
Toxicology Req 6-14 Final - Genesis · 2020-01-28 · klonopin lorazepam lorcet lyrica meperidine...
2
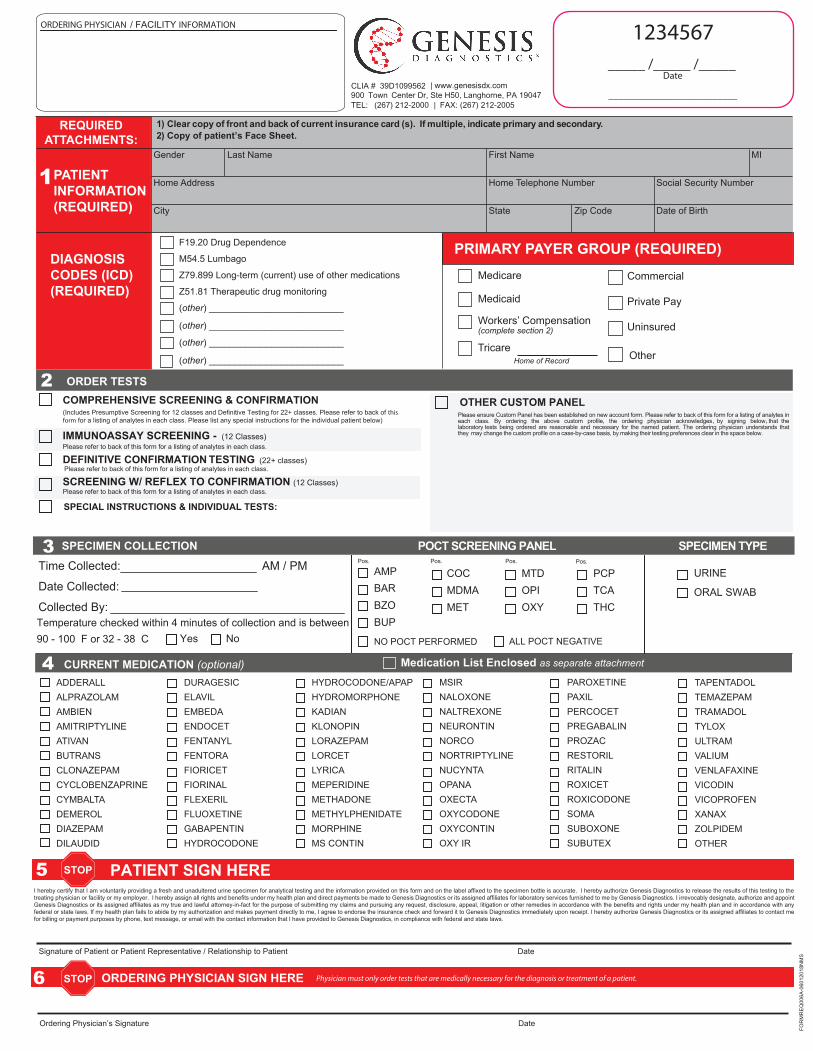
REQUIRED ATTACHMENTS: 1 PATIENT INFORMATION (REQUIRED) DIAGNOSIS CODES (ICD) (REQUIRED) Clear copy of front and back of current insurance card (s). If multiple, indicate primary and secondary. Copy of patient’s Face Sheet. Gender Home Address City Home Telephone Number Social Security Number State Zip Code Date of Birth Last Name First Name MI Medicare Medicaid Workers’ Compensation (complete section 2) Commercial Private Pay Uninsured PRIMARY PAYER GROUP (REQUIRED) F19.20 Drug Dependence M54. Lumbago Z79.899 Long-term (current) use of other medications Z51.81 Therapeutic drug monitoring (other) __________________________ (other) __________________________ (other) __________________________ (other) __________________________ Tricare Home of Record Other , , Time Collected: AM / PM Date Collected: Collected By: BUP BZO BAR AMP COC MDMA MET MTD OPI OXY PCP TCA THC Pos. Pos. Pos. Pos. NO POCT PERFORMED Temperature checked within 4 minutes of collection and is between 90 - 100 F or 32 - 38 C ALL POCT NEGATIVE URINE ORAL SWAB Yes No COMPREHENSIVE SCREENING & CONFIRMATION (Includes Presumptive Screening and Definitive Testing Please refer to back of this form for a listing of analytes in each class. Please list any special instructions for the individual patient below) ORDER TESTS SPECIMEN COLLECTION POCT SCREENING PANEL SPECIMEN TYPE PATIENT STOP I hereby certify that I am voluntarily providing a fresh and unadultered urine specimen for analytical testing and the information provided on this form and on the label affixed to the specimen bottle is accurate. I hereby authorize Genesis Diagnostics to release the results of this testing to the treating physician or facility or my employer. I hereby assign all rights and benefits under my health plan and direct payments be made to Genesis Diagnostics or its assigned affiliates for laboratory services furnished to me by Genesis Diagnostics. I irrevocably designate, authorize and appoint Genesis Diagnostics or its assigned affiliates as my true and lawful attorney-in-fact for the purpose of submitting my claims and pursuing any request, disclosure, appeal, litigation or other remedies in accordance with the benefits and rights under my health plan and in accordance with any federal or state laws. If my health plan fails to abide by my authorization and makes payment directly to me, I agree to endorse the insurance check and forward it to Genesis Diagnostics immediately upon receipt. I hereby authorize Genesis Diagnostics or its assigned affiliates to contact me for billing or payment purposes by phone, text message, or email with the contact information that I have provided to Genesis Diagnostics, in compliance with federal and state laws. Signature of Patient or Patient Representative / Relationship to Patient Physician’s Signature 19047 OTHER CUSTOM PANEL the the that the The that the the ORDERING PHYSICIAN INFORMATION STOP CURRENT MEDICATION Medication List as separate attachment ADDERALL ALPRAZOLAM AMBIEN AMITRIPTYLINE ATIVAN BUTRANS CLONAZEPAM CYCLOBENZAPRINE CYMBALTA DEMEROL DIAZEPAM DILAUDID DURAGESIC ELAVIL EMBEDA ENDOCET FENTANYL FENTORA FIORICET FIORINAL FLEXERIL FLUOXETINE GABAPENTIN HYDROCODONE HYDROCODONE/APAP HYDROMORPHONE KADIAN KLONOPIN LORAZEPAM LORCET LYRICA MEPERIDINE METHADONE METHYLPHENIDATE MORPHINE MS CONTIN MSIR NALOXONE NALTREXONE NEURONTIN NORCO NORTRIPTYLINE NUCYNTA OPANA OXECTA OXYCODONE OXYCONTIN OXY IR PAROXETINE PAXIL PERCOCET PREGABALIN PROZAC RESTORIL RITALIN ROXICET ROXICODONE SOMA SUBOXONE SUBUTEX TAPENTADOL TEMAZEPAM TRAMADOL TYLOX ULTRAM VALIUM VENLAFAXINE VICODIN VICOPROFEN XANAX ZOLPIDEM OTHER Physician must only order tests that are medically necessary for the diagnosis or treatment of a patient. 6 TESTING Please refer to back of this form for a listing of analytes in each class. Please refer to back of this form for a listing of analytes in each class. Please refer to back of this form for a listing of analytes in each class. SPECIAL INSTRUCTIONS & INDIVIDUAL TESTS: | www.genesisdx.com
Transcript of Toxicology Req 6-14 Final - Genesis · 2020-01-28 · klonopin lorazepam lorcet lyrica meperidine...
REQUIREDATTACHMENTS:
1PATIENTINFORMATION(REQUIRED)
DIAGNOSISCODES (ICD)(REQUIRED)
Clear copy of front and back of current insurance card (s). If multiple, indicate primary and secondary. Copy of patient’s Face Sheet.
Gender
Home Address
City
Home Telephone Number Social Security Number
State Zip Code Date of Birth
Last Name First Name MI
Medicare
Medicaid
Workers’ Compensation(complete section 2)
Commercial
Private Pay
Uninsured
PRIMARY PAYER GROUP (REQUIRED)F19.20 Drug Dependence
M54. Lumbago
Z79.899 Long-term (current) use of other medications Z51.81 Therapeutic drug monitoring
(other) __________________________
(other) __________________________
(other) __________________________
(other) __________________________Tricare
Home of Record Other
, ,
Time Collected: AM / PM
Date Collected:
Collected By:BUPBZOBARAMP COC
MDMAMET
MTDOPIOXY
PCPTCATHC
Pos. Pos. Pos. Pos.
NO POCT PERFORMED
Temperature checked within 4 minutes of collection and is between90 - 100 F or 32 - 38 C ALL POCT NEGATIVE
URINE
ORAL SWAB
Yes No
COMPREHENSIVE SCREENING & CONFIRMATION(Includes Presumptive Screening and Definitive Testing Please refer to back of this form for a listing of analytes in each class. Please list any special instructions for the individual patient below)
ORDER TESTS
SPECIMEN COLLECTION POCT SCREENING PANEL SPECIMEN TYPE
PATIENT STOP
I hereby certify that I am voluntarily providing a fresh and unadultered urine specimen for analytical testing and the information provided on this form and on the label affixed to the specimen bottle is accurate. I hereby authorize Genesis Diagnostics to release the results of this testing to the treating physician or facility or my employer. I hereby assign all rights and benefits under my health plan and direct payments be made to Genesis Diagnostics or its assigned affiliates for laboratory services furnished to me by Genesis Diagnostics. I irrevocably designate, authorize and appoint Genesis Diagnostics or its assigned affiliates as my true and lawful attorney-in-fact for the purpose of submitting my claims and pursuing any request, disclosure, appeal, litigation or other remedies in accordance with the benefits and rights under my health plan and in accordance with any federal or state laws. If my health plan fails to abide by my authorization and makes payment directly to me, I agree to endorse the insurance check and forward it to Genesis Diagnostics immediately upon receipt. I hereby authorize Genesis Diagnostics or its assigned affiliates to contact me for billing or payment purposes by phone, text message, or email with the contact information that I have provided to Genesis Diagnostics, in compliance with federal and state laws.
Signature of Patient or Patient Representative / Relationship to Patient
Physician’s Signature
19047
OTHER CUSTOM PANEL
the the that the The that
the the
ORDERING PHYSICIAN INFORMATION
STOP
CURRENT MEDICATION Medication List as separate attachment
ADDERALLALPRAZOLAMAMBIENAMITRIPTYLINEATIVANBUTRANSCLONAZEPAMCYCLOBENZAPRINECYMBALTADEMEROLDIAZEPAMDILAUDID
DURAGESICELAVILEMBEDAENDOCETFENTANYLFENTORAFIORICETFIORINALFLEXERILFLUOXETINEGABAPENTINHYDROCODONE
HYDROCODONE/APAPHYDROMORPHONEKADIANKLONOPINLORAZEPAMLORCETLYRICAMEPERIDINEMETHADONEMETHYLPHENIDATEMORPHINEMS CONTIN
MSIRNALOXONENALTREXONENEURONTINNORCONORTRIPTYLINENUCYNTAOPANAOXECTAOXYCODONEOXYCONTINOXY IR
PAROXETINEPAXILPERCOCETPREGABALINPROZACRESTORILRITALINROXICETROXICODONESOMASUBOXONESUBUTEX
TAPENTADOLTEMAZEPAMTRAMADOLTYLOXULTRAMVALIUMVENLAFAXINEVICODINVICOPROFENXANAXZOLPIDEMOTHER
Physician must only order tests that are medically necessary for the diagnosis or treatment of a patient.6
TESTINGPlease refer to back of this form for a listing of analytes in each class.
Please refer to back of this form for a listing of analytes in each class.
Please refer to back of this form for a listing of analytes in each class.
SPECIAL INSTRUCTIONS & INDIVIDUAL TESTS:
| www.genesisdx.com

AMPHETAMINES OPIATES: NATURAL ANTICONVULSANTSMethamphetamine Morphine CarbamazepineAmphetamine Codeine GabapentinMethylphenidate Pregabalin
OPIOIDS: SEMI-SYNTHETICHydromorphone MUSCLE RELAXANTS
BENZODIAZEPINES Noroxycodone CarisoprodolNordiazepam Norhydrocodone CyclobenzaprineOxazepam HydrocodoneTemazepam Oxycodone NON BENZODIAZEPINE
HYPNOTICSAlprazolam Oxymorphone ZolpidemAlpha-hydroxyalprazolam Buprenorphine Zopiclone/EszopicloneFlurazepam Norbuprenorphine ZaleplonLorazepam2-Hydroxyethylflurazepam OPIOIDS: SYNTHETICDesmethylflunitrazepam Fentanyl7-aminoclonazepam Norfentanyl
MeperidineILLICITS NormeperidineCocaine MethadoneBenzoylecgonine EDDP (Methadone Mtb)Ketamine NaltrexoneEcstasy (MDMA) NaloxoneMDA 6beta-NaltrexolMDEAMitragynine (Kratum) NON OPIOID ANALGESICS6-Monoacetylmorphine TramadolPhencyclidine (PCP) Desmethyltramadol
TapentadolILLICITS: CATHINONES (BATH SALTS) DesmethyltapentadolButyloneEthylone ILLICITS: SYNTHETIC
CANNABINOIDSMethylone JWH 210 5-Hydroxy pentylMDPV JWH 122 5-Hydroxy pentylMephedrone
IMMUNOASSAY SCREENING CLASSES AND CUTOFFS
CUTOFF1000 ng/mL200 ng/mL200 ng/mL300 ng/mL300 ng/mL
10 ng/mL
300 ng/mL100 ng/mL25 ng/50 ng/300 ng/mL100 mg/dL
AMPHETAMINESCLASS
BARBITURATESBENZODIAZEPINESCOCAINEMETHADONEOPIATESOXYCODONEPHENCYCLIDINE (PCP)CANNABINOIDES (THC)PROPOXYPHENE (PPX)ETHANOL6-MAM
ANTIDEPRESSANTSAmitriptylineDesipramineDesmethyldoxepinDoxepinFluoxetineImipramineNortriptylineParoxetineVenlafaxine
COMPREHENSIVE MEDICATION COMPLIANCE PANEL DRUG CLASSES AND MAIN COMPONENTS OF EACH CLASS*
P resumptive
* Each test/class can be ordered separately . Please provide special instructions on thefront of this form.
De�nitive


















