Transforming Care at the Bedside across Wisconsin Monthly Webinar for February Reducing Hospital...
32
Transforming Care at the Bedside across Wisconsin Monthly Webinar for February Reducing Hospital Acquired Conditions Please mute or phone by using *6. Un-mute to speak by using *7 Please mute your computer speakers and call into the phone line
-
Upload
warren-ashley-fowler -
Category
Documents
-
view
216 -
download
0
Transcript of Transforming Care at the Bedside across Wisconsin Monthly Webinar for February Reducing Hospital...

Transforming Care at the Bedsideacross Wisconsin
Monthly Webinar for FebruaryReducing Hospital Acquired Conditions
Please mute or phone by using *6. Un-mute to speak by using *7Please mute your computer speakers and call into the phone line

Welcome to Today’s Call
2
Agnesian St. Agnes Aurora Burlington Aurora Lakeland Aurora Sinai Calumet Med Ctr Fort Health Care Froedtert Comm Mem: Ortho Medical
Froedtert Milwaukee Hayward Area Memorial Howard Young Med Ctr Mayo – Eau Claire Mayo – LaCrosse Mercy Janesville Wm S Middleton VA Midwest Ortho Spec H
The Richland Hospital Spooner Health System St. Croix Regional Med Ctr St. Elizabeth Hospital Tomah Memorial H Westfield’s Hospital Wheaton Fran - Franklin Zablocki VA Hospital
Please confirm your hospital is in attendance(if you miss roll call – please e-mail Stephanie by 4 pm)

Today’s Agenda1. Announcements
– Site Visit Update from Judy
2. Reducing/Preventing Hospital Acquired Conditions
3. 90 Day Challenge Slides (continued)
4. Wrapping up Cohort 2
3

Reducing / Preventing Hospital Acquired Conditions
Nationwide, for every 1,000 hospital patients admitted:• 49 patients experienced adverse drug events (accounting for
34.1% of HACs).• 40 patients developed pressure ulcers (27.8 %).• 27 patients developed some other hospital-acquired condition
(18.8 %).• 12 patients developed catheter-associated urinary tract infections
(8.4 %).• 8 patients fell while in the hospital (5.5%).• 3 patients developed surgical site infections (2.1%).• 3 patients experienced obstetric adverse events (1.7%).
Source: AHRQ National Quality Report

“Attacking” the HACs
5
TCAB Teams
You have the skills to apply systematic improvement to reduce or prevent any Hospital Acquired Condition….
6

Intend to continue?WHA is currently recruiting for Partners for
Patients initiatives
7
Adverse Drug Events Pressure Ulcers CAUTI OB Adverse Events Falls CLABSIReadmissions (including Med Rec)
Sepsis Surgical Site Infection
VTE Prevention Improving Pt. and Family Engagement/HCAHPS

8
“Active” Improvement Teams are the Key
Prioritize which HAC would benefit from an active teamTeams consist of front-line staff and unit leadersGather knowledge & evidenceGuide improvement Measure and Monitor the results

9
Learning while ImprovingMonthly Webinar format by topic for Active TeamsSame day and time each month, beginning in March One hour – recorded for later access
• 30 minutes of Data, Evidence, Best Practices & Presentations
• 30 minutes of “How to” instruction on applying systematic improvement
Teams will have 30-Day Action Items to select from to help adapt and adopt best practices

10
Webinars Alone ≠ ImprovementActive Teams have 4 Deliverables:1)Attend/view monthly webinar and complete action items2)Submit monthly outcome measure data3)Submit monthly process measure data4)Share progress, learnings, and best practices about implementing changes on webinars and discussions
Learning Resources
11
Monthly webinars reference the WHA Improvement Workbook
Tools and Templates are also available for download from the WHA Quality Center
12
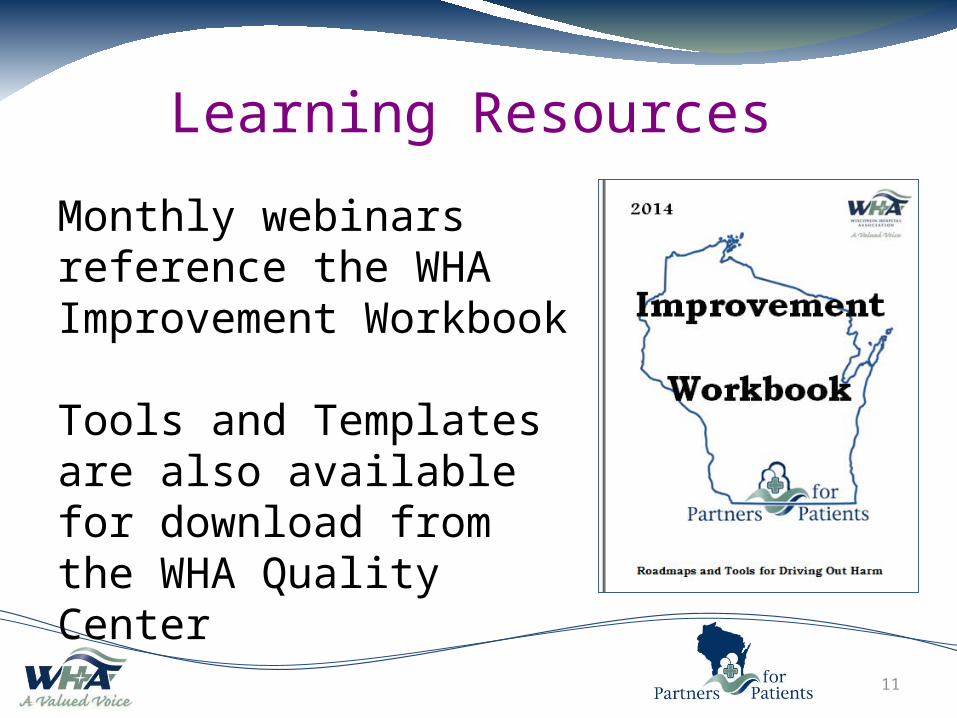
Initiative Day of Month Regular TimeADE Fourth Wednesday 12-1PMCAUTI First Wednesday 12-1PMCLABSI Dates will vary 10-11AMFALLS First Tuesday 2-3PMOB EED Second Thursday 1-2PMOB Harm Third Thursday 12-1PMIPFE/HCAHPS Second Wednesday 2-3PMPULC Second Tuesday 2-3PMREAD Third Tuesday 2-3PMSEPSIS Fourth Tuesday 2-3PMSSI Second Tuesday 10-11AMTCAB First Thursday 2-3:30PM
VTE Second Wednesday 12-1PM
Improvement Forum Fourth Thursday 12-1PM

90 Day Challenge Slides(Continued)
13
14
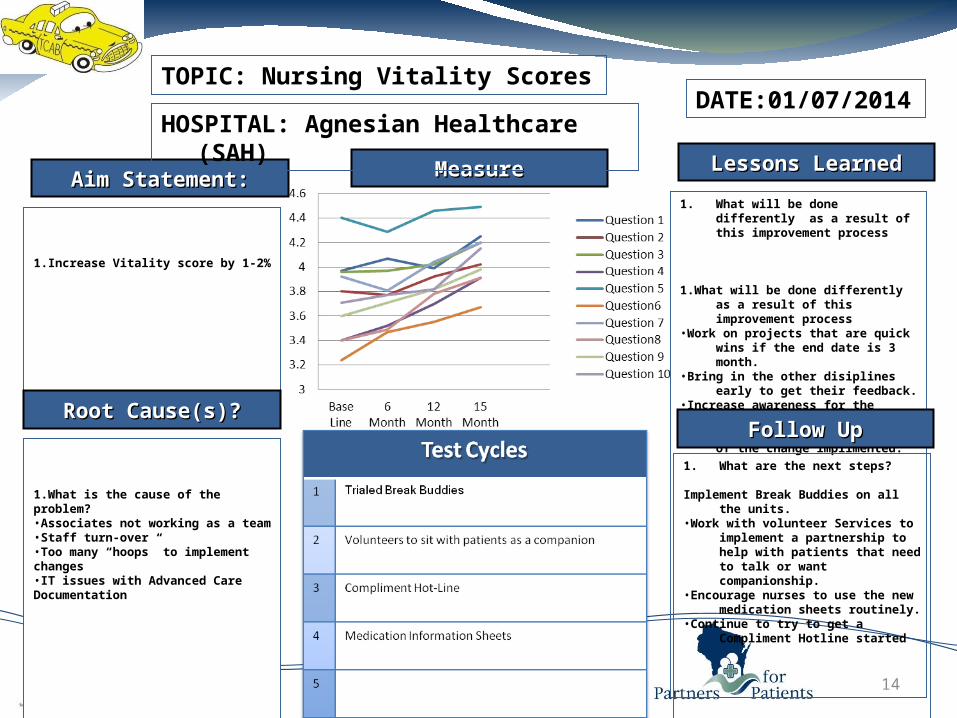
1.Increase Vitality score by 1-2%
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Nursing Vitality Scores
HOSPITAL: Agnesian Healthcare (SAH)DATE:01/07/2014
1. What will be done differently as a result of this improvement process
1.What will be done differently as a result
of this improvement process •Work on projects that are quick wins if
the end date is 3 month. •Bring in the other disiplines early to get
their feedback. •Increase awareness for the associates
working through the process. Often reminders of the change implimented.
Follow UpFollow Up
1. What are the next steps? Implement Break Buddies on all the
units. •Work with volunteer Services to
implement a partnership to help with patients that need to talk or want companionship.
•Encourage nurses to use the new medication sheets routinely.
•Continue to try to get a Compliment Hotline started
1.What is the cause of the problem? •Associates not working as a team •Staff turn-over •Too many “hoops” to implement changes •IT issues with Advanced Care Documentation
15
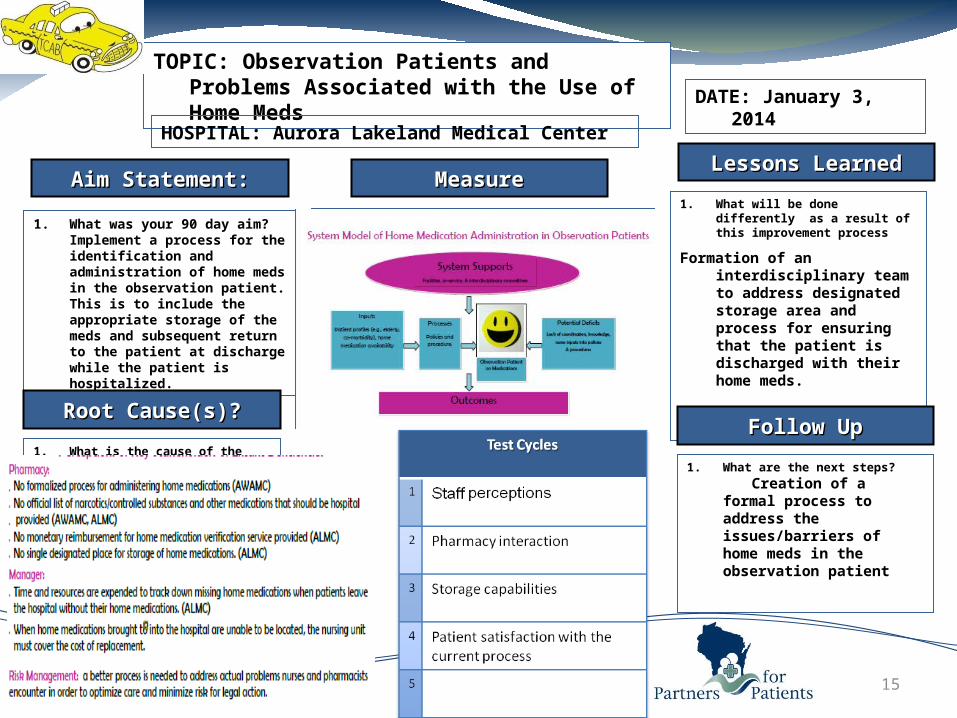
1. What was your 90 day aim? Implement a process for the identification and administration of home meds in the observation patient. This is to include the appropriate storage of the meds and subsequent return to the patient at discharge while the patient is hospitalized.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Observation Patients and Problems Associated with the Use of Home Meds
HOSPITAL: Aurora Lakeland Medical Center
DATE: January 3, 2014
1. What will be done differently as a result of this improvement process
Formation of an interdisciplinary team to address designated storage area and process for ensuring that the patient is discharged with their home meds.
Follow UpFollow Up
1. What are the next steps?
Creation of a formal process to address the issues/barriers of home meds in the observation patient
1. What is the cause of the problem?

16
1. Aim was to increase time at bedside to 60%.
2. Goal was met, 61% of RN’s time was spent at the bedside
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Increase Time at the Bedside
HOSPITAL: Aurora SinaiDATE: 12/28/2013
1.) Focus again on supplies and equipment. Are they available, in working condition and readily accessible.
2.) Need to continue to enforce real time charting in rooms.
3.) Need to work on bedside reporting at shift change. Some staff are willing to try it and adopt it, while others still are reluctant.
4.) Hourly rounding has been adopted and is working.
5.) Implement rounding with MD’s and nursing staff when rounding on patients.
1. Will repeat time study in one month and see if the inventions we have placed above will increase our time at the bedside to 65%.
Follow UpFollow Up
1.) Supplies and equipment issues
2.) Time management
3.) Poor shift to shift report/ transition
4.) Reluctance to change
5.) MD’s rounding on patients without nursing staff
Test CyclesTest Cycles
1.) Re-introduced Bedside reporting with RN’s and purposeful rounding -Staff willing to adapt and adopt2.) Hourly rounding -Adopted and working3.) Re-addressed supplies and equipment issue
0
10
20
30
40
50
60
70
Oct-12
J an-13
Apr-13
J ul-13 Oct-13
% at Bedside

17
1. By December 31, 2013, 75% of patients will answer yes to a question about participation in planning their care.
According to collected data, 100% of patients called feel involved in their plan of care since implementation.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Bedside Shift Reporting
HOSPITAL: Froedtert Health: CMH - MedDATE: 1/2/2014
1. Increased patient involvement in plan of care enhances overall patient satisfaction with nurse communication.
2. Identify barriers to bedside report prior to implementation. Ours was time, once this was decreased it was an easier transition.
3. You need a few dedicated staff to keep the ball rolling and people motivated to continue bedside report.
Follow UpFollow Up
1. Auditing compliance and use of bedside shift report
1. Patients felt separate from the care they were receiving. Care was done “to them” not “with them”.
2. Some important information was being missed on patients that were staying for long periods of time.
Pre TCAB Kardex Bedside
18
1. What was your 90 day aim?.
Our aim is to pilot a new process for implementing patient discharge teaching upon admission. It will be a detailed process followed by all staff on the unit.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
Patient Education Discharge Teaching
Milwaukee VA Medical Center01/08/2013
1. What will be done differently as a result of this improvement process
Discharge teaching will begin upon admission instead of the day of discharge. Also, there will be specified teaching topics individualized to each veteran based on their medical conditions and teaching needs.
Follow UpFollow Up
1. What are the next steps?
The next steps are to implement the pilot, obtain feedback from staff, and make adjustments based upon these recommendations prior to full implementation.
1. What is the cause of the problem?
Currently, there is no standardized process for determining discharge teaching needs or timeframes for completing discharge teaching.

19
1. What was your 90 day aim?.
Increase % of nurses who score 5/5 to the questions regarding communication between shifts and hand-off communication on the Team Vitality Survey.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
Percentage of 5/5 responses
Shift Change Patient Handoff
mo/yr Info. Exchange Info Exchange
10/12 32 24
03/13 25 5
10/13 25 15
(Will not have results of test until next survey)
TOPIC: Team Vitality
HOSPITAL: Spooner Health SystemDATE: 1/1/14
a) Staff will stop chatting and wait until the end of report for each patient to ask questions.
b) Staff will ask how well a patient is known thereby preventing leaving out pertinent information to new nurses
c)Recommend to expand use of whiteboards in patient room to communicate further info ie: fall risk, activity level, diet, etc.
d)Recommend use of white board for staff in report room.
Follow UpFollow Up1. What are the next steps?
a) Coach/teach staff to use SBAR during report.
b) Nursing Management to be approached regarding option of assignments, role of charge nurse, use of staff white board.
c) Continue to investigate pro’s/con’s of taped vs. verbal report.
1. What is the cause of the problem?
a) Hand off from ED to floor feels rushed, not enough time to ask questions.
b)Distraction is a large issue during report and at handoff., especially when sidebar conversations take place.
c)unable to find reporting RN in a timely manner to ask questions after listening to taped report.
d)Information is not always thorough during report.
e) Some staff give oral report and others tape report.

20
1. Increase bedside report compliance by 50% on all shifts through standardizing bedside report process
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
Place Run Chart or Graph here
TOPIC: Bedside Report
HOSPITAL: Mercy HospitalDATE: Jan 2014
1. Share testimonials from nurse to nurse about benefits of change process
2. Temperature check of unit and team prior to implementing change process
3. Encourage and praise
4. Share progress with other departments
Follow UpFollow Up
1. Continue temperature check
2. Onboarding of new staff
3. Problem solving and intervention
4. Remain open to improvements
1. Miscommunication
2. Lack of confidence
3. Fear of change in process
4. Misunderstanding of process
21
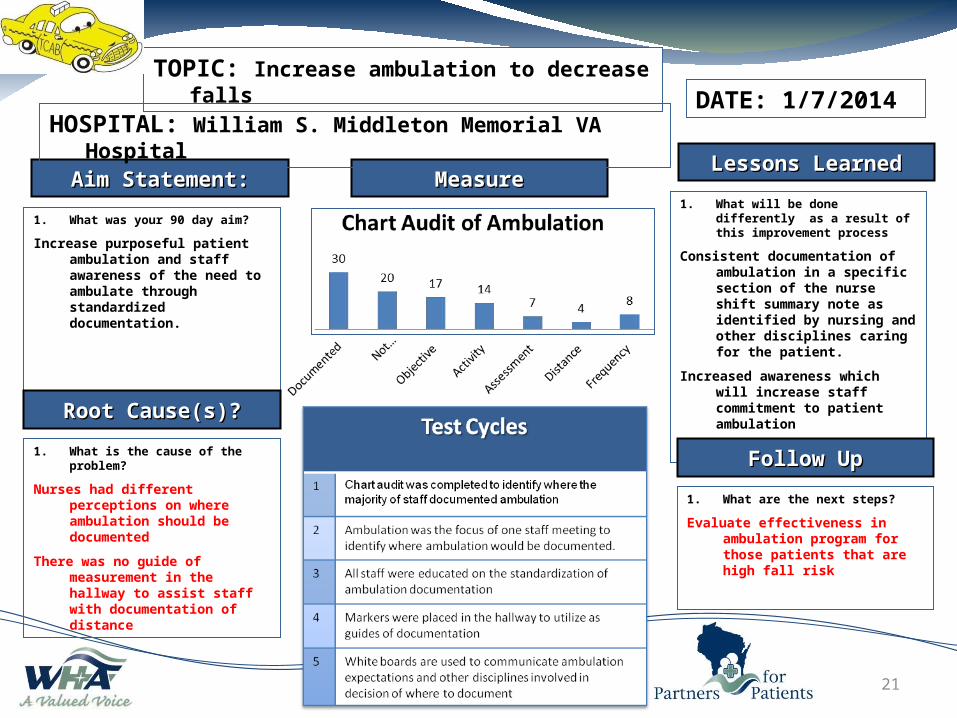
1. What was your 90 day aim?
Increase purposeful patient ambulation and staff awareness of the need to ambulate through standardized documentation.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Increase ambulation to decrease falls
HOSPITAL: William S. Middleton Memorial VA HospitalDATE: 1/7/2014
1. What will be done differently as a result of this improvement process
Consistent documentation of ambulation in a specific section of the nurse shift summary note as identified by nursing and other disciplines caring for the patient.
Increased awareness which will increase staff commitment to patient ambulation
Follow UpFollow Up
1. What are the next steps?
Evaluate effectiveness in ambulation program for those patients that are high fall risk
1. What is the cause of the problem?
Nurses had different perceptions on where ambulation should be documented
There was no guide of measurement in the hallway to assist staff with documentation of distance
No Lunch Punches by Pay Period
05
10152025303540
Pay Period
# of
No
Lunc
he P
unch
esRN
TC
UC
22
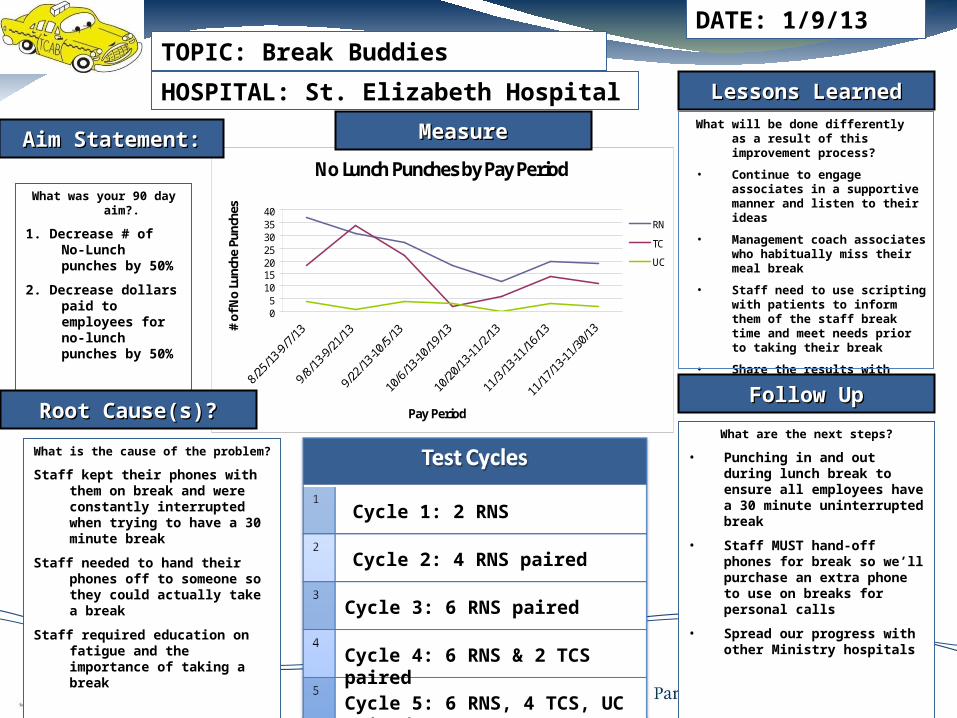
What was your 90 day aim?.
1. Decrease # of No-Lunch punches by 50%
2. Decrease dollars paid to employees for no-lunch punches by 50%
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Break Buddies
HOSPITAL: St. Elizabeth Hospital
DATE: 1/9/13
What will be done differently as a result of this improvement process?
• Continue to engage associates in a supportive manner and listen to their ideas
• Management coach associates who habitually miss their meal break
• Staff need to use scripting with patients to inform them of the staff break time and meet needs prior to taking their break
• Share the results with associates regularly to track progress
Follow UpFollow Up
What are the next steps?
• Punching in and out during lunch break to ensure all employees have a 30 minute uninterrupted break
• Staff MUST hand-off phones for break so we’ll purchase an extra phone to use on breaks for personal calls
• Spread our progress with other Ministry hospitals
What is the cause of the problem?
Staff kept their phones with them on break and were constantly interrupted when trying to have a 30 minute break
Staff needed to hand their phones off to someone so they could actually take a break
Staff required education on fatigue and the importance of taking a break
f
Cycle 1: 2 RNS
Cycle 2: 4 RNS paired
Cycle 3: 6 RNS paired
Cycle 4: 6 RNS & 2 TCS paired
Cycle 5: 6 RNS, 4 TCS, UC paired
23
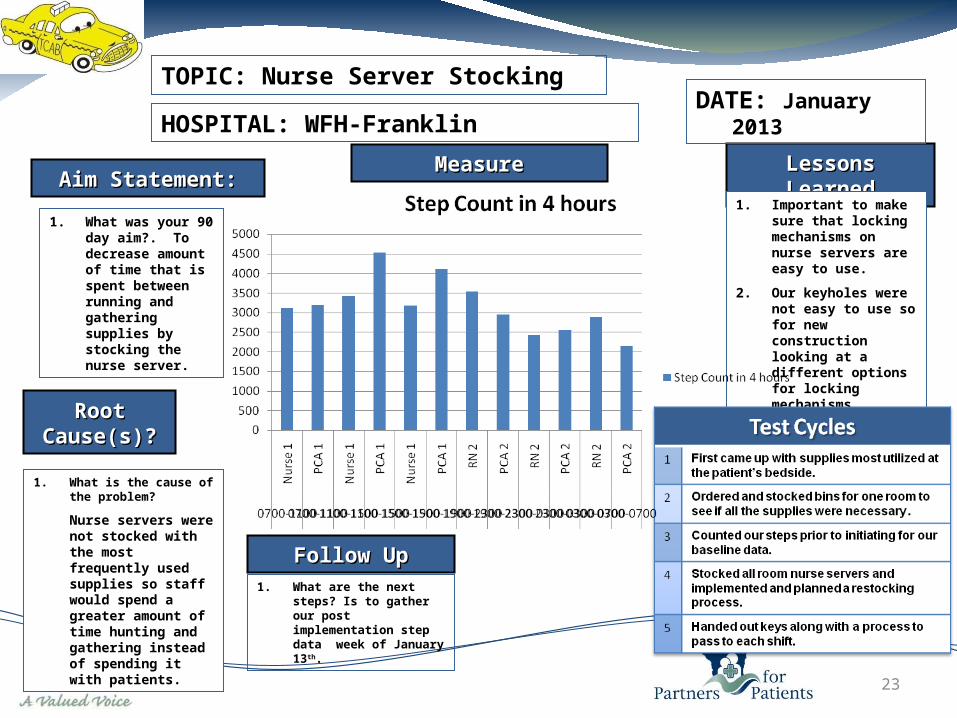
1. What was your 90 day aim?. To decrease amount of time that is spent between running and gathering supplies by stocking the nurse server.
Lessons LearnedLessons Learned
Root Root Cause(s)?Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Nurse Server Stocking
HOSPITAL: WFH-FranklinDATE: January 2013
1. Important to make sure that locking mechanisms on nurse servers are easy to use.
2. Our keyholes were not easy to use so for new construction looking at a different options for locking mechanisms.
Follow UpFollow Up1. What are the next steps?
Is to gather our post implementation step data week of January 13th.
1. What is the cause of the problem?
Nurse servers were not stocked with the most frequently used supplies so staff would spend a greater amount of time hunting and gathering instead of spending it with patients.

24
1. We will have no falls for 100 days.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
Place Run Chart or Graph here
TOPIC: Fall Prevention
HOSPITAL: Aurora Memorial Hospital - BurlingtonDATE: Jan 8
1. What will be done differently as a
result of this improvement process
There will be guidelines based on the Morse fall scale of 45 or greater that the beds will be set as follows.
Brake on, Bed plugged into nurse call system, side rails up, bed in low position, bed alert on and programed to zone two, ibed on. All alarms are programed into every staffs phone and if the alarm goes off everyone goes.
Fall tree on the unit with leaves placed with every day there is no falls, if a fall occurs all the leaves will come off. Follow UpFollow Up
1. What are the next steps?
Bed audits to ensure all the above criteria are met
No further falls for the 100 days we set for out goal.
1. What is the cause of the problem?
Increase in falls from July thru September that doubled our yearly fall total. Did not meet our goal of no falls with injury and to reduce falls my 50% from previous years total.

25
To improve and be consistent with medication education and documenting purpose of med in patient copy of med list at least by 50% in 90 days.
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
Manual audit of patient copy of med list at discharge to reflect purpose
HCAHPS: Understood the purpose of medication
TOPIC: Medication Education
HOSPITAL: Calumet Medical CenterDATE:11/1/13
1) Time consuming- needs to be done prior to discharge
2) Provider compliance is a challenge
3) Written info appreciated by patients
4) Pt education is easier and consistent with medication cheat sheet.
Follow UpFollow Up
1. Manual audit for med-purpose and reinforce
2. Work with providers to improve documentation
3. Encourage use of med-educ cheat sheet for consistency, validate on rounding with patient
1. Patient don’t always know their meds and its purpose – potentially impacting compliance.
2. Pt education is inconsistent and lacking ( purpose, side effects and when best to take)

26
1. What was your 90 day aim?
Increase patient satisfaction with discharge education as evidenced by an increase in HCHAPS scores by 12/31/13.flkasjflkdjflkjsdfkljf
Lessons LearnedLessons Learned
Root Cause(s)?Root Cause(s)?
MeasureMeasureAim Statement:Aim Statement:
TOPIC: Discharge teaching
HOSPITAL: Hayward Area Memorial HospitalDATE: 1/7/14
1. What will be done differently as a result of this improvement process?
A randomized audit of charts was done for the month of November and December to audit for documentation of “teach back” on discharge. This audit found nursing used teach back in 38% of the randomized chart review in November and 39% in December.
Nursing will be re-educated on the teach back method and the importance.
Follow UpFollow Up
1. What are the next steps?
To continue to audit the use of teach back and trend HCAHPS scores related to patient understanding of medications and discharge instructions.
Re-educate Nursing on “teach back” method.
1. What is the cause of the problem?
Nursing was instructing the patient on discharge, in regards to signs and symptoms and medications. However, the patient was not always understanding what was being taught. Therefore, when the patients returned home, the HCAHPS scores reflected that the patient did not feel that teaching was done to prepare them for self care at home.
Summarizing Lessons Learned from
the 90 Day Challenge
27

Wrapping Up Cohort 2
What we need from you: Complete data submission through March 30 Do last Time at the Bedside measurement Do last Team Vitality Report out on April webinar: what would you
do differently if you started TCAB now? Send a 3 question narrative summary
28

Cohort 2 Summary Narrative
1) What has been the most significant impact of TCAB on your unit?
2) What change or improvement has your unit adopted that you are most proud of?
3) What would you do differently if you started TCAB now?
29

Wrapping Up Cohort 2
What we will provide you: A final CNO Report Final write up of Cohort 2 Quarterly TCAB Spread Coaching Calls
May, August, November
30

31
Upcoming TopicsLeadership Staff becoming leaders among staffBest Practices in Leader Rounding
Mar
Spreading TCAB – A joint webinar with Cohort 3Staff participation and feedback with TCABEngagement of more staff in TCABTCAB to other units
April

Questions?
32