Trauma “This ain’t ER”
72
Trauma “This ain’t ER” Ben Zarzaur, MD UNC Department of Surgery Section of Trauma and Critical Care
description
Trauma “This ain’t ER”. Ben Zarzaur, MD UNC Department of Surgery Section of Trauma and Critical Care. What is trauma?. Real Life & Death. What is trauma?. Trauma Epidemiology. Years of Potential Life Lost. MMWR 1982;31,599. Mechanisms of Injury: Blunt Trauma. MVC - PowerPoint PPT Presentation
Transcript of Trauma “This ain’t ER”

Trauma“This ain’t ER”
Ben Zarzaur, MD
UNC Department of Surgery
Section of Trauma and Critical Care

What is trauma?


Real Life & Death

What is trauma?

Trauma Epidemiology

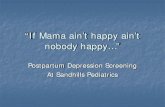
Years of Potential Life Lost
18.00%
16.40%
24.80%
40.80%
Injury
Cancer
Heart Disease
All Other Diseases
MMWRMMWR 1982;31,599. 1982;31,599.

Mechanisms of Injury: Blunt Trauma
• MVC
• Pedestrian vs Vehicle
• Falls

Mechanisms of Injury:Special Situations
• Explosions– Blunt + penetrating + burns
• Burns• Crush injuries• Drowning• Hypothermia/ exposure

Compression injury
• Frontal brain contusion
• Pneumothorax • Rupture of Left
hemidiaphragm • Small bowel
rupture• Chance fracture

Deceleration Injury
• Aortic tear– Fixed descending
aorta– Mobile arch
• Acute subdural brain hematoma
• Kidney avulsion• Splenic pedicle

Mechanisms of Injury: Penetrating Trauma
• Gun shot wounds• Stab wounds• Impalement

Gun Shot Wounds: Mechanism• Energy transfer
– Shape/size of bullet– Distance to target
• Velocity (most important)– Kinetic energy = (Mass × Velocity2 )/2
• Surface area distributed– Tumble and yaw– Fragmentation
• Anatomy– Viscoelasticity
• Muscle• organs

Stab wounds• Mechanism
– Blunt: Crush injury – Sharp:Tissue disruption
• Extent of Injury– Weapon size, length,
sharpness, penetration
• Severe injury– Chest and abdomen– 4+ wounds


What happens when the
patient comes to a Level I
Trauma Center?

Trauma Team“Doin it 24/7”
• ED Physicians• Anesthesiology• Surgeons
– General and Trauma and Critical Care– Neurosurgery– Orthopedics
• Medical Students• Nurses• Radiology Techs• Radiologists


What happens when this patient comes to the ER where you are
moonlighting?


What the heck do I do now?

Don’t panic!

Trauma is not rocket science!

• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong

Initial Assessment: Prerequisites
• Wide-angled view
• Pattern recognition skills
• Ability to triage and set priorities
• Organized structure

Trauma is not rocket science!

ABCDEF

Initial Assessment: Primary Survey
• A = Airway• B = Breathing • C = Circulation• D = Disability• E = Exposure• F = Fracture

• Clear & establish a good airway– Consider intubation
for coma, shock, and thoracic injuries
• C-spine stabilization
Initial Assessment: Airway


Airway: Cricothyrotomy

Initial Assessment: Breathing
• Chest excursion & breath sounds– Flail chest
• Pneumothorax– Open – Tension
• Massive Hemothorax



Initial Assessment: Circulation• Perfusion (mental status, skin, pulse)• Control bleeding with pressure• Pericardial Tamponade
– Beck’s Triad
• Establish 2 large bore (16G or larger) IV’s in upper extremity peripheral veins
• Resuscitate with Lactated Ringers– After 4 L think about resuscitation with
blood

Initial Assessment: Disability
• Neurologic status– Glasgow Coma Scale
• Eye• Motor-best predictor of long term
outcome• Verbal
– Spinal Cord Injury

Initial Assessment: Exposure
• Remove clothes
• Temperature– warm blankets
• Finger and tube in every orifice
• Maintain full spine precautions– Log Roll

Initial Assessment: Fracture• Stabilize Fractures
• Relocate dislocated joints
• Reassess pulses

Secondary Survey• Patient history• Head to toe physical exam• Radiography
– Lateral C-spine, C-xray, pelvis– One cavity above/below entrance/exit wounds– FAST
• Urinary bladder drainage• NGT• Blood sampling/monitoring

Does this patient need to go to the
OR ?


Penetrating Abdominal Trauma
GSW KSW
OR HD Unstable HD Stable/No peritonitis
OR Peritoneal Penetration
Positive Negative
OR Observation
Penetrating Abdominal Trauma

Blunt Trauma
Peritonitis Indeterminate
OR HD Stable HD Unstable
CT FAST/DPL
Positive Negative
OR Keep Looking
Blunt Abdominal Injuries

Liver Injury

Liver Injury
• blunt or penetrating injury • mortality: 10 - 20% • may be associated with right lower rib
fracture• Signs / Symptoms
– RUQ pain abdominal wall spasm ,guarding hypoactive or absent BS signs of hemorrhage


Liver Injury: ManagementBlunt Injury
• ICU monitoring– For more severe injuries– Serial HCT
• Floor Monitoring– Less severe injuries– Serial HCT
• OR if patient becomes unstable or requires excessive blood transfusions

Surgical Management

Surgical Management

Surgical Management

Spleen Injury

Splenic Injury
• Blunt or Penetrating • Signs / Symptoms
– LUQ pain – Kehr’s sign– involuntary guarding hypoactive or absent BS– signs of hemorrhage– point tenderness


Splenic Injury Management
• ICU monitoring– Serial Physical exams– Serial HCT
• Floor Monitoring– Not indicated at this time
• Further intervention needed if patient becomes unstable or requires blood transfusion– Embolization vs Splenectomy







Splenectomy
• Complications– postsplenectomy infection
• Vaccination
– wound infection – subdiaphragmatic abscess – pulmonary complications– hypovolemic shock

Stomach and Small Bowel Injury
• Stomach & Small Bowel – Blunt vs penetrating
• Diagnosis – Pneumoperitoneum or free fluid on CT scan– small bowel injury may be difficult to detect– Found at laparotomy
• Management– Primary repair or resection

Colon and Rectal Injury• Colon
– Diagnosis • Pneumoperitoneum or free fluid on CT scan• injury may be difficult to detect• Found at laparotomy
– Management• Colostomy vs primary repair
• Rectum– Intraperitoneal- treat as colon injury– Extraperitoneal- primary repair with diversion
• +/- presacral drains

Pancreas & Duodenum
• Diagnosis – often delayed diagnosis – frequently seen together – most often contused due to blunt injury– Seen on CT Scan or at laparotomy– intramural hematoma in wall of duodenum
obstruction bilious vomiting severe abdominal pain distention


Pancreas Injury• Management
– if the result of blunt trauma• nonoperative management NG/OG decompression
serial physical exams monitoring signs of infection controversial - 3 weeks of bowel rest with TPN
– Complications of nonoperative care• pancreatic fistula pseudocyst formation
– Operative management is necessary if: pain fever ileus elevated serum amylase

Duodenal Injury• Management
– For hematoma• NG/OG decompression serial physical
exams monitoring signs of infection– controversial - 3 weeks of bowel rest with TPN
– For perforation• Primary repair with duodenal exclusion• Efferent/Afferent Duodenal tubes

Pelvic Injury
• Introduction– significant blood loss if bilateral
– may settle in retroperitoneal space
– 3% of all fractures
– mortality 8 - 50%
– 2nd most common cause of traumatic death


Pelvic Fracture
• Signs & Symptoms – pelvic instability – pain (suprapubic also) – crepitus – bloody meatus – neurovascular deficits

Pelvis
• Interventions– Stable patient
• analgesia • Repair vs mobilization
– Unstable patient• Immobilize• Ex-fix• Angiography
– embolization