Trauma in Elders handout - cdn.ymaws.com · Acute Care Practice Stacey Maguire, PT, DPT, Neurologic...
85
Trauma In Elders: Applying Evidence to Acute Care Practice Stacey Maguire, PT, DPT, Neurologic Certified Specialist Laura Driscoll, PT, DPT, Geriatric Certified Specialist Shannon Stillwell, PT, DPT, Geriatric Certified Specialist
-
Upload
trinhthien -
Category
Documents
-
view
217 -
download
0
Transcript of Trauma in Elders handout - cdn.ymaws.com · Acute Care Practice Stacey Maguire, PT, DPT, Neurologic...

Trauma In Elders:Applying Evidence to Acute Care Practice
Stacey Maguire, PT, DPT, Neurologic Certified SpecialistLaura Driscoll, PT, DPT, Geriatric Certified Specialist
Shannon Stillwell, PT, DPT, Geriatric Certified Specialist

Disclosures
• The presenters have no potential conflicts of interest to report.

Learning Objectives
• Recall how the aging process leads to physiological changes that compromise the ability of elders to respond to the stress of injury.
• Explain the PT’s role in reviewing medications and recognizing psychosocial issues and their potential impact upon health, impairments, functional limitations, and disabilities.
• Apply a hypothesis driven examination strategy to initial evaluation of an elder after trauma in the hospital setting.
• Appreciate the risk factors for development of delirium, as well as tests for screening and interventions to delirium.
• Create therapeutic interventions of proper intensity to address a variety of common impairments in elders who have been hospitalized after trauma.
• Recognize the value of utilizing standardized tests and outcome measures to help drive clinical decision making.
• Understand the value of developing a patient-centered discharge plan.

Why Geriatric Trauma?

Epidemiology
• Those aged 65 or over.
• The most rapidly growing segment of the population.
• By 2050, this number of geriatric individuals is expected to grow to 2 billion.
• Living longer and leading more active lifestyles.(Tieland, 2017)

Geriatric trauma
Why does trauma happen in older adults?• Leading causes:
• #1 Falls• #2 Motor vehicle accidents
What makes elders unique?• Elders are more susceptible to injury.
• Pre-existent comorbidities• Pre-existent impairments in body structure and function
• Traditional trauma outcomes are not applicable to elders.(Gaebel, 2017; Brooks, 2017)

Geriatric traumaElders are less likely to receive care in trauma centers.• Under triaged = Adverse Outcomes
How prevalent is trauma in elders?• 9th leading cause of death amongst the elderly, BUT:
• 35% of trauma healthcare expenditures(Gaebel, 2017; Brooks, 2017)
What Are the Physiological Changesthat Make Elders Vulnerable?

Physiological Changes
• Connective Tissue Changes• Decreased water content• Increased stiffness• Decreased strength• Decreased cross sectional area and volume
• Joint Structure and Function Changes• Limited healing• High load activities/occupations = OA• Decreased water content in discs• Increased stiffness and decreased ROM
(Guccione, 2011)

• Boney Changes• Increased osteoclast activity, decreased osteoblast
activity• Decreased ability to absorb load• Increased risk of fracture with age
• Muscular Changes• Atrophy of muscle à muscles mass replaced with fat• Steady decline of strength• Slowing of contractile properties
• Type II fast twitch atrophy faster than Type I slow twitch• Decreased force production
• Sarcopenia(Guccione, 2011)

• Cardiovascular Changes• Stiffer myocardium = Decreased pump effectiveness
• Decreased cardiac output• Loss of heart rate variability• Cardiac function declines by 50% by the time we are 80
• Pulmonary Changes• Anatomic, muscular and connective tissue changes • Ineffective pulmonary system• Decreased ability to fight off post-operative complication
• Neurological Changes• Cortical atrophy• Plaque build up
(Sharma, 2006; Vigorito, 2014)
• Other Systyems• Endocrine Changes
• Decreased VitaminD• Decreased Estrogen and Testosterone• Increased Insulin resistance
• Malnutrition• Altered Drug Metabolism
(Guccione, 2011)
So what does this mean for Elders?

Physiological Frailty Phenotype
• Weight Loss
• Exhaustion
• Physical Activity
• Walk Time
• Grip Strength(Bellal, 2014; Fried, 2001)

Application to PT

ICF Model
• Impairments in body functions and structures:
• ROM• Strength/Force Production• Joint Mobility/Integrity• Posture• Endurance
• Activity Restrictions• Impaired Balance• Impaired Gait• Impaired ADLs
• Participation Restrictions• Family roles• Occupational roles• Leisure roles• Loss of independence

Mrs M.• 87 year old female admitted s/p fall down stairs• Found down by her sister
• + Loss of consciousness
• Sustained several injuries• Non-displaced fractures of maxillary wall• L orbital floor fracture, small L subdural hematoma• L 8th and 9th rib fractures.
• Hypotensive on admission
• Found to have urinary tract infection

Past medical/surgical history
• Ventricular arrhythmia s/p pacemaker placement• Mitral regurgitation• Coronary artery disease s/p stents 2014• Congestive heart failure (ischemic cardiomyopathy with reduced
ejection fraction: 25%)• Hypertension• Hyperlipidemia • Gallstone pancreatitis s/p laparoscopic cholecystectomy • Hard of hearing in right ear• s/p hysterectomy • s/p back surgeries (unknown)

Imaging
• Head CT: small acute L subdural hematoma without evidence of midline shift. Non-displaced fractures of maxillary wall, L orbital floor fracture.
• Chest XR: L posterolateral 8th and 9th rib fractures

Labs
• Positive Urine Culture (Klebsiella Oxytoca)
Test Name Value Reference RangeWBC 8.7 4.0-10.0 K/uLHgb 8.0* 11.2-15.7 g/dLHct 25.4 34-35%Plts 242 150-400Cr 1.3* 0.4-1.1 mg/dLBUN 30* mg/dL

What do we want to learn about Mrs M?

Patient Interview
• Social and Work History
• Living Situation
• Baseline functional and activity level
• Detailed information regarding falls: frequency, symptomatology, situational information
• Medications and management
• Screening for psychosocial considerations (depression, neglect, abuse)

Social / Functional History
• Retired. Previously employed in various jobs. Enjoys crafting.
• Widowed. Lives with son and daughter-in-law. Enjoys time with her twin, who lives in Maine.
• Two story home with 10 steps to enter with bilateral railings.
• Baseline independent ambulation without assistive device. Independent in ADLs. Family assist with IADLs. Independent medication management. Drives short distances. Sedentary.
• +hard of hearing R ear (doesn’t use hearing aide), no visual aides
• History of falls, usually about 2/year, but reports 2 in past 2 weeks.

Patient Interview
• Social and Work History
• Living Situation
• Baseline functional and activity level
• Detailed information regarding falls: frequency, symptomatology, situational information
• Medications and management
• Screening for psychosocial considerations (depression, neglect, abuse)

“Physical Therapist patient/client management integrates an understanding of a patient’s/client’s prescription and nonprescription medication regimen with consideration of it’s impact upon health, impairments, functional limitations, and disabilities.” https://www.apta.org/uploadedFiles/APTAorg/Payment/Medicare/Coding_and_Billing/Home_Health/Comments/Statement_MedicationManagement_102610.pdf
APTA Position Statement

Why is medication management an important consideration with elders?
POLYPHARMACY
• The use of multiple medications by a patient
• Varying definitions of number of medications (range 5-10)
• In a 2003 survey 46% of Medicare beneficiaries were taking 5 or more medications
(Fried et al, 2014)
AGE-RELATED CHANGES
•Increased distribution
•Natural decline of renal and hepatic function
•Larger drug storage and decreased clearance = increased plasma concentrations
•Increased sensitivity

Consequences of Polypharmacy
• Increased health care costs
• Adverse drug reactions
• Drug interactions
• Non-adherence
• Cognitive Impairments
• Falls
• Urinary incontinence
• Poor nutrition
• Functional decline

Polypharmacy and falls
Kojima et al, 2012: • Followed 172 patients for two years and documented fall
occurrence (by self report).• Falls were associated with older age, osteoporosis, number of
comorbid conditions and number of medications. • Number of medications (5 or more) was independent
predictor of falls.

American Geriatric SocietyBeers Criteria:
Potentially inappropriate medications
• Anticonvulsants
• Antipsychotics
• Benzodiazepines
• Eszopiclone, Zaleplon, Zolpidem (Nonbenzodiazepine Hypnotic Agents)
• Tricyclic Antidepressant Agents (TCAs)
• Selective Serotonin Reuptake Inhibitors (SSRIs)
• Opioids (excludes pain management due to recent fracture or joint replacement)
(American Geriatrics Society 2015 Beers Criteria Update Expert Panel)
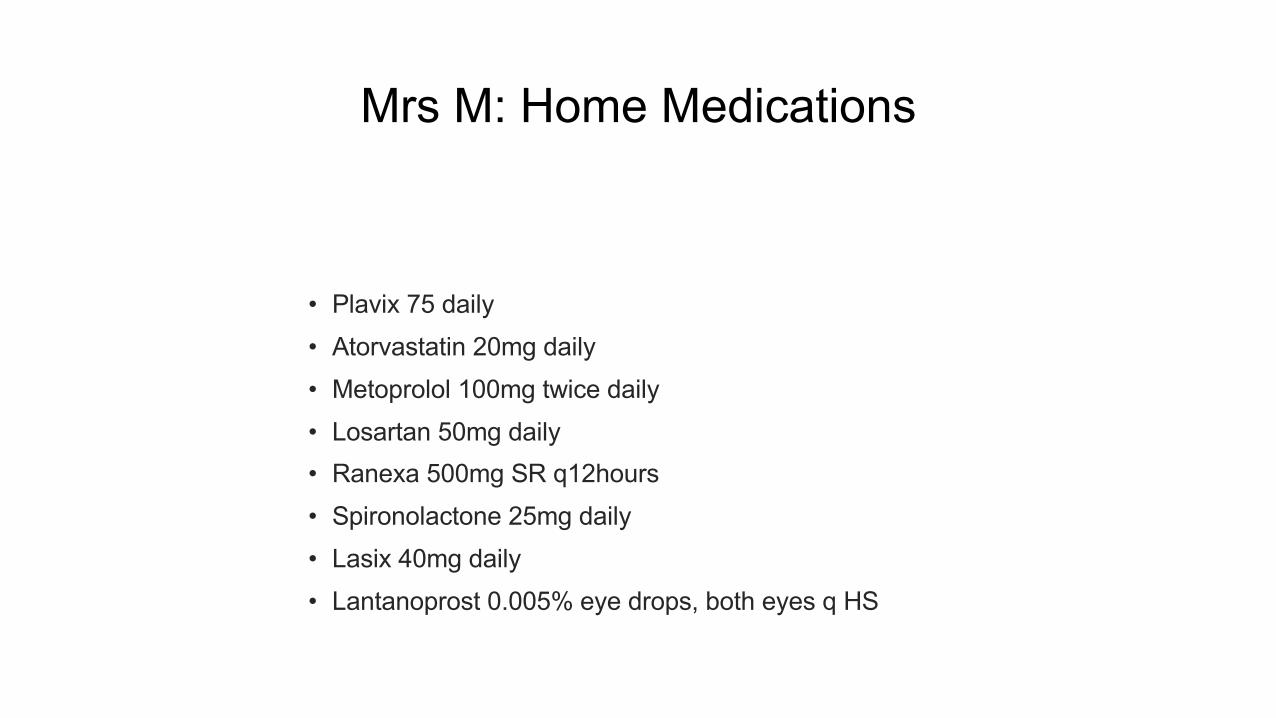
Mrs M: Home Medications
• Plavix 75 daily
• Atorvastatin 20mg daily
• Metoprolol 100mg twice daily
• Losartan 50mg daily
• Ranexa 500mg SR q12hours
• Spironolactone 25mg daily
• Lasix 40mg daily
• Lantanoprost 0.005% eye drops, both eyes q HS

Patient Interview
• Social and Work History
• Living Situation
• Baseline functional and activity level
• Detailed information regarding falls: frequency, symptomatology, situational information
• Medications and management
• Screening for psychosocial considerations (depression, neglect, abuse)

Depression
> 1 in 10 elders in the US has depression.• This frequency increases in elders with chronic illness.
(Steffens, 2009)
Associated with poor physical performance• 970 non-depressed elders in Italy, followed for 4 years• Associated identified between poor performance at baseline
and the development of depression(Veronese et al, 2017)
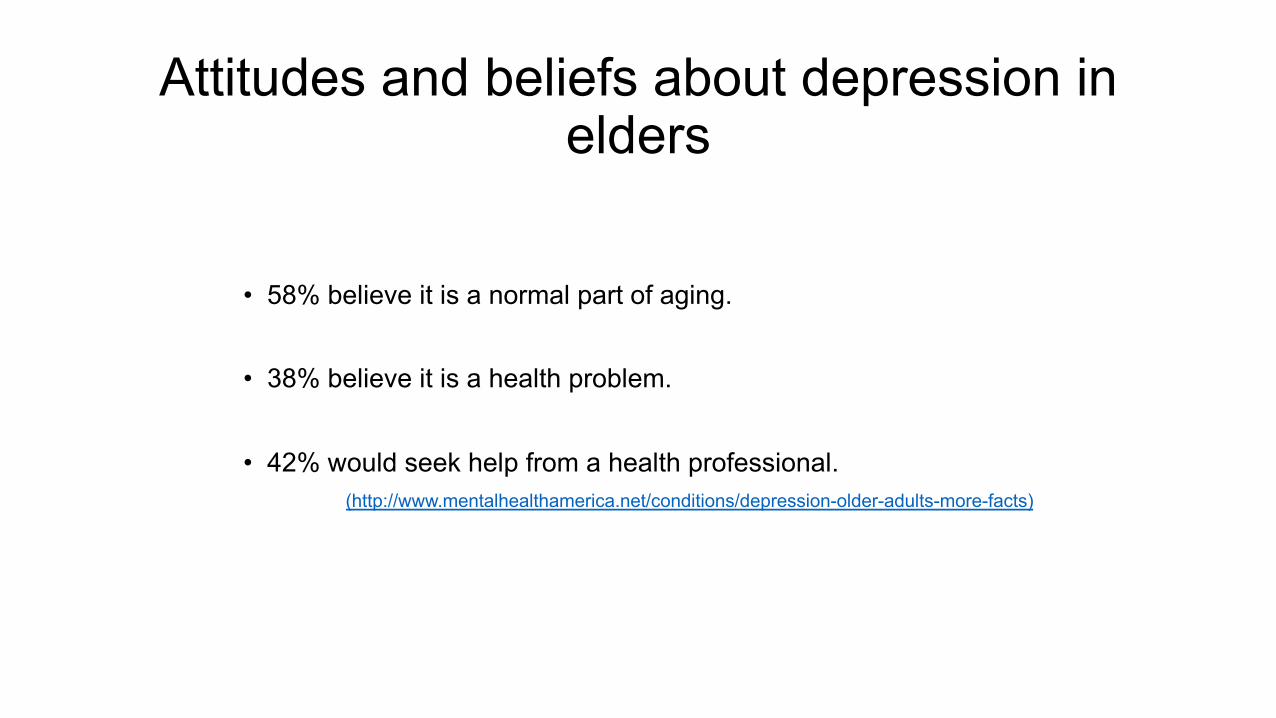
Attitudes and beliefs about depression in elders
• 58% believe it is a normal part of aging.
• 38% believe it is a health problem.
• 42% would seek help from a health professional.(http://www.mentalhealthamerica.net/conditions/depression-older-adults-more-facts)

Hypothesis-driven exam
• Targeted impairment-level testing• Standardized outcome measures
• Goals:o Make a clear connection from Pathology to Activity to
Participation.o Determine etiology of falls.

What are the priorities of her physical exam?

IMPAIRMENT LEVEL TESTING: Cognition
• Alert and oriented to self, birthdate, place, date and situation.
• Follows all simple and 2 step commands with single verbal cue.
Is this enough?

Impairment level testing: cognition
(Ahmed, 2014)
Risk factors for delirium among older people in acute hospital medical units
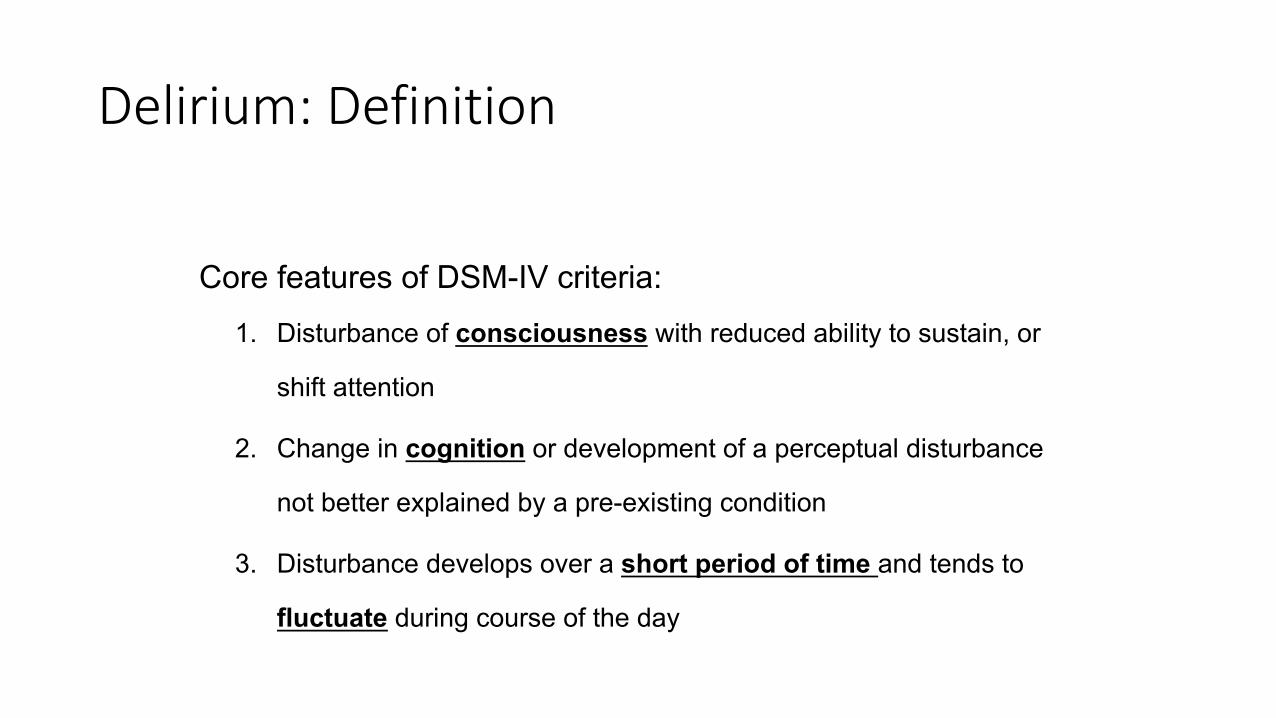
Delirium: Definition
Core features of DSM-IV criteria:1. Disturbance of consciousness with reduced ability to sustain, or
shift attention
2. Change in cognition or development of a perceptual disturbance
not better explained by a pre-existing condition
3. Disturbance develops over a short period of time and tends to
fluctuate during course of the day

Epidemiology
More than 7 million hospitalized Americans experience delirium each year

Clinical Variants
Mixed
Hyperactive Hypoactive
Restless/agitatedAggressive/hyper-reactiveAutonomic arousal15-47% of cases
Lethargic/drowsyApathetic/inactiveQuiet/confusedOften escapes diagnosisOften mistaken for depression19-71% of cases
43-56% of cases

DELIRIUM: LONG TERM EFFECTS
• Neurocognitive sequelae following critical illness:• Common• May be permanent • Associated with impaired ADLs/QOL and inability to return to work
• Evidence from 10 cohorts suggest 25 to 78% survivors experience neurocognitive impairments
• In patients with ARDS the prevalence of neurocognitive impairment may be as high as:
• 78% at d/c • 46% at one year• 25% at 6 years
Hopkins, R et al 2005

Confusion Assessment Method (CAM)

IMPAIRMENT LEVEL TESTING: Hemodynamic Response Considerations
• Goal directed: What are you looking for?• Positional Tolerance • Activity Tolerance • Pulmonary Tolerance
• Assessing a baseline is crucial.• Consider the position of the patient.
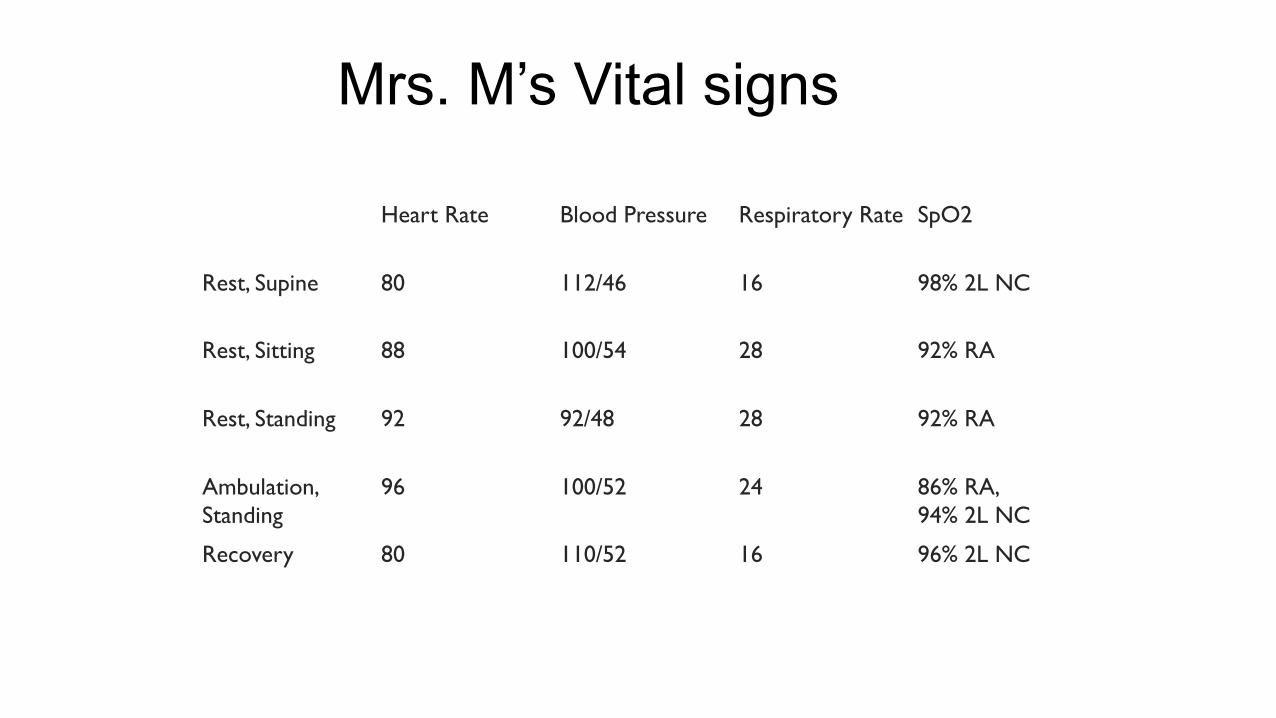
Mrs. M’s Vital signs
Heart Rate Blood Pressure Respiratory Rate SpO2
Rest, Supine 80 112/46 16 98% 2L NC
Rest, Sitting 88 100/54 28 92% RA
Rest, Standing 92 92/48 28 92% RA
Ambulation, Standing
96 100/52 24 86% RA, 94% 2L NC
Recovery 80 110/52 16 96% 2L NC

Integumentary
• Bilateral LE 2+ pitting edema distal to knee to foot
• Bilateral LE hypertrophic toe nails
• Bruising noted throughout L thorax and under chin
Functional Performance
• Bed mobility: MinA with use of bed rail • Sit to stand: minA, required multiple attempts• Ambulation: 50’x2 with RW and CGA, seated
break• Decreased step length and cadence with wide base of
support • Flexed posture with inability to achieve full hip
extension
• Stand to Sit: minA 2/2 poor eccentric control
Musculoskeletal findings
Posture• Flexed trunk with increased thoracic kyphosis, scapular protraction
Strength• Bilateral UEs grossly 3+/5, limited by pain from rib fractures• Bilateral LEs 4/5, suspect B hip extensors weakness which were
observed to be weak with both ambulation and stand to sit
ROM• WFL bilateral UEs/LEs except bilateral ankle DF to neutral only
Sensation• Denies paresthesias, bilateral great toe proprioception intact

Pain
INTENSITY
• 7/10 rest
• 9/10 mobility/deep breaths
• 8/10 recovery
LOCATION
• L thorax
QUALITY
• Constant, worst with deep breaths and mobility
• Sharp, aching
Pulmonary Exam
• Gas Exchange: impaired with ambulation, requires supplemental O2 via nasal cannula
• Ventilation: impaired with incentive spirometer noted to 500mL • Thoracic Excursion: impaired, decreased excursion L > R• Cough Strength/Effectiveness: weak, congested cough, non-
productive of sputum• Auscultation: crackles noted throughout posterior lungs,
diminished L > R

What does all of this information mean?
Physiological Frailty Phenotype

Initial interventions

Interventions
Interdisciplinary Care
Coordination Exercise Prevention Advocacy
Medication changesPain controlPsychosocial Concerns
Targeted therexPulmonary careFunctional mobilityBalance
DeliriumPNAFalls
D/C dispositionRehab needs after d/cLong term outcomesPatient’s values

Physical therapy intervention: Exercise

Exercise Considerations
• MODE
• FREQUENCY
• INTENSITY
• DURATIONExercise

Exercise Intensity
• Overload stimulus is key• 60-80% of 1 rep maximum• At least one set• 2-3x/week • Intersperse strengthening with aerobic exercises and motor
learning activities• Continual re-assessment• Consider Rate of Perceived Exertion (RPE) use, especially in
the hospital setting
(Guccione, 2011; Avers, 2009)Exercise
What does this mean in the Hospital Setting?
• Prescribe therapeutic exercise of adequate intensity
• Use RPE• Target weak muscles that will improve
function• Utilize your rehab aides and other ancillary staff• Empower your patients to perform their exercise
programs independently
Exercise
How do we intervene for pulmonary deficits?

Thoracic Trauma Interventions
• Main goal is to prevent pneumonia (PNA) and other complications
• Pain control• Pulmonary hygiene
• Splinted Coughing• Deep breathing• Chest wall excursion• Incentive Spirometer use• Advocate for frequent walking with nursing
(Shulzhenko, 2017; Winters, 2009)Exercise

Advocate for optimal medical management

Evidenced Based Intervention: Advocate for Optimal pain management
• Increased pain means decreased likelihood of discharge home.
(Brotemarkle, 2015)
• Scheduled acetaminophen if appropriate.(Inouye, 2015)
• Adequate pain control reduces delirium.(American Geriatrics Society, 2015)
Interdisciplinary Care
Coordination
Interventions to Address Medication management
• Patient/Caregiver Education: • Timing• Understanding of effects • Management • Empower to advocate for changes if indicated
• Medication Reconciliation: • Consider Beers Criteria and discuss high risk medications • Advocate for Pharmacist or Geriatrician involvement (Pellegrin, 2017)
• Communicate suspected medication effects and impact on patient presentation Interdisciplinary
Care Coordination

Evidence Based Interventions: Advocate for Geriatrics consultation
• Involvement of geriatricians has been associated with:
• Lower rates of delirium and discharge to long term care.
(Lenartowicz, 2012)• A reduction in hospital-acquired complications such as
functional decline, falls, delirium, and death. (Fallon, 2006)
• Better recovery of function over the year following injury.
(Tillou, 2014) Interdisciplinary Care
Coordination

Address psychosocial issues
• Advocate for social work consult: • Emotional support and coping• Possible facilitation of outpatient follow up
with mental health services
Interdisciplinary Care
Coordination

Minimize risk of delirium
Delirium is preventable in 30–40% of cases
(Sidiqqi, 2016)

Evidence Based Intervention: Best Practice Statement from the American Geriatrics Society
• Sensory enhancement• Mobility enhancement • Orientation protocols • Cognitive stimulation• Nutritional and fluid repletion enhancement• Sleep• Medication review • Minimization of restraints and tethers
(Inouye, 2015)Prevention
Discharge Planning

Evidence Based Interventions: Discharge Planning
• 30% of patients reported having received < 1 day advance notice of discharge.
(Horwitz, 2013)
• Poorly coordinated transitions of care can lead to:• Adverse medication events• Patient and caregiver dissatisfaction• Functional decline
(Jeffs, 2017)
Advocacy
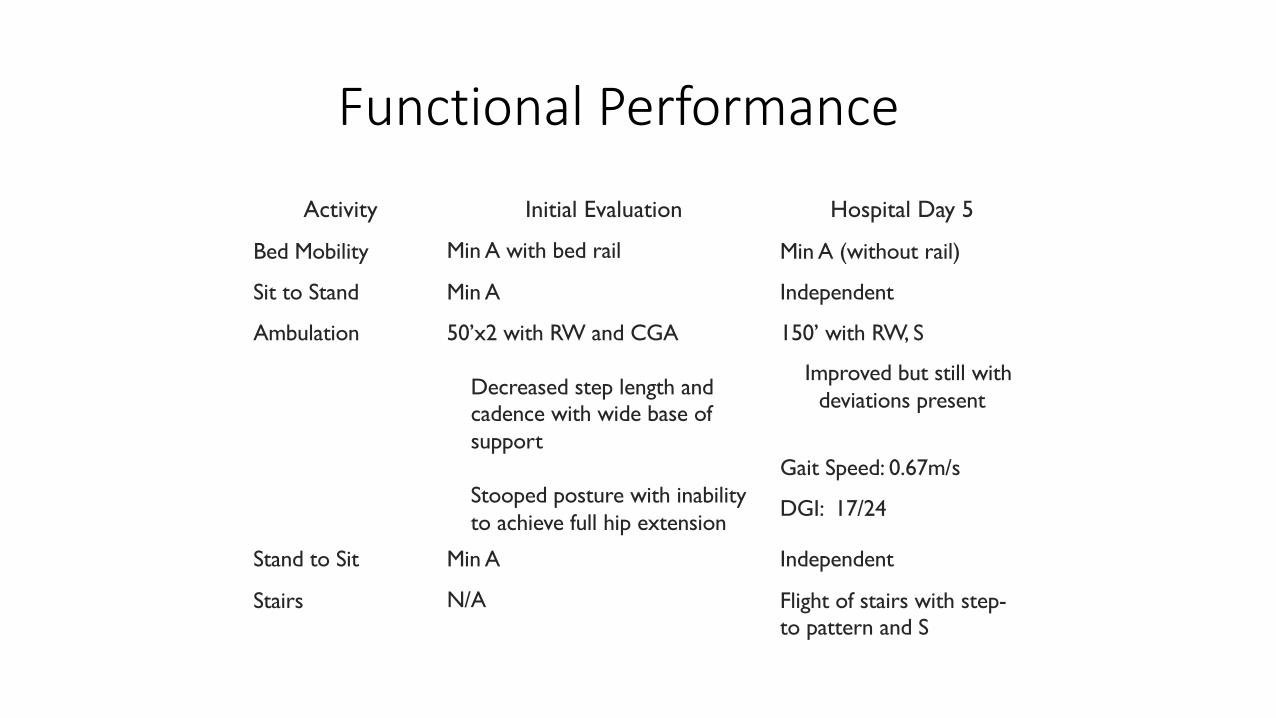
Functional Performance
Activity Initial Evaluation Hospital Day 5
Bed Mobility Min A with bed rail Min A (without rail)
Sit to Stand Min A Independent
Ambulation 50’x2 with RW and CGA
Decreased step length and cadence with wide base of support
Stooped posture with inability to achieve full hip extension
150’ with RW, S
Improved but still with deviations present
Gait Speed: 0.67m/s
DGI: 17/24
Stand to Sit Min A Independent
Stairs N/A Flight of stairs with step-to pattern and S

Ongoing evidence based examination: Value of standardized tests and outcome measures
• Inform discharge recommendations (Bland, 2014)
• Evidence-based approach (Jette, 2003)
• Quantify observations (Potter, 2011; Sullivan, 2011)
• Improve continuity of care between settings (Thier, 2006)
• Identification of impairments (Guide to Physical Therapist Practice)
• Establish a baseline (Guide to Physical Therapist Practice)

How Do You Select an Appropriate Standardized Test or Outcome Measure?
• Feasibility of use in setting• Valid and reliable for population• Identify impairments central to patient presentation • Functional prognosis/Discharge disposition• Responsiveness to change
Mrs M’s Results
Comfortable Walking Speed• Pt demonstrated a comfortable
walking speed of 0.67m/s over 10m using a RW.
Dynamic Gait Index• Pt scored a 17/24.
How do we make a decision?
DISCHARGE PLANNING:PATIENT CENTERED PRACTICE
• “Physical therapists should account for patient’s sense of identity, goals, history, and social context in order to engage in a process of communication and deliberation with the patient, with the goal of maximizing patient autonomy and developing a patient-centered care plan that call can accept.”
• For action to qualify as autonomous, a substantial degree of understanding is required. (Hunt, 2011)
Advocacy

Discharge planning
• Optimal care of the injured older adult does not end with
acute care
• Proper rehab is important to maximize functional outcomes
• Trauma admissions to SNF doubled from 2003-2009
• (Ayoung-Chee, 2013)
• Recent legislation enforcing joint hospital – SNF
responsibility for outcomes and associated costs may
intensify the focus on patient selection for SNF (Burke, 2017)
Advocacy

Discharge planning: Home vs. Rehab
• Values• Safety• Amount and Intensity of Therapy• Functional Outcomes
Advocacy

Discharge planning: Drivers
• Advances in medical care and changes in payer reimbursement lead to decreased LOS and expedited D/C
• SNF becomes a safety net• Knowledge deficit re: SNF practices, quality and patient
outcomes• Lack of standardized evaluation process or clear primary
decision maker• (Burke, 2017)
Advocacy

Evidence to support disposition
HOME REHAB

Impairments in body functions & structures:
• Exercise• Pulmonary
Activity Restrictions• Balance• Mobility• ADL
Participation Restrictions• Family role
Health Condition• Medication changes• UTI treatment
Personal Factors• Depression screen• Delirium prevention• Patient’s goals
Environmental Factors• Family assistance• Home set up AdvocacyPrevention
Interdisciplinary Care
CoordinationExercise

In Conclusion…
• Consider age related changes and how they affect the performance and care of older adults
• Consider impact of medications and the PT role in management• Maximize examinations by performing strategic hypothesis-
driven exams• Maximize interventions with knowledge of pathophysiology and
application of evidence• Perform patient-centered discharge planning

References
Ahmed, S., Leurent, B., Sampson, E. ; Risk factors for incident delirium among older people in acute hospital medical units: a systematic review and meta-analysis, Age and Ageing, Volume 43, Issue 3, 1 May 2014, Pages 326 -333, https://doi.org/10.1093/ageing/afu022
American Geriatrics Society 2015 Beers Criteria Update Expert Panel. 2015. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc 63 (11): 2227-2246.
Avers D, Brown M. White paper: strength training for the older adult. Journal of Geriatric Physica Therapy. 2009; 32(4):148-158.
Ayoung-Chee, P et al. Beyond the hospital doors: Improving long-term outcomesfor elderly trauma patients. 2013. J Trauma Acute Care Surg. Volume 78, Number 4 DOI: 10.1097/TA.0000000000000567
Bellal J, Pandit V, Zangbar B. Superiority of frailty over age in predicting outcomes among geriatric trauma patients: a prospective analysis. JAMA Surg. 2014; 149(8):766-772.
Beswick AD, Gooberman HR, Smith A, Wylde V, Ebrahim S. Maintaining independence in older people. Reviews in Clinical Gerontology. 2010;20:128.-153
Bland MD, Whitson M, Harris H, et al. Descriptive data analysis examining how standardized assessments are used to guide post-acute discharge recommendations for rehabilitation services after stroke. Phys Ther. 2014;95(5):710-719.
Brooks S, Peetz A. Evidenced based care of geriatric trauma patients. Clin Surg N Am. 2017; 1157-1174.
Brotemarkle, Rebecca A., et al. "Length of hospital stay and discharge disposition in older trauma patients." Geriatric Nursing 36.2 (2015): S3-S9.
Brummel, Nathan E., et al. "Delirium in the intensive care unit and subsequent long-term disability among survivors of mechanical ventilation." Critical care medicine 42.2 (2014): 369.
Burke, R. et al. Use of post-acute care after hospital discharge in urban and rural hospitals. Am J Accountable Care. 2017 Mar; 5(1): 16–22.
Fallon Jr, William F., et al. "Geriatric outcomes are improved by a geriatric trauma consultation service." Journal of Trauma and Acute Care Surgery 61.5 (2006): 1040-1046.
Fang CK, Chen HW, Liu SI, et al. Prevalence, detection and treatment of delirium in terminal cancer inpatients: a prospective survey. Jpn J Clin Oncol 2008;38:56–63.
Flanagan, Elaine, et al. "Infection Control in Alternative Health Care Settings." Infectious Disease Clinics 30.3 (2016): 785-804.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerotol A Biol Sci Med Sci. 2001; 56(3):M146-156.

Fried TR, et al. 2014. Health Outcomes Associated with Polypharmacy in Community-Dwelling Older Adults: A Systematic Review. J Am Geriatr Soc 62 (12): 2261-2272.
Fritz, S. & Lusardi, M. "White paper:“walking speed: the sixth vital sign”." Journal of geriatric physical therapy 32.2 (2009): 2-5.
Gaebel A. Challenges in the management of geriatric trauma: a case report. Journal of Trauma Nursing. 2017; 245-250.
Guccione A, Wong R, Avers D. Geriatric Physical Therapy. 3rd ed. Mosby; 2011.
Guide to Physical Therapist Practice 3.0. Alexandria, VA: American Physical Therapy Association; 2014. Available at: http://guidetoptpractice.apta.org/. Accessed 11/10/2017.
Horwitz, Leora I., et al. "Quality of discharge practices and patient understanding at an academic medical center." JAMA internal medicine 173.18 (2013): 1715-1722. Objective To conduct a multifaceted evaluation of transitional care from a patient-centered perspective.
Hunt, Matthew R., and Carolyn Ells. "Partners towards autonomy: risky choices and relational autonomy in rehabilitation care." Disability and Rehabilitation 33.11 (2011): 961-967.
Inouye, Sharon K., et al. "Postoperative delirium in older adults: best practice statement from the American Geriatrics Society." Journal of the American College of Surgeons 220.2 (2015): 136-148.Jeffs, Lianne, et al. "The role of caregivers in interfacility care transitions: a qualitative study." Patient preference and adherence 11 (2017): 1443.
Jette, Diane U., et al. "Evidence-based practice: beliefs, attitudes, knowledge, and behaviors of physical therapists." Physical therapy 83.9 (2003): 786-805.
Jønsson, Line R., et al. "Intra-and interrater reliability and agreement of the Danish version of the Dynamic Gait Index in older people with balance impairments." Archives of physical medicine and rehabilitation 92.10 (2011): 1630-1635.
Kenny, R. A., et al. "Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons." Journal of the American Geriatrics Society 59.1 (2011): 148-157.
Kiely, Dan K., et al. "Association between delirium resolution and functional recovery among newly admitted postacute facility patients." The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 61.2 (2006): 204-208.
Kojima T, Akishita M, Nakamura T, et al. 2012. Polypharmacy as a risk for fall occurrence in geriatric patients. Geriatr Gerontol Int. 12; 425-430.
Leland, Natalie E., et al. "Falls in newly admitted nursing home residents: a national study." Journal of the American Geriatrics Society 60.5 (2012): 939-945.
Lenartowicz, Magda, et al. "An evaluation of a proactive geriatric trauma consultation service." Annals of surgery 256.6 (2012): 1098-1101.
Leppin, Aaron L., et al. "Preventing 30-day hospital readmissions: a systematic review and meta-analysis of randomized trials." JAMA internal medicine 174.7 (2014): 1095-1107.
Marcantonio, Edward R., et al. "3D-CAM: Derivation and Validation of a 3-Minute Diagnostic Interview for CAM-Defined DeliriumA Cross-sectional Diagnostic Test Study3D-CAM: Derivation and Validation of a 3-Minute Interview for Delirium." Annals of internal medicine 161.8 (2014): 554-561.
Ostir, Glenn V., et al. "Assessing gait speed in acutely ill older patients admitted to an acute care for elders hospital unit." Archives of internal medicine 172.4 (2012): 353-358.
PATIENT, GERIATRIC. "American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults." J Am Geriatr Soc 63.1 (2015): 142-150.
Pardasaney, Poonam K., et al. "Sensitivity to change and responsiveness of four balance measures for community-dwelling older adults." Physical therapy 92.3 (2012): 388-397.
Perera, Subashan, et al. "Meaningful change and responsiveness in common physical performance measures in older adults." Journal of the American Geriatrics Society 54.5 (2006): 743-749.
Potter K, Fulk GD, Salem Y, et al. Outcome measures in neurologic physical therapy practice: part I. Making sound decisions. J Neurol Phys Ther. 2011;35(2):57–64.
Ryan DJ, O'Regan N, Caoimh RO, et al. Delirium in an adult acute hospital population: predictors, prevalence and detection. BMJ Open 2013;3:e001772.
Sharma G, Goodwin J. Effects of aging on respiratory system physiology and immunology. Clinical Interventions in Aging. 2006; 1(3): 253-260.
Shulzhenko N, Zens T, Beems M, et al. Number of Rib Fractures thresholds independently predict worse outcomes in older patients with blunt trauma. Surgery. 2017; 161(4):1083-1089.
Sidiqqi, N et al. Interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2016 Mar 11;3:CD005563. doi: 10.1002/14651858.CD005563.pub3.

Smith, G. Bennett, S.F. Bradley, et al. Infection prevention and control in long-term care facilities. Infect Control Hosp Epidemiol, 29 (2008), pp. 785-814
Steffens DC, Fisher GG, Langa KM, Potter GG, Plassman BL. 2009. Prevalence of depression among older Americans: the Aging, Demographics and Memory Study. Int Psychogeriatr 21(5): 879-888.
Stevens LE, de Moore GM, Simpson JM. Delirium in hospital: does it increase length of stay?. Australian and New Zealand Journal of Psychiatry 1998;32(6):805-8.
Sullivan JE, Andrews AW, Lanzino D, et al. Outcome measures in neurological physical therapy practice: part II. A patient-centered process. J Neurol Phys Ther. 2011;35(2):65–74.
Thier SO. Forces motivating the use of health status assessment measures in clinical settings and related clinical research. Med Care. 1992;30(5 Suppl):MS15–MS22.
Tieland M, Trouwborst I, Clark BC. Skeletal Muscle Performance and Ageing. Journal of Cachexia, Sarcopenia and Muscle. 2017; 1-17.
Tillou, Areti, et al. "Long-term postinjury functional recovery: outcomes of geriatric consultation." JAMA surgery 149.1 (2014): 83-89.
Veronese N, Stubbs B, Trevisan C, et al. 2017. Poor Physical Performance Predicts Future Onset of Depression in Elderly People: Progetto Veneto Anziani Longitudinal Study. Phys Ther 96 (6): 659-668.
Vigorito C, Giallauria F. Effects of exercise on cardiovascular performance in the elderly. Frontiers in Physiology. 2014; 5(51): 1-8.
Voyer P, McCusker J, Cole MG, et al. Factors associated with delirium severity among older patients. J Clin Nurs 2007;16:819–31.
Vu, M., N. Weintraub, and L. Rubentstein. United States. National Library of Medicine. Falls in the nursing home: are they preventable?. PubMed Health, 2004
Ward, Derek, et al. "Care home versus hospital and own home environments for rehabilitation of older people." The Cochrane Library (2008).
Winters B. Older adults with traumatic rib fractures: an evidence-based approach to their care. Journal of Trauma Nursing. 2009; 16(2): 93-97.
Wrisley, Diane M., and Neeraj A. Kumar. "Functional gait assessment: concurrent, discriminative, and predictive validity in community-dwelling older adults." Physical therapy 90.5 (2010): 761-773.