
Towards universal coverage in DRC: spatial and financial barriers to accessing care Presented by...
23
Towards universal coverage in DRC: spatial and financial barriers to accessing care Presented by Caryn Bredenkamp Health Economist, World Bank, Washington DC based on analysis by Brian Blankespoor, Caryn Bredenkamp, Patrick Mullen, Danic Ostiguy and Waly Wane African Health Economics and Policy Association (AfHEA) Dakar, Senegal 16 March 2011
-
date post
19-Dec-2015 -
Category
Documents
-
view
216 -
download
1
Transcript of Towards universal coverage in DRC: spatial and financial barriers to accessing care Presented by...

Towards universal coverage in DRC: spatial and financial
barriers to accessing care
Presented by Caryn BredenkampHealth Economist, World Bank, Washington DC
based on analysis by Brian Blankespoor, Caryn Bredenkamp, Patrick Mullen, Danic Ostiguy and Waly Wane
African Health Economics and Policy Association (AfHEA) Dakar, Senegal16 March 2011

Not on track to meet the MDGs 1c, 4 and 5
Health outcomes are improving, but remain poor: - - 45.5% of children are chronically malnourished- - under-five mortality is 148 per 1,000 live births - - maternal mortality ratio is 549 per 100,000 live births Coverage of many high impact interventions, especially
preventive, is low:- 31% of one-year-old children are fully immunized- 6% of under-five children sleep under insecticide-
treated bednets
=> Demand-side barriers - financial and spatial - to accessing care
Source: DHS 2007
Objective
1. Explore how spatial data and GIS techniques can be used to broaden our understanding of physical/spatial access to health care
2. Identify the areas that are insufficiently served by primary health care services in order to inform decisions about service expansion
3. Highlight financial costs of seeking care
Study area
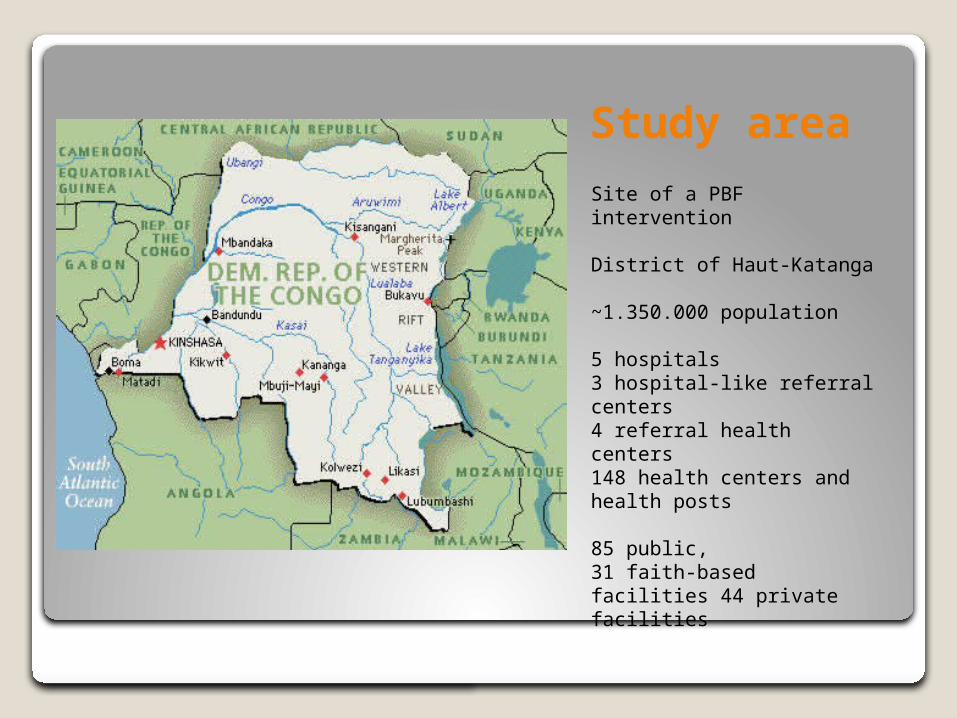
Site of a PBF intervention
District of Haut-Katanga
~1.350.000 population
5 hospitals3 hospital-like referral centers4 referral health centers148 health centers and health posts
85 public, 31 faith-based facilities 44 private facilities
Data sources
Baseline data from PBF impact evaluation – Sept-Oct 2009
- Household survey - Community survey - Patient exit interviews - Facility surveys – with staff interviews - GPS coordinates
Secondary GPS data
Measuring spatial access to care

Data description I
Primary data collection: • GPS coordinates of health facilities
were collected - as part of the baseline
• Hand-drawn maps of the boundaries of health zones and health areas were obtained from the chief doctors of the health zones in Haut-Katanga

Data description II
Secondary data collection: Geographic Information System (GIS) data
• Road networks from multiple sources• Village locations• Administrative units• Hydrography• Elevation• Slope
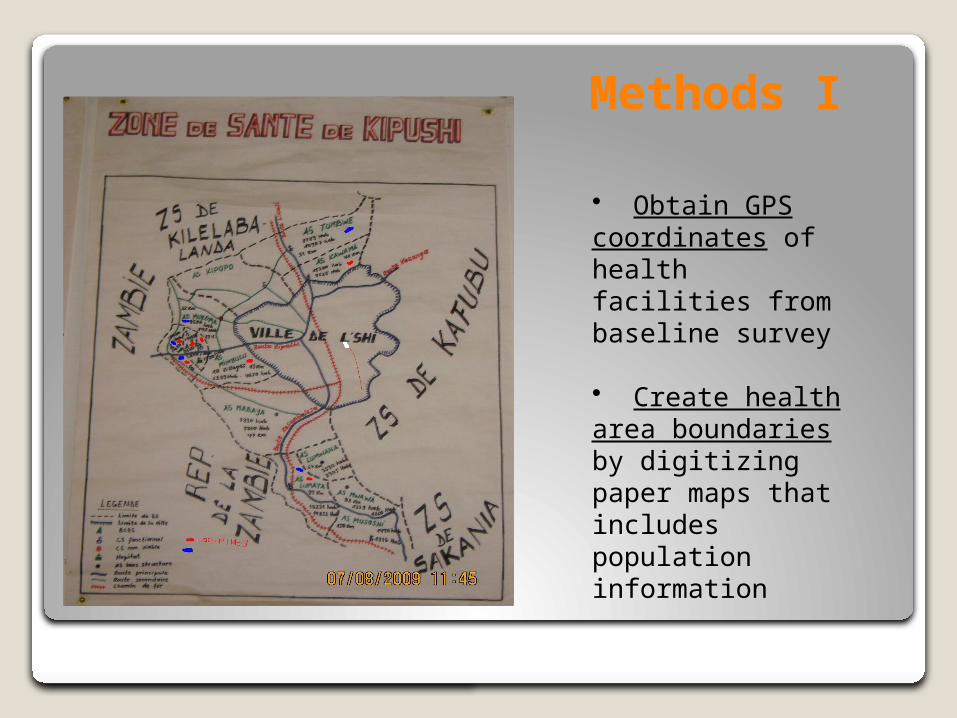
Methods I
• Obtain GPS coordinates of health facilities from baseline survey
• Create health area boundaries by digitizing paper maps that includes population information
Methods II
3. Define catchment area Includes all villages/settlements that are closest to the particular health facility relative to all other facilities
4. Integrate road network information to estimate travel time. First, by using data on the GPS coordinates of health facilities and villages/settlements, and adding known transportation routes, we are able to build a spatial model that estimates average travel time to the health centers for each village using GIS data based on an approach by Nelson (2008).
5. Summarize information on population to display the distribution of population among the health centers
Nelson, A. 2008. Travel time to major cities: A global map of Accessibility. Global Environment Monitoring Unit - Joint Research Centre of the European Commission, Ispra Italy. Available at http://gem.jrc.ec.europa.eu
Results
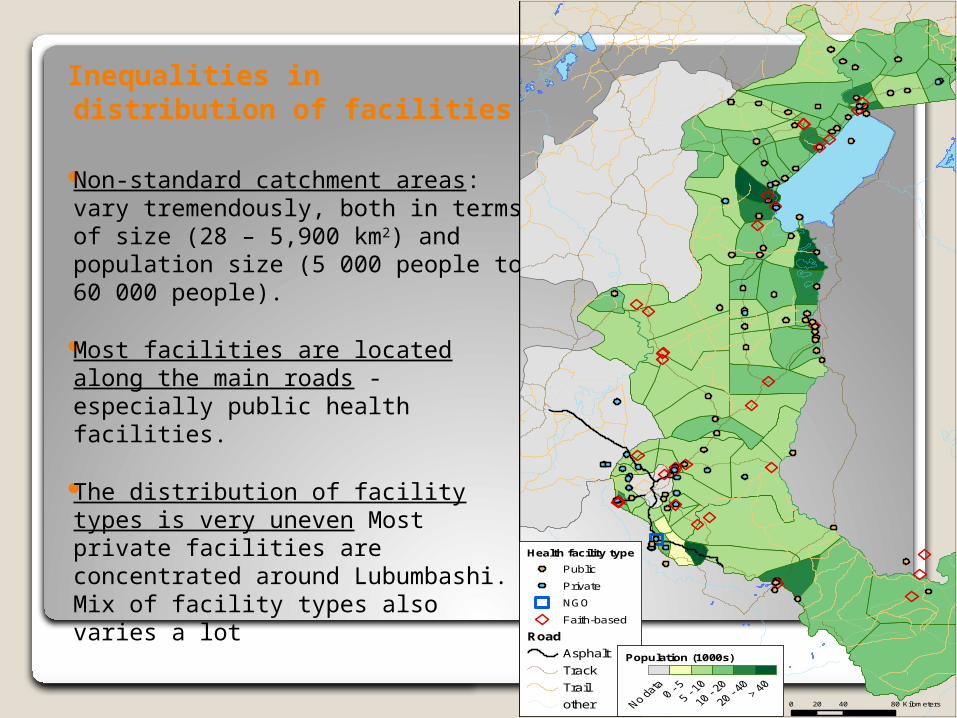
Inequalities in distribution of facilities
Non-standard catchment areas: vary tremendously, both in terms of size (28 – 5,900 km2) and population size (5 000 people to 60 000 people).
Most facilities are located along the main roads - especially public health facilities.
The distribution of facility types is very uneven Most private facilities are concentrated around Lubumbashi. Mix of facility types also varies a lot
Health facility type
Public
Private
NGO
Faith-based
Road
Asphalt
Track
Trail
other
Population (1000s)
0 40 8020 Kilometers

Inequalities in travel time
•Translate road-type information into travel time using method of Nelson (2008)•=> map
• Assume even population distribution by health area, find: Population with more than 4 hours travel time to nearest facility: 610,000Population with less than 4 hours travel time:483,000
• Settlement point population would improve the health area population estimates
")
")")")")
")
")
")
")
")
")
")
")") Referral health centre / hospital
Health area
Travel time (hrs)
< 1
1 - 2
2 - 3
3 - 4
> 40 60 12030
Km
Adding information from household surveys and exit
interviewsA more nuanced picture of access
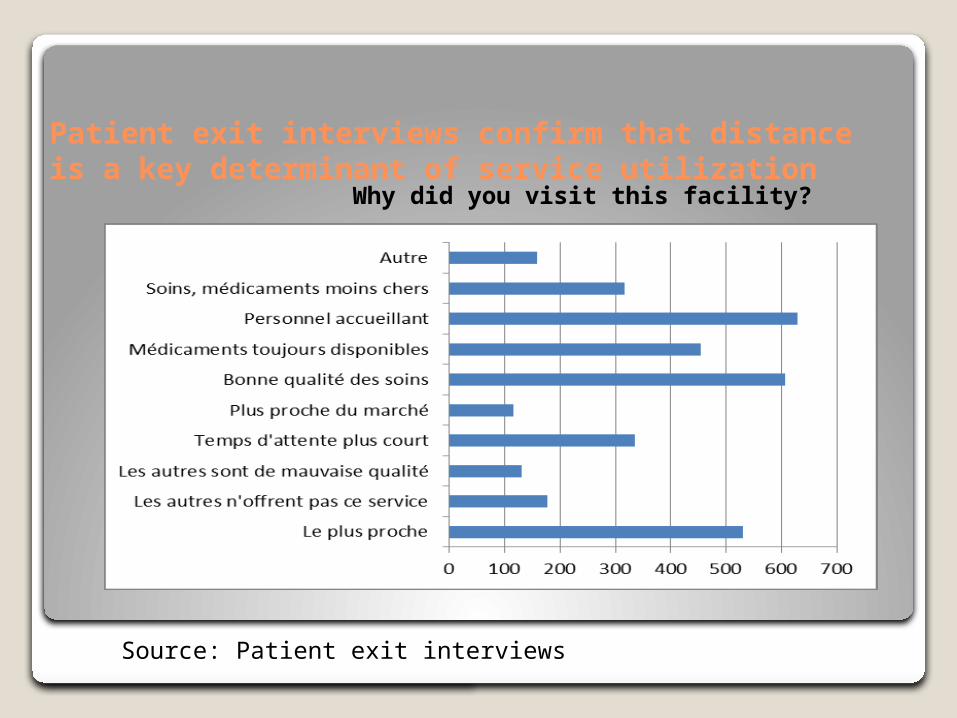
Patient exit interviews confirm that distance is a key determinant of service utilization
Source: Patient exit interviews
Why did you visit this facility?
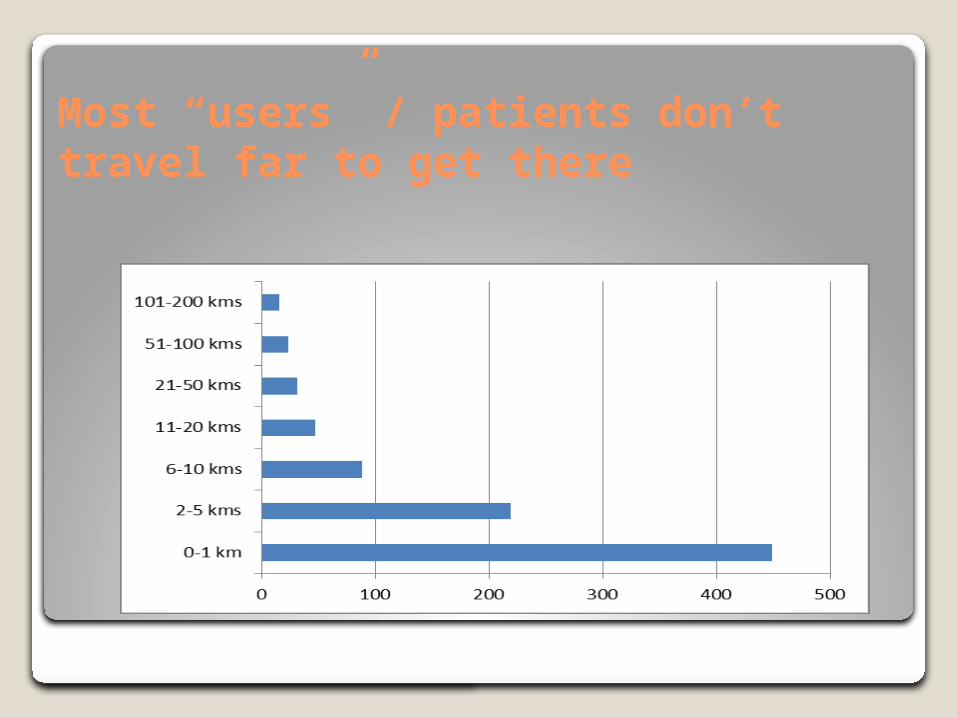
Most “users” / patients don’t travel far to get there

Most travel by foot
voiture, moto
transport public
Bicyclette
Charrette
A pied
Autre
0 100 200 300 400 500 600 700
41
24
186
6
608
7
Type of transportation used to reach facility (exit interviews)
Implication: It is likely that most households in the “green areas” are hardly accessing care (as expected)

This is confirmed by travel cost information
54
818
Number of patients who incurred transportation costs
OuiNon

Costs of care dominated by consultations and medicines
CS public CS privé CS confessionnelGuérisseur trad.0
500
1000
1500
2000
2500
3000
3500
4000
4500
ConsultationsDonsMédicamentsTestsTransport
Source: Household survey

So, given the barriers, how high are utilization rates?
Number of people using primary care in the last four weeks:- Public 436- Private 247- Faith-based 80- Traditional 113- Total 876 out of 6817 people
(12.9%)Source: Household survey

• The population in Haut-Katanga faces substantial spatial barriers to accessing care. These include great distances to primary and referral health facilities and a poor road network that contribute to long travel times
• With relatively little additional data collection – and even without household surveys - much can be learnt about a population’s spatial access to care
• But, patient interviews and household surveys add useful additional information – costs of accessing care, and utilization rates
Conclusion
Acknowledgments
Funding for the data collection of this project was provided by the Health Results Innovation Trust Fund (HRITF), World Bank. The findings, interpretations, and conclusions expressed on this poster are entirely those of the authors.
For further information
Please contact [email protected] or [email protected].
More information on related research projects can be obtained at http://econ.worldbank.org; http://www.worldbank.org/hnp; and http://www.rbfhealth.org



















