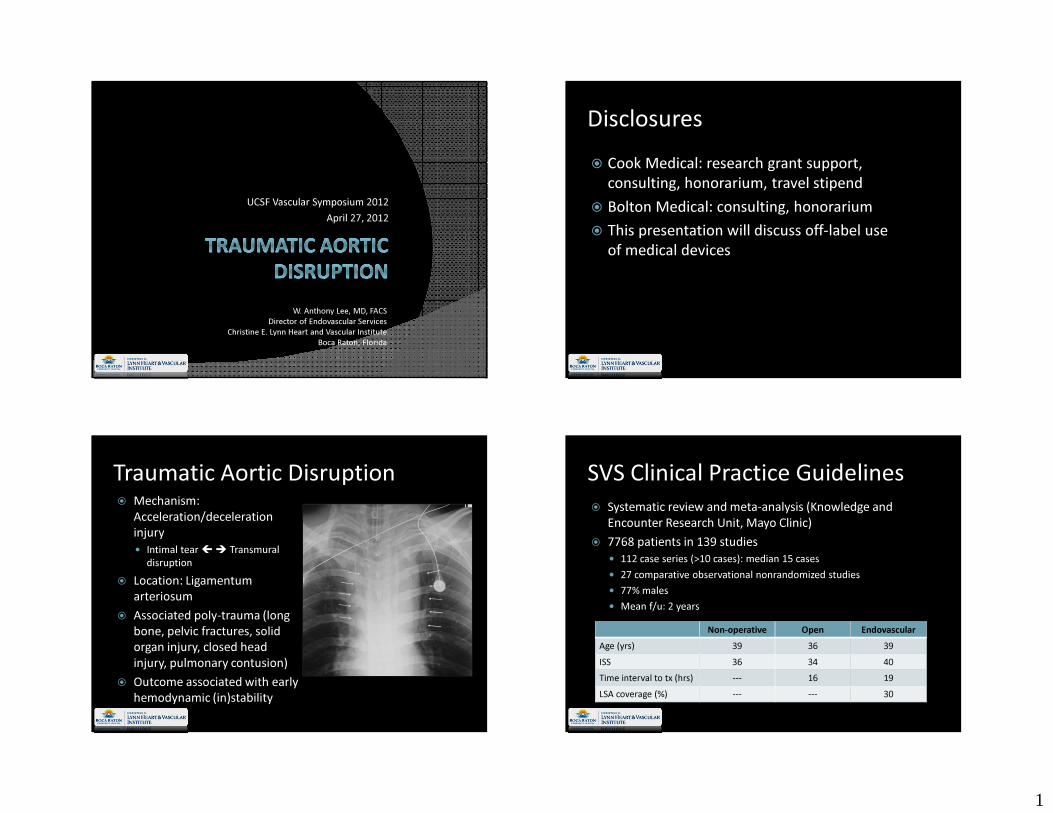
Traumatic Aortic Disruption� Mechanism:
Acceleration/deceleration injury� Intimal tear �� Transmural
disruption� Location: Ligamentum
arteriosum� Associated poly-trauma (long
bone, pelvic fractures, solid organ injury, closed head injury, pulmonary contusion)� Outcome associated with early
hemodynamic (in)stability
SVS Clinical Practice Guidelines� Systematic review and meta-analysis (Knowledge and
Encounter Research Unit, Mayo Clinic)� 7768 patients in 139 studies� 112 case series (>10 cases): median 15 cases� 27 comparative observational nonrandomized studies� 77% males� Mean f/u: 2 years
Non-operative Open EndovascularAge (yrs) 39 36 39ISS 36 34 40Time interval to tx (hrs) --- 16 19LSA coverage (%) --- --- 30

2
Systematic Review: Key Findings� Mortality (p<0.01)� Non-operative 46%� Open 19% (correlated w/ ISS)� Endovascular 9%
Non-operative
Open Endo p
Stroke (%) 2 3 3 NSSCI (%) 3 9 3 0.01Renal failure 5 8 3 0.01Infections 5 13 5 0.01Secondary procedures --- 6 10 0.07
Failures of TEVAR� Endoleak 60%� Stent graft collapse 11%� Intraoperative rupture 2%� Iliac artery injury 1%� Aortic perforation 1%� Unspecified 25%
Comparative Analysis: Open vs. TEVAR� 27 studies� Mortality: RR 0.61 (0.46-0.80)� SCI: RR 0.34 (0.16-0.74)� For BOTH open and TEVAR� Longer lag time associated with
improved survival� No difference between urgent and
delayed repair
Consensus Opinion on Select Issues (Grade 2, Level C)� Most repairs should be performed
<24 hours� Expectant management for type I
(minimal aortic injury/periadventitial hematoma)� TEVAR suitable for young patient
with good anatomy� Selective SCA revascularization for
zone 2 deployments in traumatic TEVAR

3
Consensus Opinion on Select Issues (Grade 2, Level C)� Routine heparin anticoagulation during
TEVAR� Spinal drainage NOT required� General anesthesia preferred� Open (vs. percutaneous) femoral exposure� No consensus on optimal follow-up strategy
Conclusion� Based on the systematic review of the
available literature, the Committee suggeststhat endovascular repair of traumatic thoracic aortic injuries be performed preferentially over open surgical repair or non-operative management (Grade 2, Level C)
Technical Issues� Optimal TAD imaging� Endograft sizing� Aortic growth� Left subclavian artery management� Arch conformation
Optimal TAD Imaging� H/N/C/A/P CTA� Cardiac gating (aortic pulsatility ↓ with
class III/IV shock)� Posterior (vertebral) circulation� Access� IVUS� Equivocal CTA findings� More sensitive than angiography� (TEE/angiography)
4
Endograft Sizing� Aortic diameter and volume status
of polytrauma victim� Aortic diam ↓ 38% (class III/IV shock)� Aortic diam ↑ 13% a�er resuscita�on� Endograft infolding associated with
oversizing� 60% related to traumatic TEVAR � 0.4% overall incidence� 33% device oversizing
Aortic Size Increase over Time� Forbes et al (J Vasc Surg, July 2010)� 21 patients� Prox thoracic aortic dilation: 0.74-0.83 mm/year� Hartley et al (Ann Vasc Surg, Sept 2009)� 1000 Chest CTA examined� Variables: age, gender, HTN, COPD, race, DM,
tobacco� Prox desc TA: 22.9 mm (<40 yrs) vs. 27.1 mm
(≥40 yrs)
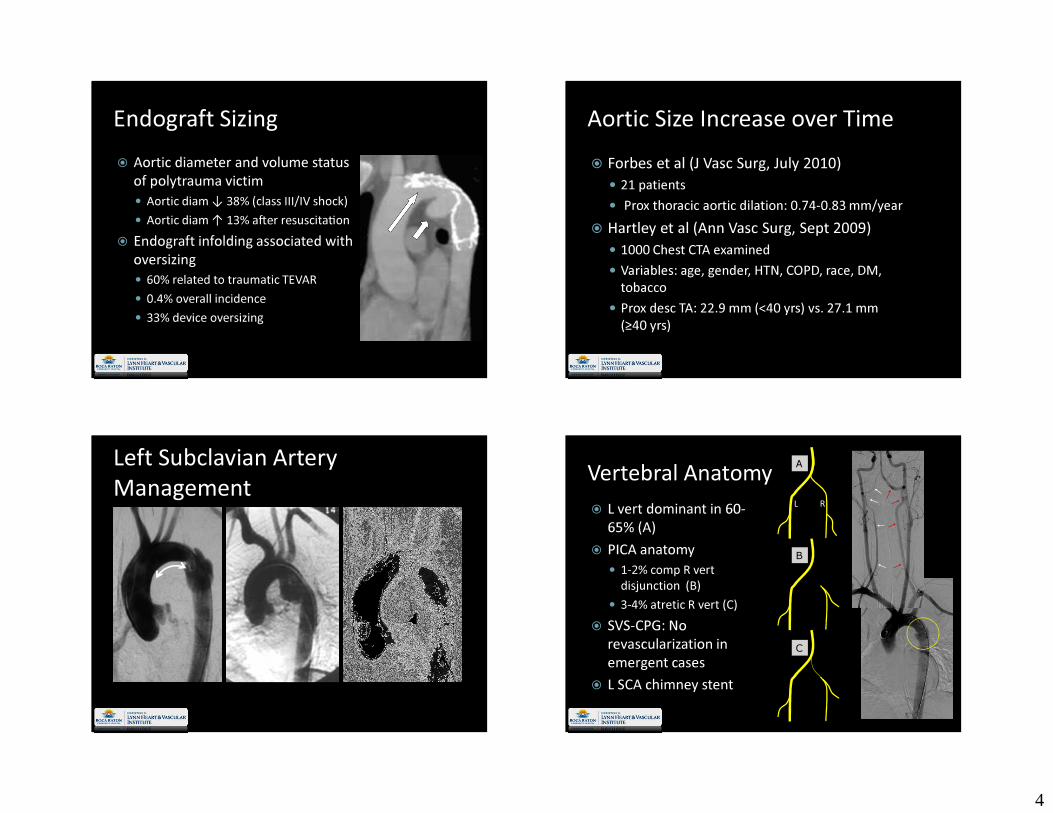
Left Subclavian Artery Management Vertebral Anatomy
� L vert dominant in 60-65% (A)� PICA anatomy� 1-2% comp R vert
disjunction (B)� 3-4% atretic R vert (C)� SVS-CPG: No
revascularization in emergent cases� L SCA chimney stent
A
C
B
L R
5
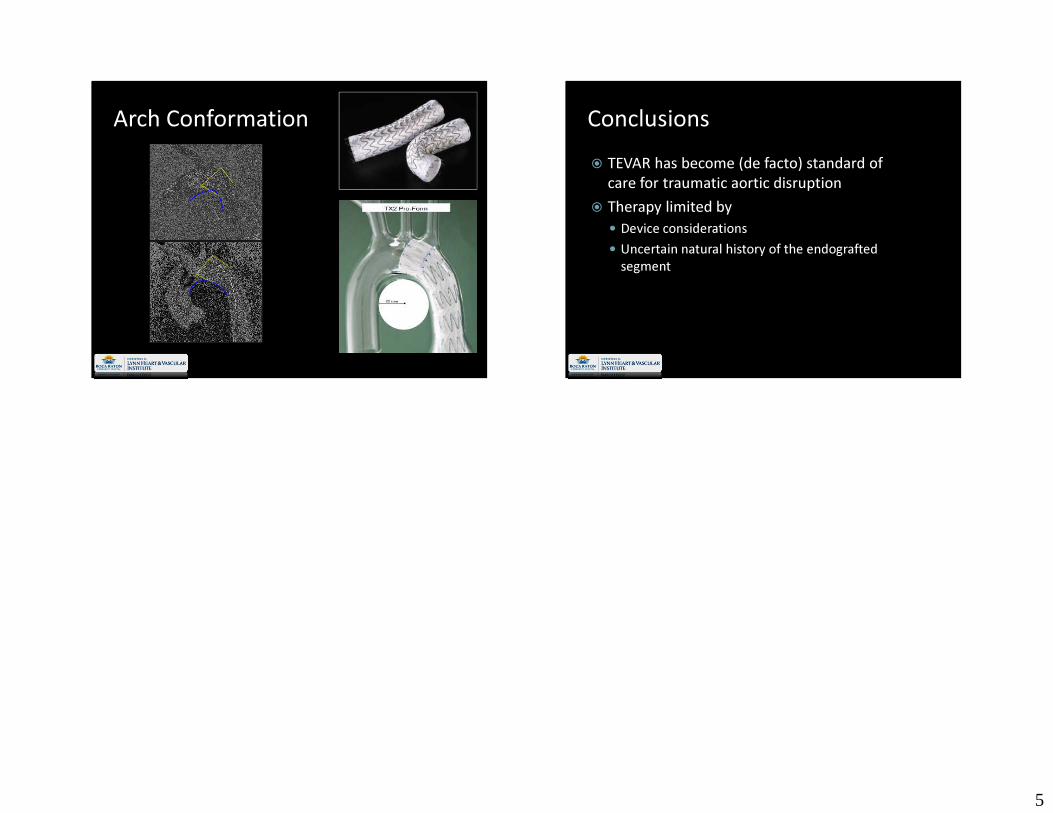
Arch Conformation Conclusions� TEVAR has become (de facto) standard of
care for traumatic aortic disruption� Therapy limited by � Device considerations� Uncertain natural history of the endografted
segment










![Svs Agencies[1]](https://static.fdocuments.us/doc/165x107/577cc7a71a28aba711a191e1/svs-agencies1.jpg)







