Compositional Networks for Unsupervised Tumor Localization ...
Upload
bernard-fisherCategory
view
214download
0
TRAUMA AND THE LOCALIZATION OF TUMOR CELLS
BERNARD FISHER, MD,* EDWIN R. FISHER, M D ~ AND NICHOLAS FEDUSKA, BS*
Injection of ‘‘Cr labeled Walker tumor cells either intravenously or via the aorta into normal rats or those subjected to mechanical, chemical or surgical trauma of a hind limb resulted in (a) equal distribution of cells to both hind legs when neither was traumatized; (b) a lodgement of a greater number of cells in legs subjected to either of the three types of trauma than in the untraumatized extremity of the same animal; (c) a failure of adequate heparinization to alter cell localization at sites of trauma; (d) no difference in tumor cell localization between normal limbs of control or traumatized animals, minimizing the roll of stress or other systemic factors. It is concluded that increased numbers of tumor cells lodge at sites of trauma and may well be the reason for the ob- served augmented metastases.
ORE THAN 50 YEARS AGO LUBARSCH24 NOTED M that mouse tumors could be made to localize secondarily about splinters implanted in the liver, and Jones and RousZ2 demon- strated the role of trauma in the localization of serosal metastases when neoplastic cells were injected into the peritoneal cavity. Since then, convincing experimental evidence has accumulated which demonstrates that tissue damaged physically, chemically, or by hypoxia provides an especially “fertile soil” for the de- velopment of metastases from hematogenously disseminated tumor cells. Robinson and Hoppe27 observed that following the intra- aortic injection of V2 carcinoma cells both mechanical trauma and ischemia of the rab- bit hind leg resulted in the occurrence of more tumors in the damaged than normal extrem- ity. Alexander and Altemeir,2 employing the same tumor, noted that injury due to ischemia and nitrogen mustard perfusion of the spleen and to simple abdominal incision enhanced susceptibility of the injured tissues to tumor growth from circulating tumor cells. Accord- ing to Agostino and Clifftonl the number of metastases in the hind legs of rats was greatly
From the Departments of Surgery and Pathology, University of Pittsburgh School of Medicine, Pitts- burgh, Pa.
Aided by U.S. Public Health Service grants CA-05949, CA-05716 and American Cancer Society grant P-142.
* Professor of Surgery, University of Pittsburgh. t Professor of Pathology, University of Pittsburgh. $ U.S. Public Health Service Summer Trainee. The valuable assistance of Miss Joyce Mitchell is
Received for publication May 16, 1966. gratefully acknowledged.
increased following the intra-aortic inocula- tion of Walker carcinoma cells if they had been traumatized by a prior injection of tur- pentine. A high incidence of metastases from Brown-Pearce carcinoma implanted intratesti- cularly was observed by Black3 to occur in subcutaneous abscesses and granulation tissue induced by turpentine.
Our own investigations have demonstrated that the incidence of hepatic metastases is greatly augmented by either direct hepatic trauma7 or liver damage induced by a variety of modalities, such as altered hepatic blood
interferences with reticuloendothelial function,l7 or cirrhosis produced with carbon tetrachloride.18 In addition, we have reported that the growth of dormant tumor cells could be stimulated by hepatic injury,lo that the intraportal inoculation of tumor cells in one animal of a parabiotic pair resulted in hepatic metastases in the other uninjected animal if its liver had been traumatized,lg and that tu- mors occurred at the site of injection of sub- cutaneous liver homogenate in both single and parabiotic animals when the homogenate was separate from the location of tumor cell inoculation.ll Such homogenates were fre- quently the cause of sterile abscesses with an inflammatory response.
ClinicaI reports of augmented tumor growth following trauma by Ewing,6 Willis31 and others59 21925 appear coincident with these ex- perimental findings.
Mechanisms responsible for this affect of trauma are speculative. One may cogently in-
23

24 CANCER January 1967 Vol. 20
quire whether they are the result of growth- promoting factors released by damaged tissues or the result of a predilection for greater num- bers of circulating tumor cells to lodge at sites of trauma, thus enhancing the chance for a metastasis. In an effort to supply informa- tion relative to the latter, investigations were carried out employing 51Cr labeled tumor cells in animals subjected to mechanical, chemical and surgical trauma. In addition, since i t has recently been reported1 that the number of metastases in the area of local trauma could be reduced by anticoagulants, the effect of heparin upon tumor cell lodgment at sites of injury was also evaluated.
MATERIALS AND METHODS
Sprague-Dawley male rats (Holtzman Farms, Madison, Wis.) weighing 250 to 300 Gm were used in all experiments. They were housed in individual cages and permitted water and a standard laboratory chow diet ad libitum.
All animals were traumatized while anesthe- tized with open drop ether. Trauma was uni- formly applied to the thigh of the left hind leg, the right serving as a control. A standard- ized mechanical trauma was produced by repetitively dropping a 68 Gm weight 14 times during 30 to 45 seconds from a height of 45 cm. The weight was suspended in a glass tube so that the angle of fall could be con- trolled. This resulted in contusion of the thigh muscles without overt damage to the skin or fracture of the bone.
Chemical trauma was induced with 0.5 ml of turpentine (Sherwin-Williams) which was injected into the thigh muscle. In one experi- ment surgical trauma was produced by mak- ing a 2 cm longitudinal incision through the skin and muscle of the thigh and immediately closing the wound with silk sutures. I n another, in addition to the incision the sev- ered edges of the muscle on either side were clamped with hemostats for 15 seconds prior to closure of the wound.
The Walker carcinoma employed in this study has been propagated in this laboratory since 1957 and the techniques used in the preparation and counting of cell suspensions have been described,16 as has been the tech- nique employed for labeling tumor cells with 51Cr.839 The latter is similar, with slight varia- tion, to that first described by Rajam et aLZ6 for labeling Ehrlich mouse ascites tumor cells, and by Selecki.28
Tumor cells were injected intravenously via a PE 50 polyethylene catheter inserted into the jugular vein 24 hours prior to trauma. Intra-aortic injection of cell suspensions were in the direction of blood flow through a 27- gauge needle inserted 3 to 5 mm above the bi- furcation. Following withdrawal of the needle bleeding was easily controlled by gentle pres- sure with a gauze sponge. Each animal was injected with 0.5 ml of a tumor cell suspension containing 5 x 106 cells having an average radioactivity of 14,000 counts/min (CPM). Jugular catheters were rinsed with an addi- tional 0.25 ml of saline.
Animals were sacrificed by exsanguination 1, 6 or 24 hours following tumor cell inocula- tion. Hind legs were removed by a uniform incision through skin and muscle at the level of the hip, and the lower leg was removed at the knee joint. Muscle and skin of the thigh was stripped from the femur and 51Cr assay of these tissues was carried out in a Baird- Atomic sodium iodide-thallium activated well scintillation counter. Since the activity of labeled tumor cell suspensions exhibited daily variation, the actual CPM obtained in each sample was arbitrarily corrected to an injec- tion dose of 50,000 CPM to provide uniform- i ty. Since in any suspension employed there was a direct relationship of number of cells to radioactivity, it may be assumed that there is random distribution of the chromium tag within the cell population. Consequently, re- sults are presented as comparisons of radioac- tivity and/or tumor cells between traumatized and uninjured legs. T o evaluate differences between the two legs, the t,95 test for paired observations was employed.
In studies performed to evaluate the effect of anticoagulants on tumor cell lodgment in traumatized tissue, jugular catheters were in- serted 4 days prior to tumor cell injection so as to avoid excessive bleeding upon cannula- tion. Heparin (700 units/100 Gm body weight) was administered 30 minutes prior to tumor cell injection and 12 hours later. In such ani- mals the Lee-White clotting time was longer than one hour during the entire experimental period.
RESULTS
Distribution of Tumor Cells in Untraumatized Controls (Table 1)
Animals injected with 5 x lo6 labeled Walker tumor cells via a jugular vein catheter
No. 1 TRAUMA AND LOCALIZATION OF TUMOR CELLS * Fisher et al. 25
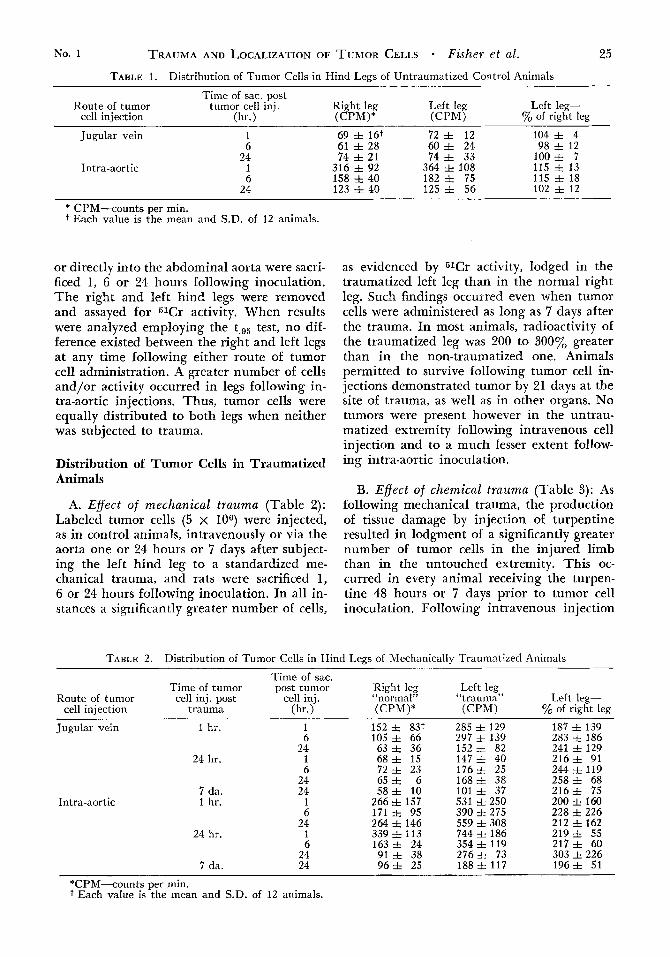
TABLE 1. Distribution of Tumor Cells in Hind Legs of Untraumatized Control Animals
Time of sac. post Route of tumor tumor cell inj. Right leg Left leg Left leg-
cell injection (hr.) (CPM)* ( C P W % of right leg
Jugular vein
Intra-aortic
1 6
24 1 6
24
69 f 16t 72 f 12 104 f 4 61 f 28 60 f 24 98 f 12 74 + 21 74 * 33 100 i 7
316 92 364 108 158 f 40 182 f 75 123 f 40 125 i 56
115 13 115 f 18 102 * 12
* CPM-counts per min. t Each value is the mean and S.D. of 12 animals.
or directly into the abdominal aorta were sacri- ficed 1, 6 or 24 hours following inoculation. The right and left hind legs were removed and assayed for 61Cr activity. When results were analyzed employing the t.95 test, no dif- ference existed between the right and left legs at any time following either route of tumor cell administration. A greater number of cells and/or activity occurred in legs following in- tra-aortic injections. Thus, tumor cells were equally distributed to both legs when neither was subjected to trauma.
Distribution of Tumor Cells in Traumatized Animals
A. Eflect of mechanical trauma (Table 2): Labeled tumor cells (5 x 106) were injected, as in control animals, intravenously or via the aorta one or 24 hours or 7 days after subject- ing the left hind leg to a standardized me- chanical trauma, and rats were sacrificed 1, 6 or 24 hours following inoculation. In all in- stances a significantly greater number of cells,
as evidenced by 61Cr activity, lodged in the traumatized left leg than in the normal right leg. Such findings occurred even when tumor cells were administered as long as 7 days after the trauma. In most animals, radioactivity of the traumatized leg was 200 to 300y0 greater than in the non-traumatized one. Animals permitted to survive following tumor cell in- jections demonstrated tumor by 21 days at the site of trauma, as well as in other organs. No tumors were present however in the untrau- matized extremity following intravenous cell injection and to a much lesser extent follow- ing intra-aortic inoculation.
B. Effect of chemical trauma (Table 3): As following mechanical trauma, the production of tissue damage by injection of turpentine resulted in lodgment of a significantly greater number of tumor cells in the injured limb than in the untouched extremity. This oc- curred in every animal receiving the turpen- tine 48 hours or 7 days prior to tumor cell inoculation. Following intravenous injection
TABLE 2. Distribution of Tumor Cells in Hind Legs of NIechanically Traumatized Animals
Time of sac. Time of tumor post tumor Right leg Left leg
cell injection trauma (hr.) (CPM)* ( C P W % of right leg Route of tumor cell inj. post cell inj. “normal” “trauma” Left leg-
Jugular vein 1 hr.
24 hr.
Intra-aortic 7 da. 1 hr.
1 6
24
152 f 83+ 285 f 129 187 f 139 105 f 66 297 f 139 283 f 186 63 f 36 152 f 82 241 f 129
1 68 f 15 1 4 7 f 40 216f 91 6 72 f 23 1 7 6 f 25 244 f 119
24 65 + 6 168-t 38 2 5 8 i 68 ~- 24
1 6
~~~ - 581 10 101 f 37 2 1 6 I 75 266 f 157 531 f 250 200 f 160 171 f 95 390 f 275 228 f 226
24 264 f 146 559 f 308 212 f 162 24 hr. 1 339 h 113 744 =k 186 2 1 9 h 55
6 1 6 3 f 24 354 f 119 217f 60 276+ 73 303 f 226
7 da. 24 9 6 f 25 188 f 117 1 9 6 f 51 24 91 f 38
*CPM-counts per min. t Each value is the mean and S.D. of 12 animals.
26 CANCER January 1967 VOl. 20
TABLE 3. Distribution of Tumor-Cells in Hind Legs of Chemically Traumatized Animals
Time of sac. Time of tumor post tumor Right leg ,, Left leg
cell injection trauma (hr.1 (CPM)* (CPM) '% of right leg Route of tumor cell inj. post cell inj. "normal" trauma" Left leg-
Jugular vein 48 hr. 1 6
24
109 f 89t 393 i 265 360 f 158 8 6 f 80 689 f 188 801 f 143
1 2 0 i 69 670 f 423 558 f 148 21 days 72 f 46 319 f 233 443 f 199
7 da. 24 85 f 15 455 f 102 535 f 204 Intra-aortic 48 hr. 1 332 f 227 919 f 351 277 f 173
6 279 f 251 905 f 712 324 f 110 24 67f 29 657 f 128 980 f 937 21 days 25 f 13 151 f 65 604 f 510
7 da. 24 81 f 16 583 f 347 720 f 407
* CPM-counts per min. t Each value is mean and S.D. of 12 animals.
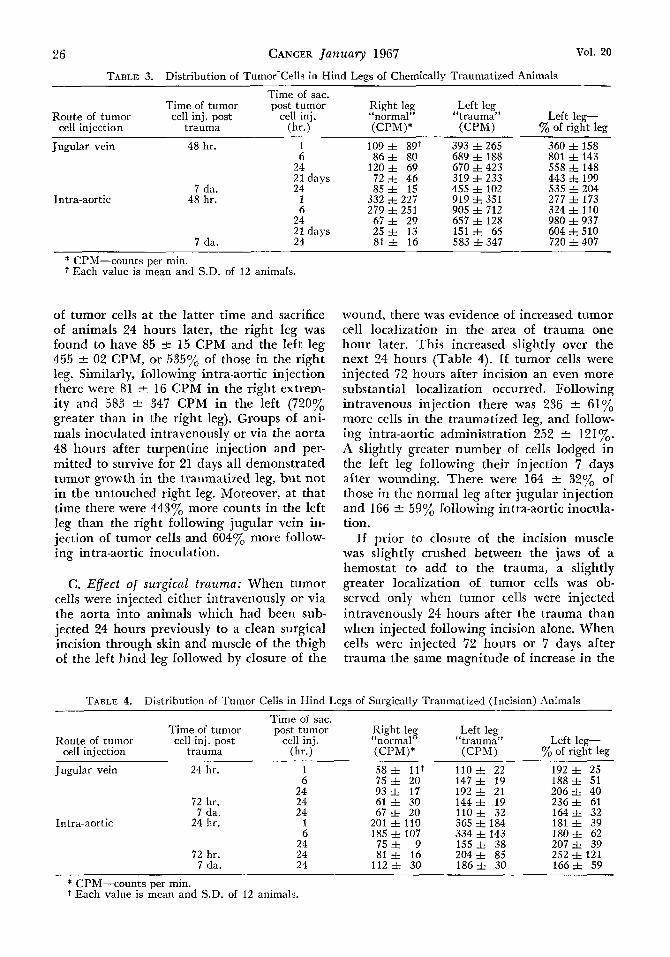
of tumor cells at the latter time and sacrifice of animals 24 hours later, the right le, 0 was found to have 85 -i- 15 CPM and the left leg 455 2 02 CPM, or 535% of those in the right leg. Similarly, following intra-aortic injection there were 81 2 16 CPM in the right extrem- ity and 583 2 347 CPM in the left (720y0 greater than in the right leg). Groups of ani- mals inoculated intravenously or via the aorta 48 hours after turpentine injection and per- mitted to survive for 21 days all demonstrated tumor growth in the traumatized leg, but not in the untouched right leg. Moreover, at that time there were 443% more counts in the left leg than the right following jugular vein in- jection of tumor cells and 604% more follow- ing intra-aortic inoculation.
C. Eflect of surgical trauma: When tumor cells were injected either intravenously or via the aorta into animals which had been sub- jected 24 hours previously to a clean surgical incision through skin and muscle of the thigh of the left hind leg followed by closure of the
wound, there was evidence of increased tumor cell localization in the area of trauma one hour later. This increased slightly over the next 24 hours (Table 4). If tumor cells were injected 72 hours after incision an even more substantial localization occurred. Following intravenous injection there was 236 t 61y0 more cells in the traumatized leg, and follow- ing intra-aortic administration 252 * 121%. A slightly greater number of cells lodged in the left leg following their injection 7 days after wounding. There were 164 t 32y0 of those in the normal leg after jugular injection and 166 2 59% following intra-aortic inocula- tion.
If prior to closure of the incision muscle was slightly crushed between the jaws of a hemostat to add to the trauma, a slightly greater localization of tumor cells was ob- served only when tumor cells were injected intravenously 24 hours after the trauma than when injected following incision alone. When cells were injected 72 hours or 7 days after trauma the same magnitude of increase in the
TABLE 4. Distribution of Tumor Cells in Hind Legs of Surgically Traumatized (Incision) Animals
Time of sac. Time of tumor Dost tumor Rirht lev Left lev
0
Route of tumor cell inj. post A cell inj. c6normal" "trauma" Left leg- cell injection trauma (hr.1 (CPM)* (CPM) yo of right leg
Jugular vein 24 hr. 1 58% 1 1 7 1 1 O f 22 192 f 25 1 8 8 f 51
24 93, 17 192+ 21 206, 40 6 75 f 20 147 f 19
Intra-aortic
72 hr. 7 da.
24 hr.
24 24
1
61 30 i 4 4 I i 9 236f 61 67 f 20 110f 32 164f 32
201 f 110 365 f 184 181 f 39 6 185 f 107 334 f 143 180f 62
24 75 f 9 155 f 38 2 0 7 5 39 72 hr. 24 81 f 16 204 f 85 252 f 121
7 da. 24 112 f 30 1 8 6 f 30 1 6 6 h 59
* CPM-counts per min. t Each value is mean and S.D. of 12 animals.
No. 1 TRAUMA AND LOCALIZATION OF TUMOR CELLS Fisher et al.
TABLE 5. Distribution of Tumor Cells in Hind Legs of Surgically Traumatized (Incision + Muscle Crush) Animals
27
Time of sac. Time of tumor post tumor Right leg ( ( Left leg
cell injection trauma (hr.1 (CPM)* (CPM) % of right leg Route of tumor cell inj. post cell inj. “normal” trauma” Left leg-
Jugular vein 24 hr. 24 96 f 41t 220 f 52 229 f 114 72 hr. 24 75 i 20 176 f 38 235 f 80
7 da. 24 79 f 13 127 f 30 161 f 38 ~ _ _ _ _ _
* CPM-counts per min. t Each value is mean and S.D. of 12 animals.
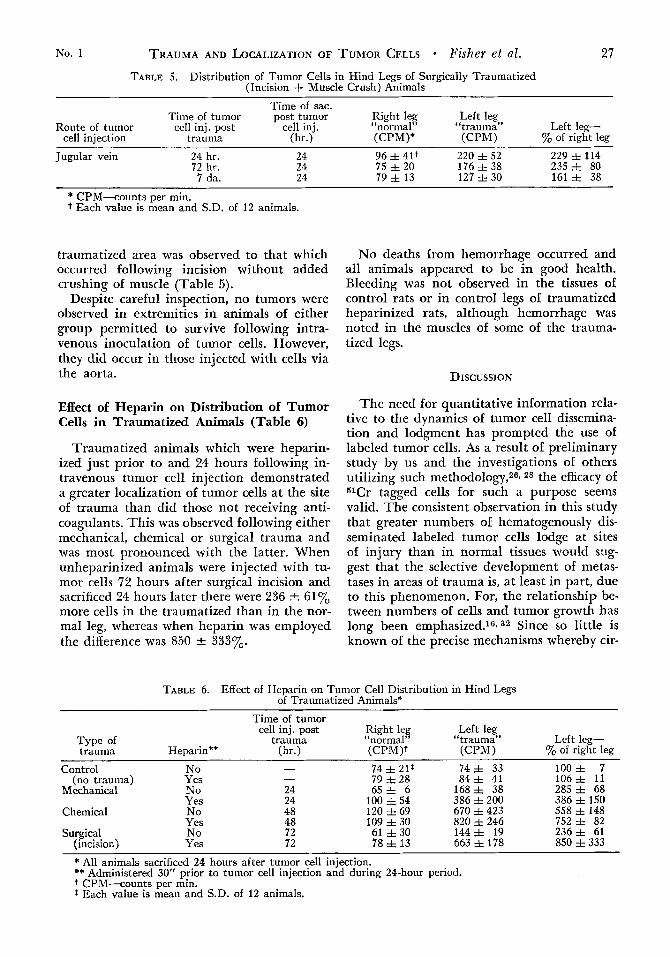
traumatized area was observed to that which occurred following incision without added crushing of muscle (Table 5).
Despite careful inspection, no tumors were observed in extremities in animals of either group permitted to survive following intra- venous inoculation of tumor cells. However, they did occur in those injected with cells via the aorta.
Effect of Heparin on Distribution of Tumor Cells in Traumatized Animals (Table 6)
Traumatized animals which were heparin- ized just prior to and 24 hours following in- travenous tumor cell injection demonstrated a greater localization of tumor cells at the site of trauma than did those not receiving anti- coagulants. This was observed following either mechanical, chemical or surgical trauma and was most pronounced with the latter. When unheparinized animals were injected with tu- mor cells 72 hours after surgical incision and sacrificed 24 hours later there were 236 & 61% more cells in the traumatized than in the nor- mal leg, whereas when heparin was employed the difference was 850 k 333%.
No deaths from hemorrhage occurred and all animals appeared to be in good health. Bleeding was not observed in the tissues of control rats or in control legs of traumatized heparinized rats, although hemorrhage was noted in the muscles of some of the trauma- tized legs.
DISCUSSION
The need for quantitative information rela- tive to the dynamics of tumor cell dissemina- tion and lodgment has prompted the use of labeled tumor cells. As a result of preliminary study by us and the investigations of others utilizing such methodology,269 28 the efficacy of 51Cr tagged cells for such a purpose seems valid. The consistent observation in this study that greater numbers of hematogenously dis- seminated labeled tumor cells lodge at sites of injury than in normal tissues would sug- gest that the selective development of metas- tases in areas of trauma is, at least in part, due to this phenomenon. For, the relationship be- tween numbers of cells and tumor growth has long been emphasized.16, 32 Since so little is known of the precise mechanisms whereby cir-
TABLE 6. Effect of Heparin on Tumor Cell Distribution in Hind Legs of Traumatized Animals*
Time of tumor Right leg Left leg
Type of trauma “normal” “trauma” Left leg- trauma Heparin** (hr.1 (CPM)? (CPM) ’% of right leg
cell inj. post
Control No - 74 f 2 l r 7 4 k 33 100 f 7 106f 11
Mechanical No 24 6 5 f 6 168% 38 285 f 68 Yes 24 100 + 54 386 + 200 386 f 150
(no trauma) Yes - 79 f 28 8 4 f 41
Chemical
Surgical (incision>
- _ _ No Yes No Yes
~~
48 48 72 72
i20 Z 69 670 423 558 $148 109 f 30 820 f 246 752 f 82 61 f 30 144 f 19 236f 61 78 f 13 663 i 178 8.50 i 333
* All animals sacrificed 24 hours after tumor cell injection. ** Administered 30” prior to tumor cell injection and during 24-hour period. t CPM-counts per min. t Each value is mean and S.D. of 12 animals.

28 CANCER January 1967 VOl. 20
culating tumor cells become arrested when trauma is not a factor, explanation when the latter is involved must be even more conjec- tural. However, information is available to provide some insight into the possible mecha- nisms involved. There is evidence that (a) the coagulation mechanism plays a role in the initial adherence of cancer cells and their sub- sequent development into overt metastases: (b) adhesion of tumor cells occurs most fre- quently in the microvasculature; and (c) tu- mor cells ordinarily traverse capillary beds. Moreover, the investigations of Knisely23 and of Gelin20 attracting attention to cell aggrega- tion or “sludging” of blood flow through the micro-circulation following trauma merit con- sideration in this regard.
The presence of metastases at sites of trauma may thus, in part at least, be due to increased adherence of tumor cells to vessels in the micro-circulation of such foci as a result of endothelial damage pursuant to the trauma and perhaps also as a result of alteration of peripheral flow and/or altera- tion in the coagulation mechanism. Conse- quently, i t might be reasonable to anticipate that agents, such as heparin and fibrinolysin, by preventing the formation of microthrombi and cell agglutination, could prevent the lodgment of tumor cells, permitting them to traverse capillary beds and become dispersed throughout the body. In fact, Agostino and Cliffton,l as previously noted, reported less metastases in hind legs following turpentine trauma when heparin and fibrinolysin were employed. This present study, however, fails to confirm the view that heparin will inhibit tumor cell lodgment. No difference in num- bers of tumor cells was observed in either traumatized or normal legs whether or not adequate heparinization was accomplished. Other studies by us13 also support the view that anticoagulants do not interfere with the development of metastases by inhibiting tu- mor cell lodgment.
Since low molecular-weight dextran reduces blood viscosity and reverses cell aggregation, resulting in increased peripheral flow, its use also might be expected to inhibit tumor cell lodgment. Yet, prior studies in our lab- oratory with dextranl4 have demonstrated the converse, or an enhancement of metasta- ses.
In this study tumor cells were inoculated both intravenously as well as intra-arterially. The latter route “may not allow clinical in-
terpretation because human tumor cells (lung cancer excepted) escape into the vein^."^ Yet, results in this study following both routes of injection were essentially the same. Although, as might be expected, more tumor cells gained access to the legs following direct intra-aortic injection, the per cent dif- ference between normal and traumatized legs was similar to that observed following intrave- nous inoculation.
Of special interest was the observation that the degree of local response to the trauma was related to the magnitude of the cell lodgment and tumor growth in the injured leg. Chemical trauma (turpentine), which produced the greatest inflammatory response, resulted in the greatest incidence and size of tumor growth. Even when tumor cells were inoculated, 7 days after injury the difference between the two legs was still pronounced. Clean surgical incision with its minimum of reaction, on the other hand, resulted in less of a difference in localization of tumor cells a t the site of trauma, and tumor growth was not observed following intravenous injection. The latter is in keeping with the observations of Vernick30 who failed to find metastases in the scars of 520 incisions made in rats after intravenous Walker tumor cell injection. In our experiments tumor growth did occur at the site of incision following intra-aortic in- jection. While there was an increased lodg- ment of cells in such sites following intra- venous injection, the numbers were perhaps insufficient to produce tumors before such animals died of lung metastases. Response to mechanical trauma was intermediate to the chemical and surgical injury.
Failure to observe a consistent difference in tumor cell lodgment between normal limbs of traumatized animals and control animals minimizes the role of “stress” or other systemic humoral factors in this phenomenon. I t has been suggested1 that an increase in blood flow as a result of the inflammatory reaction could be responsible for bringing more tumor cells to the area. T h e magnitude of aug- mented flow necessary to account for the results noted seems unlikely. I t has also been suggested3 that perhaps a substance elaborated by connective tissue may attract tumor cells or that the network of capillaries (some end- ing blindly) which are a part of granulation tissue trap circulating tumor cells in a favor- able environment. Such possibilities would seem to have little application in animals

No. 1 TRAUMA AND LOCALIZATION OF TUMOR CELLS - Fisher et al. 29
injected with tumor cells shortly after the trauma, although they may be significant in animals inoculated at a later time. Also, the importance of a highly cellular proliferating connective tissue resulting from the injury in aiding tumor stromatization, as has been sug- gested,22s 29 cannot be excluded.
While this study demonstrates that the in- creased number of tumor cells which may lodge at sites of trauma appear significant in accounting for greater tumor growth at such sites, it does not exclude the participation of other local factors. A local tumor growth- promoting factor, possibly a product of dead or dying normal cells, may be involved. Prev- ious work11 employing tissue homogenates from various organs, lends some support to this view. Moreover, enhanced cell lodgment has not been observed in livers subjected to a variety of traumatic factors which were noted to enhance hepatic metastases. These studies are the subject of another report.12 Further,
the present findings fail to provide evidence concerning the precise mechanism of such augmented lodgment of tumor cells at sites of trauma.
T h e hazards of translating findings from an experimental model to events which may occur in man are fully appreciated, yet to disregard the evidence relating trauma to metastases as being inconsequential appears equally inappropriate. There are many clini- cal observations that surgery, chemotherapy, and even irradiation (all forms of trauma) may augment metastases. Such modalities may change host-tumor-relationships allowing for unexpected neoplastic growth. In this regard it must be noted that surgeons have long practiced self incrimination for local recurrences of tumor following an “adequate” operation when actually these recurrences may have been the result of a biological phe- nomenon beyond his control, i.e., circulating tumor cells lodging at a site of trauma.
REFERENCES
1. Agostino, D., and Cliffton, E. E.: Trauma as a cause of localization of blood-borne metastases: Pre- ventive effect of heparin and fibrinolysin. Ann. Surg.
2. Alexander, J. W., and Altemeier, W. K.: Suscepti- bility of injured tissues to hematogenous metastases: An experimental study. Ann. Surg. 159:933-944, 1964.
3. Black, J. W.: The localization of metastatic Brown-Pearce carcinoma in granulation tissue. Brit. J. Cancer 18:143-145, 1964.
4. Cole, W. H., Roberts, S. S., Webb, R. S., Jr., Strehl, F. W., and Oates, G. D.: Dissemination of cancer with special emphasis on vascular spread and implantation. Ann. Surg. 161:753-768, 1965.
5. Crowley, J. D., and Still, W. J. S.: Metastatic carcinoma at the site of injection of iron-dextran complex. Brit. M e d . J. 1:1411-1412, 1960.
6. Ewing, J.: Modern attitude toward traumatic cancer. Archives of Path. 19:690-728, 1935.
7. Fisher, B., and Fisher, E. R.: Experimental studies of factors influencing hepatic metastases: 111. Effect of surgical trauma-with special reference to liver injury. Ann. Surg. 150:731-744, 1959.
8. - , and Fisher, E. R.: The interrelationship of hematogenous and lymphatic tumor cell dissemi- nation. Surg. Gynec. Obst. 122:791-798, 1966.
9. ~ , and Fisher, E. R.: The organ distribution of disseminated 51Cr labeled tumor cells. In press.
10. - , and Fisher, E. R.: Experimental evidence in support of the dormant tumor cell. Science 130 (3380): 918-919, 1959.
11. - , and Fisher, E. R.: Local factors af- fecting tumor growth. I. Effect of tissue homogenates. Cancer Res. 23:1651-1657, 1963.
12. - , and Fisher, E. R.: Liver trauma and enhanced metastases: Further investigations employing labeled tumor cells. In press.
161:97-102, 1965.
13. ~ , and Fisher, E. R.: Anticoagulants and tumor cell lodgment: An experimental re-evaluation. In press.
14. __ , and Fisher, E. R.: Experimental studies of factors influencing hepatic metastases: XVI. Rheo- logic alterations. Cancer Res. 26:183-192, 1966.
15. - , Fisher, E. R., and Lee, S. H.: The effect of alteration of liver blood flow upon experimental hepatic metastases. Surg. Gynec. Obst. 112:ll-18, 1961.
16. Fisher, E. R., and Fisher, B.: Experimental studies of factors influencing hepatic metastases. I. Effect of number of tumor cells injected and time of growth. Cancer 12:926-928, 1959.
17. - , and Fisher, B.: Experimental studies of factors influencing hepatic metastases: VII. Effect of reticuloendothelial interference. Cancer Res. 21 :275- 280, 1961.
18. - , and Fisher, B.: Experimental studies of factors influencing hepatic metastases: IV. Effect of cirrhosis. Cancer 13:860-864, 1960.
19. - , and Fisher, B.: Experimental studies of factors influencing hepatic metastases. XIII. Effect of hepatic trauma in parabiotic pairs. Cancer Res.
20. Gelin, L. E.: Rheologic disturbances and the use of low viscosity dextrans in surgery. Rev. Surg. (Phila.) 19:385-400, 1962.
21. Jewell, W. R., and Romsdahl, M. M.: Recurrent malignant disease in operative wounds not due to surgical implantation from the resected tumor. Surgery
22. Jones, F. S., and Rous, P.: On the cause of the localization of secondary tumors at points of injury. J. Exp. Med. 20:404-412, 1914.
23. Knisely, M. H., Bloch, E. H., Eliot, T. S., and Warner, L.: SIudged Blood. Science 106:431-440, 1947.
23:896-900, 1963.
58:806-809, 1965.
30 CANCER January 1967 VOl. 20
24. Lubarsch, 0.: Die Bedentung des Traumas fur Entstehung und Wachstum krankhafter Gewachse. Med. Klin. 8:1651-1654, 1912.
25. Raichev, R., and Andreev, V.: The problem of injury and the development of metastases. Khirurgija (Sofia) 13:1045-1047, 1960. In Excepta med. Amst. Sect. XVI, 10, 298.
26. Rajam, P. C., Jackson, A. L., and Black, S. H.: The intracellular labeling of Ehrlich mouse ascites tumor cells with radiochromate. J . Lab. CZin. Med.
27. Robinson, K. P., and Hoppe, E.: The develop- ment of blood-borne metastases-effect of local trauma and ischemia. Arch. Surg. 85:720-724, 1962.
28. Selecki, E. E.: A study of the metastatic distribu-
51:767-772, 1958.
tion of Ehrlich ascites tumour cells in mice. Australian J. Ex$. B i d . Med. Sci. 37:489-498, 1959.
29. Vasiliev, J. M.: The role of connective tissue proliferation in invasive growth of normal and ma- lignant tissues. Brit. J . Cancer 1?:524-536, 1958.
30. Vernick, J., Garside, G., and Hoppe, E.: Lack of growth of intravenously inoculated tumor cells in peripheral wounds. Cancer Res. 24:1507-1508, 1964.
31. Willis, R. A.: The Spread of Tumours in the Human Body, 2nd Ed. London (Butterworth), 1952.
32. Zeidman, I., McCutcheon, M., and Coman, D. R.: Factors affecting number of tumor metas- tases; experiments with a transplantable mouse tumor. Cancer Res. 10:357-359, 1950.
p. 299.
Erratum T h e September 1966 issue of CANCER carried a n error i n the abstract for
“Morbidity from Cancer i n Lebanon” by Kamal T. Abou-Daoud, MD. On page 1293 the eleventh line of the abstract reads, “Cancer of the lung was twice as frequent i n Moslem as i n Christian males.” T h e correct sentence is, “Cancer of the lung was half as frequent i n Moslem as in Christian males,” as is evident from the text.