TRANSPARENCY IN THE PHARMA SUPPLY CHAIN: KNOWLEDGE … · Roundtable Summary Recommendations...
65
TRANSPARENCY IN THE PHARMA SUPPLY CHAIN: KNOWLEDGE IS POWER!
Transcript of TRANSPARENCY IN THE PHARMA SUPPLY CHAIN: KNOWLEDGE … · Roundtable Summary Recommendations...

TRANSPARENCY IN THE PHARMA
SUPPLY CHAIN: KNOWLEDGE IS POWER!


Welcome & Topic Overview
Chris Skisak, PhD, HBCH
Executive Director




“Every
employer needs
to hear this”
June 2019
Employer-Only
Roundtable

Roundtable
Summary
Key Insights
Employers define value as having the right drug at the right price
Challenges include transparency
Biggest problem is high cost sharing
Need for effective formularies
Little confidence in a legislative fix

Roundtable
Summary
Recommendations
Recommend Recommend independent third-party audits
Assist Assist employers identify value comparison tools
Push Push for federal legislation
Support Support collaboration across employers and coalitions
Hold Hold PBMs accountable for formulary cost savings strategies
Implement Implement integrated site-of-care solutions
Eliminate Eliminate rebates and require full transparency

Agenda
8:40–9:00 Understanding the Pharmacy Supply Chain
James Dolan, PhD, Vice President, EY Parthenon, Life Science Strategy
9:00-9:20 Understanding Specialty Drugs
Heather Sundar, PharmD, SVP, Archimedes-Rx
9:20-9:40 Understanding & Surviving PBM Contracting
Tim Thomas, R.Ph. President, Crystal Clear Rx
9:40-10:00 Understanding Waster Drugs
Lauren Vela, Senior Director, Pacific Business Group on Health
10:00-10:15 Networking Break
10:15-11:00 Panel Discussion, Q and A

Resources
Report on 2019 Employer Rx Roundtables
2019 Purchasers Guide to PBM Quality
https://www.nationalalliancehealth.org/initiatives/initiatives-national/pharmacy-and-medical-drugs

© ARCHIMEDES 2018
The Specialty Challenge
• Price, Price, Price
• Overprescribing and questions of
value
• Siloed vendors
• Lack of cost transparency
• Vendor conflicts of interest
12
Confidential and Proprietary

© ARCHIMEDES 2018
What is a SWAT?
13
• Description: An analysis of the waste and
inappropriate use of specialty drugs across
the pharmacy and medical benefit
• Purpose: To identify opportunities to better
manage specialty drug utilization from a
cost and quality perspective
• Scope: Includes reimbursement, clinical
management, and benefit design
• Prioritization: Prioritize recommendations
and finalize an action plan for
implementation
Specialty
Waste
And
Trend Analysis
Confidential and Proprietary


Understanding the Pharma
Supply Chain
James Dolan, Vice President, EY-
Parthenon, Life Science Strategy

Overview of Pharmacy Trends in the US
Market Trends Impacting the Future
February 2020

EY-Parthenon | Page 17
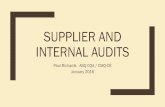
Illustrative funds flowThe following schematic represents the flow of funds across the pharmacy value chain, underscoring the considerable value “lost” through PBM intermediation
Source: EY-Parthenon Analysis
PBM/PBA
PharmaManufacturer
Carriers
Employer
Pharmacy
Provider
Patient
Admin fees to PBM
Copay
Wholesaler
Funds flow
Rebate transferred to Employer

EY-Parthenon | Page 18
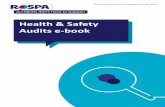
Illustrative product flowPhysical product flow is relatively direct from manufacturers to pharmacies; PBMs deliver utilization reports as part of contracted services
Source: EY-Parthenon Analysis
PBM/PBA
PharmaManufacturer
Carriers
Employer
Pharmacy
Provider
Patient
Patient fills prescription
Wholesaler
Product flow
Utilization report of generic and branded medicines

EY-Parthenon | Page 19
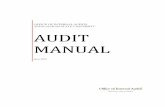
CAGR
(‘11-‘17)
6%
4%
-3%
17%
Market context and trendsIndustry growth is being driven by specialty pharmaceuticals on a revenue basis, and generics by volume
Source: IQVIA
300
100
0
200
400
$500b
20132011 2012 2014 2015 2016 2017
$328b$318b
$332b
$379b
$425b$446b $453b
Branded Specialty
Branded Traditional
Generics
2009 20132011 2015 2017
50%
60%
70%
80%
90%
% o
f T
ota
l R
x
U.S. Pharmaceutical Spend (Non-Discounted)
Generic Share of Dispensed Presciptions

EY-Parthenon | Page 20
Market context and trendsSeveral key factors across pharma and healthcare are transforming the macro landscape in which PBMs and payers operate
Source: EY-Parthenon Analysis

EY-Parthenon | Page 21Source: EY-Parthenon Analysis, incorporating public and proprietary sources for market sizing and sector allocations
Final Macro TrendU.S. Healthcare Spending: $3.5T and growing
U.S. Health Expenditures, 2018
Provider Life Sciences
Payer Gov’t/Public Health

EY | Assurance | Tax | Transactions | Advisory
About EY
EY is a global leader in assurance, tax, transaction and advisory services. The
insights and quality services we deliver help build trust and confidence in the capital
markets and in economies the world over. We develop outstanding leaders who team
to deliver on our promises to all of our stakeholders. In so doing, we play a critical role
in building a better working world for our people, for our clients and for our
communities.
EY refers to the global organization, and may refer to one or more, of the member
firms of Ernst & Young Global Limited, each of which is a separate legal entity. Ernst
& Young Global Limited, a UK company limited by guarantee, does not provide
services to clients. For more information about our organization, please visit ey.com.
Ernst & Young LLP is a client-serving member firm of
Ernst & Young Global Limited operating in the US.
EY-Parthenon refers to the combined group of
Ernst & Young LLP and other EY member firm
professionals providing strategy services worldwide.
Visit parthenon.ey.com for more information.
© 2020 Ernst & Young LLP.
All Rights Reserved.
This material has been prepared for general informational purposes
only and is not intended to be relied upon as accounting, tax or other
professional advice. Please refer to your advisors for specific advice.
ey.com

Understanding Specialty Drugs
Heather Sundar, SVP, Consulting
and Employer Solutions,
ArchimedesRx
No Presentation for Heather Sundar Attached
at ArchimedesRx Request


Understanding & Surviving PBM
Contracting
Tim Thomas, President, Crystal
Clear Rx

slide 26
Understanding PBM Contracting

slide 27
Understanding PBM Contracting
(OK surviving PBM Contracting)

slide 28

KEY POINTS TO REMEMBER
There are only two ways to manage Rx cost
1) Manage distribution cost by negotiating
the Best Pharmacy Price Mgt (PBM)
contract possible
2) Manage member utilization
(Formulary and clinical choices)
29

KEY POINT TO REMEMBER ONE (Manage Distribution Cost)
30
We do an Request For Promises
We choose a Pharmacy Price Mgt. (PBM) model
(Traditional, Transparent or Pass Through)
We try to get the best deal by
1) Pitting PBMs against each other
2) Negotiating the best contract

Types of Pharmacy Price Management (PBM) Service Models
TraditionalMakes $ in three main ways
1) Network Spread
2) Rebates
3) Operations from owned
pharmacies
Usually no administration fee
TransparentMakes $ the same
way as Traditional
Pass ThroughMakes $ by charging an
administration fee
31

The current way Pharmacy Price Mgt. (PBMs) are judged
AWP (Ain’t What’s Paid)
Discounts are a flawed and
misleading way of judging
PBM performance
1) It is not an average
2) The discount is easily
manipulated

How are baseball statistics and AWP
Discounts similar?
The Houston Astros batting average
for 2019 was 0.274.
Do you think their batting average
will go up or down in 2020?
IT DEPENDS

Assumption: Good AWP Discounts are a
good way to judge PBM performance
Is an AWP discount of 78 % for retail
generics good?
IT DEPENDS

Unit Cost may be a better way to judge
Example (ALL Retail Generics) for 2018:
AWP Discount Cost per Unit
Group 1
(Big 3 PBM)
Group 2
(Pass Thru PBM)
AWP - 77.94%
AWP - 78.48%
$0.595
$0.362
35

Contract negotiations
36
Definitions are critical
a) Brand/Generic
b) What is missing?
Monitor your PBM and have a Market check done by you or
your consultant (Not PBM) and have actions tied to the
results
Be absolutely clear on any price lists (MAC, Specialty)
What is included or excluded in any pricing GUARANTEE?

What Pharmacy Price Management (PBMs) do well
Develop and maintain network of pharmacies
Provide a transaction processing system
Negotiate with Pharmaceutical manufacturers
(Provide a drug “formulary”)
Provide basic clinical services
Prior Authorization
Step Therapy
Provide a Mail Order/Specialty Pharmacy

What some Pharmacy Price Management (PBMs) don’t do well
Provide Transparency and Trust that they are
working for your best interests
Look for the lowest net cost drug THERAPY
Manage the 2 % of the population that is costing
groups the most money

KEY POINT TO REMEMBER TWO (Manage Member Util.)
39
2 to 5 % of your population are
likely to be costing your
organization 50 to 60 % of the
total spend for prescription drugs

Should that 2 – 5 % be managed differently than the rest?
Patients are lucky to get 15 minutes with their doctor
Pharmacists are forced to fill hundreds of Rxs/day
Internet can be helpful, but also dangerous

Medication Care Management
Among Heart Failure patients eligible for all
classes of medication, 1% (ONE PERCENT)
were receiving target doses of medication.*
According to the American Heart Association, poor medication
adherence takes the lives of 125,000 Americans annually, and
costs the health care system nearly $300 billion a year in
additional doctor visits, emergency department visits and
hospitalizations
* CHAMP-HF (Change Management of Patients with Heart Failure study)

What if you have negotiated a GREAT PBM contract rate?
Even with the best negotiated PBM contract you
could still be paying way too much

Even with a good PBM contract things can cost way too much
Vimovo (Nexium 20 mg and Naprosyn 500 mg combination in
one pill)
Cost for 60 pills (Good Rx) $ 2,465
Nexium 20 mg (Generic) $ 28
Naprosyn 500 mg (Generic) $ 8
Total $ 36
If member doesn’t know about this then the group pays $ 29,148
MORE each year for EACH member
43

Rebate Driven FORMULARY Stomach acid/reflux therapy
Example: Dexilant
On many PBM
Formularies because
of high rebate
But net cost doesn’t
justify decision
Dexilant Ingredient Cost per pill approx. $ 9.00
Dexilant Rebate per pill approximately $ 5.00
Net Cost to Group per pill $ 4.00
Generic Nexium Ingredient Cost
approximately $ 0.75
Net Cost to Group for every Dexilant pill $ 3.00
44

KEY POINTS TO REMEMBER
There are only two ways to manage Rx cost
1) Manage distribution cost by negotiating
the Best Pharmacy Price Mgt (PBM)
contract possible
2) Manage member utilization
(Formulary and clinical choices)
45

slide 46
Things you can do before it goes off the rails
• Get the best unbiased and only working for you help
• Review and improve your PBM contract(s)
• Monitor what goes on and have market check provision
• Engage your providers and members

slide 47
Questions?

slide 48
Contact Information
Tim Thomas, R.PhPresident, Crystal Clear [email protected]@crystalclearrx.com

Understanding Wasteful Drugs
Lauren Vela, Senior Director,
Pacific Business Group on Health

HBCH
Knowledge is PowerFebruary 27, 2020

Pacific Business Group on Health
PBGH Mission:To be a change agent creating increased value in the healthcare system through purchaser collaboration, innovation and action, and through the spread of best practices
Purchasing Value
• Employers Center of Excellence (ECEN)
• Purchaser Value Network (PVN)
• Maternity Payment Reform
• Meaningful Measures/Common ACO Measures
• Accountable Pharmacy
• Low Value Care
• Mental health/Primary Care integration
• Benefit design best practices
Functional Markets
• Influence CMS Policy
• Health Care Payment Learning and Action Network (HCPLAN)
• Health Care Transformation Task Force (HCTTF)
• Antitrust advocacy
• Drug Pricing Policy
• Measurement/transparency
Advanced Primary Care (Care Redesign)
• Intensive Outpatient Care Program (IOCP/AICU)
• Practice Transformation
• California Quality Collaborative (CQC)
• Maternity Transformation
• Patient Reported Outcomes
• Measurement/transparency
51

52Agents for Change PBGH Members - Partial List

53The PBM Business Model is a problem

54PBM Revenue Streams are an intermingled mess…that you can’t see through the sauce!
• Rebate negotiations with pharma will impact formulary design and PBM revenues
• Non “rebate” revenue from pharma also impact formulary placement
• Rebates and fees associated with one drug will often be connected to, or “bundled” with other drugs
• Rebate negotiations are impacted by pre-authorization protocol
• Pre-authorization can impact number of scripts, and the drugs selected, all of which impacts PBM bottom lines
• PBM collects UM fees from clients and utilizes pharma-supplied UM services, for which they might also get paid.
• PBMs pay pharmacies less than they charge employers (spread)
• PBM management of generic definition, AWP source, and AWP date will embellish revenues
• Pharmacy relationships will impact DIR and other fees• Pharmacies might be owned by PBM• Mail order might imply more fees for packaging/labeling
drugs• PBMs will aggregate rebates for a “wholesaler” market
• Rebate “pass through” for jumbo employers will increase market share (and rebate retention) for smaller clients
• ETC.!!!!

55
1. Is there substantial waste on the formularies of large, self-insured employers? YES
2. Would doctors prescribe to a common, waste-free formulary?
3. NOT NECESSARILY, NOT PRACTICAL
4. Would employers adopt a common waste-free formulary?
5. EMPLOYERS WILL ELIMINATE WASTE
Managing a formulary pays off
1.Is there substantial waste on the formularies of large, self-insured employers?
2. Would doctors prescribe to a common, waste-free formulary?
3. Would employers adopt a common waste-free formulary?

56
• 15 Data Donors submitted data (4 ESI, 8 CVS, 3 Optum)
• 2,543,907 claims evaluated of which 6% were wasteful, consisting of 868 different drugs
• Data was limited, assumptions were conservative➢No controversial drugs (.01% specialty)
➢Only considered if excluding the drug saved > 25%
➢Savings had to apply across formularies, i.e. specific formulary “deals” were excluded
➢Case study-based assumptions about patients’ behavior
➢Savings were 11% less than comparative case studies due to conservative assumptions
• Estimated savings of this data set was $63.3 million
• Represented 2.8% to 24% of total PBM spend (for 9 data donors for whom we knew total spend. 10-24% for 7 of the 9. Two of the 9 had already begun managing their formulary.
PBGH Waste Free Formulary Project

573. Will employers remove waste?
http://www.pbgh.org/news-and-publications/pbgh-in-the-news/539-save-4-25-off-your-pbm-spend

58
Biosimilars =
Specialty drugs manufactured using same processes as their “reference drugs” with NO clinical difference

59Patent “Thicket”
26 Approved Biosimilars
-12 Launched Biosimilars
= 14 Tied up in a Patent Thicket

60Problem YOU Can Solve. 12 biosimilars launched. Uptake slow.
Health plan /PBM Rebates
Buy and Bill
As EASY as 1-2-31. Ask your health plan to report on the opportunity for you to save if biosimilars were used2. Ask your health plan their coverage policies for all biosimilars3. Talk with your providers about why they are not using biosimilars



NETWORKING BREAK
15 Minutes

Panel Discussion and Q&A