Ulster Grassland Society Environmental sustainability in Agriculture Challenges to 2030

T R A N S A C T I O N S O F T H E U L S T E R M E D I C A L S O C I E T Y .
SESSION 1879-80.
President--PROFESSOR DILL, M.D.
Hon. Secretary---WILLIA~I WHITLA, M.D.
Tuesday, January 13, 1880.
PROFESSOR DILL~ President, in the Chair.
Exhibition of Specimens.
DR. J. W. BROWNE showed a spongy exostosis which he removed from the ungual phalanx of the great toe of a healthy man who had suffered from it for two years the most distressing agony.
He exhibited a diseased larynx removed after death from a patient upon whom he had performed the operation of tracheotomy. He did not believe that the ulceration was syphilitic or tubercular. There was extensive congestion of one lung and a clot in the pulmonary artery.
He exhibited~ also, a bladder from a patient which he tapped per rectum. The case was a very interesting one. The patient was a subject of the h~emorrhagic diathesis. There had been a narrow stricture of the urethra~ and before he came under Dr. Browne's care an extensive false passage had been made, tunnelling through the prostate on the right side and entering the bladder ; from this opening blood was oozing~ but on account of the high pressure within, owing to the distended bladder, the bleeding was prevented~ and when he tapped for complete retention this pressure was removed~ and the consequence was the bladder filled with large clots of blood. He detailed how he attempted to get rid of these. He injected pepsine and dilute muriatic acid with a view of digesting and breaking up the clots~ as recommended by Dr. Foot, of the Meath Hospital. The man sank from ur~emic poisoning. A very interesting and unusual point in the case was, as the specimen showed~ the remarkable malposition of the ure ter - -one opened in the middle line at the apex of the trigone. His incision~ as they would see~ just per- forated the bladder in the right spot. He could not say how or by whom the false passage was formed.
He next showed a cyst~ semi-solid~ which had been removed from a pat ient ; and he gave the following history : - - T h e woman had been tapped twice outside hospital~ and the fluid collected rapidly. Finally she consented to have it removed; and he made the usual incision upon

Transactions of the Ulster Medical Society. 565
Sunday last, and found such universal adhesions and such thorough continuity of tissue as he had never seen before. He related all the difficulties as they presented themselves, and how he met them. The cyst which he showed was from the interior of the large one. He removed it to gain room, after taking away all the cyst wall possible and the fluid. He concluded the operation, which was performed under the spray, by putting in the usual sutures and a glass drainage tube designed by Keith ; and he here stated that this latter appliance he never would use again, as in removing the dressing next day he found that the glass flange had broken off, though fortunately the glass did not slip inside the abdomen. The patient did well for nearly twenty-four hours, when she suddenly commenced to sink, and died ve~ 7 soon, apparently from shock.
DR. BROWrCE next showed a beautiful specimen of compound commi- nuted fracture of the forearm, extending through the elbow, and showing the T-shAped fracture as described by the late Mr. Adams of Dublin. The limb required instant removal.
DR. WmTLA had examined the specimen of diseased larynx, and he quite agreed with Dr. Browne about its origin ; and he was firmly con- vinced of the fact omitted in nearly all the text books- - tha t true chronic inflammation of the larynx could and does often occur, ending in ulcera- tion, and having neither syphilitic nor tubercular origin. He described the character of the ulceration met with in ordinary chronic bronchitis of long standing causing death, and he believed it was precisely the same state of matters in the larynx. He could recall, in his short experience, three cases where neither a tubercular nor a syphilitic nor a cancerous origin existed. He had tapped the ovarian patient outside hospital, and seen her tapped in the hospital, and he had examined the inner cyst then, and failed to get from it any fluid by inserting the trocar further in. I t was, however, evident what it was through the relaxed abdominal walls.
DR. W~BELER commented upon the interest of the specimens exhibited by Dr. Browne. He thought Dr. Browne could not possibly have done anything else than operate in the ovarian case. I f a man only selected such cases as must succeed, and avoided all doubtful ones, his power for good was very limited.
DR. WITH~l~S detailed a case where two exploratory operations had been made and the patient recovered, the capital operation being aban- doned.
DR. KEvI• detailed a very interesting case bearing upon the bladder specimen, where the organ was tapped three times in twenty-four hours.
DR. O'NEILn spoke of the careful and dexterous way in which he wit- nessed the ovariotomy performed by Dr. Browne. The adhesions could not have been previously foreseen.
PROFESSOR DILL commented upon the care required in the selection of

566 Transactions of the Ulster Medical Society.
cases of ovarian disease before operation~ strongly recommending the exploratory tapping before operating as the best guide to diagnosis. He pointed out the great advantage in operating at the Throne Hospital and not in the Royal.
Tuesday, Pebruary 9, 1880.
PaOFESSOR DILL, President, in the Chair.
Remarks on Colles' Fracture and its Treatment with Professor Gordon's Splint. By HENRX 0'NEILL~ M.D, M.Ch. ; Assistant Surgeon, Belfast Royal Hospital.
FaACTURES at the lower end of the radius are of great practical import- ance~ from their frequency and the evil consequences arising from the common methods of treatment still recommended in most surgical works. There are two chief forms. The first form is usually called Colles' Frac- ture, so named from having been accurately described by Dr. Colles, Dublin~ in The Edinburgh Medical and Surgical Journal for 1814, Vol. X., pp. 182-186, and is usually caused by a fall on the palm of the hand, with a simultaneous forcible extension backwards of the hand. The second form is produced by a fall on the back of the hand with the wrist flexed. The latter form is very rare, so I shall confine my remarks to the first variety.
Causes.--It is usually caused by falling on the palm of the hand, with the wrist violently extended ; the anterior common ligaments and flexor tendons being forcibly stretched, act on the anterior border of the carpal surface of the radius at right angles to its long axis, forcing it backwards so that the radius breaks almost transversely, or with a variable degree of obliquity from before backwards and upwards.
Signs and Symptoms.--1. Swelling over the posterior surface of the wrist, extending upwards on the forearm for about 1~- inches, as the natural hollow over the wrist-joint behind is obliterated, and seems to be transferred to 1 inch or 1~ inches upwards on the forearm. This is caused by the lower end of the lower fragment being displaced back- wards with the carpus and metacarpus, and the tonicity of the muscles displaces the lower fragment outwards. This deformity disappears when moderate extension is made; and returns immediately when the extending force is withdrawn, as fo~vnerly described by Dr. Colles himself.
2. Swelling at the lower end of the radius in front, beginning close above the wrist joint and extending upwards from 1 to 2 inches on the anterior surface, the natural concavity of the radius at this part being replaced by a prominence.
3. The lower end of the styloid process of the radius is directed

Transactions of the Ulster Medical Society. 567
towards the base of the metacarpal bone of the index finger~ instead of being in a line with the metacarpal bone of the thumb, as in the normal condition.
4. Acute pain along the seat of fracture in front and behind and over the lower end of the ulna. The pain over the ulna is longest of being recovered from.
5. Inability to pronate or supinate the hand because of the severe pain caused by the attempt to do it ; therefore the patient keeps the hand mid- way between pronation and supination, at the same time supporting the forearm across the chest with the sound hand.
6. By firmly grasping the lower end of the radius close to the carpal border by one hand~ and at a point two or three inches upwards on the radius by the other hand, and making moderate extension with backward and forward movement, distinct mobility with occasional crepitus are felt between these points. This sign is conclusive evidence that a frac- ture exists.
The line of fracture in this accident is described as transverse from before backwards by Smith (-' On Fractures in the vicinity of Joints," page 165~ Dublin, 1847), Holmes (" Principles and Practice of Surgery," page 247~ 2nd edition), and Packard (American Journal of Medical Science, January, 1879, page 124); but Professor Gordon, Belfast, who has carefully studied this subject~ states " that of 27 specimens of this frac- ture in the Belfast Queen's College Museum 19 are oblique from before backwards and upwards, and 8 are directly transverse" (" On Fractures of lower end of Radius," page 4; Gordon, 1875).
In the recent forms of this fracture, produced artificially~ the line of fracture is oblique from before backwards and upwards, and from within outwards and upwards, extending in front �88 of an inch above the carpal border~ and behind from s a to 13 of an inch above the carpal border. The lower end of the upper fragment is found to be convex from before backwards and upwards~ and from within outwards and upwards, and the upper end of the lower fragment is concave in these directions.
Mons. Voillemier (" Archives Gdn~rales de M6decine, Mars, 1842) maintains that all fractures of the lower end of the radius (that is, within an inch of its carpal surface) are examples of impacted fracture~ and considers that impaction of the upper into the lower fragment prevents crepitus from being detected in this form of fracture. ~dlaton agrees with him in this view (" ]~ldments de l~athologie Chirurgicale," tome I., page 742). Smith (" On Fractures in the vicinity of Joints~" pages 159, 160) denies that impaction does occur, and remarks that "unt i l the result of the examination of recent specimens can be adduced in support of the theory of impaction I shall be inclined to believe that the impaction is only apparent, and that the compact tissue of the shaft is not found enveloped in bone~ from its having penetrated the lower fragment at the

568 Transactions o f tile Ulster 2~[edieal Society.
time of the occurrence of the injury~ but because it becomes subsequently incased in osseous matter during the process by which the bony union of the fracture is accomplished."
Professor Gordon, in 18757 and his pupils since then, produced this fracture artiflcially~ in the dissecting rooms of the Queen's College, Belfast~ by forcibly extending the hand; and now the more important varieties of this fracture have been represented by artificial ones. On careful dissection of these fractures produced artificially the line of frac- ture begins~ as a rule r from �88 of an inch above the carpal border of the radius in front, and passes from within outwards and upwards, and from before backwards and upwards~ for about an inch ; the upper fragment being convex and the lower concave in these directionswviz., from within outwards and upwards~ and from before backwards and upwards. In none of these specimens was impaction observed--in fact, it will be easily understood that no impaction can take place in this form of fractur% as its direction is oblique in the directions before mentioned, and because the force which produces this accident acts at right angles to the longi- tudinal axis of the radius~ and rotates the lower fragment upwards and backwards on the lower end of the upper fragment.
Treatment.--Extend the wrist-joint, then apply Gordon's spl int--by placing the bevelled portion of the anterior part of the splint a little above the lower end of the upper fi'agment--to fix it; now flex the wrist to an angle of 45 ~ and apply the posterior part of the splint to press forwards, and retain the lower fragment in that position. The splints must be well padded with spongiopitin% flannel~ tow~ or other soft material. Place a thick elongated pad of tow (about 1 inch • �89 • �89 against the outer border of the carpus longitudinally~ pass a narrow strap through the ulnar part of the splint and over this pad~ so as to press the carpus inwards towards the ulna. Fasten the splints by two more straps--one over the splints close to the lower end~ and the other over the splints close to the upper end. Secure all by a bandage extending from the fingers to the elbow. Should severe inflammatory swelling of the hand occur during the first twenty-four hours~ I remove the posterior part of the splint and readjust the padding. This may be repeated once weekly to watch the progress of the cas% and any displacement of the fragments should it arise. In patients under fourteen years of age three weeks will be sufficient time to allow the splints to remain on ; above fourteen )'ears four or five weeks will be required. After removing the splints entirely envelope the hand and forearm in cotton wool~ and lightly bandage for two or three weeks. See that the fingers are kept frequently moved from the second week after the accident to prevent prolonged stiffness~ which may occur if this point is not attended to.
I have*treated more than 150 cases in the Belfast Royal Hospital by applying Gordon's splint in tho method above described, and~ with few

Transactions of tI~e Ulster Medical Society. 569
exceptions~ have found that the patients soon regained the perfect use of the forearm and hand. Several patients, especially those over fifty years of age, suffered from pain of a rheumatic character along the line of fracture in cold weather, but this was easily remedied by applying cotton wool and a bandage for a longer time after the splint was removed than in younger patients.
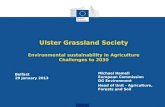
The accompanying diagram represents Gordon's splint accurately applied for the treatment of Colles' fracture.
PROFESSOR GORDO~, after the paper was read, made the following observations : - - T h e first thing to be determined i s - - W h a t is Colles' f racture? I would define it as the usual fracture of the lower end of the radius, caused by falling on the palm of the hand, and very rarely extending above an inch from its lower end. In such cases, if the splint be properly applied, the lower end of the radius will be so perfectly restored that it will be difficult to say after five or six weeks which radius was fractured. I f the radius be broken from an inch and a quarter to an inch and a half above the lower end, then both fragments are usually displaced inwards, diminishing the interosseous space. In such cases the splint will fail in correcting the displacements inwards, especially of the upper fragments, as it is held in this position by the extensor muscles of the thumb ; but I do not know of any more efficient splint for the treatment of this variety of fracture. Indeed the question has often forced itself upon me as to the necessity of limitation of Colles' fracture, so as to give it a precise meaning, and draw the distinction between fractures of the lower end of the shaft of the radius and Colles' fracture. I f the fracture be in the lower inch of the radius, and the term Colles' fracture be restricted to that inch, then the treatment of i t will be found most satisfactory by my splint ; but if the fracture be a little higher up, then a slight diminution of the interosseous space and transverse breadth of the forearm will occur, which neither the radial splint nor any other mode of treatment with which I am acquainted will correct. As to the age at which i t occurs, I have seen it in persons from five to twenty-three years of age, and from twenty-five to thirty-five years it becomes very rare ; and after fifty years, when senile atrophy begins to manifest itself~ i t becomes very f requent- -so that even the slightest force may produce

570 "l;'ansactions of the Ulste~ Medical Society.
it. As to the palmar swelling, it is mainly inflammatory, and is caused by the lower end of the upper fragment starting forwards and wounding the soft parts in front. By pressing the upper fragment backwards and the lower forwards, the apposition becomes perfect, all stimulus to inflammatory action is removed, and in many cases there is no swelling of the fingers nor tingling sensation, which was, before the introduction of my splint, considered a necessary accompaniment of Colles' fracture.
And as to the doctrine of impaction in this accident, all I can say on the subject is this-- that I have seen and carefully examined several hundreds of the specimens of the artificial fracture, and in none, either produced by myself or by others, was there the slightest appearance of impaction--as the force exerted on the anterior border of the carpal surface, as stated by Dr. O'Neill, drives the lower fragment backwards, whilst the lower end of the upper fragment, being in projectile force by the weight of the body, is forced forwards against and into the flexor muscles, and, therefore, I regard impaction almost as a mechanical impossibility; but as regards that form of fracture produced by failing on the back of the wrist, as referred to in the paper just read, I regard it as a truly impacted fracture, of which I have two admirable specimens in the Queen's College Museum.
DR. JOHN WALES did not think that the successful treatment of Colles' fracture was by any means confined to the use of the "Gordon splint."
Da. WALES (senior) thought there could be little doubt as to the great value of the Gordon splint in the treatment of Colles' fracture, as defined by Professor Gordon, if correctly applied. We see, however, even amongst well-informed surgeons, considerable difference in its mode of application. For example, it is frequently applied so as to make lateral pressure on the upper fragment of the radius, near the seat of the fracture, the result of which must be to aid the pronators in diminishing the interosseous space-- thus creating a deformity which he had frequently seen as a sequence of this fracture. He thought, therefore, that the principles enunciated by Professor Gordon, rather than his splints, commend themselves mos t - - for attention to the former will enable any intelligent surgeon to construct, out of materials at hand, an appliance which will produce satisfactory results, where such can be produced, by the Gordon splint. But this is not always the case, even with the latter. A suitable pad on the anterior aspect of the upper fragment, immediately above, but not on, the llne of fracture ; a pad on the end and posterior aspect of the lower fragment and carpus, secured by two plain splints--leaving the hand well flexed and the fingers free, to prevent stiffness from adhesions--would, he believed, meet all requirements in a simple manner.
DR. FAGAN approved of Ndlaton's method of treatment instead of Professor Gordon's. He had not much experience of the practical application of the splints, and though he spoke more theoretically than

~'ansactions of the Ulster Medical Society. 571
praetically~ he had given the matter some thought~ and he must say he failed entirely to see the intention of the bevelled portion of the splint ; nor could he see why the accident could not be as well treated by a piece of straight and fiat wood properly padded. While he could see no use in this part of the splint~ he thought that its convexity would be sure to produce some lessening of the interosseous space. From an anatomical study of the subject there was no necessity for it. He Could not see how it would keep the radius and ulna from approaching each other~ as was contended by those who advocated its use.
DR. A. iVI~CoNNELI, said he had considerable experience of Gordon's splint, and used it in all cases to which it was applicable. I ts advantages are very evident in cases which have been neglected from two to three weeks. I t is easily applied, retains its position without troubl% and effectually corrects any deformity. The splint is a great boon to the practical surgeon, and we owe a deep debt of gratitude to Dr. Gordon for his invention.
DR. WHITL& said he would refer to a point which was overlooked in the discussionwviz.~ the latest period in which one was justified in treating a fracture by the Gordon splint. He had applied it in one case where the accident was of four weeks' standing~ in another of three and a half, and in several where the bones had been more than a fortnight f rac tu red- -a l l with great benefit. He thought there could hardly be a l imit put to the time, as the splint, properly applied~ would restore the natural condition of the parts so perfectly that~ even if firm osseous union had taken place, great good would follow its use~ as the alteration in the direction of the articular surfaces would be prevented even after a very long time. As regarded the use of the bevelled portion of tile splint~ he thought that there was hardly room for a difference of opinion when anyone looked at the beautiful natural antero-posterior curve in the perfect bone which he held in his hand. In case of fracture this con- cavity in the radius was almost always changed into a convexity. The inventor of the splint had early seen and recognised the vast importance of restoring this concavity, and he made the bevelled portion of his splint the keystone of his arch~ and with consummate skill succeeded with the simplest contrivance to remedy a deformity that had previously baffled every surgeon. He had used~ or seen the splints used in, he believed, over 200 cases~ and in no instance where it was applied properly, had he seen any but highly satisfactory results follow; and he believed he was perfectly correct in saying that in nine cases out of ten no proof of fracture could now be detected upon the most critical exami- nation.
DR. WORKMAN understood Dr. Fagan to speak of the bevelled portion of Dr. Gordon's radial splint as being used to make and keep up a lateral ~eparation between the radius and ulna. Dr. Workman had always been

572 Transactions of the Ulster Medical Society.
taught by Dr. Gordon that the bevelled portion was not intended for, nor was it capable of performing~ such a duty~ but was intended to keep the upper fragment of the radius in a plane posterior to that of the ulna ; and he knew of no p]an of padding which would be at all so effectual as the radial splint. Dr. Workman considered it unnecessary~ as a rule~ to place the little pad which Dr. O'Neill recommended on the outer side of the carpns~ under the carpal strap, but wished to call attention to the advantage of placing a very thick~ small pad on the back of the carpus. A pad so placed would keep the carpus with the lower fragment of the radius well forward~ and this carpal strap, passing from the back splint to the prominent base of the metacarpal bone of the thumb, would exer- cise no injurious pressure on the veins. From his experience be had found it better~ as a rule~ not to keep the splint on for more than about four weeks, for in several cases where the splints had been left on for about six weeks~ on removing them he found that~ although there was no deformity~ the fingers and wrist were very stiff--apparently from the hand being kept in one position for such a length of t ime--so much so that it was many weeks before the hand had perfectly resumed its functions. Dr. Workman thought that spongiopiline or felt was the best substance for padding the splint~ but in hospital he was in the habit of using tow~ only on account of its cheapness~ and had found it to work admirably.
The PRESIDENT said :---I believe I am warranted in the statement~ and I think I reflect the minds of the members~ when I say that a more important practical and useful paper has not been brought before the Society for a long time than ' th is on% to which we have been listening with so much attention~ by Dr. O'Neill~ on Colles' fracture and the Gordon splint~ and which has been so ably supplemented, and minutely and clearly demonstrated, by Professor Gordon. I have had a lengthened and ample experience in the use of this splint~ and I may say that its value cannot be exaggerated~ neither can we bestow too much praise upon its admirable adaptation to the wrist and forearm, the great comfort experienced by the patient~ and the very satisfactory results which have been found to follow from its proper application. I am free to state that, before this instrument was designed and came into use, I always experienced a want or a deficiency in the treatment of those cases of Colles' fracture which came under my care, as there was a greater or lesser degree of deformity following in each case ; but I have invariably found the results to be most satisfactory since I began the use of it. When I first saw and carefully examined for myself the Gordon splint~ it at once commended itself to my mind and judgment as a mechanical contrivance which was admirably suited to the object for which it was designeff; and I cannot imagine anyone possessed of a mechanical mind or genius but who must see and acknowledge its undoubted merits.

Traltsactions o f the Ulster Medical Society. 573
And yet, with all this, I regret to say that, from what I have both seen and heard, there are those in the profession, far and near, who, as has been stated, require still to be educated into the use and proper applica- tion of this instrument. To prove this I shall offer you one or two instances. The first is that of a lady who came to me from a little distance. She had her arm in a sling~ had on it the Gordon splint, and she was suffering much pain. I found, upon examination, she had received a Colles' fracture, and that the splint was actually alSplied upside down. No wonder~ indeed~ that she suffered so much. I need not say I altered the splint, and adjusted i t so as to afford her much ease, and the case did well. The next case was told me by one of our young graduates (a Belfast student) who, while visiting a metropolitan school, dropped into a lecture-hall. The subject of clinique was Colles' fracture, and, after exhibiting the "Gordon splint," the lecturer proceeded to show how it should be applied. The young graduate could scarcely preserve his countenance when he saw it being applied in the wrong way, or upside down. He took the liberty of introducing himself afterwards to the lecturer~ and correcting the error which to a Belfast man was a palpable blunder. As a few of the members are not agreed upon what constitutes a proper padding between the splint and the wr i s t and forearm, I may say that I have often applied it without any padding whatever~ and when it is made to fit in size and shap% I have seen it to suit the purpose admirably. But before using it in this way I have found it necessary to round off the anterior sharp edge. This I would venture to suggest to Professor Gordon as an improvement under any circumstances. Allow me to conclude by saying that, if, as I assume it to be a test of genius to supply an admittedly great want by producing an original and very appropriate mechanical contrivance, and which has been furnished to us in the invention of this admirable work then, l" ~nbmit, to Professor Gordon, the author of this very valuable surgical appliance, the "Gordon splint~" must be accorded the honour of being an inventive genius.
PRIAPISIK IN I ,EUC~EMIA.
SALZ~.R relates the case of a saddler, forty-six years of age, suffering from leucmmia, probably of splenic origin. Without apparent cause he became subject to p r iap i sm--a t first only of short duration, but which afterwards became persistent for six weeks. I t was then followed by the opposite condition, one of absolute impotence. Analogous cases of pro- longed priapism are to be found in medical literature.--.Berl, klin. Woch., No. 11.
K . F .


















