Robotic prostatectomy – The way forward or is the jury still out ?
Click here to load reader

EURURO-5448; No. of Pages 9
Surgery in Motion
Transvesical Robotic Simple Prostatectomy: Initial Clinical
Experience
Scott Leslie, Andre Luis de Castro Abreu, Sameer Chopra, Patrick Ramos, Daniel Park,Andre K. Berger, Mihir M. Desai, Inderbir S. Gill, Monish Aron *
Institute of Urology, Catherine and Joseph Aresty Department of Urology, University of Southern California, Los Angeles, CA, USA
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X
ava i lable at www.sc iencedirect .com
journa l homepage: www.europea nurology.com
Article info
Article history:
Accepted December 13, 2013Published online ahead ofprint on January 3, 2014
Keywords:
Benign prostatic hyperplasia
Simple prostatectomy
Robotic surgery
Please visit
www.europeanurology.com and
www.urosource.com to view the
accompanying video.
Abstract
Background: Despite significant developments in transurethral surgery for benignprostatic hyperplasia (BPH), simple prostatectomy remains an excellent option forpatients with large glands.Objective: To describe our technique of transvesical robotic simple prostatectomy (RSP).Design, setting, and participants: From May 2011 to April 2013, 25 patients underwentRSP.Surgical procedure: We performed RSP using our technique.Outcome measurements and statistical analysis: Baseline demographics, pathology data,perioperative complications, 90-d complications, and functional outcomes were assessed.Results and limitations: Mean patient age was 72.9 yr (range: 54–88), baseline Inter-national Prostate Symptom Score (IPSS) was 23.9 (range: 9–35), prostate volume was149.6 ml (range: 91–260), postvoid residual (PVR) was 208.1 ml (range: 72–800),maximum flow rate (Qmax) was 11.3 ml/s, and preoperative prostate-specific antigenwas 9.4 ng/ml (range: 1.9–56.3). Eight patients were catheter dependent before surgery.Mean operative time was 214 min (range: 165–345), estimated blood loss was 143 ml(range: 50–350), and the hospital stay was 4 d (range: 2–8). There were no intraopera-tive complications and no conversions to open surgery. Five patients had a concomitantrobotic procedure performed. Early functional outcomes demonstrated significantimprovement from baseline with an 85% reduction in mean IPSS ( p < 0.0001), an82.2% reduction in mean PVR ( p = 0.014), and a 77% increase in mean Qmax
( p = 0.20). This study is limited by small sample size and short follow-up period. Onepatient had a urinary tract infection; two had recurrent hematuria, one requiringtransfusion; one patient had clot retention and extravasation, requiring reoperation.Conclusions: Our technique of RSP is safe and effective. Good functional outcomessuggest it is a viable option for BPH and larger glands and can be used for patientsrequiring concomitant procedures.Patient summary: We describe the technique and report the initial results of a series ofcases of transvesical robotic simple prostatectomy. The procedure is both feasible andsafe and a good option for benign prostatic hyperplasia with larger glands.
# 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. 1441 Eastlake Ave., Suite 7416, Los Angeles, CA 90089, USA.Tel. +1 323 865 3700; Fax: +1 323 865 0120.E-mail addresses: [email protected], [email protected] (M. Aron).
1. Introduction
Management options for men with symptomatic benign
prostatic hyperplasia (BPH) have increased over the last 2
decades [1]. Development of newer energy sources has added
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
0302-2838/$ – see back matter # 2013 European Association of Urology. Phttp://dx.doi.org/10.1016/j.eururo.2013.12.020
to the armamentarium available for transurethral prostate
surgery [2], and the use of lasers has gained popularity owing
to the lower morbidity compared with traditional transure-
thral resection of the prostate (TURP) [3]. However, despite
these advances, open simple prostatectomy (OSP) remains
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol
ublished by Elsevier B.V. All rights reserved.

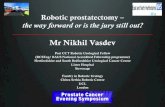
Fig. 1 – Port placement for transvesical robotic simple prostatectomy. (A) Schematic view of port placement; (B) operative view of port placement.AS = assistant; Cam = camera.
Fig. 2 – Vertical cystotomy at the dome of the bladder providingtransvesical access to the adenoma.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X2
EURURO-5448; No. of Pages 9
particularly well suited for patients with large glands
(>100 g) due to the greater volume of adenoma removed
and the subsequent excellent long-term functional outcomes
[4,5]. The first laparoscopic simple prostatectomy (LSP)
was performed in 2002 [6], and subsequent series have
demonstrated functional outcomes to be equivalent to OSP
[7,8]. However, the technical difficulty and steep learning
curve of the purely laparoscopic approach has prevented
wider acceptance of LSP among urologists. The robotic
platform potentially overcomes these constraints by provid-
ing stereoscopic three-dimensional (3D) vision and excep-
tional dexterity to facilitate the more technically demanding
steps of the simple prostatectomy procedure.
We describe our technique of transvesical robotic simple
prostatectomy (RSP) in a contemporary cohort of men with
lower urinary tract symptoms (LUTS) secondary to BPH.
Perioperative and short-term functional outcomes are
described that show RSP to be feasible, safe, and effective.
2. Methods and patients
2.1. Study cohort
Between May 2011 and April 2013, 25 patients presenting
with BPH-related LUTS underwent RSP. Initial clinical work-
up included a complete history and physical examination
(including digital rectal examination), International Prostate
Symptom Score (IPSS), office uroflowmetry, urinalysis, urine
culture, serum electrolytes and creatinine, prostate-specific
antigen (PSA), renal tract ultrasound scan with postvoid
residual (PVR), and transrectal ultrasound (TRUS) with
prostate volume calculation. All patients failed medical
therapy before opting for surgical intervention. Patients were
counseled about the surgical options available including
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
TURP, laser prostatectomy, and photovaporization. RSP was
performed following appropriate informed consent.
2.2. Positioning
All procedures were performed with the da Vinci Si Surgical
System (Intuitive Surgical, Sunnyvale, CA, USA) with
patients positioned in lithotomy and steep Trendelenburg.
Our technique involves a transperitoneal approach with a
five- to six-port placement identical to that for robotic
radical prostatectomy (Fig. 1).
2.3. Surgical technique
The dome of the bladder is identified and a midline cystotomy
is made to gain transvesical access to the prostate (Fig. 2).
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Fig. 3 – Intraoperative view of transvesical robotic simple prostatectomy.The bladder (BL) is retracted and sutured to the abdominal wall. Atransverse posterior incision is made at the junction of the trigone andadenoma (AD), and a stitch is placed through the AD allowing fordynamic retraction.
Fig. 4 – (A) Mucosal incision around the adenoma followed
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 3
EURURO-5448; No. of Pages 9
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
Four stay sutures of 2-0 Vicryl on a CT-1 needle are used to
keep the edges of the cystotomy open for access to the
adenoma (Fig. 3). A traction suture (2-0 Vicryl on a CT-1
needle) is placed through the median lobe of the adenoma to
aid with dissection (Fig. 3).Starting posteriorly, an incision
is made in the mucosa overlying the adenoma. Once the
plane between the prostatic capsule and the adenoma is
identified, enucleation is performed using monopolar
scissors and blunt dissection (Fig. 4). Upon completion, the
adenoma is placed in an Endocatch bag, and hemostasis is
obtained by direct cautery and suture ligation of specific
bleeding points in the prostatic fossa. A 22F three-way
catheter is inserted with the balloon inflated to 30 ml, and the
cystotomy is closed with 2-0 V-Loc sutures (Covidien,
Norwalk, CT, USA) (Fig. 5). Finally, a Jackson-Pratt drain is
placed in the rectovesical pouch followed by extraction of
the specimen and closure of fascia and skin.
2.4. Data collection
We prospectively collected demographic and perioperative
data including age, baseline symptoms, estimated blood
loss (EBL), operative duration, length of stay (LOS), and
by (B) enucleation. AD = adenoma; PF = prostatic fossa.
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Fig. 5 – (A) FloSeal (optional) applied to prostatic cavity to further ensurehemostasis, followed by (B) cystotomy closure. FL = FloSeal;PF = prostatic fossa.
Table 1 – Preoperative characteristics of the patient cohort
Patient demographics Results
n 25
Age, yr, mean (range) 72.9 (54–88)
Body mass index, kg/m2, mean (range) 28.2 (19.2–41)
America Society of Anesthesiologists score,
mean (range)
3 (2–4)
International Prostate Symptom Score,
mean (range)
23.9 (9–35)
Sexual Health Inventory for Men score,
mean (range)
12.8 (0–25)
PSA, ng/ml, mean (range) 9.4 (1.9–56.3)
Prostate volume, ml, mean (range) 149.6 (91–260)
Qmax, ml/s, mean (range) 11.3 (4–20)
Postvoid residual volume, ml, mean (range) 208.1 (72–800)
BPH-related complications, no. (%)
Urinary retention 13 (52)
Catheter dependent 8 (32)
Urinary tract infection 5 (20)
Macroscopic hematuria 8 (32)
Bladder calculi 2 (8)
Bladder diverticulum 1 (4)
Prior prostate surgery, no. (%)
TURP 3 (12)
TUMT 5 (20)
PVP 1 (4)
Cystoscopic findings
Prostatic urethra length, cm, mean (range) 7.2 (6–10)
Median lobes, no. (%) 15 (60)
BPH = benign prostatic hyperplasia; PSA = prostate-specific antigen;
PVP = photovaporization of the prostate; Qmax = maximum flow rate;
TUMT = transurethral microwave thermotherapy; TURP = transurethral
resection of the prostate.
Fig. 6 – Sagittal computed tomography scan demonstrating an enlargedprostate and bladder stone (arrow).
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X4
EURURO-5448; No. of Pages 9
complications. Pathologic data included specimen weight
and histologic assessment. Patients were followed with
postoperative uroflowmetry, renal tract ultrasound, and
IPSS to assess functional outcomes.
2.5. Statistical methods
Mean, range, and statistical significance were used to report
continuous and categorical data. Statistical significance
was determined based on a two-sided significance level of
0.05. Data analysis was performed using SAS v.9.2 software
(SAS Institute Inc., Cary, NC, USA).
3. Results
Table 1 presents the demographic and baseline clinical
characteristics of the cohort. Mean patient age was 72.9 yr
(range: 54–88); mean body mass index was 28.2 (range:
19.2–41). Mean IPSS was 23.9 (range: 9–35), mean PSA was
9.4 ng/ml (range: 1.9–56.3), mean maximum flow rate
(Qmax) was 11.3 ml/s (range: 4.0–20), and mean PVR was
208.1 ml (range: 72–800).
Of the 25 patients, 20 (80%) experienced a BPH-related
complication. Urinary retention occurred in 13 patients
(52%) including 8 patients who had failed their void trial and
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
were catheter dependent at the time of their operation. Five
patients (20%) experienced a urinary tract infection (UTI),
and 8 patients (32%) complained of macroscopic hematuria.
Two patients had bladder calculi (Fig. 6), and one patient
had a large bladder diverticulum (Fig. 7).
All patients had failed medical therapy (5a-reductase
inhibitors and/or a-blockers), and seven patients had
undergone previous surgical intervention for BPH including
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Fig. 7 – Fluoroscopic images during a urodynamic study. (A) A large right-sided bladder diverticulum is demonstrated (B and C) that does not empty onvoiding.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 5
EURURO-5448; No. of Pages 9
TURP, transurethral microwave thermotherapy, and photo-
vaporization of the prostate (PVP).
Preoperative flexible cystoscopy identified mean pro-
static urethra length to be 7.2 cm (range: 6–10) with 15
patients (60%) having a prominent intravesical median lobe.
All patients successfully underwent RSP with no intrao-
perative complications or conversions to open surgery
(Table 2). The mean operative duration was 214 min (range:
165–345); mean EBL was 143 ml (range: 50–350). Average
LOS was 4 d (range: 2–8), and average length of catheter
insertion was 9 d (range: 7–23). Patients underwent a
cystogram 1 wk postoperatively prior to catheter removal
(Fig. 8). Two patients were noted to have a small leak on
initial cystogram necessitating a longer catheter insertion of
18 and 23 d, respectively.
Five patients had a concomitant procedure in addition
to the simple prostatectomy. These included a bladder
diverticulectomy, heminephrectomy for a duplex system,
inguinal hernia repair, and two cases of cystolithotomy. All
procedures were completed robotically.
We report a total of five postoperative complications
(20%) in four patients. Despite perioperative injectable
third-generation cephalosporin, one patient developed a
UTI treated with oral antibiotics (Clavien-Dindo grade 2).
Table 2 – Perioperative outcomes and complications
Results
Perioperative outcomes
Operative time, min, mean (range) 214 (165–345)
Blood loss, ml, mean (range) 143 (50–350)
Concomitant procedures, no. (%) 5 (20)
Blood transfusions, no. (%) 1 (4)
Conversions, no. (%) 0 (100)
Length of hospital stay, d, mean (range) 4.0 (2–16)
Length of catheter insertion, d, mean (range) 9.0 (7–23)
Preoperative hemoglobin, g/dl, mean (range) 14.0 (10.0–18.5)
Lowest postoperative hemoglobin, g/dl,
mean (range)
11.3 (8.4–14.6)
Clavien-Dindo complications, no. (%)
Grade 1 0 (0)
Grade 2 2 (8)
Grade 3a 2 (8)
Grade 3b 1 (4)
Grade 4 or 5 0 (0)
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
Two patients were readmitted following recurrent hema-
turia leading to clot retention and the need for recatheter-
ization and bladder irrigation (Clavien-Dindo grade 3a).
Both patients restarted anticoagulation therapy that was
halted for their initial surgery. In one case the hemoglobin
dropped to 8.4 g/dl requiring transfusion with a total of
3 units of packed red cells (Clavien-Dindo grade 2). In both
cases, the hematuria resolved with bladder irrigation and
cessation of the anticoagulation. The final complication
involved a blocked catheter on postoperative day 1 due to
clot retention within the bladder associated with extra-
vasation into the peritoneal cavity. The patient underwent
robotic exploration with opening of the cystotomy and clot
evacuation under general anesthesia (Clavien-Dindo grade
3b). The patient subsequently had an uneventful post-
operative recovery and was discharged on day 4.
The mean specimen weight of the resected adenoma was
88.0 g (range: 50–172). Three cases of prostate cancer were
identified including two patients with a small focus of
Gleason 6 (pT1a) who are currently on active surveillance.
The third patient was found to have Gleason 7 (3 + 4)
involving the left lobe. Follow-up TRUS biopsy demon-
strated residual Gleason 7 cancer, and the patient was
subsequently treated with focal cryotherapy.
Early functional outcomes were assessed postopera-
tively with a mean follow-up of 6 mo (Table 3). Mean
postoperative IPSS was 3.58 (range: 0–6), which repre-
sented an 85% improvement from preoperative scores
( p < 0.01). Mean postoperative PVR was 36.9 ml (range:
0–175) indicating an 82.2% reduction ( p = 0.014). Mean Qmax
increased from 11.3 ml/s preoperatively to 20 ml/s following
surgery (77.0% improvement); however, this did not reach
statistical significance ( p = 0.20). One patient was wearing
one pad per day at 5 mo postoperatively for mild urinary
incontinence. None of the other patients had any incon-
tinence or erectile dysfunction as a result of the procedure.
4. Discussion
Our series represents one of the largest RSP cohorts in the
literature, demonstrating good perioperative outcomes
with excellent short-term symptomatic and functional
improvements. TURP and OSP are traditionally the main
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Fig. 8 – Anteroposterior and oblique views of a postoperative cystogram demonstrating no leak and a large prostatic fossa occupied by the catheterballoon.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X6
EURURO-5448; No. of Pages 9
surgical options for men with BPH, with the latter most
appropriate for larger glands (>100 g). Improved morbidity
profiles of newer technologies such as PVP and holmium
laser enucleation of the prostate (HoLEP) make these viable
options alongside TURP and OSP. Randomized trials
comparing these laser treatments with OSP for large glands
have demonstrated equivalent short-term outcomes in
terms of improvements in IPSS, Qmax, and PVR [9,10].
One of the concerns about OSP is the high rate of adverse
events, specifically perioperative bleeding. In a randomized
trial comparing HoLEP with OSP for glands >100 g, Kuntz
and Lehrich [11] demonstrated a higher rate of adverse
events in the OSP group (26.7% vs 15%), largely a result of
the 13.3% rate of perioperative blood transfusion. This high
transfusion rate with OSP is consistently reported in the
literature. A large series of 902 patients undergoing OSP
demonstrated an overall complication rate of 17.3% with
68 patients (7.5%) requiring a blood transfusion due to
excessive bleeding [12]. In a prospective study of 56
patients, the mean EBL was 1181.3 ml (range: 500–2020)
with 36% of patients receiving a blood transfusion [13].
Mariano et al. [6] first demonstrated the benefits of the
minimally invasive approach in terms of less pain and shorter
convalescence compared with OSP [7]. However, in a study
comparing the morbidity of LSP and OSP, bleeding was still
noted to be significant in both groups with a transfusion rate
Table 3 – Prostate-specific antigen and functional outcomes onfollow-up
Preoperative Postoperative Percent change p value
Mean (range) Mean (range)
PSA 9.4 (1.9–56.3) 1.48 (0.06–4.0) �84.3 0.012
IPSS 23.9 (9–35) 3.58 (0–6) �85.0 <0.0001
Qmax 11.3 (4–20) 20 (12–35) +77.0 0.20
PVR 208.1 (72–800) 36.9 (0–175) �82.2 0.014
IPSS = International Prostate Symptom Score; PSA = prostate-specific
antigen; PVR = postvoid residual; Qmax = maximum flow rate.
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
of 15.8% in the LSP group and 10.2% in the OSP group [8]. This
is likely related to the demanding ergonomics of pure
laparoscopy when operating within the narrow confines of
the pelvis and the subsequent difficulty of dissection and
intracorporeal suturing of bleeding vessels.
The adoption of the robotic platform to simple prosta-
tectomy largely overcomes these issues with our series
demonstrating a mean EBL of only 143 ml (range: 50–350)
and only one patient requiring a perioperative blood
transfusion (4%). These excellent results are consistently
seen in published reports of RSP (Table 4). Apart from the
first series by Sotelo et al., perioperative transfusion
rates following RSP have been consistently reported as
0% [14–19]. Contributing factors for this minimal blood loss
include the pneumoperitoneum resulting in tamponade of
open venous channels within the prostatic fossa during
dissection; the excellent 3D stereoscopic vision and
articulation of the robotic instruments allowing for accurate
control of specific bleeding vessels both within the fossa as
well as at the bladder neck; and the transvesical approach
used in our cohort that provides direct access to the
adenoma via the dome of the bladder, thus allowing optimal
visualization into the prostatic fossa from base to apex such
that individual bleeders can be easily seen and controlled
with electrocautery or suture ligation. These factors
combined resulted in minimal blood loss, and our 4%
transfusion rate is comparable with that seen for both PVP
and HoLEP in similar size glands [9,11].
The mean hospital LOS for our cohort was 4 d (range:
2–8). This is significantly shorter than four contemporary
OSP series where the mean LOS ranged from 6 to 11.9 d
[4,5,12,13]. The advantages of a minimally invasive
approach most likely explain this difference. Furthermore,
the reduced bleeding as discussed previously may play a
role because it potentially allows for an earlier cessation of
bladder irrigation and thus an earlier discharge from the
hospital. A low rate of early postoperative complications
(20%) was demonstrated in our series. Although the average
length of postoperative catheterization of 9 d in our cohort
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Ta
ble
4–
Ro
bo
tic
sim
ple
pro
sta
tect
om
yse
rie
s
Stu
dy
No
.o
fp
ati
en
tsA
pp
roa
chA
cce
ssto
ad
en
om
aM
ea
ng
lan
dv
olu
me
,m
l
Me
an
EB
L,m
l
Me
an
op
era
tiv
eti
me
,m
in
Tra
nsf
usi
on
rate
,%
Me
an
ho
spit
al
len
gth
of
sta
y,
d
Me
an
Fole
yca
the
ter
du
rati
on
,d
Me
an
pa
tho
log
ysp
eci
me
nw
eig
ht,
g
No
.o
fp
ati
en
tsw
ith
po
sto
pe
rati
ve
inco
nti
ne
nce
So
telo
et
al.
[14
]7
Tra
nsp
eri
ton
ea
lT
ran
sve
rse
cyst
oto
my
just
pro
xim
al
toth
e
pro
sta
tov
esi
cal
jun
ctio
n(t
ran
sve
sica
l)
77
.72
98
20
51
4.2
1.4
75
0.6
NR
Joh
ne
ta
l.[1
5])
13
Ex
tra
pe
rito
ne
al
Ve
rtic
al
cyst
oto
my
at
the
pro
sta
tov
esi
cal
jun
ctio
n(t
ran
sve
sica
l)
10
05
00
21
00
66
82
NR
Uff
ort
[16
]1
5E
xtr
ap
eri
ton
ea
lT
ran
sve
rse
inci
sio
nin
the
pro
sta
tov
esi
cal
jun
ctio
n(t
ran
sve
sica
l)
70
.91
39
12
90
2.5
4.6
46
.4N
R
Su
the
rla
nd
et
al.
[17
]9
Tra
nsp
eri
ton
ea
lT
ran
sve
rse
inci
sio
nin
the
pro
sta
teca
psu
le
(ex
tra
ve
sica
l)
13
6.5
20
61
83
01
.31
31
12
1
Co
elh
oe
ta
l.[1
8]
6T
ran
spe
rito
ne
al
Tra
nsv
ers
ein
cisi
on
just
pro
xim
al
toth
e
pro
sta
tov
esi
cal
jun
ctio
n(e
xtr
av
esi
cal)
15
72
08
90
01
4.8
14
50
Vo
rae
ta
l.[1
9]
13
Tra
nsp
eri
ton
ea
lT
ran
sve
rse
cyst
oto
my
just
pro
xim
al
toth
e
pro
sta
tov
esi
cal
jun
ctio
n(t
ran
sve
sica
l)
16
32
19
17
90
2.7
8.8
12
7N
R
Ma
tei
et
al.
[22
]3
5T
ran
spe
rito
ne
al
Ho
rizo
nta
lcy
sto
tom
yju
stp
rox
ima
lto
the
pro
sta
tov
esi
cal
jun
ctio
n(t
ran
sve
sica
l)
10
6.6
12
11
80
03
.17
7.4
87
.04
9
Th
isse
rie
s2
01
32
5T
ran
spe
rito
ne
al
Ve
rtic
al
cyst
oto
my
at
do
me
of
bla
dd
er
(tra
nsv
esi
cal)
14
9.6
14
32
14
44
.09
.08
8.0
1
EB
L=
est
ima
ted
blo
od
loss
;N
R=
no
tre
po
rte
d.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 7
EURURO-5448; No. of Pages 9
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
was longer than transurethral techniques, only one patient
developed a postoperative UTI.
Functional outcomes in our cohort were excellent and
comparable with those reported for other RSP series and for
HoLEP and PVP [9,11]. Currently, there is no long-term data
on functional outcomes following RSP; however, extra-
polation from OSP series would indicate that IPSS, Qmax,
and PVR improvements are longstanding with a low
reoperation rate between 2% and 5% [4,5]. This durability
is in part related to the amount of adenoma removed
because the robot allows complete enucleation of the
adenoma with the angles of dissection easily conforming to
the contours of the gland. The mean pathology specimen
weight in our series was 88 g, with other published RSP
series reporting a mean specimen weight between 46.4 g
and 145 g [14–19]. The amount of tissue removed by PVP is
typically less than for surgical enucleation. This explains
why a higher proportion of these treatments may fail over
time. In a prospective randomized study comparing PVP
with OSP, postoperative prostate volume had decreased less
in the PVP cohort and was associated with inferior IPSS
quality-of-life scores at 18 mo [20].
An advantage of performing RSP is the ability to treat
coexistent pathology, which occurred in five patients in our
series (20%). Concomitant procedures included cystolithot-
omy in two patients where the calculi were extracted from
the bladder following the vertical cystotomy (Fig. 9). One
patient had an inguinal hernia, and following the prosta-
tectomy a Prolene mesh was anchored in place over the
hernia defect (Fig. 10). One patient had a right-sided bladder
diverticulum. Following the vertical cystotomy in the dome
of the bladder, the neck of the diverticulum was identified
(Fig. 11), and it was dissected from the perivesical tissue
until it was completely free. The bladder defect was closed
with 3-0 Vicryl in a running fashion after excising the
diverticulum. Enucleation of the prostatic adenoma was
then performed. The last concomitant procedure was a
left robotic heminephrectomy for a duplex system. The
patient had a duplicated left collecting system with a
nonfunctioning upper pole moiety. The patient was placed
in the lateral position and the robot docked as standard for
renal surgery. Following the heminephrectomy, the robot
was undocked, the patient repositioned in lithotomy, and
the RSP continued as usual. All procedures were performed
successfully without complications, although as expected,
the operative time was longer for these five cases with a
mean duration of 243 min.
In an attempt to amplify the benefits seen with
minimally invasive surgery, Fareed et al. reported the first
series of single-port RSP in nine patients [21]. Their
technique involves a single GelPort (Applied Medical, Santa
Margarita, CA, USA) positioned at the bladder dome through
which the robot was docked to perform the enucleation.
Despite improvements in uroflowmetry parameters, peri-
operative complications were significant with two patients
requiring a blood transfusion due to excessive intraopera-
tive blood loss (>1000 ml) and two patients developing
significant postoperative hematuria requiring cystoscopic
clot evacuation and coagulation of bleeding tissue within
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

Fig. 9 – (A) Robotic cystolithotomy with concomitant simple prostatectomy; (B) respective specimen weighting 155 g.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X8
EURURO-5448; No. of Pages 9
the prostatic fossa. Although single-port RSP is feasible, the
high complications rate indicates further refinement of
ports, instrumentation, and robotics is necessary before it
can be more widely endorsed.
Never before have we been presented with such a wide
array of treatment options for men with BPH. Newer laser
techniques have been increasingly utilized, offering an
improved morbidity profile over traditional options such as
TURP and OSP. The purely laparoscopic approach to simple
prostatectomy has been explored over the last decade but
has not been embraced enthusiastically owing to its
technical difficulty and reports indicating no improvement
in adverse events when compared with conventional OSP.
The unmatched dexterity and vision afforded by the robotic
platform allows a more precise anatomic dissection of the
adenoma and facilitates accurate and swift intracorporeal
suturing to control bleeding. These factors combined offer
Fig. 10 – Concomitant robotic mesh repair of inguinal hernia.
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
excellent short-term perioperative outcomes as well as
durable functional improvements. This series adds to the
growing evidence that RSP not only confers the benefits of
minimally invasive surgery but is also associated with low
rates of postoperative complications comparable with that
of transurethral laser techniques.
Our report is still limited by a small sample size. A future
study with a larger patient cohort would be beneficial to
determine the reproducibility of this study’s results. In
addition, some patients currently have a short postopera-
tive follow-up. Long-term outcomes are beneficial for this
type of study. Finally, we did not address the costs of using
the robot for the procedure. However, in a RSP series by
Matei et al. [22], the overall costs of RSP were less than for
OSP and equivalent to TURP. Although initial operative costs
were higher for RSP, they identified lower hospitalization
costs when compared with both OSP and TURP [22].
Fig. 11 – Bladder diverticulum. Neck of diverticulum scored withelectrocautery. Note ureteral catheter in right ureteric orifice and tip ofurethral catheter advanced into neck of diverticulum. AD = adenoma;DN = diverticulum neck; FC = Foley catheter; UC = ureteral catheter.
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 9
EURURO-5448; No. of Pages 9
5. Conclusions
Our technique of transvesical RSP in men with BPH from
large glands demonstrates excellent improvements in
functional outcomes with an acceptable perioperative
morbidity profile. It is of particular benefit in those patients
with associated pathology requiring a concomitant proce-
dure. Prospective studies comparing RSP with endoscopic
laser options are required to further define their respective
roles for men with BPH.
Author contributions: Monish Aron had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Leslie, Abreu, Aron.
Acquisition of data: Chopra, Ramos.
Analysis and interpretation of data: Park.
Drafting of the manuscript: Leslie, Abreu, Chopra, Aron.
Critical revision of the manuscript for important intellectual content: Gill,
Desai, Aron.
Statistical analysis: Chopra.
Obtaining funding: None.
Administrative, technical, or material support: Park, Berger.
Supervision: Aron, Gill, Desai.
Other (specify): Video compilation: Berger, Chopra, Abreu.
Financial disclosures: Monish Aron certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
Appendix A. Supplementary data
The Surgery in Motion video accompanying this article can
be found in the online version at http://dx.doi.org/10.1016/
j.eururo.2013.12.020 and via www.europeanurology.com.
References
[1] Yu X, Elliott SP, Wilt TJ, McBean AM. Practice patterns in benign
prostatic hyperplasia surgical therapy: the dramatic increase in mini-
mally invasive technologies. J Urol 2008;180:241–5, discussion 245.
[2] Metcalfe C, Poon KS. Long-term results of surgical techniques and
procedures in men with benign prostatic hyperplasia. Curr Urol Rep
2011;12:265–73.
[3] Reich O, Gratzke C, Bachmann A, et al. Morbidity, mortality and early
outcome of transurethral resection of the prostate: a prospective
multicenter evaluation of 10,654 patients. J Urol 2008;180: 246–9.
[4] Suer E, Gokce I, Yaman O, Anafarta K, Gogus O. Open prostatectomy
is still a valid option for large prostates: a high-volume, single-
center experience. Urology 2008;72:90–4.
Please cite this article in press as: Leslie S, et al. Transvesical Robo(2014), http://dx.doi.org/10.1016/j.eururo.2013.12.020
[5] Varkarakis I, Kyriakakis Z, Delis A, Protogerou V, Deliveliotis C.
Long-term results of open transvesical prostatectomy from a con-
temporary series of patients. Urology 2004;64:306–10.
[6] Mariano MB, Graziottin TM, Tefilli MV. Laparoscopic prostatectomy
with vascular control for benign prostatic hyperplasia. J Urol 2002;
167:2528–9.
[7] Baumert H, Ballaro A, Dugardin F, Kaisary AV. Laparoscopic versus
open simple prostatectomy: a comparative study. J Urol 2006;175:
1691–4.
[8] McCullough TC, Heldwein FL, Soon SJ, et al. Laparoscopic versus
open simple prostatectomy: an evaluation of morbidity. J Endourol
2009;23:129–33.
[9] Alivizatos G, Skolarikos A, Chalikopoulos D, et al. Transurethral
photoselective vaporization versus transvesical open enucleation
for prostatic adenomas >80 ml: 12-mo results of a randomized
prospective study. Eur Urol 2008;54:427–37.
[10] Kuntz RM, Lehrich K, Ahyai SA. Holmium laser enucleation of the
prostate versus open prostatectomy for prostates greater than 100
grams: 5-year follow-up results of a randomised clinical trial. Eur
Urol 2008;53:160–8.
[11] Kuntz RM, Lehrich K. Transurethral holmium laser enucleation
versus transvesical open enucleation for prostate adenoma greater
than 100 gm.: a randomized prospective trial of 120 patients. J Urol
2002;168:1465–9.
[12] Gratzke C, Schlenker B, Seitz M, et al. Complications and early
postoperative outcome after open prostatectomy in patients with
benign prostatic enlargement: results of a prospective multicenter
study. J Urol 2007;177:1419–22.
[13] Helfand B, Mouli S, Dedhia R, McVary KT. Management of lower
urinary tract symptoms secondary to benign prostatic hyperplasia
with open prostatectomy: results of a contemporary series. J Urol
2006;176:2557–61, discussion 2561.
[14] Sotelo R, Clavijo R, Carmona O, et al. Robotic simple prostatectomy.
J Urol 2008;179:513–5.
[15] John H, Bucher C, Engel N, Fischer B, Fehr JL. Preperitoneal robotic
prostate adenomectomy. Urology 2009;73:811–5.
[16] Uffort EE. Robotic-assisted laparoscopic simple prostatectomy:
an alternative minimal invasive approach for prostate adenoma.
J Robot Surg 2010;4:7–10.
[17] Sutherland DE, Perez DS, Weeks DC. Robot-assisted simple pros-
tatectomy for severe benign prostatic hyperplasia. J Endourol 2011;
25:641–4.
[18] Coelho RF, Chauhan S, Sivaraman A, et al. Modified technique of
robotic-assisted simple prostatectomy: advantages of a vesico-
urethral anastomosis. BJU Int 2012;109:426–33.
[19] Vora A, Mittal S, Hwang J, Bandi G. Robot-assisted simple prosta-
tectomy: multi-institutional outcomes for glands larger than
100 grams. J Endourol 2012;26:499–502.
[20] Skolarikos A, Papachristou C, Athanasiadis G, Chalikopoulos D,
Deliveliotis C, Alivizatos G. Eighteen-month results of a randomized
prospective study comparing transurethral photoselective vapor-
ization with transvesical open enucleation for prostatic adenomas
greater than 80 cc. J Endourol 2008;22:2333–40.
[21] Fareed K, Zaytoun OM, Autorino R, et al. Robotic single port supra-
pubic transvesical enucleation of the prostate (R-STEP): initial
experience. BJU Int 2012;110:732–7.
[22] Matei DV, Brescia A, Mazzoleni F, et al. Robot-assisted simple pros-
tatectomy (RASP): does it make sense? BJU Int 2012;110: E972–9.
tic Simple Prostatectomy: Initial Clinical Experience. Eur Urol


















