
Transposition of a maxillary canine and a lateral incisor ... · tooth positions were corrected...
11
Transposition of a maxillary canine and a lateral incisor and use of cone-beam computed tomography for treatment planning Jason Pair Valencia, Calif This report describes the orthodontic treatment of a 12-year-old girl with transposition of the maxillary left canine and the lateral incisor. Cone-beam computed tomography was used during treatment planning. The transposed tooth positions were corrected with an unconventional orthodontic approach. Treatment alternatives and their clinical concerns are presented. (Am J Orthod Dentofacial Orthop 2011;139:834-44) T ransposition is defined as an unusual type of ec- topic eruption where a permanent tooth develops in the position normally occupied by another per- manent tooth. 1 It is a rare occurrence that affects less than 1% of the population. 2-5 Transposition affects the maxillary dentition (68.5%-76%) more frequently than the mandibular dentition. 6-8 The most common type of transposition (55%-70%) is that of the maxillary canine and the first premolar (Mx.C.P1). 4,6,9 Twenty-seven per- cent of Mx.C.P1 patients demonstrate bilateral occur- rence. 8 Maxillary canine-lateral incisor transposition (Mx.C.I2) is the second most common type at 20% to 42%, with only 5% having bilateral occurrence. 8,9 Peck et al 10 described Mx.C.P1 as an anomaly “result- ing from genetic influences within a multifactorial inher- itance model.” This was based on an elevated frequency of associated dental anomalies, elevated bilateral occur- rence (27%), familial occurrence (11%), and differences between male and female prevalence (females 1.55:1 males). 10,11 Others have demonstrated elevated frequencies of associated dental anomalies with Mx.C.P1 patients. 6,9,11-13 These associated dental anomalies included hypodontia, submerged deciduous teeth, retained deciduous teeth, and supernumerary teeth. Unlike Mx.C.P1, it has been hypothesized that the etiology of Mx.C.I2 is more environmental than genetic. Dentofacial trauma in the deciduous dentition, with subsequent drifting of the developing permanent teeth is the most common etiologic factor. 2,8 There are few reports of familial occurrence or dental anomalies associated with Mx.C.I2 transpositions. 14 The only den- tal anomaly that has an apparent association with Mx.C.I2 is increased third molar agenesis. 15 Treatment of Mx.C.I2 depends on many factors. If the central incisor has significant root resorption (ei- ther from past dentofacial trauma or due to the ectop- ically erupting canine), the central incisor can be extracted and the canine moved into its position, as has been reported. 16 Significant restorative work is necessary for acceptable smile esthetics with this treat- ment plan. If extractions are indicated because of severe crowd- ing or a desire for a change in the soft-tissue profile, then the following extraction pattern should be considered: the transposed canine and the 3 first premolars in the re- maining quadrants. If this option is chosen, it could be necessary to intrude the first premolar next to the lateral incisor so that the height of the gingival margin matches that of the contralateral canine. The premolar crown could then be veneered and brought into occlusal func- tion. It also might be necessary to extract the transposed lateral incisor (rather than the canine) if it has already demonstrated root resorption. Extraction of transposed peg-shaped lateral incisors and substitution of canines has also been described. 14 Another possibility—leaving the canine and the lateral incisor transposed—is rarely a good esthetic or functional option. The difficulty of resolving the transposition is the risk of root interference as the canine passes distally around the lateral incisor. This interference could lead to significant root resorption and subsequent pathologic Private practice, Valencia and Northridge, Calif; volunteer faculty, Orthodontic Residency Program, University of California at Los Angeles. The author reports no commercial, proprietary, or finanical interest in the prod- ucts or companies described in this article. Reprint requests to: Jason Pair, 23838 Valencia Blvd, Suite 42, Valencia, CA 91355; e-mail, [email protected]. Submitted, July 2009; revised and accepted, August 2009. 0889-5406/$36.00 Copyright Ó 2011 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2009.08.035 834 CASE REPORT
Transcript of Transposition of a maxillary canine and a lateral incisor ... · tooth positions were corrected...

CASE REPORT
Transposition of a maxillary canine and a lateralincisor and use of cone-beam computedtomography for treatment planning
Jason PairValencia, Calif
PrivatResidThe aucts oReprin91355Subm0889-Copyrdoi:10
834
This report describes the orthodontic treatment of a 12-year-old girl with transposition of the maxillary left canineand the lateral incisor. Cone-beam computed tomography was used during treatment planning. The transposedtooth positions were corrected with an unconventional orthodontic approach. Treatment alternatives and theirclinical concerns are presented. (Am J Orthod Dentofacial Orthop 2011;139:834-44)
Transposition is defined as an unusual type of ec-topic eruption where a permanent tooth developsin the position normally occupied by another per-
manent tooth.1 It is a rare occurrence that affects lessthan 1% of the population.2-5 Transposition affects themaxillary dentition (68.5%-76%) more frequently thanthe mandibular dentition.6-8 The most common type oftransposition (55%-70%) is that of the maxillary canineand the first premolar (Mx.C.P1).4,6,9 Twenty-seven per-cent of Mx.C.P1 patients demonstrate bilateral occur-rence.8 Maxillary canine-lateral incisor transposition(Mx.C.I2) is the second most common type at 20% to42%, with only 5% having bilateral occurrence.8,9
Peck et al10 describedMx.C.P1 as an anomaly “result-ing from genetic influences within a multifactorial inher-itance model.” This was based on an elevated frequencyof associated dental anomalies, elevated bilateral occur-rence (27%), familial occurrence (11%), and differencesbetween male and female prevalence (females 1.55:1males).10,11 Others have demonstrated elevatedfrequencies of associated dental anomalies withMx.C.P1 patients.6,9,11-13 These associated dentalanomalies included hypodontia, submerged deciduousteeth, retained deciduous teeth, and supernumerary teeth.
Unlike Mx.C.P1, it has been hypothesized that theetiology of Mx.C.I2 is more environmental than genetic.
e practice, Valencia and Northridge, Calif; volunteer faculty, Orthodonticency Program, University of California at Los Angeles.uthor reports no commercial, proprietary, or finanical interest in the prod-r companies described in this article.t requests to: Jason Pair, 23838 Valencia Blvd, Suite 42, Valencia, CA; e-mail, [email protected], July 2009; revised and accepted, August 2009.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2009.08.035
Dentofacial trauma in the deciduous dentition, withsubsequent drifting of the developing permanent teethis the most common etiologic factor.2,8 There are fewreports of familial occurrence or dental anomaliesassociated with Mx.C.I2 transpositions.14 The only den-tal anomaly that has an apparent association withMx.C.I2 is increased third molar agenesis.15
Treatment of Mx.C.I2 depends on many factors. Ifthe central incisor has significant root resorption (ei-ther from past dentofacial trauma or due to the ectop-ically erupting canine), the central incisor can beextracted and the canine moved into its position, ashas been reported.16 Significant restorative work isnecessary for acceptable smile esthetics with this treat-ment plan.
If extractions are indicated because of severe crowd-ing or a desire for a change in the soft-tissue profile, thenthe following extraction pattern should be considered:the transposed canine and the 3 first premolars in the re-maining quadrants. If this option is chosen, it could benecessary to intrude the first premolar next to the lateralincisor so that the height of the gingival margin matchesthat of the contralateral canine. The premolar crowncould then be veneered and brought into occlusal func-tion. It also might be necessary to extract the transposedlateral incisor (rather than the canine) if it has alreadydemonstrated root resorption. Extraction of transposedpeg-shaped lateral incisors and substitution of canineshas also been described.14
Another possibility—leaving the canine and the lateralincisor transposed—is rarely a good esthetic or functionaloption. The difficulty of resolving the transposition is therisk of root interference as the canine passes distallyaround the lateral incisor. This interference could leadto significant root resorption and subsequent pathologic

Pair 835
tooth mobility of the affected teeth. However, resolvingthe transposition is ideal for esthetics and function.
DIAGNOSIS AND ETIOLOGY
A girl, aged 12 years 5 months, came to my practicewith the chief complaint of malaligned teeth (Figs 1and 2). She was physically healthy with no history ofdental trauma. She had a slightly convex profile withmild chin asymmetry to the right. She had a pleasingsmile and lip competence. The intraoral examinationshowed half-cusp Class II molar relationships withcrowding of 3.5 mm in the mandibular arch and 9 mmin the maxillary arch. The maxillary left canine wasblocked out of the arch, and the maxillary left lateral in-cisor was proclined labially. The maxillary left caninecould not be palpated labially or palatally. Her maxillarydental midline was displaced 2 mm to the left of the fa-cial midline and mandibular dental midline. Overbitewas 25% with an exaggerated curve of Spee of 3 mm.
The panoramic radiograph showed normal root andtooth development, with the exception of transpositionof the maxillary left canine and the lateral incisor (Fig 3).Cephalometric assessment showed a Class I, mesofacialskeletal pattern (Wits, 1.5 mm; ANB, 2.5�; SN-GoGn,33�) with normally inclined incisors (Fig 4, Table).
TREATMENT OBJECTIVES
Ideally, the treatment objectives would include fullresolution of the transposition. However, achievementof this objective might subject the transposed teeth tomechanics that have significant root resorption risks.Class I molar and canine relationships, ideal overjetand overbite, and an esthetic smile with minimal changein the profile were desired.
TREATMENT ALTERNATIVES
The following treatment alternatives were consideredand discussed with the patient and her parents.
1. Extraction of 3 first premolars (14, 34, 44) and thetransposed canine (23) with intrusion of the maxil-lary left first premolar (24) to match the gingivalheight of the contralateral canine. After orthodontictreatment, a veneer would be placed on tooth 24 tomatch the morphology of the contralateral canineand bring it into occlusion for canine disclusion. Ex-tractions without careful anchorage control couldnegatively affect her profile.
2. Nonextraction treatment without resolution of thetransposition followed by postorthodontic veneersin an attempt to normalize crown morphology andcreate ideal function. The disadvantage is the un-
American Journal of Orthodontics and Dentofacial Orthoped
likelihood of ideal smile esthetics. The advantageis the minimal risk of root interferences duringalignment. There is also less chance of bony lossof the buccal cortical plate of the canine, since itdoes not have to pass labially to the lateral incisor.
3. Extraction of the maxillary left lateral incisor (22),normalization of the canine, and a future implantin the lateral position. This would be considered if,when analyzing the initial records, significant rootresorption was found on the lateral incisor. The ad-vantage is a relatively short treatment time. How-ever, the future cost of an implant-supportedcrown must be considered.
4. Nonextraction treatment with full resolution of thetransposition. This plan has been described previouslyin the literature.1,2,17 One disadvantage of resolvinga transposition is the likelihood of a protractedtreatment time, as has been demonstratedpreviously.1,2,17,18 Another disadvantage is thelikelihood of root resorption to the lateral incisor ifroot interferences are not eliminated duringmechanics. Also, there is the potential for loss of thebuccal cortical plate on the canine as it passesdistally and labially to the lateral incisor. It wasexplained to the patient’s family that, if the lateralincisor suffered significant root resorption, it wouldbe extracted, the canine would be normalized, anda future implant-supported crown would be placedin the lateral incisor’s position (alternative 3).
All treatment options would achieve an ideal Class Imolar relationship and ideal overjet. However, the pa-tient and her parents wished to avoid postorthodonticrestorative work if possible and were willing to accepta protracted treatment plan (alternative 4). The risks ofroot resorption to the lateral incisor and loss of the buc-cal bony plate on the canine were understood andaccepted by the patient.
TREATMENT PROGRESS
The exact relative positions of the transposed teethwere impossible to ascertain on the pretreatment pano-ramic radiograph. We instead planned on initially level-ing the maxillary arch (with no bracket on 22, except fora metal pad to satisfy the patient, who was self-conscious about having a front tooth without a bracketattached). After leveling, we planned to open space forthe transposed teeth, followed by more radiographsand, possibly, a cone-beam computed tomography(CBCT) scan to better assess the position of the caninerelative to the root of the lateral incisor.
Fixed appliances (self-ligating Damon2, 0.022-inslot; Ormco Corporation, Orange, Calif) were placed in
ics June 2011 � Vol 139 � Issue 6

Fig 1. Pretreatment photographs.
836 Pair
the maxillary arch in May 2005. A nickel-titanium (NiTi)open coil was used to gain more space for the trans-posed teeth. Radiographs taken after the arch was lev-eled did not clearly show the relative tooth positions(Fig 5); an occlusal image suggested that the caninecrown was palatal to the root of the lateral incisor,but the periapical images suggested that the crown ofthe canine was buccal to the lateral incisor root.19 ACBCT scan was obtained in December 2005 (Fig 6). Thescan and the composite video showed a complete trans-position, with the crown of the canine buccal to the rootof the lateral incisor, yet palatal to the crown of the lateralincisor (still images, Fig 6). Bracket placement and arch-wire engagement at this time on the lateral incisor wouldbring the root labially and into the crown of the canine,most likely leading to root resorption. Surgically expos-ing the canine and pulling it distally would drag thecrown of the canine across the cervical junction of thelateral incisor, also a risky proposition. It appeared in-stead that, if the lateral incisor could be simply tippedpalatally, it would create enough space to bring the ca-nine into the arch without engaging the lateral incisor
June 2011 � Vol 139 � Issue 6 American
on its way down. A palatal bar was fabricated with sol-dered hooks; the bar and buttons were placed on thecrown of the lateral incisor. The lateral incisor was acti-vated with a power chain (Fig 7). After 6 weeks, a secondCBCT scan was taken. It showed complete separation ofthe lateral incisor root and the canine crown (still images,Fig 8). A path had been cleared for surgical exposure andtraction of the canine. No root resorption was noted onthe lateral incisor.
The canine was brought into the arch with a light0.014-in NiTi wire (in the bracket slots), while the archform was stabilized with a stainless steel overlay arch(0.016 3 0.025 in) (Fig 9). The overlay arch was ligatedover the closed doors of the self-ligating brackets. Thismechanical setup allows for minimal friction acting onthe leveling arch as it pulls the canine down, while theintegrity of the arch is maintained with the stainless steelarchwire. The manner in which the overlay wire is ligatedto the brackets (over the wings) does not allow the liga-tion wires to interfere with the slots of the bracket, so the0.014-in NiTi wire can slide through with minimal fric-tion. After the canine was brought into the arch, the
Journal of Orthodontics and Dentofacial Orthopedics

Fig 2. Pretreatment dental casts.
Fig 3. Pretreatment radiographs showed normal root andtooth development with the exception of the transpositionof the maxillary left canine and the lateral incisor.
Fig 4. Pretreatment cephalometric tracing showeda Class I mesofacial skeletal pattern (Wits, 1.5�; ANB,2.5�; SN-GoGn, 33�) with normally inclined incisors.
Pair 837
American Journal of Orthodontics and Dentofacial Orthopedics June 2011 � Vol 139 � Issue 6

Table. Cephalometric analysis
Pretreatment PosttreatmentSNA 75� 76�
SNB 72.5� 75�
ANB 2.5� 1�
Wits �1.5 mm �3 mmSN Go-Gn 31.5� 37�
FMA 29.5� 28�
Max 1-NA 4 mm 8 mmMax 1-SN 93.5� 105�
Mand 1-NB 5 mm 7 mmMand 1-Go-Gn 91� 96�
E-line 0 mm �1 mm
Fig 5. Radiographs after leveling the occlusal arch.
838 Pair
lateral incisor was released from traction, and the caninewas distalized into its normal position. The lateral incisorwas teased back into the arch form with elastic thread. Alocalized gingivectomy was performed on the lateral in-cisor to remove the excessive labial gingiva beforea bracket was placed, and the tooth was engaged withthe archwire. The bracket used on the lateral incisorwas placed upside down (�8�) to affect labial root tor-que. Class II elastics, anterior box elastics (both 0.25-in,4 oz), and interproximal reduction of the mandibularincisors were used to idealize the occlusion. The final 8months of treatment were used to effect as much labialroot torque on tooth 22 as possible to match the inclina-tion of the contralateral lateral incisor.
After 43 months of treatment, the appliances wereremoved, the final records were taken, and a fixed lin-gual retainer was placed canine-to-canine in the man-dibular arch (Figs 10-13). An Essix-type retainer fordaytime use and a Hawley retainer for nighttime usewere given for retention of the maxillary arch.
TREATMENT RESULTS
The transposition was fully resolved, and ideal Class Imolar and canine relationships were achieved. Idealoverjet and overbite were achieved with adequate caninedisclusion and protrusive guidance.
Cephalometric analysis showed that a Class III growthpattern had occurred during the treatment, with signif-icant mandibular growth (both vertically andhorizontally) and no maxillary change (Figs 13 and 14,Table). Cast and cephalometric analysis showed thatthe crowding was resolved in 2 ways: through lateralarch expansion and proclination of the incisors. Themandibular molars expanded by 4 mm, the mandibularfirst premolars expanded by 4 mm, the maxillary firstmolars expanded by 6 mm, and the maxillary firstpremolars expanded by 8 mm. However, themandibular canines showed no expansion, consideredimportant for long-term stability. The mandibular
June 2011 � Vol 139 � Issue 6 American
incisors proclined 5� to 96�, but stayed within a standarddeviation from a normal value of 92�. The maxillary in-cisors, however, changed inclination by 112.5�. Thecomposite tracing demonstrates that the changes inmaxillary inclination were both labial crown tippingand palatal root torque. It makes sense that the maxillaryincisors had to be proclined labially tomaintain a positiveoverjet as the mandible grew at a faster pace than themaxilla.
The composite tracings show no negative change inher soft-tissue profile with some straightening of theprofile as her mandible grew forward. This was a goalof both the parents and the clinician.
The gingival margins of the maxillary anterior teethwere not ideal but could be idealized with a minimallyinvasive gingivectomy procedure. There also appearedto be mild canting of the occlusal plane in the final re-sult, not uncommon in patients with unilateral canineimpactions. Despite the effort and subsequent successto upright the maxillary left lateral incisor with labialroot torque, the maxillary first premolars were finishedwith too much buccal crown tip.
The final panoramic radiograph demonstrates idealroot alignment except for the maxillary left lateral inci-sor, which was angulated distally (Fig 12). Because ofa discrepancy between the long axes of the root andthe crown, the clinical crown appears well aligned inher smile. About 2.5 mm of root resorption was notedon the tip of the maxillary left lateral incisor (18%). Noroot resorption was noted on the CBCT scan after thecrown of this tooth was tipped back into the palate.The root resorption most likely occurred as heavy labial
Journal of Orthodontics and Dentofacial Orthopedics

Fig 7. A palatal bar with soldered hooks and buttons was placed on the crown of the lateral incisor andactivated with a power chain.
Fig 6. The CBCT scan showed a complete transposition, with the crown of the canine positionedbuccally to the root of the lateral incisor but palatally to the crown of the lateral incisor.
Pair 839
root torque was being expressed during the last 8months of treatment.
After 9 months, the patient returned, and the reten-tion photos were taken, demonstrating good stability ofthe final result (Fig 15).
DISCUSSION
This patient presented with a challenging case of uni-lateral transposition of the left lateral incisor and canine.The transposition was complete, with both the crownand the root of the canine mesial to the crown and theroot of the lateral incisor. The case was further compli-cated because the canine was unerupted, and conven-tional radiographs offered conflicting evidence of itsrelative position to the lateral incisor. Other reportedcases of Mx.C.I2 transposition had initial presentationswith the canine fully erupted labially in the archform.1,2 Orthodontic mechanics are certainly easier toconceive when all affected teeth can be absolutelylocalized.
Complete transpositions require complex and oftenprotracted treatment plans with no guarantee of success.Parker20 suggested that heroic efforts to resolve transpo-sitions can be disappointing. Therefore, careful consid-eration must be given to the specific circumstancesof the patient, including predicted compliance and
American Journal of Orthodontics and Dentofacial Orthoped
tolerance of protracted treatment, before embarkingon a heroic treatment plan.
The ultimate success of the treatment plan hinged onaccurate assessment of the relative positions of thetransposed teeth. Conventional radiography in thiscase gave conflicting viewpoints. Ericson and Kurol21 re-ported that, in a sample of Swedish children, assessmentusing conventional periapical radiography was only 80%successful in the localization of ectopic canines. Theother 20% required tomography for accurate localiza-tion. The conventional periapical assessments were leastsuccessful in patients whose canine overlapped thelateral incisor (similar to this case report).
There have been reports of successful use of comput-erized tomography (CT) in the localization of impactedcanines.22 Although useful for elucidating the exact lo-cation of the impacted tooth, the cost to the patient isoften prohibitive. The amount of radiation exposure isalso an argument against the routine use of medicalCT scans for localization of impacted teeth. However,the value of CT scans was evident in these reports. Eric-son and Kurol21 reported that CT can detect 50% morecases of resorption than periapical and panoramic radi-ography. They also stated that, when clinicians weregiven the additional information from a CT scan, theychanged their treatment plan 43% of the time.
ics June 2011 � Vol 139 � Issue 6

Fig 8. A second CBCT scan showed complete separation of the lateral incisor root and the caninecrown. A path had been cleared for surgical exposure and traction of the canine. No root resorptionwas noted on the lateral incisor.
Fig 9. A, The canine was brought into the arch with light 0.014-in NiTi wire; B, the arch form was sta-bilized with a stainless steel overlay arch (0.0163 0.025 in); C, the lateral incisor was teased back intothe arch form with elastic thread; D, a localized gingivectomy was performed on the lateral incisor toremove the excessive labial gingiva, and a bracket was then placed and the tooth engaged with thearchwire.
840 Pair
Today, we have the ability to gather undistorted, ac-curate 3-dimensional views of the jaws with CBCT ata cost that is not prohibitive and at a radiation dosethat is considerably less than that of conventional med-ical CT. The problem with panoramic images is that theyare magnified and distorted. Distortion is the unequalmagnification of different parts of the same image. Pan-oramic distortion makes it unreliable for making mea-surements.23 Panoramic and periapical radiographyprovide only 2-dimensional images, whereas CBCT canprovide buccolingual, axial, coronal, sagittal, and pano-ramic views. And, with the use of software, these images
June 2011 � Vol 139 � Issue 6 American
can be easily converted into accurate 3-dimensionalimages and videos.
Panoramic and periapical films in this case reportcould not provide an accurate assessment of the relativepositions of the transposed teeth. They also could notprovide an accurate assessment of whether the lateralincisor suffered any root resorption as the canine erup-ted ectopically. Ericson and Kurol24 reported that CTscanning substantially increased the detection of rootresorption on incisors adjacent to ectopically eruptingmaxillary canines. The sensitivity of intraoral (periapi-cal) films was low when diagnosing the resorptions.
Journal of Orthodontics and Dentofacial Orthopedics

Fig 10. Posttreatement photographs.
Pair 841
Any signs of pretreatment root resorption (especiallymidroot and into the pulp canal) would have swayedmy treatment plan to extraction of the affected lateralincisor and an eventual implant-supported crownrestoration.
The necessity of moving the lateral incisor palatallyhas been discussed before.2,13 Doing so in this patientavoided potential root interferences and preventedpotential loss of the cortical plate by allowing thecanine to erupt into the arch rather than too farlabially. The second CBCT scan confirmed the rootseparation, so that the treatment plan could proceedwith confidence.
Once space was gained for the lateral incisor, it wasnecessary to bring it into the arch form. Effecting signif-icant labial root torque through archwire manipulationand bracket placement (upside down to effect�8� of tor-que) was the thrust of the final 8 months of treatment.
The final result demonstrated mild root resorption(2.5 mm, 18%) on the maxillary left lateral incisor thatshould have no long-term consequences with regardto loss of tooth vitality or tooth mobility. Kokich25
American Journal of Orthodontics and Dentofacial Orthoped
defined moderate to severe root resorption as greaterthan a 20% reduction in the original root length.
Several authors have looked at the long-term conse-quences of orthodontically induced apical root resorp-tion. Some evidence suggests that orthodonticallyinduced root resorption does not progress once the ap-pliances are removed.26,27 Falahat et al28 demonstrateda favorable long-term prognosis in a long-term fol-low-up (2-10 years) of resorbed maxillary incisors. Of32 teeth in the study, 13 had repair of the resorption la-cunae, 12 remained unchanged, and 7 had increasedroot resorption. However, of the 7 incisors with increasedresorption, none lost vitality or exhibited ankylosis.Jonsson et al29 demonstrated that postorthodonticroot resorption remained stable up to 25 years aftertreatment, if the roots were at least 10 mm in lengthand had a healthy periodontium.
Despite the difficulty of planning the treatment forthis patient, the protracted treatment time, and theadditional costs of imaging, the final result was grat-ifying for the clinician, the patient, and the patient’sfamily.
ics June 2011 � Vol 139 � Issue 6
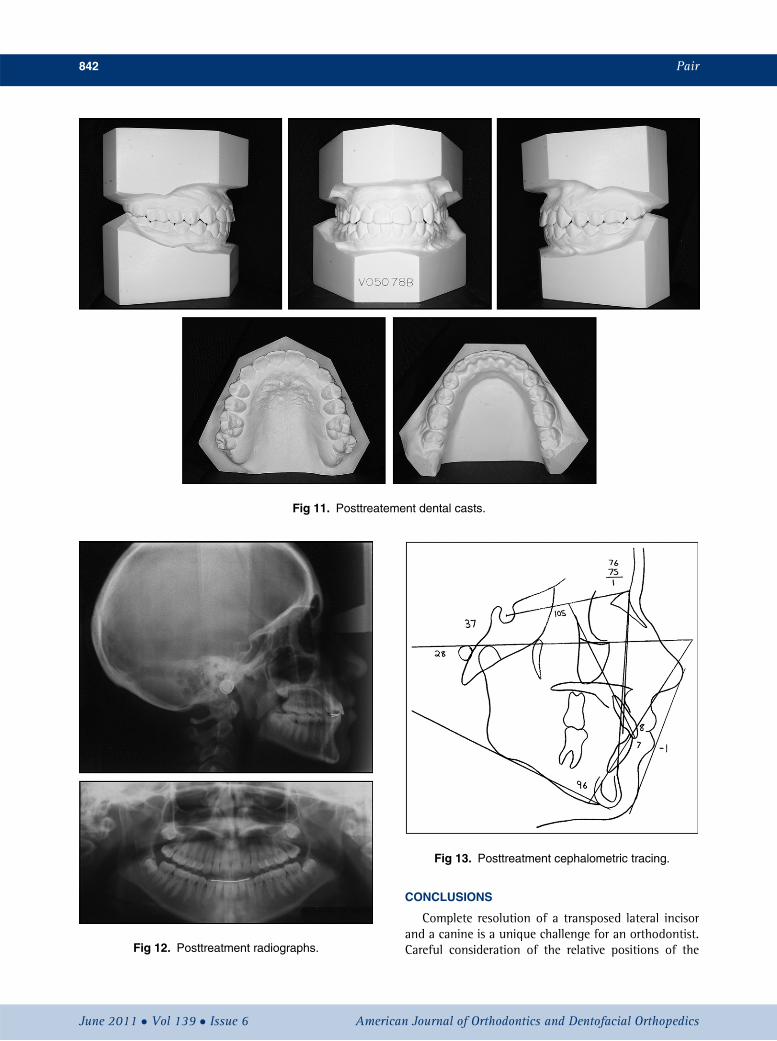
Fig 11. Posttreatement dental casts.
Fig 12. Posttreatment radiographs.
Fig 13. Posttreatment cephalometric tracing.
842 Pair
June 2011 � Vol 139 � Issue 6 American
CONCLUSIONS
Complete resolution of a transposed lateral incisorand a canine is a unique challenge for an orthodontist.Careful consideration of the relative positions of the
Journal of Orthodontics and Dentofacial Orthopedics

Fig 14. Cephalometric analysis showed that a Class III growth pattern had occurred during the treat-ment, with significant mandibular growth (both vertically and horizontally) and no maxillary change.
Fig 15. Nine months postretention.
Pair 843
American Journal of Orthodontics and Dentofacial Orthopedics June 2011 � Vol 139 � Issue 6

844 Pair
transposed teeth is imperative for developing a plan thatwill minimize the likelihood of negative treatmentconsequences (root resorption with subsequent toothmobility and periodontal issues). This case report dem-onstrates the difficulty of using conventional radiogra-phy to adequately assess the relative positions oftransposed teeth. CBCT imaging was necessary to confi-dently execute a successful treatment plan that resultedin an esthetic and functional outcome.
REFERENCES
1. Shapira Y, Kuftinec M. Maxillary canine-lateral incisor transposi-tion—orthodontic management. Am J Orthod Dentofacial Orthop1989;95:439-44.
2. Maia F. Orthodontic correction of a transposed maxillary canineand lateral incisor. Angle Orthod 2000;70:339-48.
3. Yilmaz H, Turkkahraman H, Sain M. Prevalence of tooth transpo-sitions and associated dental anomalies in a Turkish population.Dentomaxillofac Radiol 2005;34:32-5.
4. Burnett SE. Prevalence of maxillary canine-first premolar transposi-tion in a composite African sample. Angle Orthod 1999;69:187-9.
5. Ruprecht A, Batniji S, El-Neweihi E. The incidence of transpositionof teeth in dental patients. J Pedod 1985;9:244-9.
6. Ely N, Sherrif M, Cobourne M. Dental transposition as a disorder ofgenetic origin. Eur J Orthod 2006;28:145-51.
7. Plunkett DJ, Dysart PS, Kardos TB, Herbison GP. A study of trans-posed canines in a sample of orthodontic patients. Br J Orthod1998;25:203-8.
8. Peck S, Peck L. Classification of maxillary tooth transpositions. AmJ Orthod Dentofacial Orthop 1995;107:505-17.
9. Shapira Y, Kuftinec M. Maxillary tooth transpositions: characteris-tic features and accompanying dental anomalies. Am J OrthodDentofacial Orthop 2001;119:127-34.
10. Peck L, Peck S, Attia Y. Maxillary canine-first premolar transposi-tion, associated dental anomalies and genetic basis. Angle Orthod1993;63:99-109.
11. Camilleri S. Maxillary canine anomalies and tooth agenesis. Eur JOrthod 2005;27:450-6.
12. Newman GV. Transposition: orthodontic treatment. J Am DentAssoc 1977;94:544-7.
June 2011 � Vol 139 � Issue 6 American
13. Shapira Y, Kuftinec M. Tooth transpositions—a review of the liter-ature and treatment considerations. Angle Orthod 1989;59:271-6.
14. Bracco P, Titolo C, Zaretta L, Moretti A, Debernardi C. Orthodontictreatment in a bilateral lateral incisor-canine transposition. Mi-nerva Ortognatod 2004;22:61-5.
15. Peck S, Peck L, Kataja M. Concomitant occurrence of canine mal-position and tooth agenesis: evidence of orofacial genetic fields.Am J Orthod Dentofacial Orthop 2002;122:657-60.
16. Goyenc Y, Karaman A, Gokalp A. Unusual ectopic eruption ofmaxillary canines. J Clin Orthod 1995;29:580-2.
17. Shapira Y, Kuftinec M. A unique treatment approach for maxillarycanine-lateral incisor transposition. Am J Orthod DentofacialOrthop 2001;199:540-5.
18. Halazonetis D. Horizontally impacted maxillary premolar and bi-lateral canine transposition. Am J Orthod Dentofacial Orthop2009;135:380-9.
19. Goaz P, White S. Oral radiology. 2nd ed. St Louis: C. V. Mosby;1987. p. 120.
20. Parker W. Transposed premolars, canines, and lateral incisors. Am JOrthod Dentofacial Orthop 1990;97:431-8.
21. Ericson S, Kurol J. Radiographic examination of ectopically erupt-ing maxillary canines. Am J Orthod Dentofacial Orthop 1987;91:483-92.
22. Schmuth GP, Freisfeld OK, Schuller H. The application of comput-erized tomography (CT) in cases of impactedmaxillary canines. EurJ Orthod 1992;14:296-301.
23. Serman NJ. Pitfalls of panoramic radiology in implant surgery. AnnDent 1989;48:13-6.
24. Ericson S, Kurol PJ. Resorption of incisors after ectopic eruption ofmaxillary canines: a CT study. Angle Orthod 2000;70:415-23.
25. Kokich V. Orthodontic and nonorthodontic root resorption: theirimpact on clinical dental practice. J Dent Educ 2008;72:895-902.
26. Remington DN, Joondeph DR, �Artun J, Riedel RA, Chapko MK.Long-term evaluation of root resorption occurring during ortho-dontic movement. Am J Orthod Dentofacial Orthop 1989;96:43-6.
27. Copeland S, Green LJ. Root resorption in maxillary central incisorsfollowing active orthodontic treatment. Am J Orthod 1986;89:51-5.
28. Falahat B, Ericson S, D’Amico RM, Bjerklin K. Incisor root resorp-tion due to ectopic maxillary canines. Angle Orthod 2007;78:778-85.
29. Jonsson A, Malmgren O, Levander E. Long-term follow-up oftooth mobility in maxillary incisors with orthodontically inducedapical root resorption. Eur J Orthod 2007;29:482-7.
Journal of Orthodontics and Dentofacial Orthopedics


















