
Translation of Methodology Used In Human Myocardial...
12
* Corresponding author: Elizabeth Bailey, Department of Nuclear Medicine, Royal North Shore Hospital, St Leonards, NSW. Australia 2065; Fax: +61 (0)2 9926 4099; Phone: +61 (0)2 9926 4440; Email: [email protected] © 2013 mums.ac.ir All rights reserved. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Translation of Methodology Used In Human Myocardial Imaging to a Sheep Model of Acute Myocardial Infarction Elizabeth A Bailey *1,3 , Dale L Bailey 1,3,4 , Stephen Hunyor 2,4,5 , Leigh Ladd 5,6 , George J Bautovich 1 1 Department of Nuclear Medicine, Royal North Shore Hospital, Australia 2 Department of Cardiology, Royal North Shore Hospital, Australia 3 Discipline of Medical Radiation Sciences, University of Sydney, Australia 4 Sydney Medical School, University of Sydney, Australia 5 Cardiac Technology Centre, North Shore Heart Research Group, Kolling Institute, Australia 6 Charles Sturt University, Wagga Wagga, Australia ARTICLE INFO Article type: Original article Article history: Received: 12-Jun-2013 Revised: 18-Jul -2013 Accepted: 23-Jul -2013 Keywords: Myocardial perfusion Imaging, SPECT/CT, Ovine model, Mesenchymal stem Cells ABSTRACT Introduction: Pre-clinical investigation of stem cells for repairing damaged myocardium predominantly uses rodents, however large animals have cardiac circulation closely resembling the human heart. The aim of this study was to evaluate whether SPECT/CT myocardial perfusion imaging (MPI) could be used for assessing sheep myocardium following an acute myocardial infarction (MI) and response to intervention. Methods: Eighteen sheep were enrolled in a pilot study to evaluate [ 99m Tc]-sestamibi MPI at baseline, post-MI and after therapy. Modifications to the standard MPI protocols were developed. All data was reconstructed with OSEM using CT-derived attenuation and scatter correction. Standard analyses were performed and inter- observer agreement was measured using Kappa (). Power determined the sample sizes needed to show statistically significant changes due to intervention. Results: Ten sheep completed the full protocol. Data processed was performed with pre-existing hardware and software used in human MPI scanning. No improvement in perfusion was seen in the control group, however improvements of 15%-35% were seen after intra-myocardial stem cell administration. Inter-observer agreement was excellent (К=0.89). Using a target power of 0.9, 28 sheep were required to detect a 10-12% change in perfusion. Conclusion: This study demonstrates the suitability of large animal models for imaging with standard MPI protocols and its feasibility with a manageable number of animals. These protocols could be translated into humans to study the efficacy of stem cell therapy in heart regeneration and repair. Please cite this paper as: Bailey EA, Bailey DL, Hunyor S, Ladd L, Bautovich GJ. Translation Of Methodology Used In Human Myocardial Imaging To A Sheep Model Of Acute Myocardial Infarction. Asia Oceania J Nucl Med Biol 2013; 1(2):10-21. Introduction Advances in developmental and cell biology have created great interest in the potential of stem cell therapy to repair and regenerate the damaged heart, however, substantial challenges remain before this becomes an effective and safe therapeutic option (1). One of the major issues is the discrepancy between positive outcomes from stem cell therapy in rodent models following experimental myocardial infarction (MI) and the results from clinical trials performed in humans (2-5). While rodent studies show functional improvements of 15-20% in heart pumping capacity, a meta-analysis of human trials only showed a small transient (~4%) improvement in left ventricular ejection fraction (LVEF), with one
Transcript of Translation of Methodology Used In Human Myocardial...

* Corresponding author: Elizabeth Bailey, Department of Nuclear Medicine, Royal North Shore Hospital, St Leonards, NSW. Australia 2065; Fax: +61 (0)2 9926 4099; Phone: +61 (0)2 9926 4440; Email: [email protected]
© 2013 mums.ac.ir All rights reserved. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Translation of Methodology Used In Human MyocardialImagingtoaSheepModelofAcuteMyocardialInfarction
Elizabeth A Bailey*1,3,DaleLBailey1,3,4,StephenHunyor2,4,5,Leigh Ladd 5,6,GeorgeJBautovich1
1DepartmentofNuclearMedicine,RoyalNorthShoreHospital,Australia2DepartmentofCardiology,RoyalNorthShoreHospital,Australia3DisciplineofMedicalRadiationSciences,UniversityofSydney,Australia4SydneyMedicalSchool,UniversityofSydney,Australia5CardiacTechnologyCentre,NorthShoreHeartResearchGroup,KollingInstitute,Australia6CharlesSturtUniversity,WaggaWagga,Australia
ARTICLEINFO
Article type: Originalarticle Article history: Received:12-Jun-2013Revised:18-Jul-2013Accepted:23-Jul-2013 Keywords: MyocardialperfusionImaging,SPECT/CT,Ovinemodel,MesenchymalstemCells
ABSTRACT
Introduction: Pre-clinical investigation of stem cells for repairing damagedmyocardium predominantly uses rodents, however large animals have cardiaccirculationcloselyresemblingthehumanheart.TheaimofthisstudywastoevaluatewhetherSPECT/CTmyocardialperfusionimaging(MPI)couldbeusedforassessingsheep myocardium following an acute myocardial infarction (MI) and response tointervention.Methods:Eighteensheepwereenrolledinapilotstudytoevaluate[99mTc]-sestamibiMPI at baseline, post-MI and after therapy. Modifications to the standard MPIprotocolsweredeveloped.AlldatawasreconstructedwithOSEMusingCT-derivedattenuation and scatter correction. Standard analyses were performed and inter-observeragreementwasmeasuredusingKappa().Powerdeterminedthesamplesizesneededtoshowstatisticallysignificantchangesduetointervention. Results: Tensheepcompletedthefullprotocol.Dataprocessedwasperformedwithpre-existinghardwareandsoftwareusedinhumanMPIscanning.Noimprovementin perfusion was seen in the control group, however improvements of 15%-35%wereseenafterintra-myocardialstemcelladministration.Inter-observeragreementwasexcellent(К=0.89).Usingatargetpowerof0.9,28sheepwererequiredtodetecta10-12%changeinperfusion.Conclusion: This study demonstrates the suitability of large animal models forimagingwithstandardMPIprotocolsanditsfeasibilitywithamanageablenumberofanimals. These protocols could be translated into humans to study the efficacy ofstemcelltherapyinheartregenerationandrepair.
Please cite this paper as:
Bailey EA, Bailey DL, Hunyor S, Ladd L, Bautovich GJ. Translation Of Methodology Used In HumanMyocardialImagingToASheepModelOfAcuteMyocardialInfarction.AsiaOceaniaJNuclMedBiol2013;1(2):10-21.
Introduction
Advances in developmental and cell biologyhave created great interest in the potential ofstem cell therapy to repair and regenerate thedamaged heart, however, substantial challengesremainbeforethisbecomesaneffectiveandsafetherapeuticoption(1).Oneofthemajorissuesisthediscrepancybetweenpositiveoutcomesfrom
stem cell therapy in rodent models followingexperimentalmyocardial infarction (MI) and theresults from clinical trials performed in humans(2-5). While rodent studies show functionalimprovements of 15-20% in heart pumpingcapacity, a meta-analysis of human trials onlyshowedasmalltransient(~4%)improvementinleftventricularejectionfraction(LVEF),withone

Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 11
study showing no benefit(6). Complexities arisepartly from the use of a variety of stem cellsincluding embryonic (ESC) and adult stem cells(ASC) derived fromseveral tissues such as bonemarrow, induced pluripotent stem cells (iPSC)andresidentcardiacstemorprogenitorcells(7-9).
Theup-scalingfrombasicscienceinrodentstoclinical trials in humans often encounters a“translationalgap”whichcanbeovercomebytheuseofanintermediatestageusinglargeanimals.Functional and cellular consequences ofmyocardial infarction and response to therapycan be readily studied in sheep and pigs withtechniquesdirectlyapplicabletohumansubjectsdue to similarities in heart size, anatomy,coronary supply and molecular machinery(10).One such example is the use of stem cells torepair damaged myocardiumwherecontroversyabounds as to the appropriate method ofadministration of the cells i.e., systemic, intra-arterialordirectlyintothemyocardium.
Manyimagingstudieswithmesenchymalstemcells (MSCs) have attempted to trace the fate ofthe implanted cells using a label suitable forimaging.Studiesonrodentsusingdirectinjectionof [111In]-labelled bone marrow-derived MSCsinto the affected area of heart muscle to assessstem cell therapies have presented difficultiesduetothesmallheartsize(11).Imagingthefateof transplanted cells using labelling techniqueswithradionuclides,paramagneticironoxidewithMRI, or optical probes are problematic (11, 12).Therelativelyshorthalf-lifeofsomeradiotracersmay preclude long-term tracking and theradiation effects on cell viability have not beendetermined, making such studies largelyunsuccessfulandchallenginginhumans(13).
Thereare nopublishedstudiesusinganovine(sheep)modeltostudymyocardialfunctionusingSPECT/CT.Wethereforesetouttoinvestigatethepotential to image the myocardium before andafter stem cell transplantation using readilyavailable myocardial perfusion imaging (MPI)techniques.Theaimofthestudywastoevaluatethe potential for SPECT/CT and diagnostic toolsroutinely used in the clinical setting to assessmyocardial injury and potential recoveryfollowing stem cell transplantation in a sheepmodel of acute myocardial infarction. Ifsuccessful, these approaches could be widelyemployed to more rapidly facilitate translationfromtheanimalmodelintoman.
Methods
A pilot study approved by the localInstitutional Animal Care and Ethics Committee(RNHS/UTS 0504-018A) was undertaken to
study eighteen Border Leicester/Suffolk-crossfemalesheepusingMPISPECT/CTat(i)baseline,(ii)followingmyocardialinfarction,and(iii)aftertherapeuticintervention.
Imaging Parameters and Protocols All studies were acquired using a hybrid
SPECT/CT system consisting of a SKYLightgamma camera (Philips, Milpitas, USA) and aPQ5000CTscanner(PickerCorp,Cleveland,USA)(14). The sheep were positioned in the rightdecubitus position with the limbs folded andsecured against the torso. In this position theheart has an orientation with respect to thedetector above the animal, similar to a leftanterior oblique in man with the apex of theheart being caudal (equivalent to inferior) andmedial, and the base of the heart more cranial(equivalenttosuperior)andtotheleft,asseeninFigure1.
A resting MPI study was commenced 15minutes after injection of 1.5 GBq [99mTc]-Sestamibi (Cardiolite®, Lantheus MedicalImaging, Massachusetts, USA) to assessmyocardial perfusion and function. TheacquisitionconsistedofagatedMPISPECTstudyusinga 128×128matrix with 16 timebinsat15seconds per projection for 120 projections (60perdetector, 3° radial increments) using ahigh-resolution collimator (VXGP), followed by a CTscan using a �ixed beam current of 100 mAs, atubevoltageof120kVpandapitchof1givingaslice thickness of 4 mm. After two days, an MIwasinducedusinga60minuteballoonocclusion(5F Judkins catheter, MayoHealthcare) of thedominant branch of the paraconal artery(equivalenttotheleftanteriordescendingarteryin man) using a carotid artery cut-downapproach followed by reperfusion. Between 5and 7 days after MI, a repeat MPI study wasperformed to confirm the presence, location,extent, size and severity of the defect. If asignificant or measurable defect was identified,then the sheep were allocated to one of threearms of the study with the imaging teamremainingblindedtothefinaltreatmentarm:
Group1:thecontrolsheepweregiven1mLof a placebomedium (stem cell suspension)injecteddirectlyintothemyocardium;
Group2:MSCs(10106cells)insuspensionwereinfusedover1minuteviaintra-arterialcatheter (IC) into the left coronary arterywith the cells most commonly injected intothe arteries supplying the border zones oftheMI(15);
Group 3: MSCs (10 106 cells) weredelivered by intra-myocardial (IM) methodsusing10injectionsof0.1mLdirectlyintothe

Bailey EA et al Translation of Human MPI methods to a sheep AMI model
12 Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21.
peri-infarct zone of the myocardium eitherunder direct vision at thoracotomy orepicardially via cardiac catheter into theinjured“borderzone”(16).
Fivetosixweeksfollowingtheinterventionthestandard MPI imaging protocol was repeated asoutlinedabove.
Anaesthesia Protocol The sheep were fasted of solids but allowed
water ad libitum the night beforeanaesthesia todecreasetheriskofaspiratingstomachcontentsand to avoid interference with cardiac imaging.Thecephalicveinintheneckwascannulatedforthe anaesthesia. For the myocardial perfusionstudies, light anaesthesia was induced withAlfaxalone(Alfaxan,Jurox,Australia)atadoseof1 to 1.5 mg/kg I.V. and then maintained withisoflurane in oxygen titrated to maintain effectwhile respiration was controlledby intermittentpositive pressure ventilation. Pupil size, jawtone, movement, ECG and blood pressure wereusedtomonitorthelevelofanaesthesia.Surgerywasperformedbyanexperiencedcardiovascularsurgeon to minimise tissue damage and anyprocedure related complications. Post-operatively the sheep were treated withBuprenorphine and Carprofen (a non-steroidalanti-inflammatory) for analgesia and werecontinuously monitored until standing, at whichpoint respiration and heart rate stabilised andnormaleatinganddrinkingbehaviourresumed.
Image Reconstruction of Myocardial Perfusion Images
Studies were reconstructed using twomethods: Filtered Back-Projection (FBP) (200%zoomand2Dpre-filteringwithButterworthfilterat an order of 10 and cut-off of 1.0 cycle/cmfollowed by FBP using a ramp filter) and aniterativereconstructionusingtheOrderedSubsetExpectation-Maximisation (OSEM) algorithm(17)using8subsetsoftheprojectiondataand4iterations. After reconstruction the data were�ilteredwitha3DButterworth�ilter(orderof1.2and cut-off of 0.8 cycles/pixel). Due to thedifferent anatomical orientation of the sheepheart compared to the human heart, the studieswere rotated +270° during reconstruction andthenre-oriented-180° intheX-Ydirectionand-120° in the Y-Z plane to generate conventionalcardiacobliqueshortaxisslices.
Attenuation and scatter correction wereperformed using a CT-derived attenuation mapthat was generated by converting the CTHounsfield units to the linear attenuationcoefficients () for 99mTc (18). A transmission-dependent scatter correction (TDSC) method
usingtheCTdatawasusedtocorrectforscatterintheprojectiondata(19).Thisthenallowedforquantitative analysis of the data. The resultanttransverse �iles were resampled into a 6464matrix (a requirementof the analysis software )with the heart centred in the field of view andreviewedqualitativelyusingtheCedars-SinaiQPScardiac software review package (20).Investigatorsanalysing the studieswere blindedtothetreatmentgroup.
Data Analysis Polar maps of myocardial perfusion were
generated using the QPS package with a 20segment scoring system of relative perfusion.These relative perfusion scores were used tocalculate a normalised perfusion index for eachsegment on both the immediate post-MI imagesand post-therapy images. Perfusionrecovery(ormean change) as a percentage of baseline wasthen calculated for each study. LVEF, enddiastolic volume (EDV) and end systolic volume(ESV)werecalculatedfromthegatedMPIimagesat baseline, post-MI and post-therapy to assessLV functional change using the 4DMSPECTcardiacsoftwarereviewpackage(21).
The data were also qualitatively reviewedindependently by two experienced nuclearmedicine physicians with over 35 man-years ofexperience reporting MPI SPECT between them.Datawereviewedinmatchingpairsof,inthefirstinstance,thebaselineandpost-MIstudies,andinthesecondcasecomparingthebaselineandfinalimaging time-point to assess changes inperfusion,includingareviewofthegatedimagesto assess wall motion abnormalities. A clinicalreport was generated for each pair of studiesusing the standard cardiac review format asrecommendedby the current guidelines forMPIreporting(22,23).
Eachreviewerwasprovidedwithapolarmapdisplay template containing the 20 segmentmodeloverlaywithascoringguidelinetorecordthe location and severity of the abnormality(Figure2).Acategorical5-pointscoringscalewasusedrangingfrom0fornormalthroughto4forasevere abnormality. The results were analysedusingaKappa()statistictomeasureagreementbetweenreviewers(24).
Matching pairs of data (Baseline/Post-MI andBaseline/Post-therapy) were analysed using thePERfitCardiacpackage(HermesMedical,NuclearDiagnostics,Sweden).Shortaxissliceswereusedtogeneratecircumferentialprofilesfromapextobaseofheartthatcontained12pro�ileseachwith40 elements, giving a total 480 elements perstudy (9° arcs). The meanchange frombaselineto post-MI and post-therapy for each elementwas calculated with a change of ≥ 10% being

Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 13
considered significant. The z-score of eachelementwascalculatedtoquantifythenumberofstandard deviations that the original value isrelativetothemeanandtodeterminechangeinperfusionfrombaseline.
Echocardiography Protocol Anechocardiogramwasperformedatbaseline
in all animals and after the intervention in aselected cohort of the animals. The sheep werepositioned in the right decubitus position andsecured to the imaging bed with the limbsextendedforward.Thesheepremainedconsciousduring the procedure however a patch wasplacedovertheeyestoreduceanimalstressandmovement.Anareabehindthe left forelimbwasshavedtoensuregoodcontactofthetransducerwith the skin. Measures of LVEF, EDV and ESVwererecordedtoassessmyocardialfunctionandforcomparisonwithgatedMPIresults.
Post Mortem Procedures
The sheep were euthanized after the finalimagingtime-point6-8weeksaftertheMI.Whilstanaesthetised, the sheep were injected with400MBq of [99mTc]-Sestamibi soas toallow imagingoftheheartforvisualconfirmationoftheinfarctlocationwith the ex-vivo anatomicslices. After5minutes the sheep were sacrificed withoutrecoveryfromanaesthesiausinga lethaldose(2g I.V.) of potassium chloride (KCl) givenintravenouslyviatheindwellingvenouscatheter.After the heart ceased beating, body tissuesincludingtheheart, lung, liverandkidneyswereexcised for further examination. The heart wasfixed with formalin and then sectioned evenlythrough the short axis plane into 5 to 10 mmthick slices for histological sampling. The heartslices were placed on a template ordered fromapextobaseandimagedbyplacingthetemplatedirectly on top of the collimator of an upturnedgammacamerausinga512512matrixfor300seconds. The heart sections were reviewedmicroscopic-ally to confirm the presence of anMI, to assess the extent, if any, ofneovascularisation,and forcorrelation withMPIfindings.
Results
The studyenrolled 18 ewes ranging in weightfrom45to50kgwithabaselinerestingLVEDVof 80 to 90 ml measured by echocardiography.Ten sheep completed the full protocol includingpost mortem anatomical correlation. Within thethreetreatmentgroupstherewasacontrolgroup(n=3), an intra-coronary infusion group (n=3)andanintra-myocardialinjectiongroup(n=4).
During the MI induction procedure six sheephad irreversible ventricular fibrillation andsuccumbed. Of the remaining 12 animals, sheep#8 had a perfusion abnormality at baselineimaging in the apical region and was excluded.
Figure1.CoronalprojectionfromthechestCTperformedonsheep 12 showing the orientationof the heart in the humanstandingposition.Alignmentofthesheepheartismirroredascomparedtothehumanorientation.
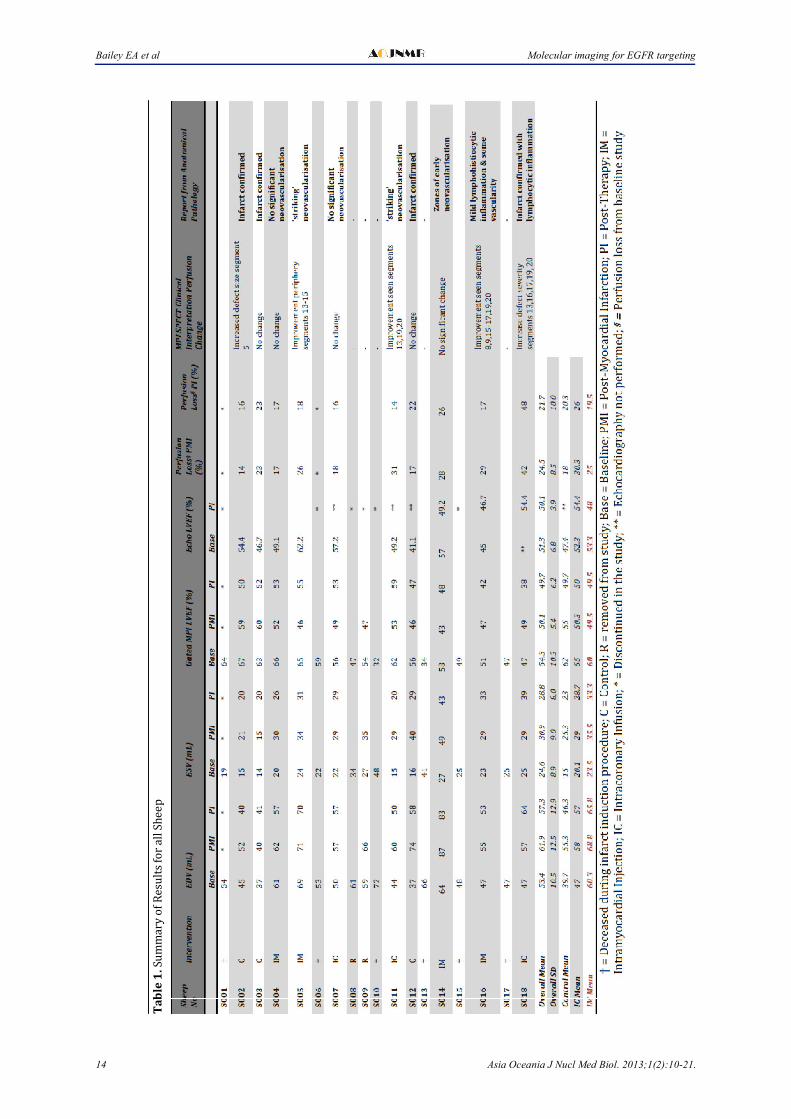
Sheep #9 successfully completed baselineimagingandproceededtoMIinduction,however,no subsequent perfusion defect was seen on theMPI study and was therefore excluded. TheresultsforallanimalsaresummarisedinTable1.
Clinical Interpretation All images from the final cohort of sheep thatcompletedthefullimagingprotocolweresuitablefor reconstruction and analysis using theconventionalsoftware toolsavailable forclinicalinterpretation of MPI studies in man. In thecontrol arm, no improvement in perfusion wasidentified from the post-MI images to the finalimaging time-point. An example is shown inFigure 3 (sheep #12), where the baseline studyshows normal uniform tracer distributionthroughout the myocardium with a subsequentperfusiondeficitseenpost-infarctionintheapexwith a change in perfusion of -17%. The defectsize increased at the final time-point with afurther loss in perfusion to -22% relative tobaseline. This was correlated microscopicallywith identification of fibrous scar tissue withlymphoid aggregates, histiocytes and calciumdepositsinthesameregion.ThegatedMPILVEFshowedadeclineof-14%frombaselinetopost-therapy(Table1).
Quantitative Analyses Overall,inthissmallcohortthemeanLVEFfor
both the IC and IM MSC implantation methodsshowed no statistically significant improvementin LV function. An average change of -7% and
Bailey EA et al Molecular imaging for EGFR targeting
14 Asia Oceania J Nucl Med Biol. 2013;1(2):10-21.
Ta
ble
1.S
um
mar
yo
fR
esu
lts
for
allS
hee
p
Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 15
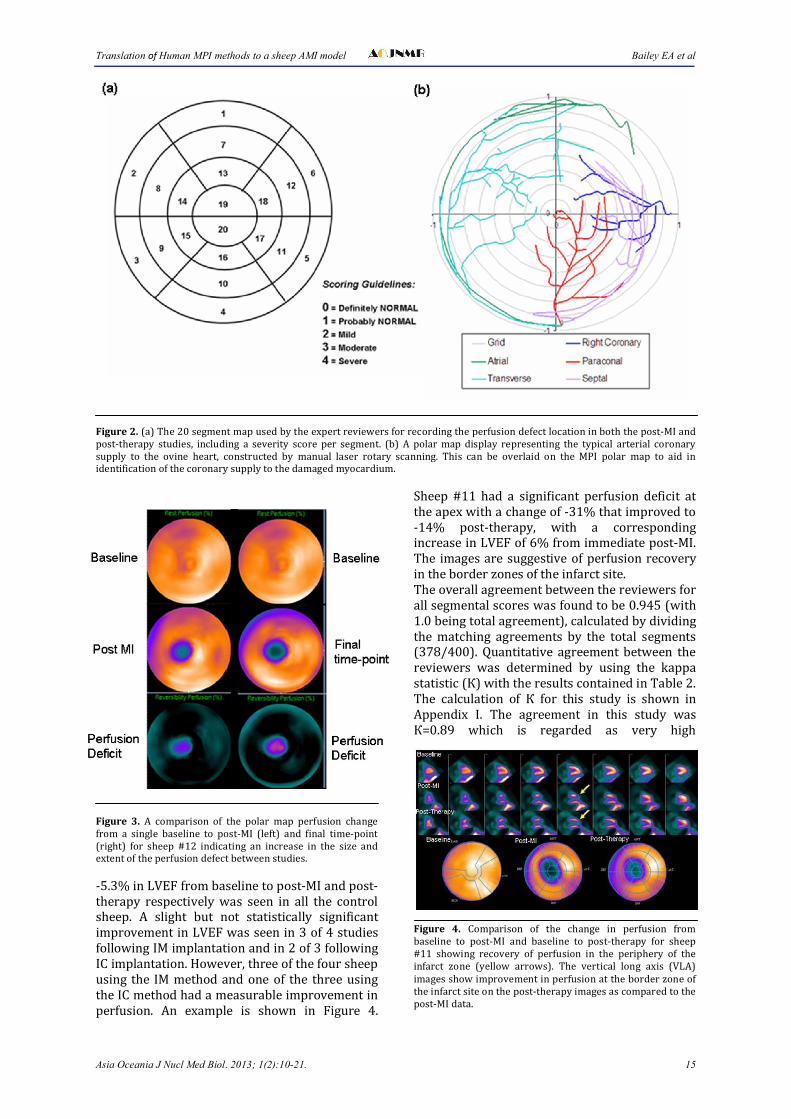
Figure2.(a)The20segmentmapusedbytheexpertreviewersforrecordingtheperfusiondefectlocationinboththepost-MIandpost-therapy studies, including a severity score per segment. (b) A polar map display representing the typical arterial coronarysupply to the ovine heart, constructed by manual laser rotary scanning. This can be overlaid on the MPI polar map to aid inidentificationofthecoronarysupplytothedamagedmyocardium.
Figure 3. A comparison of the polar map perfusion changefrom a single baseline to post-MI (left) and final time-point(right) for sheep #12 indicating an increase in the size andextentoftheperfusiondefectbetweenstudies.
-5.3%inLVEFfrombaselinetopost-MIandpost-therapy respectively was seen in all the controlsheep. A slight but not statistically significantimprovementinLVEFwasseenin3of4studiesfollowingIMimplantationandin2of3followingICimplantation.However,threeofthefoursheepusing the IM methodand one of the three usingtheICmethodhadameasurableimprovementinperfusion. An example is shown in Figure 4.
Sheep #11 had a signi�icant perfusion deficit attheapexwithachangeof-31%thatimprovedto-14% post-therapy, with a correspondingincreaseinLVEFof6%fromimmediatepost-MI.The imagesaresuggestiveof perfusion recoveryintheborderzonesoftheinfarctsite.Theoverallagreementbetweenthereviewersforallsegmentalscoreswasfoundtobe0.945(with1.0beingtotalagreement),calculatedbydividingthe matching agreements by the total segments(378/400). Quantitative agreement between thereviewers was determined by using the kappastatistic(К)withtheresultscontainedinTable2.The calculation of К for this study is shown inAppendix I. The agreement in this study wasК=0.89 which is regarded as very high
Figure 4. Comparison of the change in perfusion frombaseline to post-MI and baseline to post-therapy for sheep#11 showing recovery of perfusion in the periphery of theinfarct zone (yellow arrows). The vertical long axis (VLA)imagesshowimprovementinperfusionattheborderzoneoftheinfarctsiteonthepost-therapyimagesascomparedtothepost-MIdata.

Bailey EA et al Molecular imaging for EGFR targeting
16 Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21.
Figure5.Themeanchangeinperfusionfrombaselinetopost-MI(PMI)intheaffectedsegmentswasintherangeof6%to82%/Following intervention (a) the control arm (red) showed no signi�icant improvement in perfusion, however in (b) 1 of 3intracoronarygroup(green)and(c)3ofthe4intheintramyocardialgroup(blue)showedmildtomoderateperfusionrecovery.
agreement(24).
Using Pilot Data Results to Design Future Trials The significance of change was assessed using asemi-quantitative scoring algorithm (QPSsoftware) with a change in perfusion of >10%considered significant. Based on data alreadyavailable for assessing LV function using eithergated blood pool imaging or echocardiography,perfusionrecoveryfrompost-MItopost-therapyof≥5%couldbeconsideredasigni�icantchange(25-27).
and a maximum change of 12%. The standarddifference for a 7% change and standarddeviationof±10is0.7andfora12%changeitis1.2. Therefore the numberof subjects neededtodetect a 7% change with a study power of 0.8wouldbe60andforapowerof0.9itwouldbe80animals.However,ifthechangeinperfusionwasgreater,e.g.12%,thenumberofanimalsrequiredbecomes22(for0.8)and28(0.9)respectively.
The previous methods described to assessperfusionrecoveryfollowingtherapywerebasedon mean segment values generated by the QPS
Figure6.Sheep#3siteofMIinductionasindicatedby(A)thepresenceof�ibrousscartissueontheanatomicalsheepheartslicescorrelating with (B) a perfusion defect seen in the MPI heart slices (red arrow). (C) The presence of lymphoid aggregatesmicroscopicallyindicatestheformationofscartissue.
Themeanchangeinperfusionfrombaselinetopost-MIwascalculatedas-22%,withastandarddeviation of ±10.1% (Figure 5). Tocalculate thenumber of animals needed in any future studybasedonachangefrombaselineof-22%(d)witha standard deviation of ±10 (s), the standarddifference was therefore equal to 2 (d/s =22/10). Using a study powerof 0.8, the numberofanimalsrequiredtodemonstrateachangeduetotheMIwouldbe8,andwithastudypowerof0.9,thisnumberwouldincreaseto12.
Assessing the recovery after therapy wascalculated based on a minimum change of 7%
softwarepackage.However,asmyocardialrepairis more likely to occur around the edges of theinfarcted tissue, a voxel level analysis usingPerFit was undertaken. Results would suggestthat two of the four sheep in the IM treatmentgroup (sheep #5 and #14) have shown animprovement in perfusion in the infarcted areafollowingstemcelltherapyaswellasanincreasein global LVEF of 9% and 6% respectively. Theperfusion score and infarct zone results show apositiveshiftintheperfusionscoresintheinfarctzone with the z-score values indicating adecrease in variability to those areas. This

Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 17
Table2.Segmentalscoresbyblindedreviewersofthepost-MIandpost-therapyimages. Reader A
Severity 0 1 2 3 4 Total
Reader B
0 258 0 5 0 0 263
1 3 4 0 0 0 7
2 3 0 38 0 0 41
3 3 0 1 42 3 49
4 3 0 0 1 36 40
Total 270 4 44 43 39 400
Scoringcriteriawhere0=De�initelyNormal,1=ProbablyNormal,2=Mild,3=Moderateand4=Severe.
correlates with the anatomical findings ofprominent and early neovascularisation in thesameregion.OfthethreesheepintheICarm,twoof three sheep (sheep #7 and #11) had animprovement in perfusion following MSCimplantation, correlating with an increase inglobalLVEFof4%and6%respectively.
Confirmationofanareaofinfarctedtissuewasseen microscopically for all studies byidentification of fibrous scar tissue with thepresenceoflymphoidaggregates,histiocytesandcalcium deposits indicative of myocardial injury(Figure 6C). Recovery of perfusion and functionat the periphery of the infarct zone was seen intwo of four IM and two of three IC studies thatcorrelated with anatomic findings of early orprominent neovascularisation.Thepresenceandsiteof the acutemyocardial infarction identifiedmicroscopicallycorrelatedwith the location ofaperfusiondefectontheex-vivo [99mTc]-Sestamibiheartslicesin5ofthe7sheep(Table3).
Discussion
The main aim of this study was to evaluatewhether standard nuclear medicine gammacameras, radiopharmaceuticals, software analys-es and reviewing workstations could be used toassess a large animal model of recovery frommyocardial infarction, in this case, after therapywithstemcellsdeliveredbyavarietyofroutesofadministration. After minor adjustments toaccountforthedifferentorientationoftheheartinthesheepascomparedtomanwehavefoundthat the sametechniques canbeemployed. ThisnowprovidesaplatformtostudyaspectsofMSCtherapythathavepreviouslyrequiredspecialisedsmall animal scanning equipment (e.g., for miceand rats), precluding many institutions such asourown.Ourexperiencessuggestthatthismodelcould be reproduced in many institutions withnuclear medicine departments, and thus wide-spreadexperiencewitharealisticmodelofacute
Table3.Visualcorrelationofthepresenceandlocationofaperfusionlossonthe[99mTc]-sestamibiheartslicesandscartissueontheanatomicalheartslices.
Sheep # [99mTc]-Sestamibi slices Anatomical slices Visual Correlation
3 Lateralwall;on3slicesLateralwallwhitescartissueonmatching3slices
Y
4 Latero-apicaldefect;on3slicesLatero-apicalpinkishvascularityonmatching3slices
Y
9Noperfusionabnormality;correlateswithMPIfinding
Lateralwallpinkishvascularityon2slices
N(smalldefectmicroscopically)
11Apicalperfusiondefecton4slicesonly
Apicalwhitescartissueon3slices;pinkishvascularityon3slices
Y
12Apico-septalperfusiondefecton4slices
Apico-septalwhitescartissueonmatching4slices
Y
16 NoperfusiondeficitidentifiedHeartslicesthickanduneven;cannotidentifyinfarct
N
18Largeapico-septalperfusiondefecton4slices
Largeapico-septalwhitescartissueonmatching3slices
Y

Bailey EA et al Molecular imaging for EGFR targeting
18 Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21.
myocardial infarction and response to therapycould be accelerated with many more centresparticipating. We used a SPECT/CT hybridscanner togive accurate scatterand attenuationcorrected SPECT images and such devices arenow ubiquitous in the practice of nuclearmedicine. The use of CT-based attenuationcorrectionisnowrecommended,andcommon,inmany nuclear medicine practices. Scattercorrection further improves the quality andaccuracyofthedata.
Animal models and imaging have been usedextensively to assess and trial new treatments,novel radiotracers and improved targetingtechniques prior to their use in humans. Whilesome animal models closely resemble theanatomical and physiological structure ofhumans,largedifferencesareoftenseenbetweensmalland large animalmodels. The similarity ofthe mouse to the humangenome is attractive toresearchersasitallowsforgeneticmanipulationsto be performed in the mouse that closelysimulate human disease (28), however,differences in cardiac size, anatomy andmolecularmachineryaresignificant,especiallyinlongitudinal imaging studies such as this one.Therefore, large animal models such as thecanine,porcineandovinespecieshavebeenusedto evaluate cardiac disease due to their closersimilarity to the human heart. Historically, thecanine model has been used to examine theeffects of chronic myocardial ischemia andmyocardial infarction on LV function, geometryandstructure(29).Whiledogshaveasignificantdegree of collateral circulation which make itdifficult to generate consistent myocardialinjuries(30),theporcineandovineheartexhibitscoronary artery supply and gross anatomicstructure similar to that of humans (31, 32). AquantitativestudybyWeaveret alevaluatedtheanatomy and distribution of porcine coronaryarteries in which they compared their findingswiththosereportedforcaninesandhumans(33).The existence of ‘scant coronary collaterals’ inpigswasreportedprimarily localizedtothemidmyocardiumandsub-endocardium.Studieshavealso shown that the ovine model of myocardialischemia does not exhibit significant collateralcoronary arteries with essentially separatecoronary circulations to the two ventricles (34).Bothareimportantadvantagesofthismodelforuse in metabolic and mechanical functionalstudiesofacuteMI(35).Coronaryarteryligationin sheep produces the pathological, haemodyna-mic and neurohormonal characteristics ofcompensated LV impairment secondary to MI.This is a reproducible model that reflects theclinical condition and therefore can be used toinvestigate the pathophysiology of early LV
dysfunction as well as experimental therapies(36).
ThesizeofthesheepheartissimilartoasmallfemalewithanEDVofapproximately80mlandanormalLVEFofgreaterthan50%,similartothatof a healthy human thus making it amenable toimagingwithcurrentSPECTgammacameras.Asa consequence of the small size, however,difficulties may arise in accurately tracking theendocardialand epicardialborderson the gatedMPIstudiesresultinginuncertaintiesintheLVEFvaluesobtained.Alternately,themeasurementofLVEFusinggatedheartpoolscanningwith99mTc-labelled erythrocytes (RBCs) in planar and/orSPECT modes is known to produce reliable andreproduciblemeasuresofLVfunctioninstandardclinicalpractice in man(37) that is less affectedbythespatialresolutionlimitationsofthegammacamera. The addition of this approach to theexisting study protocol should reduce errors inassessing LV function and will therefore beincludedaspartofthestandardimagingprotocolforanyfuturestudies.
Our experienced nuclear medicine physiciansfound no difficulties in interpreting the MPimagesderived.ThiswasconfirmedbyaКvalueof 0.89 indicating very good agreement. Totalagreementgivesascoreof1,with0indicatingnoagreement while negative values mean worsethan by chance. A К value between 0.81-1.0 issaidtorepresentverygoodagreement(38).
Apilotstudyenablestheinvestigatortotestaproofofconcept,withthebenefitbeing itsvalueinassessingthequalityofthedata,checkingthelogistics of the trial and enhancing reliability ofestimatesforuseinsamplesizecalculations.Thelogisticsoftestingsuchmethodologiesinhumantrials is complex and hard to undertake in acontrolled manner hence most are performedusing animal modelling. The results reportedfrom this pilot study have demonstrated thatstandard clinical imaging techniques andinvestigations used to assess myocardial injuryand response to therapy in man can be used inlarge animal models to test response to noveltreatments such as the use of stems cells formyocardialrepair.Thispilotstudyonlyincludedsmall numbers of animals in each treatmentgroup and therefore determining the mosteffective implantation method to improve bothperfusion and function following an induced MImay not be possible. However, these initialresults would suggest that both the IM and ICmethodscouldpotentiallybeusedforthistypeoftherapy, with the IM method in this pilot studyshowing an improvement in LV function andneovascularisation identified microscopically.Additionally, the experience gained with thesetechniques can be easily translated to human

Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 19
studies to assess therapeutic benefit in theclinicalsetting.
Conclusions
The anatomy and coronary arterial supply ofthe sheep heart is similar to the human heartwith very little collateral supply, and an infarctcanbereliablyandreproduciblyinducedmakingit an ideal model for testing therapeuticinterventions post-MI. The decision to study the‘functional consequences’ rather than directlylabeling the stem cells to study the fate of theMSCs in vivo was deliberate as this process hasproventobeareliableandreproduciblemethodofassessingresponsetotreatmentwhichcanbereadily translated to human studies. This pilotstudy has shown that techniques used in theclinical setting in man, which have been highlydeveloped and refined over many years andhundreds of thousands of investigations, can beused with large animals to follow theconsequences of stem cell and other therapies.Also, this study has shown that large animalmodelsaresuitableforassessmentwithstandardmyocardial perfusion imaging, radiopharmaceu-ticalsandprotocolswhichcouldsubsequentlybeapplied in human clinical trials to study theefficacy of stem cell therapy. As such, the sheepmodel and the nuclear medicine imaging andanalysis techniques used here have demonst-rated an excellent translational platform forbridging ‘mouse-bound’ pre-clinical studies andeventual clinical therapeutic use in humans.Further, both qualitative and semi-quantitativeanalysis can be applied to allow repeated non-invasivetemporalassessmentofextent,severity,defect size and LV function using standardcardiac analysis software and review packagesavailable in the majority of nuclear medicinedepartments.
Acknowledgments
TheauthorswishtothankDrIvanHoShonforhis assistance with the qualitative review of theMPIdataforthisstudy.Thisstudywasfundedbya grant from the North Shore Heart ResearchFoundation.
AppendixI
Calculation of the Kappa Statistic The possibility of agreement by chance alone
needs to be considered and this is done bycalculating the expected frequencies for eachseverityscorefromTable2asbelow:
(0)De�initelyNormal 263270/400=177.5
(1)ProbablyNormal 74/400=0.07
(2)Mild 4144/400=4.51
(3)Moderate 4943/400=5.27
(4)Severe 4039/400=3.9
Therefore, the total number of agreementsexpected by chance are 190.8, with theproportion of the total being 190.8/400 = 0.47.TheКisthen:
К =�.�����.��
�.���.��= 0.89
References
1. RasmussenTL,RaveendranG,ZhangJ,GarryDJ. Getting to the heart of myocardial stemcells and cell therapy. Circulation. 2011 Apr26;123(16):1771-9.
2. Fischer KM, Cottage CT, Wu W, Din S, GudeNA, Avitabile D, et al. Enhancement ofmyocardial regeneration through geneticengineering of cardiac progenitor cellsexpressing Pim-1 kinase. Circulation.2009;120(21):2077-87.
3. Schuleri KH, AmadoLC, BoyleAJ,Centola M,Saliaris AP, Gutman MR, et al. Earlyimprovementincardiactissueperfusiondueto mesenchymal stem cells. Am J PhysiolHeartCircPhysiol.2008;294(5)
4. GnecchiM,ZhangZ,NiA,DzauVJ.Paracrinemechanisms in adult stem cell signalingandtherapy.CircRes.2008;103(11):1204-19.
5. Abdel-Latif A, Bolli R, Tleyjeh IM, MontoriVM, Perin EC, HornungCA, et al. Adult bonemarrow-derived cells for cardiac repair: asystematic review and meta-analysis. ArchInternMed.2007;167(10):989-97.
6. JanssensS,DuboisC,BogaertJ,TheunissenK,DerooseC,DesmetW,etal.Autologousbonemarrow-derived stem-cell transfer inpatients with ST-segment elevationmyocardial infarction: double-blind,randomised controlled trial. Lancet.2006;367(9505):113-21.
7. Nelson TJ, Martinez-Fernandez A, Yamada S,Perez-Terzic C, Ikeda Y, Terzic A. Repair ofacute myocardial infarction by humanstemness factors induced pluripotent stemcells.Circulation.2009;120(5):408-16.
8. SmartN,Bollini S,DubeKN, Vieira JM,ZhouB,DavidsonS,etal.Denovocardiomyocytesfrom within the activated adult heart afterinjury.Nature.2011;2011(8).
9. SmartN,Bollini S,DubeKN, Vieira JM,ZhouB,DavidsonS,etal.Denovocardiomyocytes
Bailey EA et al Translation of Human MPI methods to a sheep AMI model
20 Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21.
from within the activated adult heart afterinjury.Nature.2011;474(7353):640-4.
10. DixonJA,SpinaleFG.Largeanimalmodelsofheartfailure:acriticallinkinthetranslationofbasicsciencetoclinicalpractice.CircHeartFail.2009;2(3):262-71.
11. ChinBB,NakamotoY,BulteJW,PittengerMF,WahlR,KraitchmanDL.111Inoxinelabelledmesenchymal stem cell SPECT afterintravenous administration in myocardialinfarction. Nucl Med Commun.2003;24(11):1149-54.
12. Zhang SJ, Wu JC. Comparison of imagingtechniques for tracking cardiac stem celltherapy.JNuclMed.2007;48(12):1916-9.
13. Nowak B, Weber C, Schober A, Zeiffer U,Liehn EA, von Hundelshausen P, et al.Indium-111 oxine labelling affects thecellular integrity of haematopoieticprogenitorcells.EurJNuclMedMolImaging.2007;34(5):715-21.
14. Bailey DL, Roach PJ, Bailey EA, Hewlett J,Keijzers R. Development of a cost-effectivemodular SPECT/CT scanner. Eur J Nucl MedMolImaging.2007;34(9):1415-26.
15. Gao J, Dennis JE, Muzic RF, Lundberg M,Caplan AI. The dynamic in vivo distributionof bone marrow-derived mesenchymal stemcells after infusion. Cells Tissues Organs.2001;169(1):12-20.
16. Kawamoto A, Tkebuchava T, Yamaguchi J,Nishimura H, Yoon YS, Milliken C, et al.Intramyocardial transplantation ofautologous endothelial progenitor cells fortherapeuticneovascularizationofmyocardialischemia.Circulation.2003;107(3):461-8.
17. Hudson HM, Larkin RS. Accelerated imagereconstruction using ordered subsets ofprojection data. IEEE Trans Med Imaging.1994;13(4):601-9.
18. BrownS,BaileyDL,WillowsonK,BaldockC.Investigation of the relationship betweenlinear attenuation coefficients and CTHounsfield units using radionuclides forSPECT. Appl Radiat Isot. 2008;66(9):1206-12.
19. Willowson K, Bailey DL, Baldock C.QuantitativeSPECTreconstructionusingCT-derived corrections. Phys Med Biol.2008;53(12):3099-112.
20. Germano G, Kavanagh PB, Waechter P,Areeda J, Van Kriekinge S, Sharir T, et al. Anew algorithm for the quantitation ofmyocardial perfusion SPECT. I: technicalprinciples and reproducibility. J Nucl Med.2000;41(4):712-9.
21. Ficaro EP, Lee BC, Kritzman JN, Corbett JR.Corridor4DM: the Michigan method for
quantitative nuclear cardiology. J NuclCardiol.2007;14(4):455-65.
22. Hansen CL, Goldstein RA, Akinboboye OO,BermanDS,Botvinick EH, ChurchwellKB, etal. Myocardialperfusionand function: singlephoton emission computed tomography. JNuclCardiol.2007;14(6):e39-60.
23. HesseB,TagilK,CuocoloA,AnagnostopoulosC, Bardies M, Bax J, et al. EANM/ESCprocedural guidelines for myocardialperfusionimaginginnuclearcardiology.EurJNuclMedMolImaging.2005;32(7):855-97.
24. Altman DG. Practical Statistics for MedicalResearch. First ed. TJ Press Ltd P, editor.Cornwall: Chapman & Hall, London; 19911991.611p.
25. Wollert KC, Meyer GP, Lotz J, Ringes-LichtenbergS,LippoltP,BreidenbachC,etal.Intracoronary autologous bone-marrow celltransfer after myocardial infarction: theBOOST randomised controlled clinical trial.Lancet.2004;364(9429):141-8.
26. AssmusB,SchachingerV,TeupeC,BrittenM,Lehmann R, Dobert N, et al. Transplantationof Progenitor Cells and RegenerationEnhancementinAcuteMyocardialInfarction(TOPCARE-AMI). Circulation.2002;106(24):3009-17.
27. AssmusB, Walter DH, Lehmann R, Honold J,Martin H, Dimmeler S, et al. Intracoronaryinfusionof progenitorcells is notassociatedwith aggravated restenosis development oratherosclerotic disease progression inpatients with acute myocardial infarction.EurHeartJ.2006;27(24):2989-95.
28. Rowland DJ, Cherry SR. Small-animalpreclinicalnuclearmedicineinstrumentationand methodology. Semin Nucl Med.2008;38(3):209-22.
29. ZhouR,ThomasDH,QiaoH,BalHS,ChoiSR,Alavi A, et al. In vivodetection of stemcellsgrafted in infarcted rat myocardium. J NuclMed.2005;46(5):816-22.
30. McDonaldKM, Francis GS, CarlylePF, HauerK, Matthews J, Hunter DW, et al.Hemodynamic,leftventricularstructuralandhormonal changes after discrete myocardialdamage in the dog. J Am Coll Cardiol.1992;19(2):460-7.
31. Yarbrough WM, Spinale FG. Large animalmodels of congestive heart failure: a criticalstep in translating basic observations intoclinical applications. J Nucl Cardiol.2003;10(1):77-86.
32. Poulsen RH, Botker HE, Rehling M.Postreperfusion myocardial technetium-99m-sestamibidefectcorrespondstoareaatrisk Experimental results from an ischemia-
Translation of Human MPI methods to a sheep AMI model Bailey EA et al
Asia Oceania J Nucl Med Biol. 2013; 1(2):10-21. 21
reperfusion porcine model. Nucl Med Biol.2011;38(6):819-25.
33. Weaver ME, Pantely GA, Bristow JD, LadleyHD.Aquantitativestudyoftheanatomyanddistributionof coronaryarteries in swine incomparison with other animals and man.CardiovascRes.1986;20(12):907-17.
34. Huang Y, Hunyor SN, Jiang L, Kawaguchi O,Shirota K, Ikeda Y, et al. Remodeling of thechronicseverelyfailingischemicsheepheartafter coronary microembolization:functional, energetic, structural, and cellularresponses. Am J Physiol Heart Circ Physiol.2004;286(6):H2141-50.
35. Markovitz LJ, Savage EB, Ratcliffe MB,Bavaria JE, Kreiner G, Iozzo RV, et al. Largeanimal model of left ventricular aneurysm.AnnThoracSurg.1989;48(6):838-45.
36. Rademaker MT, Cameron VA, Charles CJ,EspinerEA,NichollsMG,PembertonCJ,etal.Neurohormones in an ovine model ofcompensated postinfarction left ventriculardysfunction.AmJPhysiolHeartCircPhysiol.2000;278(3):H731-40.
37. Skrypniuk JV, Bailey D, Cosgriff PS, FlemingJS, Houston AS, Jarritt PH, et al. UK audit ofleft ventricular ejection fraction estimationfrom equilibrium ECG gated blood poolimages.NuclMedCommun.2005;26(3):205-15.
38. Landis JR, Koch GG. An application ofhierarchical kappa-type statistics in theassessment of majority agreement amongmultiple observers. Biometrics.1977;33(2):363-74.


















