Trauma – Update from Clinical Examples...Trauma – Update from Clinical Examples Paul D. Eleazer...
62
1 Trauma – Update from Clinical Examples Paul D. Eleazer University of Alabama at Birmingham DDS 1947 Waycross 1 2 4 3 5 6 7 8 9
Transcript of Trauma – Update from Clinical Examples...Trauma – Update from Clinical Examples Paul D. Eleazer...

1
Trauma – Update from Clinical Examples
Paul D. Eleazer
University of Alabama at Birmingham
DDS 1947
Waycross
1
2
4
35
6
78
9

2
Guidelines Guidelines are not guarantees
Guidelines change
Most trauma guidelines are based on anecdotes / “Expert Opinion”
Very few good research projects exist
Background Andreason, Danish oral surgeon - schools
AAE Guidelines – 20032004
Pedo’s are different
Recent lit.
Dentaltraumaguide.org
Exhaustive databaseThousandsSince 1962Great example of EBD
Many categories have few examples
Jens Andreasen, et al.

3
Risk / Prevention Girls fall / Boys fight (sports)
Primary tooth injuries peak @ age 2-3
Permanent tooth injuries peak @ 9-10
Trauma to the oral cavity is a Hugepublic health problem worldwide
Risks
Young
Male
Previous trauma
Crown fracture is most common
Procumbent Anteriors

4
Prevention Helmet with FacemaskMotorcycle trauma
Football
MouthguardDistributes force
May transmit force to spine, brain
Outline AssessmentPhysical Exam
History
Radiography
Head and Neck Exam
Cases
Prognosis / Follow-up visits
MD / Emergency Room Referral
Tetanus – wi/ 5y=OK
C-spine
Swallowed / Aspirated matter
Soft tissue suturing ?

5
Smooth Muscle in Artery will stop bleeding, IF CLEAN CUT
artery
Capillaries and veins continue to bleed
Middle Meningeal ArteryPasses into cranial vault in central base of brain Ragged Tear

6
Brain Movement = Easy to break MMA
Hematoma from ruptured MMA
Brain protein between microtubules ruptures with force
Microtubules inside neurons are paths for chemical transport, protein (tau) between tubules breaks when the brain moves too much and stops suddenly. Neurons lose function(die)
Shenoy, U Penn, Biophys J, 2013

7
MD / Emergency Room Referral
Tetanus – wi/ 5y=OK C-spine Fx Swallowed /
Aspirated matter Soft tissue suturing ? Occipital Artery tear? CSF leak Basilar Skull Fx
Bleeding from ear canal = really bad
Assessment - History
Force- direction and magnitude
Did tooth move? Bleed?
Consider fulcrum for fx.
Soft tissue Tear ?
PDL Compression ?
Root / Bone Fracture ?
8
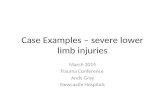
Assessment – Dental X-rays
Different horizontal and vertical angles
See fx / resorption
Cervical spine views for vertebral fx.
Vertical angle radiographs
Is this a fx?
What about this?
Change vertical angle
9
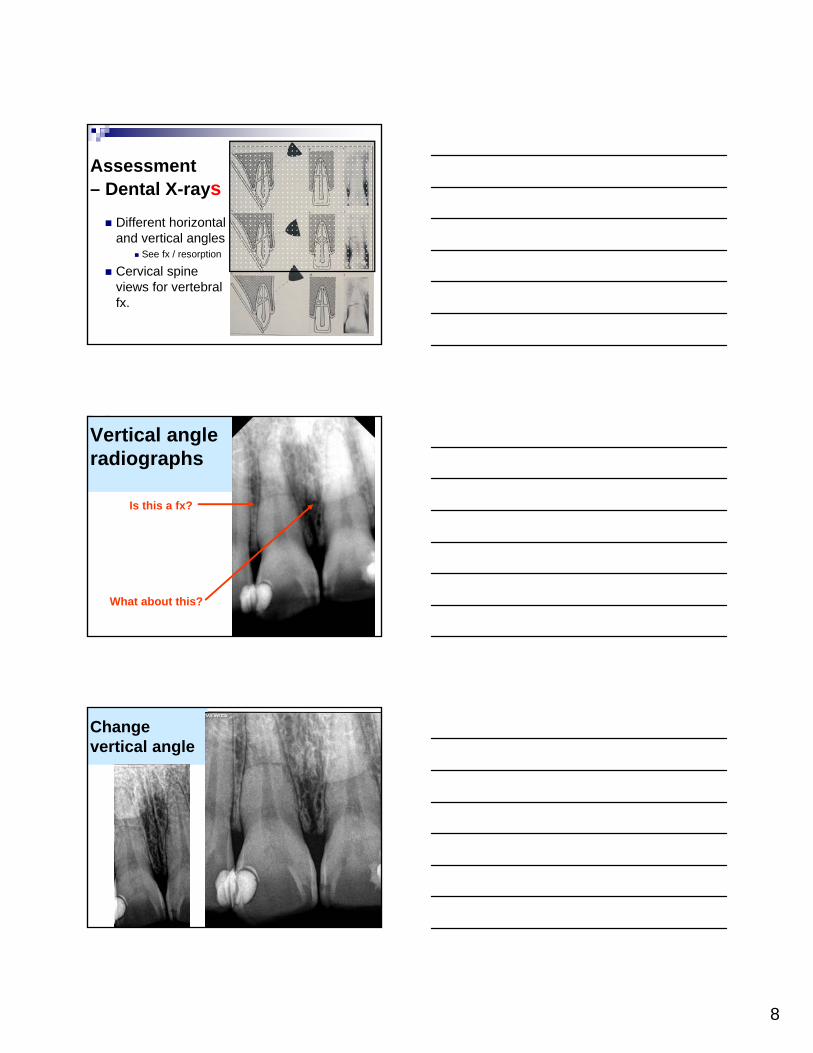
Assessment – Clinical Exam
Mobility / Percussion (Auscultation) Indicates PDL tear
DisplacementConfirm that root is repositioned
Splint
Pulp tests (negative not reliable)
Discoloration = Intrapulpal Bleed
Foreign material embedded in soft tissue
Validity of Pulp Tests, All Cases
Linda Levin, JEndo 12-09 and Andreasen text 3rded. pp. 196-215
EPT-sensitivity=.71-.93, specificity=.92-.96
Cold – .68-.92 .70-.93
Heat – .68-.86 .41-.81
Laser Doppler 1.0 1.0
May need to wait 6 w. for accurate test (longer?)
+ test early = very good sign
Concussion
Fracture – enamel only; enamel + dentin; crown only; w/ or wo/ pulp exposure
Discolorations
Subluxation and Luxation Intrusion – surgical reposition or orthodontic extrusion
Extrusion – Lateral
Avulsions – Replanted in field, in mouth, in Medium, dry time
Resorptions / Ankylosis
Fractures
Pulpal Regeneration
The Trauma Continuum

10
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
Concussion
Check for foreign body in lip / tongue / lung / stomach
Watch for symptoms
Microfracture of enamel ?
Case Study
Courtesy Dr. Jim Tinnin
Love, Endod Dent Traumatol 1996
Concussion can allow bacteria into pulp
16 Intact teeth received impact injury
No visible fracture or luxation
7 had bacteria in pulpConclusion: Micro enamel/dentin infractions
May be wise to seal enamel

11
Concussionsusually heal
BUT, can result in pulp necrosis
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
Pulp cap
Pulpotomy
Pulpectomy ______
Soft tissue
Crown Fractureenamel or enamel + dentin,w/ or wo/ pulp exposure
Bonded restoration / Bond piece back on
Pulp Cap (Frank or near exposure)
Pulpotomy
Pulpectomy (Apexification/Apexogenesis)
Pulp prognosis degrades w/
larger exposure, time open, pt’s healing, pulp blood flow

12
Enamel Only Fractures
Dr. Jim Tinnin
BUT #8 Discoloration = Previous Trauma
Enamel and Dentin, Pulp Intact
Dr. Jim Tinnin
Where did the Incisal Edges go? Lip ?
Bacterial ingress into pulp minimal for few days, (extreme thermal pain)
Dr. Jim Tinnin

13
Crown Fx
= energy dissipated
= usually heals
Rule Breaker
Accident history may have disclosed a bodily blow
in addition to enamel fracture
Why Endo ?
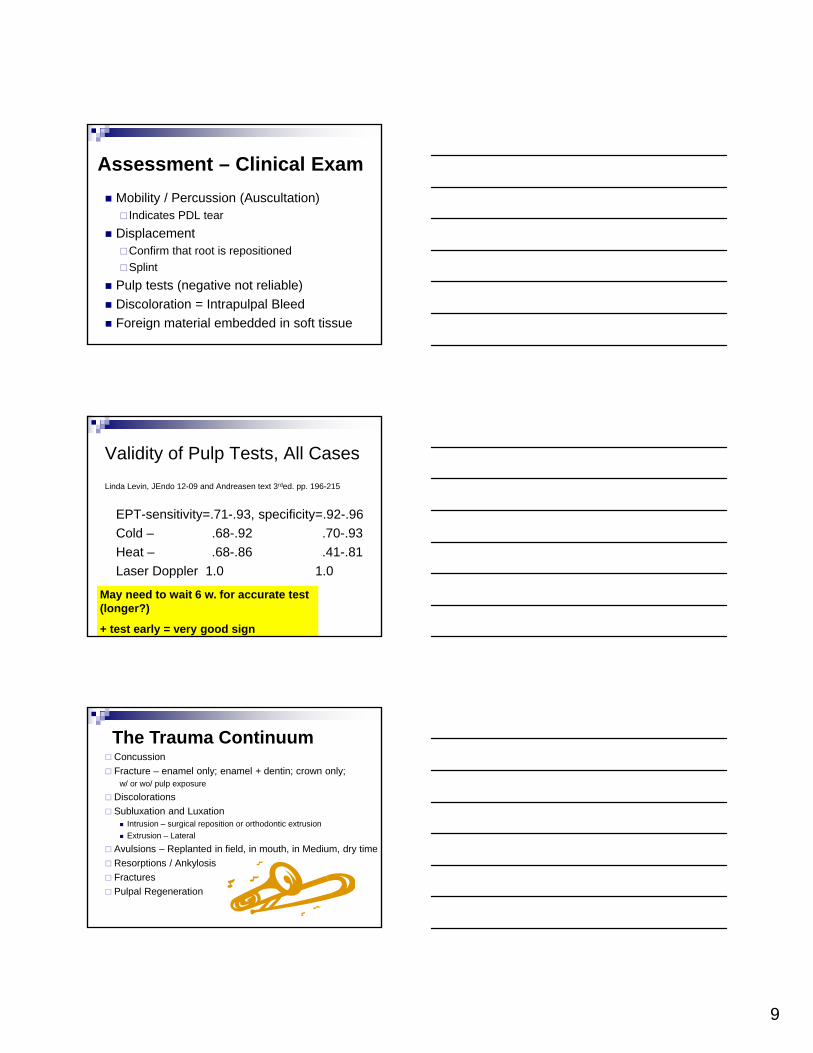
Two (+) Blows
Tooth Loose ?
14
Two Blows -#7 and 8 needed endo –#9 healed OK
Get a Good history
Required Endo #7 & 8
Concussion in addition to dentin-enamel fx
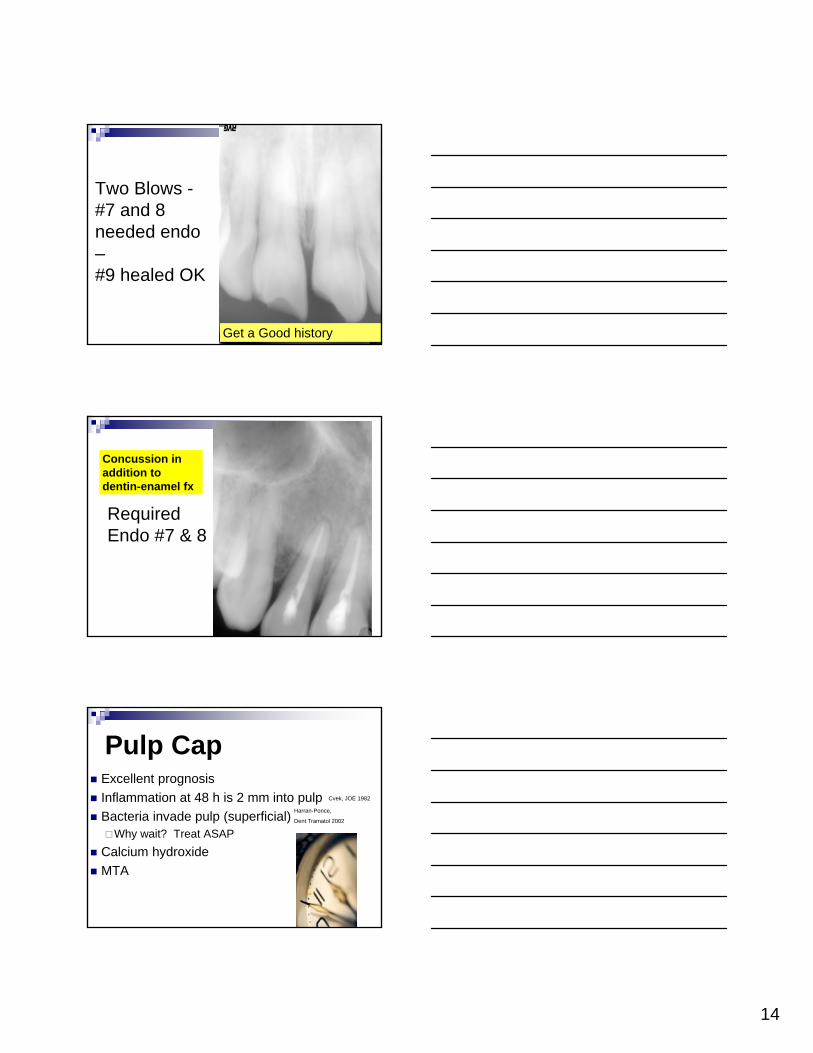
Pulp Cap Excellent prognosis
Inflammation at 48 h is 2 mm into pulp
Bacteria invade pulp (superficial)Why wait? Treat ASAP
Calcium hydroxide
MTA
Cvek, JOE 1982
Harran-Ponce,
Dent Tramatol 2002

15
Closed Apex Prognosis (Statistics mean nothing if you are the one)
Pulp cap = 99%
Pulp Prognosis (open apex =10% better)
Pulp OK
Let’s Build a Chart
Pulpotomy Cut to level where bleeding stops by itself
(No vasodilation = no inflammation)
Best wound with water-cooled large round diamond Granath & Hagman
Deep pulpotomy w/ open apex
MTA ?
Max. Time before pulpectomy:
11 days (Andreasen)
External resorption visible microscopically
Apexification vs. apexogenesis (pulp vital)
Conclusion: Pulp tests not reliable
Sooner is better !
11
Pulpectomy

16
Always, Always, Always Use aRubber Dam
File Appendix
Pulp Exposed 4-98, MTA Pulpotomy
Dr. Jim Tinnin
Pulp Still OK @ 40 m.
Dr. Jim TinninAPRIL ‘98AUGUST ‘01

17
Soft Tissue Laceration (multiple small sutures)
Abrasion
Contusion (bruise)
Debride well
Heals better if moist (Neosporin Ointment)
Peridex for intraoral wounds
Neosporin has 3 antibiotics,Ointment stays moist
Neosporin + pain relief swaps bacitracin for local anesthetic
“N” Drugs
Neosporin (Neomycin, Polymyxin B, analgesic)External topical, not absorbed thru skin
Neomycin – absorbed thru m. memb. Nystatin (N.Y.State lab) disrupts fungal
cell walls, topical, oral (not absorbed) Nizoral (ketaconazole) inhibits fungal
sterols, our corticosteroids, oral dosing systemic absorption
antibacterial antifungal
18
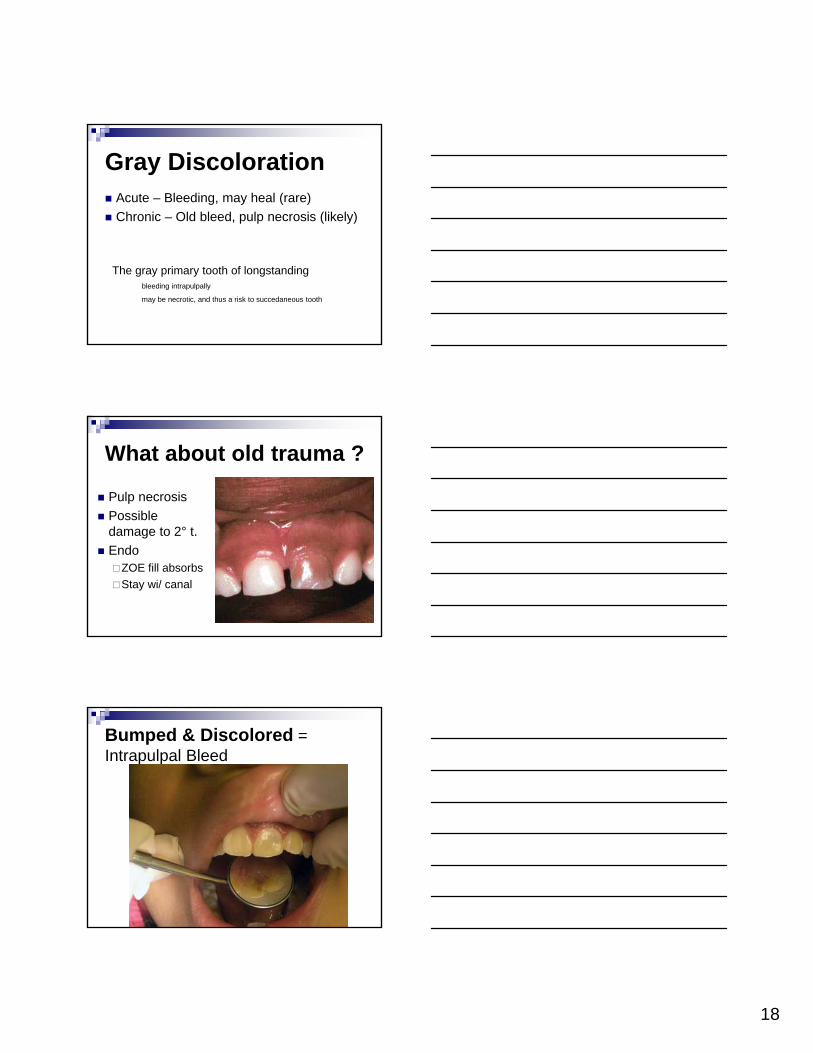
Gray Discoloration Acute – Bleeding, may heal (rare)
Chronic – Old bleed, pulp necrosis (likely)
The gray primary tooth of longstandingbleeding intrapulpally
may be necrotic, and thus a risk to succedaneous tooth
What about old trauma ?
Pulp necrosis
Possible damage to 2° t.
Endo ZOE fill absorbs
Stay wi/ canal
Bumped & Discolored = Intrapulpal Bleed
19
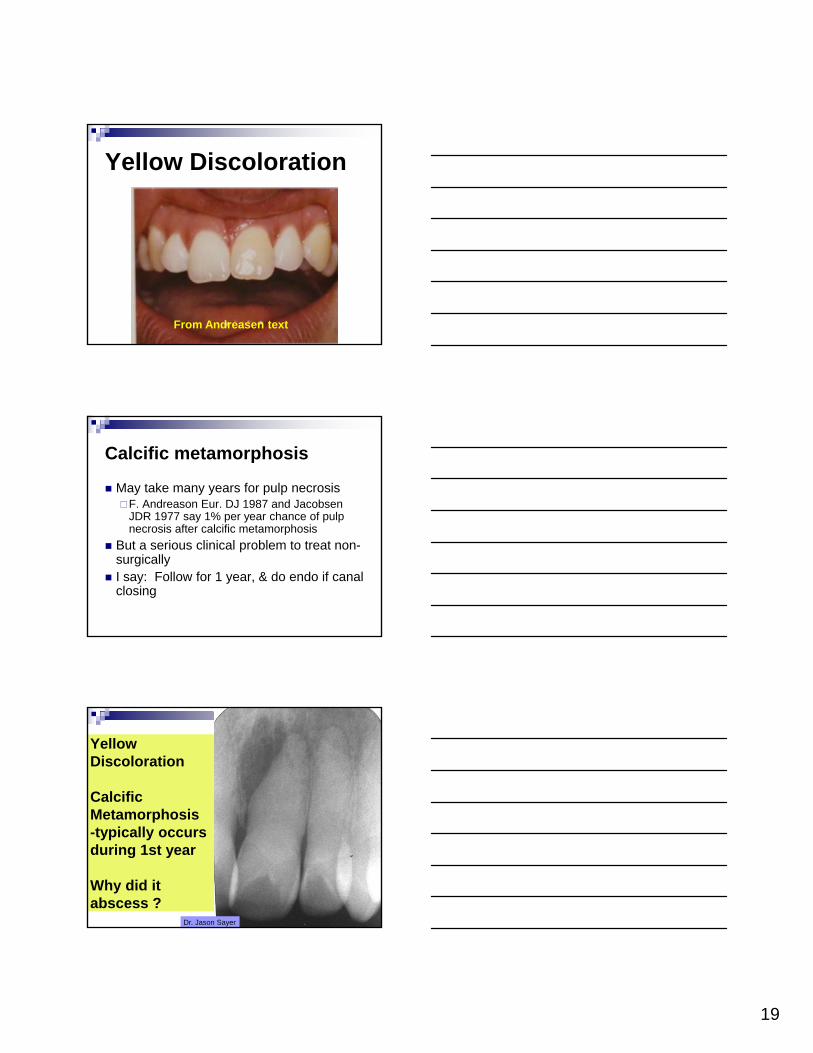
Yellow Discoloration
From Andreasen text
Calcific metamorphosis
May take many years for pulp necrosisF. Andreason Eur. DJ 1987 and Jacobsen
JDR 1977 say 1% per year chance of pulp necrosis after calcific metamorphosis
But a serious clinical problem to treat non-surgically
I say: Follow for 1 year, & do endo if canal closing
Yellow Discoloration
Calcific Metamorphosis -typically occurs during 1st year
Why did it abscess ?
Dr. Jason Sayer

20
Calcific Metamorphosis patient- dead stop - note lateral
position of radiolucency
Dr. Jason Sayer
Calcific Metamorphosis patient- note lateral
canal
Dr. Jason Sayer
#8 high school football trauma -Now age 74 and painful74-17 = 57 !
3-4 mm shorter
21
65 y o female #7 painCalcific metamorphosis or deep restoration calcified canal ?
Status of #8?
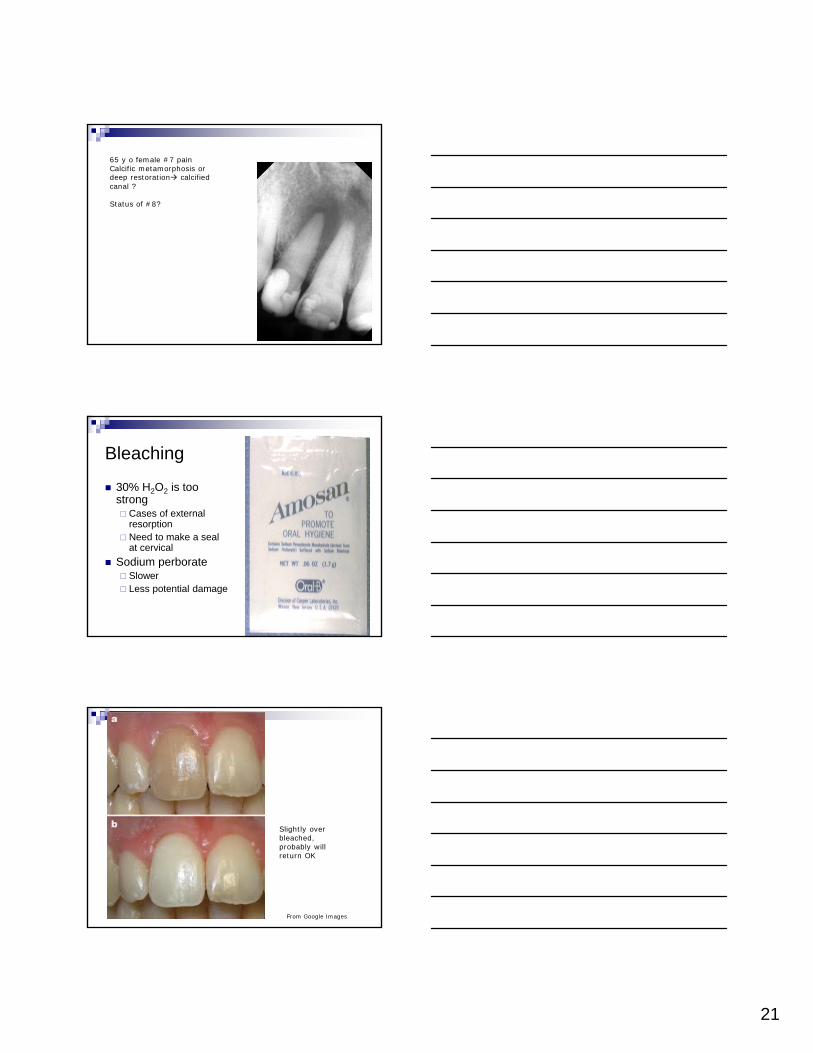
Bleaching
30% H2O2 is too strong Cases of external
resorption Need to make a seal
at cervical
Sodium perborate Slower Less potential damage
Slightly over bleached, probably will return OK
From Google Images

22
External vs. Internal Bleaching
H2O2 reaches pulp wi. 15 min. (Cooper, JOE, 92) Apparently pulp neutralizes chemical wo/ permanent damage
Sensitivity often increases dramatically (weeks)
Carbamide peroxide = 1/3 of [H2O2]
Heat degrades proteins (not for vital bleach)
Healing = Sometimes a surprise
49 years ago the patient received a trauma to #9, with subsequent pain then drainage. The patient, then a 16 year old girl, refused to allow extraction. The dentist attempted endo, but the drainage persisted for several years (with the patient still refusing extraction).
Eventually the drainage stopped – WHY ?
What killed intracanal bacteria ?
Asymptomatic w/ good bone, but crown fx at age 65, endo thru crown
3 year recall, new crownFirst file size = size at pulpal death
Resorption @ root end

23
Fell and Bumped Chin Traumato Mandibular Anteriors
How Many Need Endo ?
Test Max. too
7 Month Result –
Asymptomatic, Lateral still tests vital
Bone fill beginning
Cases: Concussion
Fractures – crown – root Intrusion Subluxation Luxation Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
24
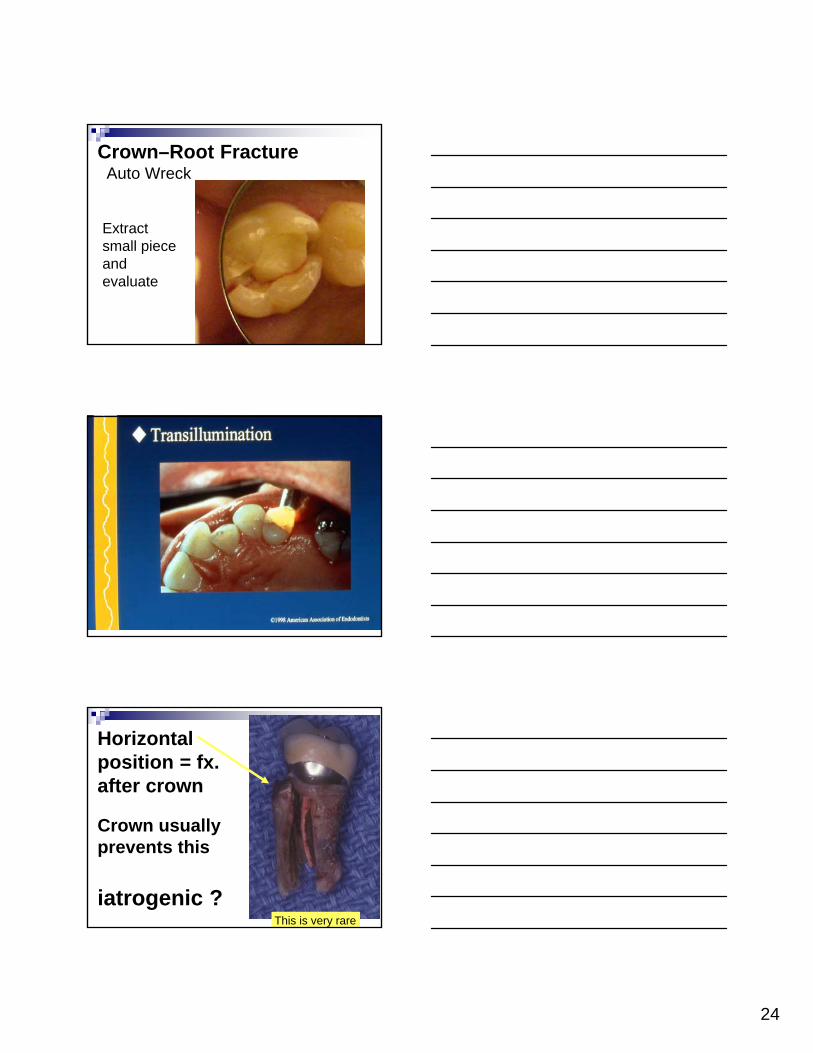
Crown–Root FractureAuto Wreck
Extract small piece and evaluate
Crown usually prevents this
iatrogenic ?This is very rare
Horizontal position = fx. after crown

25
Root FractureAngle and Force of Blow Level of Fracture ?Mobility ? Splint 3-4 weeks or more Hope for cementum “callus” Post that lutes two pieces ?
avoid cement into bone
Some Possible Fractures
Cusp Fx. Incomplete Fx. Hopeless Do these exist ?
Fractured from apex:Natural or Spreader ?

26
Mobility Issue
Dr. Chris Fleming
Apical segment did not move, and is likely vital
When to debride pulp ?
Do MTA to fracture ?
Move broken part in and splint
Horizontal Root Fx.Usually apical segment is vitalAvoid cement in fracture line
Severe Inflammation
Old Trauma, Failed Pulp Cap
Dr. Jim TinninCa(OH)2 x 6 m
G-P Fill @ 6 m
External Resorption

27
Cut threads is apical segment and draw coronal part tight
Minimal threads needed
Seal canal w. MTA slurry ?
Treatment for Crestal Level Fx.or Intrusion of whole tooth
Surgical extrusion
Orthodontic extrusion
Implant

28
Bone Crest is least favorable root fracture
Kerbl & Eleazer
Root FractureTraumatic decoronation #22
Kerbl & Eleazer
Cases: Concussion Fractures – crown – root
Intrusion Subluxation Luxation Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration

29
Intrusion Very poor pulpal prognosis
High risk to succedaneous tooth
Surgical extrusion
Orthodontic Extrusion
Antibiotic(s) in canal may decrease ext. root resorption
Prognosis Pulp Prognosis is Based on:Time of compression of vessels (1-2 hours ?)
Root Prognosis is Based on:Damage to cementum / PDL and infection
Intrusion Controversy Andreasen says pulpal necrosis almost
100% External resorption highly likely.
My dental school: Let it re-erupt
Saroglu (OOO2006 – 102(4):e60-5.
5 cases of permanent teeth w/ open apexes that spontaneously re-erupted

30
Let it Re-erupt ?Wigen (Dent Traumatol 2008)
35 of 37 primary teeth re-erupted in 3-12 months
7 forcefully erupted w/ surg and 7 w/ ortho
43% remained vital @ 4 y. (range 1-12y)
Cunha (Endodont Dent Traumatol 1995)
Severe blow in dog deep intrusion
All re-erupted wi/2 months
O.R. Case - Intrusion, Surgical Access to Linguals Dr. Brad Alley 9-04 8 w post trauma, Mixed Dentition = no ortho extrusion
Open Apexes
MTA Fills
Bradley Alley 9-04

31
O.R. Case Bradley Alley 9-04MTA Fills
Orthodontic Extrusion
Endo
Post w/ hook
(cut trans-septal fibers)
Elastic traction to ortho wire (1 week)
Stabilize (1 month)
Ortho wire allows direct extrusive force from hook cemented in canal

32
Elastic in position
Ortho Extrusion - 5 mm in 1 m.
Dr. Mark Essner
Ortho Extrusion
Gingivectomy to allow pulpectomy
Courtesy Dr. Frank Kerbl
33
Cases: Concussion Fractures – crown – root Intrusion
Subluxation – Luxation Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
Moved, but back in place by itself
= PDL tear
Subluxation (PDL tear, moves back into position)
Check occlusion
Splint (none / light for 7-10 days)
Pain pills (NSAIDs)
Soft diet
CHX rinse bid
Case Study
Sub-Luxationor
Luxation
Note Wide PDL
Is Occl. OK?

34
Closed Apex Prognosis (Statistics mean nothing if you are the one)
Pulp cap = 99%
Concussion = 90%
Subluxation = 75% -Calcif. Meta.10% 20%
Pulp Prognosis (open apex =10% better)
Pulp OK
Resorption / PDL
Cases: Concussion Fractures – crown – root Intrusion Subluxation
Luxation - Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
Still out of place,
? Blood supply
Lateral, Extrusion,
Intrusion
Luxation(Moved but still in socket)
Check occlusion
Splint (none / light for 7-10 days)
Pain pills (NSAIDs)
Soft diet
CHX rinse bid

35
Luxations Lateral luxation Intrusive luxation Extrusive luxation
Splint lightly for 1-2 w.Some mobility prevents ankylosis
Bone fracture needs more stability x 6-8 w.
Splint Maybe no splint
Light, brief = reduce ankylosis w/ movementBond wire or heavy fishing line
Titanium mesh
Attach to firm teeth first, traumatized one last
Splint 3-4 weeks (longer)(more rigid) for alveolar fx or mid-root fx (avoid cement in fx.)
If you MUST
Not like this !

36
Attach wire to sides, then lute avulsed teeth
Debride canals ASAP, Splint for 10 days, Ca(OH)2 for ___
TTS Titanium mesh splintAdatia & Kenny J Cal Dent Assoc 2006
Von Arx et al Dent Traumatol 2001
Patterson Dental $47.00
Medartis

37
Estimate Force, DirectionFacial plate fractured & root trapped
Pressure may result in resorption, or fracture
Must pull down to reposition
How far will pulpal vessels stretch before rupturing?
About 2 mm
Can vessels ends rejoin ?Maybe, but rare
Plan on Endo if moved >2 mm, dying pulp has NO BENEFIT,
remove ASAP
38
Closed Apex Prognosis (Statistics mean nothing if you are the one)
Pulp cap = 99%
Concussion = 90%
Subluxation = 75% - Calcif. Meta. 10% 20%
Extrusion = 15% - Calcif. Meta. 60% 20%
Lateral lux. = 10% - Calcif.Meta. 60% 30%
Alveolar fx. = 10% 100%
Intrusion = 0%??? 100%
Root Fx. = varies – PDL/resorption 60%
Pulp Prognosis (open apex =10% better)
Pulp OK
Resorption / PDL
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation
Avulsion Resorption Ankylosis Bone fracture Pulp Regeneration
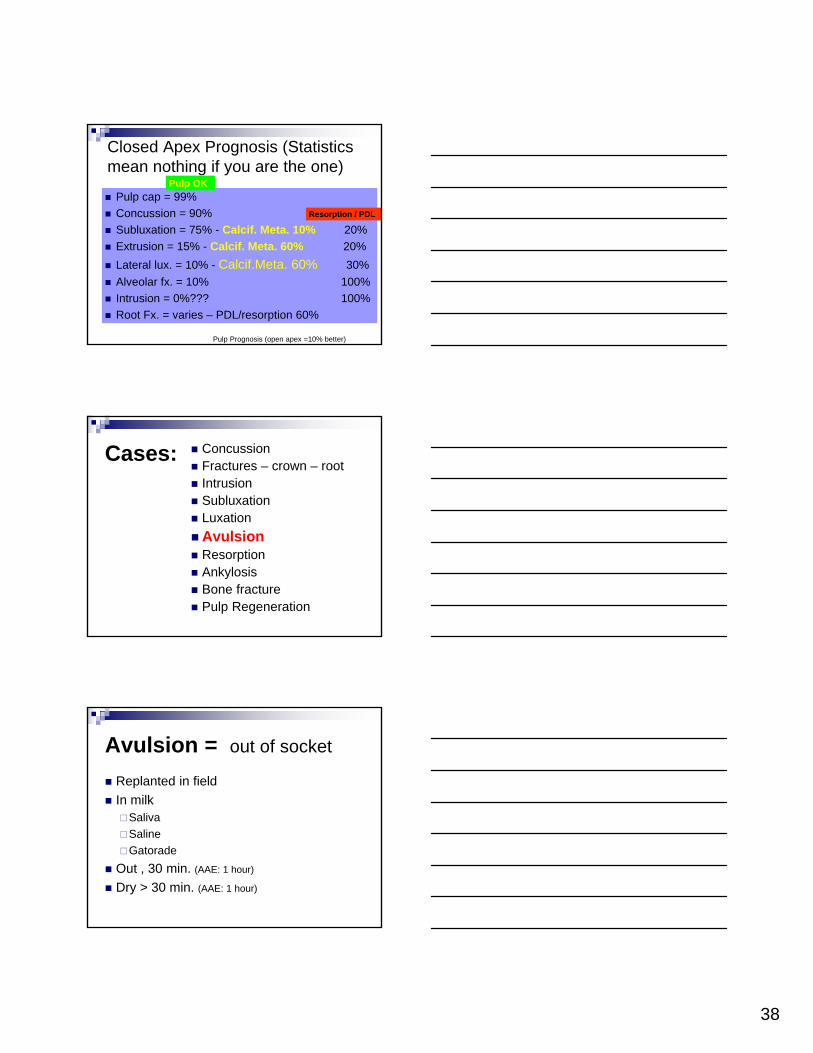
Avulsion = out of socket
Replanted in field
In milkSaliva
Saline
Gatorade
Out , 30 min. (AAE: 1 hour)
Dry > 30 min. (AAE: 1 hour)

39
Replant Permanent Teeth
If not out too long
If not mistreated (Kleenex)
Tetanus
Antibiotics
Splint briefly50% PDL strength @ 2 w
100% PDL strength @ 8 w.
Avulsions: Clot in socketRemove gently or Not (do not damage PDL)
Open apexDry > 1 h. = generally not rec. to replant
Closed apexEndo for sure
Pulpectomy ASAPAntibiotics + corticosteroid in canal
Avulsed Primary teeth
Do not replant due to damage to succedaneous t.
Tooth may already be damaged
Infection may aid / cause resorption

40
Primary tooth injury can impact tooth bud Study force
Treat before infected
Generally, extract damaged primary tooth
Primary Tooth Luxated / Avulsed = Leave It Out
Dr. Jim Tinnin
This is a Problem !Permanent Teeth Avulsed in Mixed Dentition
Dr. Jim Tinnin

41
Best Case Avulsion Replanted in fieldHold by crown, rinse, replant (even backward)
Light splint x 7-10 days (No splint)
Endo ASAP
Antibiotic / Tetanus (TIG / booster after 5 y. / q 10 y for all)
50% PDL strength @ 2 w (100%@8w) Mandell
Avulsed Tooth “high”
Compress clot, maintain pressureMay need splint
Occlusal adjustment
2nd best In mouth
Saliva is good
Hold in mouth (Do not swallow)
Antibiotic
Tetanus

42
In transport medium Via-Span
Hank’s Balanced Salts solution
Milk
Physiologic saline
Antibiotic
Tetanus
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation Avulsion
Resorption - Ankylosis Bone fracture Pulp Regeneration
Internal – External
Replacement – Inflamm.
Long time Out, Dry Case of long dry time (Kleenex)(1/2 to 1 h)Strip PDL to minimize foreign body rejectionSoak in fluoride to retard resorption
Bisphosphonate ? Emdogain, GEM 21, other growth enhancer(s) Load canal w/ calcium hydroxide / iodoform
AntibioticTetanus

43
Straumann Emdogain
Made from pig tooth buds in Sweden
Works nicely in perio
Again available in USUS FDA banned in 2007 until factory passed
inspection
Chemically remove smear layer and apply to root
1-800-448-8168
Growth- Factor Enhanced Matrix 21s
GEM 21s Osteohealth – 631-924-4000
Recombinant Platelet-Derived Growth Factor (rhPDGF-BB), and a synthetic bone matrix, Beta-tricalcium phosphate (ß-TCP)
FDA approved (2006) for perio regeneration
TraumaticExtrusion time
Extruded 1 month ago
Pulp #8 test vital to cold and EPT
Splint ? Occlusion ?
Case Study

44
Oblique Fracture
X-Trac Device1. Drill canal to size
2. Thread in self tapping screw
3. Place plate over tap-screw
4. Apply pressure w/ jack screw
A-Titan Instruments $2500.00
877-284-8261 Hamburg, NY
Implant
Bone Graft at 6 w.

45
Resorption – need break in pre-dentin / pre-cementum
Internal External
Inflammatory Replacement (ankylosis)
Osteoclasts activated by inflammation
Problem: Damage from trauma or forceps to reposition tooth
Replacement Resorption(Ankylosis)
Poor Prognosis
Body “sees” dentin as bone
Rapid External Resorption
Ca(OH)2 in canals failed on #7. Note crestal bone loss.
Inflammation 2 weeks after Ca(OH)2
Concussion from Horse Kick

46
Note Irregular Outline of Pulp w/ External Resorption
Internal Resorption – Excellent Prognosis – Did not Perforate to PDL Blood Supply
Internal resorption May have begun externally
True internal resorption has excellent prognosis if treated before perf. into PDL
? Prognosis

47
Perforated facial of root = must do surgery, perio defect
Geristore is best bet
Geristore
Dual Cure
Hybrid Ionomer-Composite
Very biocompatible
DenMat
Also need Etchant, Primer, Clear Matrix Strips, Finishing Instruments (#12 Blade, Burs, Sanding Strips)
Geristore for external resorption

48
External ResorptionMay need a Cone Beam
External Resorption at Epithelial Attachment, Extr. by Dr. Geurs
Extensive weakening of tooth
49
Clinical Crown Esthetically bonded in Position - Dr. Liu
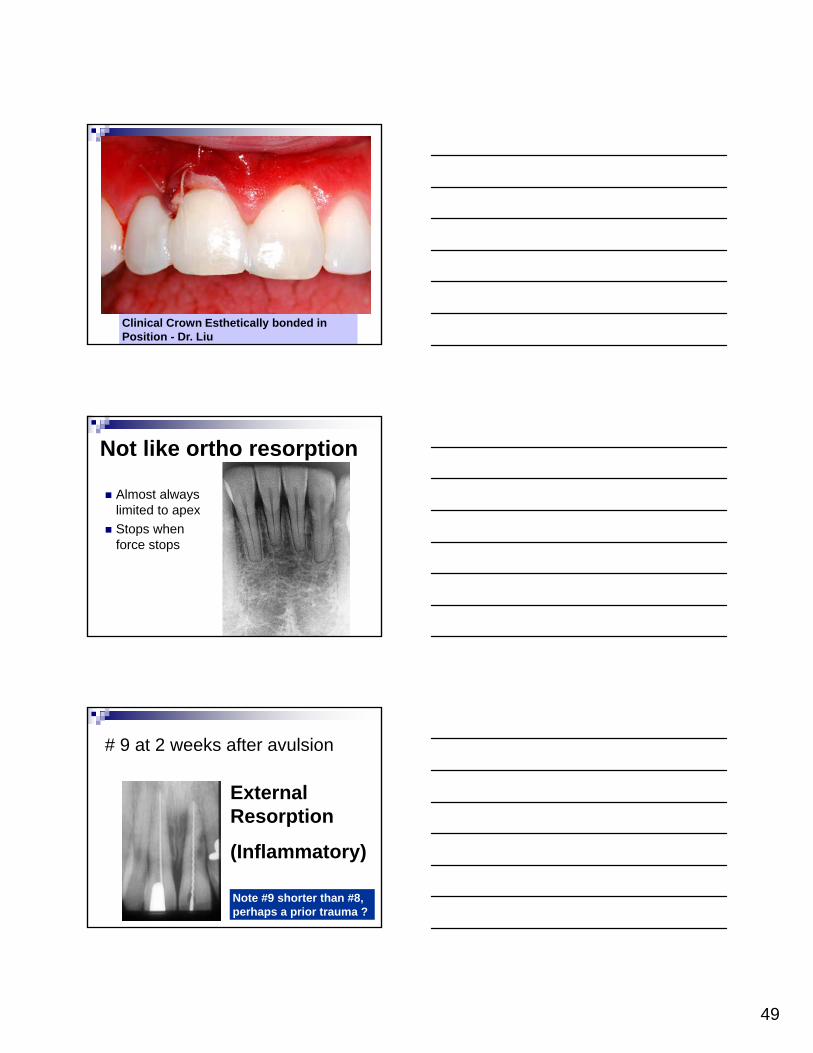
Not like ortho resorption
Almost always limited to apex
Stops when force stops
# 9 at 2 weeks after avulsion
External Resorption
(Inflammatory)
Note #9 shorter than #8, perhaps a prior trauma ?

50
Reduce Resorption Calcium hydroxide
Penicillin (Hammarstrom, Endo. Dent. Traumatol 1986;2:51-3)
Tetracycline (Selvig, Scand JDR 1992;100(4):200-3)
Stannous Flouride (ibid.)
Corticosteroid (Trope,J Endo 2009;35:663-7)
Calcium Hydroxide Decreases resorptionCounteracts osteoclast’s HCl
Coagulation necrosis = stimulates osteoid
Ca45 shows new calcium not from Ca(OH)2
Antibacterial
But it Weakens dentin (White JOE 2002)
& Kills bone and nerve
Calcium Hydroxide Needs a second germicide
Sigma-Aldrich
800-558-9160
#10,945-2 $10.40/5g
50-50 Iodoform & Ca(OH)2
51
We have grown E. faecalisin Calcium hydroxide
2004 UAB Study Chris McHugh: E. faecalisgrows in pH 11
Commercial preparations pH 10 USP Ca(OH)2 pH 12 2012 UAB Study Jason Latham: E. faecalis
grows in Calasept (pH 12+)First growth after 4 m, now adapted and grows
faster
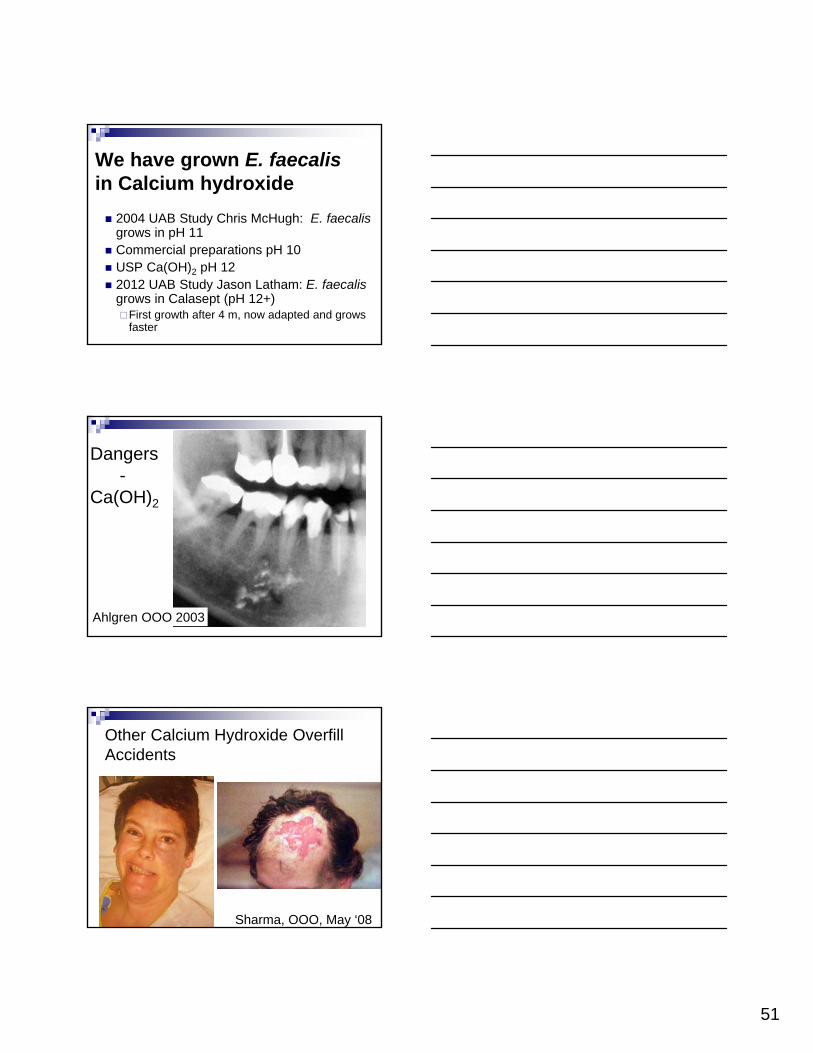
Dangers-
Ca(OH)2
Ahlgren OOO 2003
Other Calcium Hydroxide Overfill Accidents
Sharma, OOO, May ‘08

52
Calcium hydroxide is dangerous
Lindgren, J Oral Maxillofac Surg ‘02
Clorox accident
JADA 2000
External Resorption
53
Stannous Fluoride + Doxycycline
Selvig Scand J Dent Res 1992;100:200-3.
Hx: 1% SnF2 chron. inflam. resorption/ankylos
Exp: dog teeth extracted, dry for 45 min.,
0.1% SnF2 x 5 min, then 1% doxy. X 5 min.,
85% root surface OK @ 4 w.
(control 33%)
Dilute Stannous Fluoride caused less cell damage, while enhancing healing
Corticosteroid in canal
Kirakozova…Trope JOE 2009;35:663-7.
Dog teeth 60 min. dry
outcome measure: pdl healing
0.05% clobetasol intracanal 56% healed OK
0.05% fluocinonide 32%OK
control 14% OK
No systemic c/s
My Thought Bacteria wi/ tubules may be cause of
resorption
Calcium hydroxide does not kill all bacteria (E. faecalis)
Need second germicide to boost Ca(OH)2
I favor 50:50 w. IodoformVitapex has 22% silicone oil

54
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation Avulsion Resorption
Ankylosis Bone fracture Pulp Regeneration
Ankylosis Sound (Auscultation)
Only part of PDL may ankylose
Block repositioning may work
Endodontic Endosseous Stabilizer Tri-Lock™ Endodontic Titanium ImplantsPark Dental Research, NYC
Al Frank (Dent Clin N AM – 1967)
Courtesy: Dr. Robert Barfield – healing @ 2-3 y, failed at 6 y –angled out buccal
55
Cases: Concussion Fractures – crown – root Intrusion Subluxation Luxation Avulsion Resorption Ankylosis
Bone fracture Pulp Regeneration
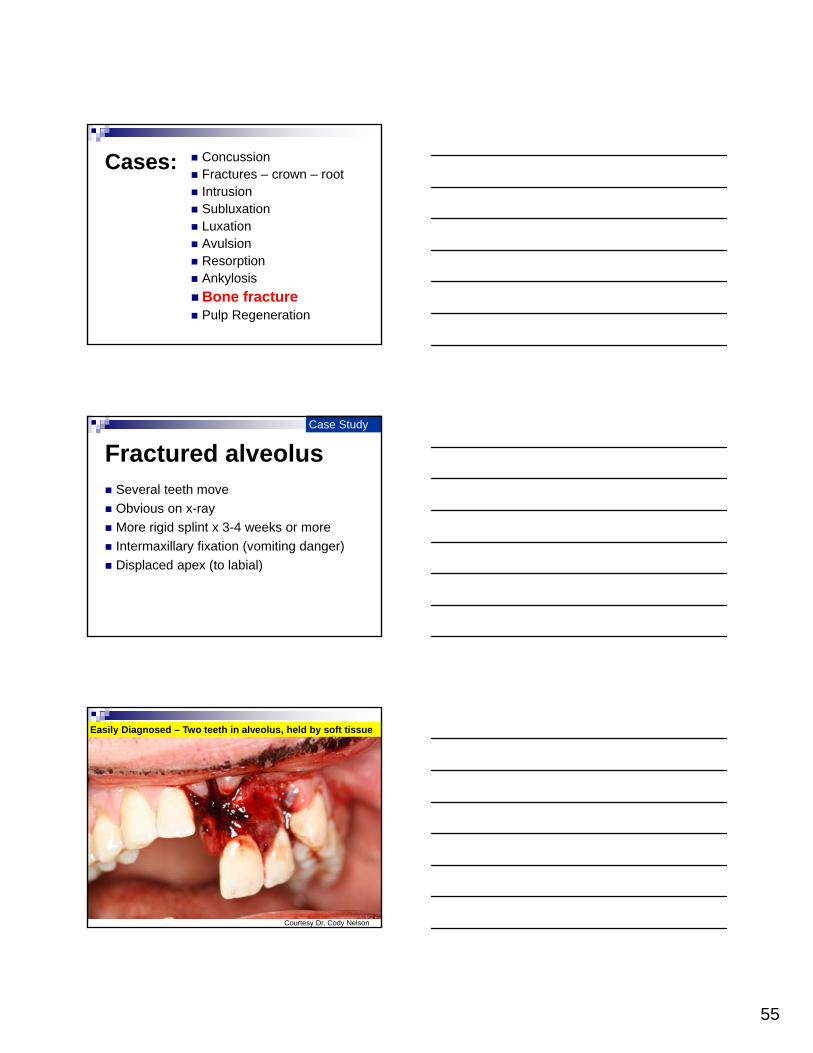
Fractured alveolus Several teeth move
Obvious on x-ray
More rigid splint x 3-4 weeks or more
Intermaxillary fixation (vomiting danger)
Displaced apex (to labial)
Case Study
Easily Diagnosed – Two teeth in alveolus, held by soft tissue
Courtesy Dr. Cody Nelson

56
Bridal wire applied from #’s 9 – 11 to re-approximate bone
Courtesy Dr. Cody Nelson
2008 Trampoline, 3 teeth pushed back w. alveolar fx. & splinting
2010 2 pulps died, why not 3?
Frequency of Mandibular Fractures
Deviation TO side of fx when opening

57
Alveolar Fx. – mixed-dentitionremovable/compos. splint
4-01
CourtesyDr. Steve Clark
4 teeth Move Together
6 m post, good color, EPT?
CourtesyDr. Steve Clark
1 1/3 y post = AOK
Note: Calcif. #26 canal
CourtesyDr. Steve
Clark
58
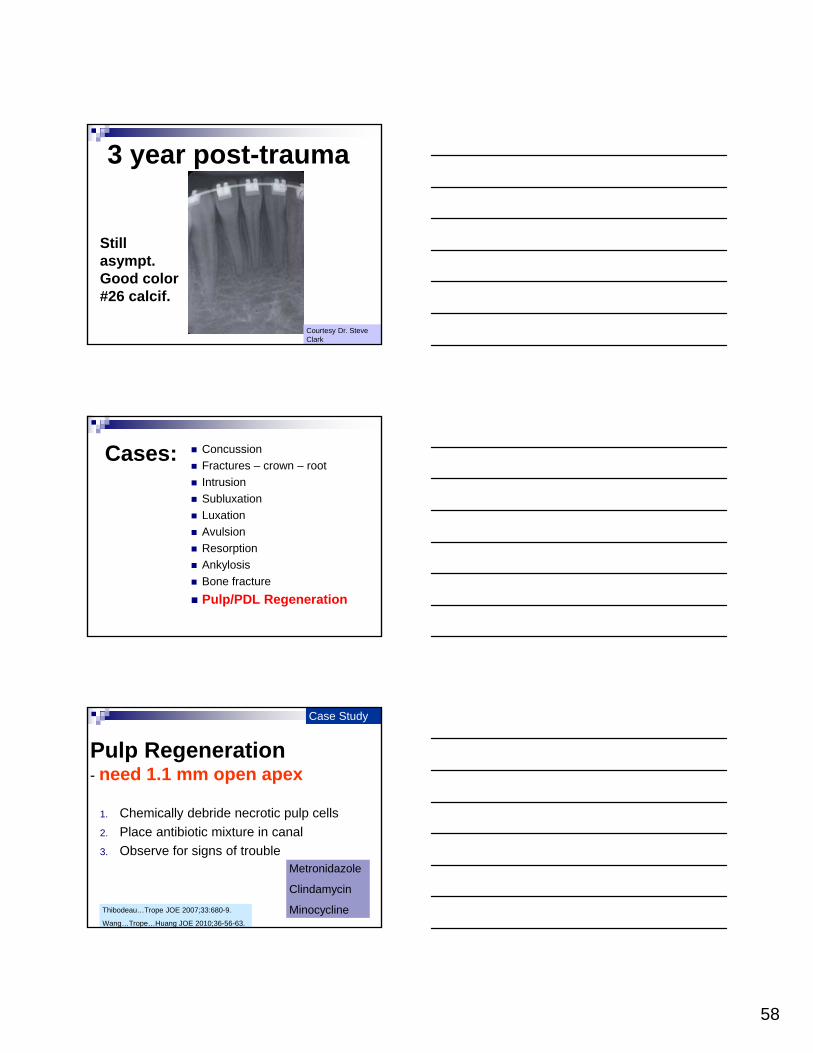
3 year post-trauma
Still asympt.Good color#26 calcif.
Courtesy Dr. Steve Clark
Cases: Concussion
Fractures – crown – root
Intrusion
Subluxation
Luxation
Avulsion
Resorption
Ankylosis
Bone fracture
Pulp/PDL Regeneration
Pulp Regeneration- need 1.1 mm open apex
1. Chemically debride necrotic pulp cells
2. Place antibiotic mixture in canal
3. Observe for signs of troubleMetronidazole
Clindamycin
Minocycline
Case Study
Thibodeau…Trope JOE 2007;33:680-9.
Wang…Trope…Huang JOE 2010;36-56-63.

59
Current Thinking for Pulp Regen.
ASAP: NaOCl debridement, instrumentation to min.110 file Dry Triple antibiotic paste (consider omitting tetracycline)
2 w. later: Saline irrigation of canal (Essner- 0.04% NaOCl = highest concentration wo/ cell
death) Induce bleeding from pulp stump (STEM CELLS) Preserve CLOT at mid root level Gently apply MTA over clot
George T-J. Huang
SCID Mice
Human roots – 6 mm long – implanted SQcanals reamed to 2 mm
1 mm of an end plugged w/ MTA
5 mm wide, open canal space
Human stem cells planted in pulp turned into pulp, with working odontoblasts on dentin
Huang et al. Tissue Eng Part A 2010 Feb;16:605-15.
Tissue Engineering:Place PDL cells on Dry Tooth
Dog: tooth extracted, PDL cells stripped and into culture medium (pulp extirpated), pulp left in dry isolation
PDL cells grow and reproduce x 30 days
PDL cells painted on root and replanted
PDL reformed (control = ankylosis & resorption)
Wang, JOE Feb. 2010

60
Cryopreservation
Magnetic cryopreservationSLOW FREEZING IN A WEAK MAG. FIELD
73% preservation of cells (5 generations of normal reproduction after thawing)
Lee JOE Aug 2010
Prognosis – Follow-ups
Ins. Co. attorney wants legal release
Test adjacent teeth Pulp cap is best bet
Closed Apex Prognosis (Statistics mean nothing if you are the one)
Pulp cap = 99% Concussion = 90%
Subluxation = 75% - Calcif. Meta. 10% 20%
Extrusion = 15% - Calcif. Meta. 60% 20%
Lateral lux. = 10% - Calcif.Meta. 60% 30% Alveolar fx. = 10% 100% Intrusion = 0%??? 100% Root Fx. = varies – 60%
Pulp Prognosis (open apex =10% better)
Pulp OK Resorption / PDL
61
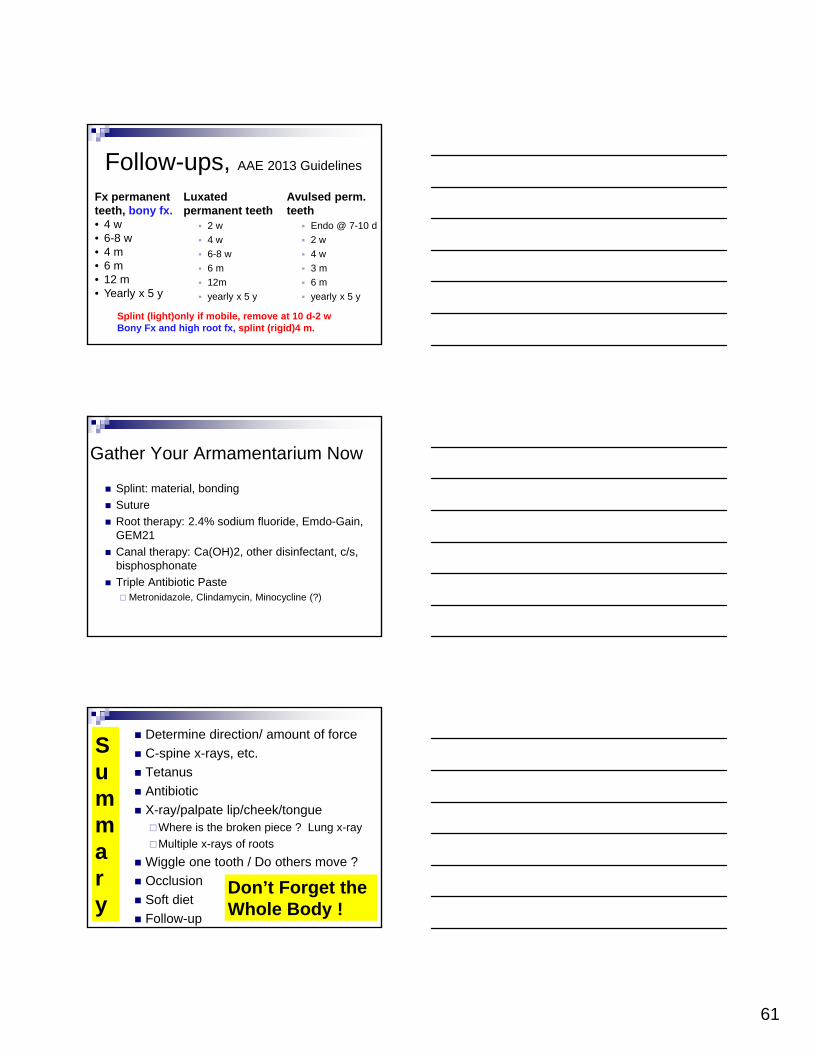
Follow-ups, AAE 2013 Guidelines
Luxated permanent teeth
2 w
4 w
6-8 w
6 m
12m
yearly x 5 y
Avulsed perm. teeth
Endo @ 7-10 d
2 w
4 w
3 m
6 m
yearly x 5 y
Fx permanent teeth, bony fx.• 4 w• 6-8 w• 4 m• 6 m• 12 m• Yearly x 5 y
Splint (light)only if mobile, remove at 10 d-2 wBony Fx and high root fx, splint (rigid)4 m.
Gather Your Armamentarium Now
Splint: material, bonding
Suture
Root therapy: 2.4% sodium fluoride, Emdo-Gain, GEM21
Canal therapy: Ca(OH)2, other disinfectant, c/s, bisphosphonate
Triple Antibiotic PasteMetronidazole, Clindamycin, Minocycline (?)
Summary
Determine direction/ amount of force
C-spine x-rays, etc.
Tetanus
Antibiotic
X-ray/palpate lip/cheek/tongueWhere is the broken piece ? Lung x-ray
Multiple x-rays of roots
Wiggle one tooth / Do others move ?
Occlusion
Soft diet
Follow-up
Don’t Forget the Whole Body !

62
SummaryWhat was the direction and concentration of force?Did a fracture dissipate some force?
Think at the microscope levelWhat are the cells doing?Can the cementum reform?
What is the healing timeline?PDL mends in 6-8w.
What is the blood supply like?
Disclaimer
These are current guidelines Not guarantees
Guidelines are NOT Absolutes














![[Huntington, Eleazer] Art of Penmanship](https://static.fdocuments.us/doc/165x107/577cd9ef1a28ab9e78a47a1d/huntington-eleazer-art-of-penmanship.jpg)