Tracheoesophageal fistula
14
TRACHEOESOPHAGEAL FISTULA & ESOPHAGEAL ATRESIA Dr. Ravi Shankar Sharma 2 nd year resident, Dept. of Anaesthesia S.S.M.C. & S.G.M.H,Rewa
-
Upload
ravishankar-sharma -
Category
Health & Medicine
-
view
179 -
download
4
Transcript of Tracheoesophageal fistula

TRACHEOESOPHAGEAL
FISTULA & ESOPHAGEAL
ATRESIA
Dr. Ravi Shankar
Sharma
2nd year resident,
Dept. of Anaesthesia
S.S.M.C. &
S.G.M.H,Rewa

HISTORY
1 day old male
Baby of Uma Kol
Resident of Chandariya, Rewa
Date of Birth- 12/02/2015
Date of Admission- 13/02/2015
Ward-Nicu,GMH
Presenting complaint:Excessive salivation & vomiting(H/o Milk aspiration)
HISTORY OF PRESENT ILLNESS
Parents of patient first noticed excessive salivation with violent coughing leading to vomiting, 6-8 hr after birth of child (immediately after brest feeding)
Onset –acute,Duration-1day
1st feeding was normal, later feeding lead to regurgitation , choking and bluish discolourationof body with excessive frothy salivation
Symptoms aggravated on feeding ,no relieving factor
Not assosiated with any other features
Later pt, breathing became laboured and
child started struggling for breaths
Was not able to feed at all

MATERNAL HISTORY(PAST HISTORY & ANC PERIOD)
G2P2L3A0
UNBooked case/no Ante natal visits/received
1T.T.only
No h/o OCP’s(estrogen/progesterone) for long time
No H/o maternal infectons(VDRL-ve,HbsAg-ve)
NO H/o Gestational D.M./Thyroid abn./PIH
NO H/o Polyhydramnios(normal amniotic fluid
volume)
All previous pregnancies were normal(none of
children had any congenital abnormalities)
MATERNAL HISTORY (DURING LABOUR)
FTNVD with vertex presentation
Twin pregnancy(Attended by Doctor)
No H/o foul smelling dischage/leaking p/v
/uterine tenderness/PPH
Amniotic fluid –clear
Labour –spontaneous & uneventfull
Cry-immediately after birth(no ventillation
was required )
Breast Fed-3 hrs after birth
GENERAL PHYSICAL EXAMINATION
Pt. was alert , conscious, normal cry
Colour-Pink
Tone-Active
No H/o apnoea , Grunting , Chest indrawing
Absence of Jaundice/Bleeding/Bulging anteror
fontanel
Absence of meconium stained cord, skin pustules
Temperature-Afebrile
RR-47/min ,HR-137/min.
Spo2-93%, Weight-3kg

SYSTEMIC EXAMINATION
Respiratory examination:-
• B/l equal air entry
• Chest movements were symmetrical
• No added sounds
Cardiovascular examination:-
s1, s2 normal.
No murmur,
No abnormality detected
Per Abdomen:-
• Soft/Non tender/Non distended
Central nervous examination:-
• Conscious , Motor function – muscle tone, power and DTR within normal limits
• Sensory function within normal limits

AIRWAY EXAMINATION
Chin-Normal sized(No anatomical
abnormality)
Mouth opening-adequate
Previous intubationattepts-Easy
Uvula-visible
No difficulty in Flexion & Extension

INVESTIGATIONS:-
• Hb-20.4 gm%
• TLC-7400 cells/cumm(P-76,L-17,M-4,E-3,B-
0)
• R.B.C-5.3millions/cumm
• MCV-110fl, MCH-39.7pg,MCHC-35.8g/dl
• Platelet-1.9lac.
• C.R.P-Non reactive
• Blood group-o+ve
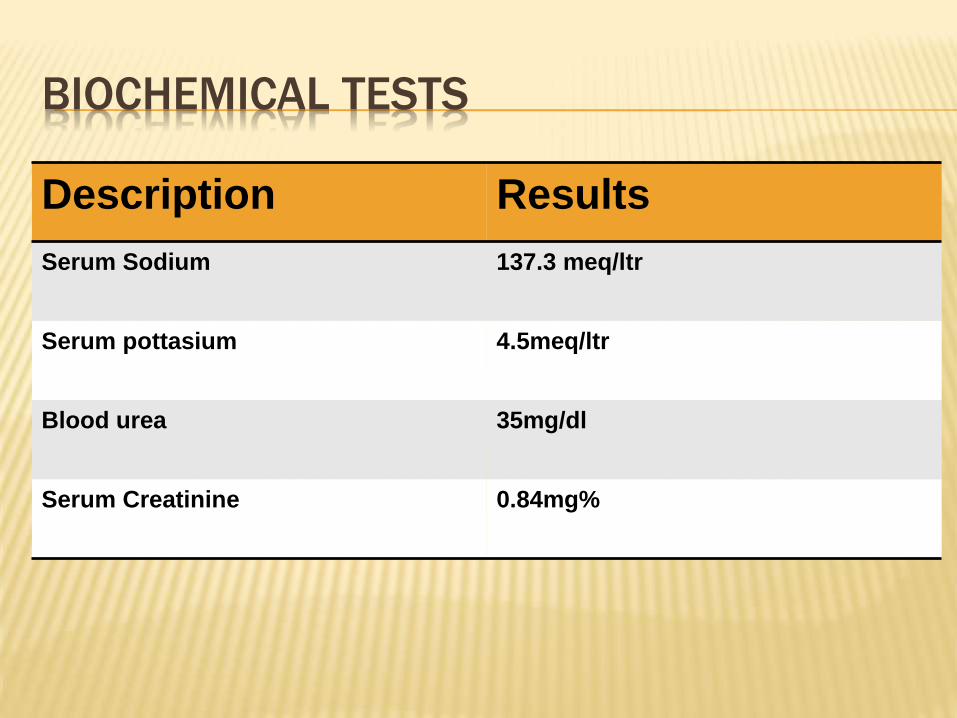
BIOCHEMICAL TESTS
Description Results
Serum Sodium 137.3 meq/ltr
Serum pottasium 4.5meq/ltr
Blood urea 35mg/dl
Serum Creatinine 0.84mg%

X-RAY:-

SUMMARY:-
A new born male child was admitted to NICU,
with chief complaints of excessive drooling of
saliva & vomiting after brest
feeding.NGT/OGT was tried to introduce in
order to stop further regurgitaion but it failed.
Finally X-Ray(Dye study )was carried out and
Provisional diagnosis of Esophageal atresia
& tracheoesophageal fistula was made by
Paediatric Surgeon