
Toric iol
24
TORIC IOL’s Jagdish Dukre
-
Upload
jagdish-dukre -
Category
Health & Medicine
-
view
97 -
download
5
Transcript of Toric iol
TORIC IOL’s
Jagdish Dukre
Modern cataract surgery is more of refractive surgery.
Myopia & hypermetropia can be corrected using appropriate spherical powers of IOL’s.
However approximately 20% of patients who undergo cataract surgery have 1.25D of corneal astigmatism or more.
It can be corrected with Toric IOL’s.
Other options for correction of co-existent cataract and astigmatism
LRI during cataract surgery( upredictable results)
Laser procedures postoperatively (are associated with new set of complications).
History of Toric IOL’s
First introduced by Shimizu et al in 1994.
It was nonfoldable 3 piece toric IOL made from PMMA.
It had oval optic with loop haptics ,available in cylinder power 2-3 D.
Postoperatively 20% IOL’s rotated > 30 degrees and 50% IOL rotated about 10 degrees.
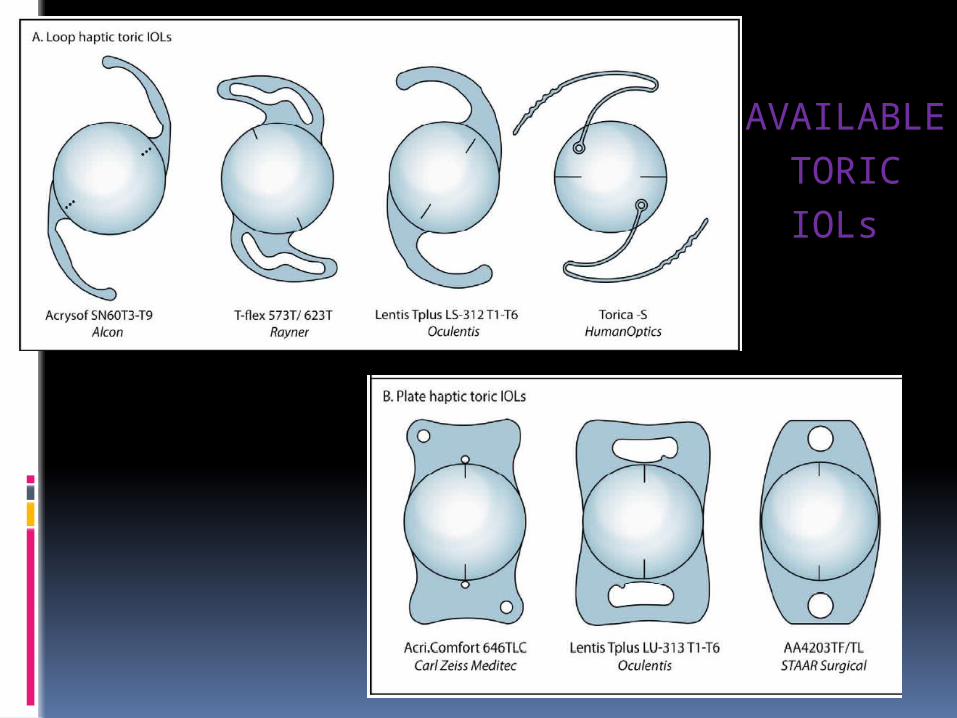
AVAILABLE
TORIC
IOLs
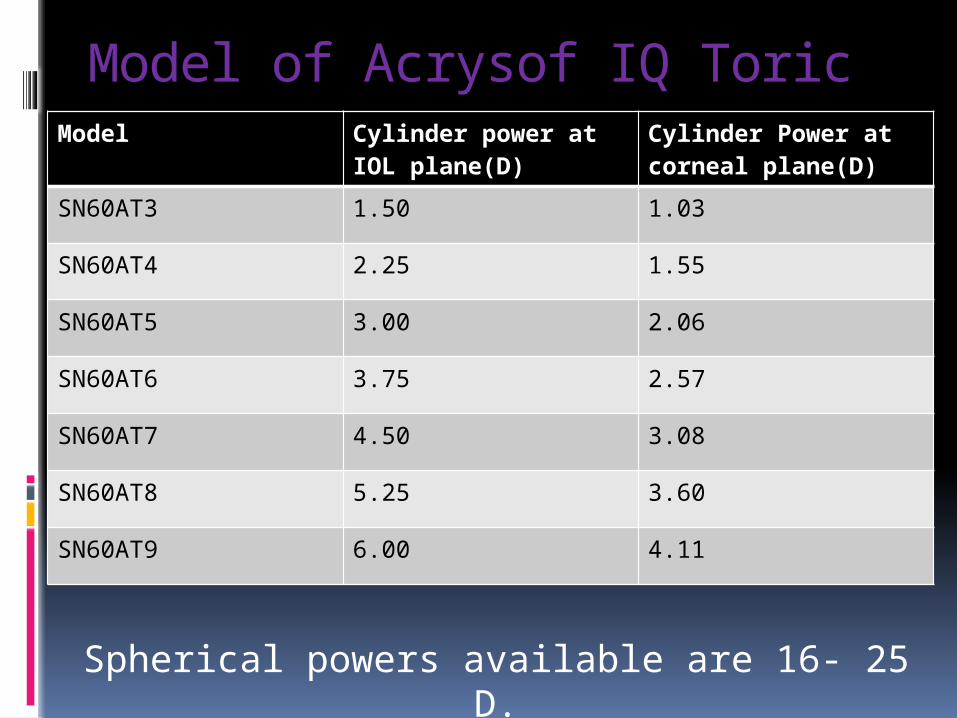
Model of Acrysof IQ ToricModel Cylinder power at IOL
plane(D)Cylinder Power at corneal plane(D)
SN60AT3 1.50 1.03
SN60AT4 2.25 1.55
SN60AT5 3.00 2.06
SN60AT6 3.75 2.57
SN60AT7 4.50 3.08
SN60AT8 5.25 3.60
SN60AT9 6.00 4.11
Spherical powers available are 16- 25 D.
Factor Affecting Rotation of Toric IOL
(1) IOL material
Hydrophobic Acrylic < Hydrophilic Acrylic < PMMA < Silicon
(2) Overall IOL diameter - Larger diameter prevents rotation . Toric IOL’s are available nowadays in 11-13 mm overall diameter.
(3) Haptic design –
Initial concept
- Loop haptics prevent early rotation .
- Plate haptics prevent late rotation.
Recent concept – No difference in incidence of post operative
rotation between plate and loop haptics provided material of
both loop and plate is same.
Patient selection
Regular corneal astigmatism > 1.5 D
Vision compromising cataract
Patient wants spectacle independence
Facts
20% of patients with cataract have astigmatism >1.25 D
Every incision on cornea induces additonal astigmatism (SIA).
Implantation of monofocal lens will require distance and near correction both in these cases.
B/L Toric IOL’s give high level of spectacle independence(97%).
Requirement of near correction can be overcome by multifocal toric IOL(AcriLisa multifocal toric IOL)
Toric IOL power calculation : Precise keratometry
Surgically induced astgmatism [SIA].
Keratometry
Can be done with Manual keratometer Automated keratometer with steps of 0.12 only Corneal topography
K readings from all the three show high repeatability and are comparable.
Manual keratometer should be calibrated regularly.
Corneal topography is required in case of unusual reading & poor quality mires.
Precautions Reading must be quick to avoid drying of cornea. Don’t rub on the cornea. Centration must be proper.
Surgically Induced Astigmatism Every incision changes the cornea.
Closer to the centre & larger the incision more effect on corneal curvature.
Other factors affecting it are preoprative corneal astigmatism, suture use and patient’s age.
In addition there is variability from patient to patient.
Overall effect can be summed up with vector analysis.
SIA Calculation
Obtain SIA calculator
Fill it for 20-30 cases minimum
Be precise about axis and incision
Calculator auto calculates SIA
15
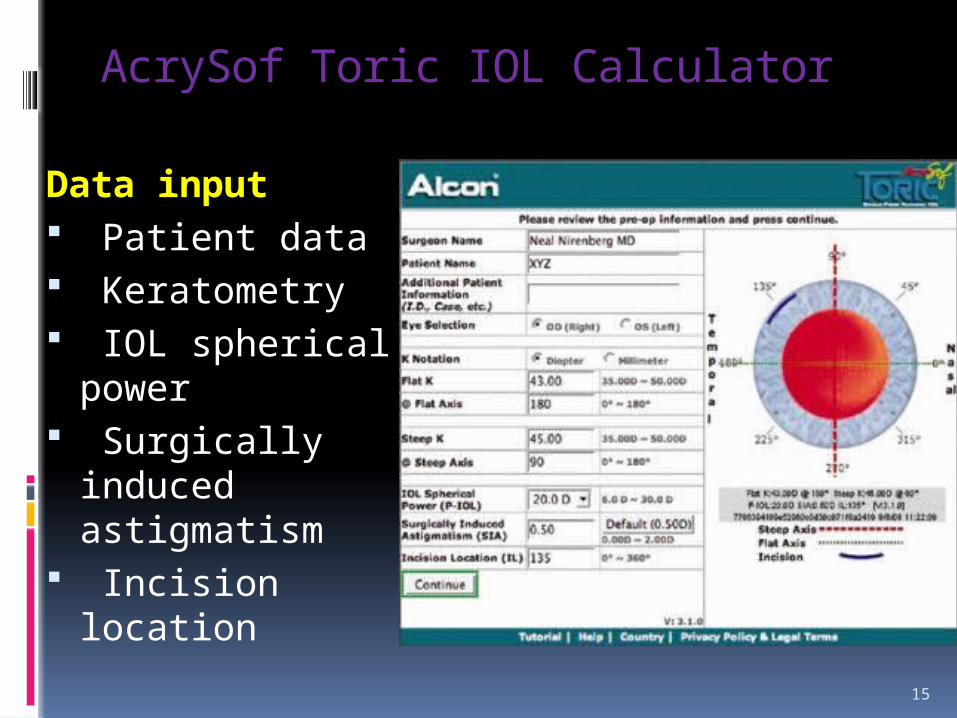
AcrySof Toric IOL Calculator
Data input Patient data Keratometry IOL spherical
power Surgically induced
astigmatism Incision location
16
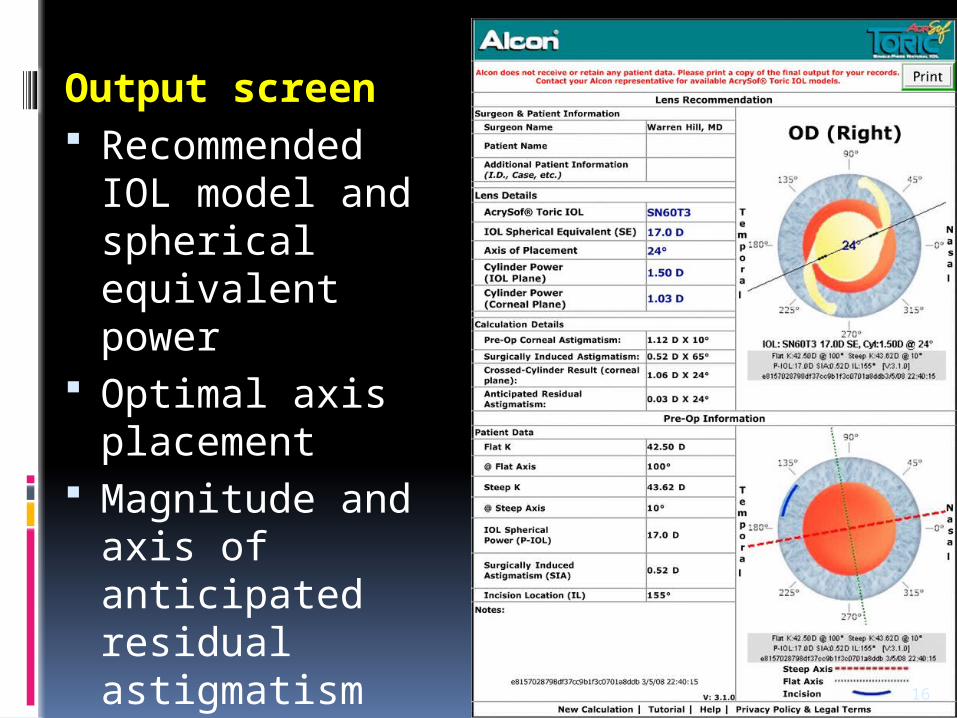
Output screen Recommended IOL
model and spherical equivalent power
Optimal axis placement
Magnitude and axis of anticipated residual astigmatism
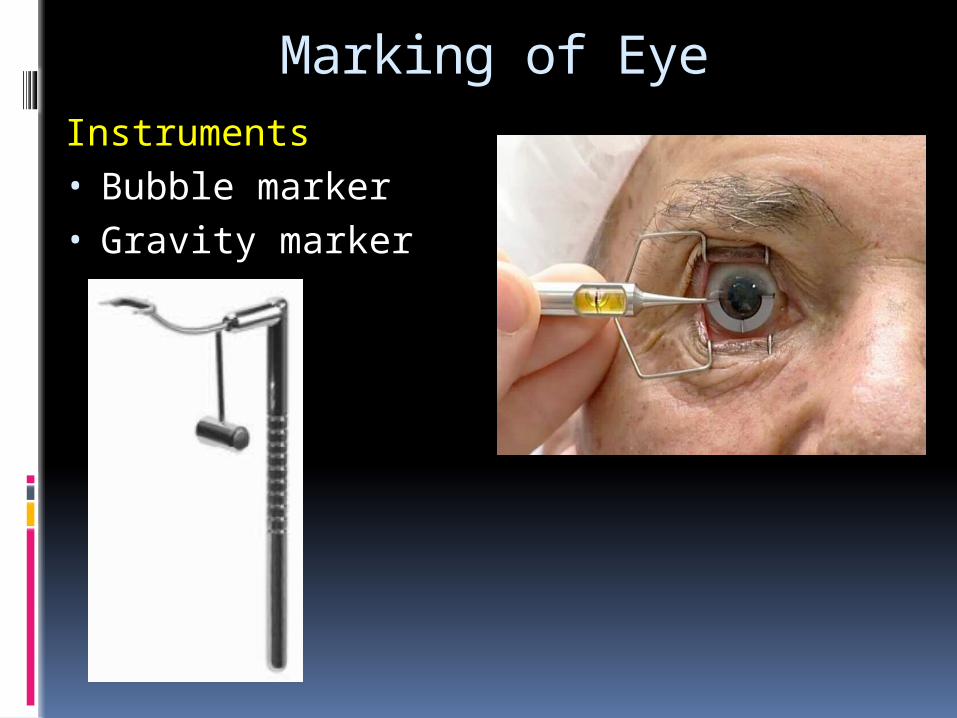
Marking of EyeInstruments • Bubble marker • Gravity marker

STEPS
A) Reference marking- Done prior to surgery with patient upright- Two reference markers placed at limbus 180 degree apart- Used to align marking instuments for placement of axis
marks
B) Axis marking : Using reference marks as a guide the patient eye is marked accurately at two positions 180 degree apart
TIPS:-
- Dry the conjunctiva with a swab
- Enhance marking at 3-9 o clock
- Apply mark with twisting action
- It lasts throughout surgery
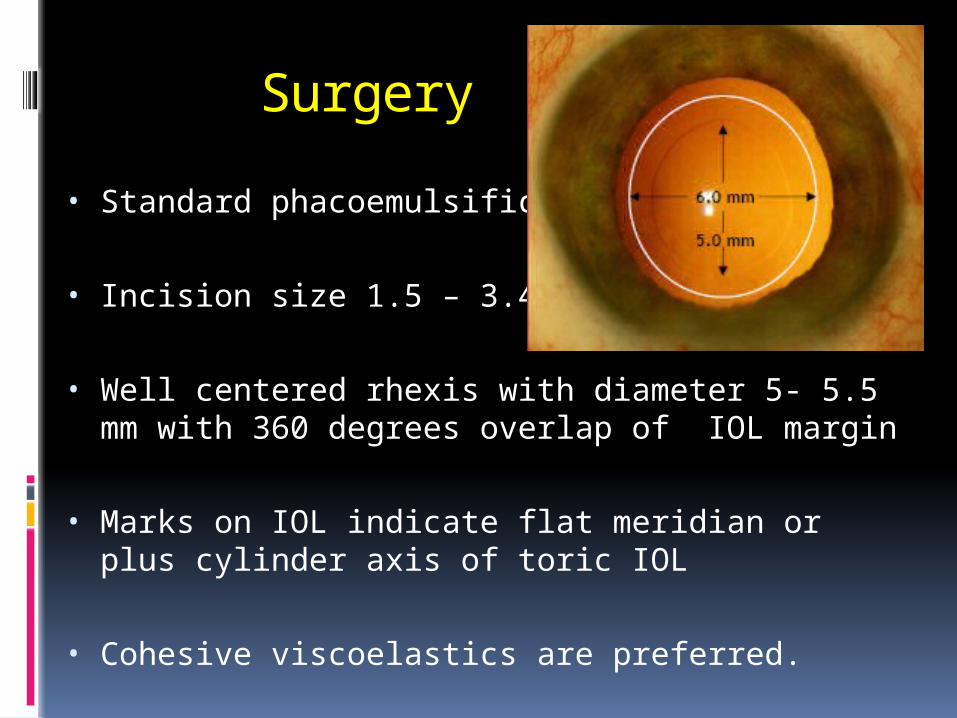
Surgery
• Standard phacoemulsification
• Incision size 1.5 – 3.4 mm
• Well centered rhexis with diameter 5- 5.5 mm with 360 degrees overlap of IOL margin
• Marks on IOL indicate flat meridian or plus cylinder axis of toric IOL
• Cohesive viscoelastics are preferred.
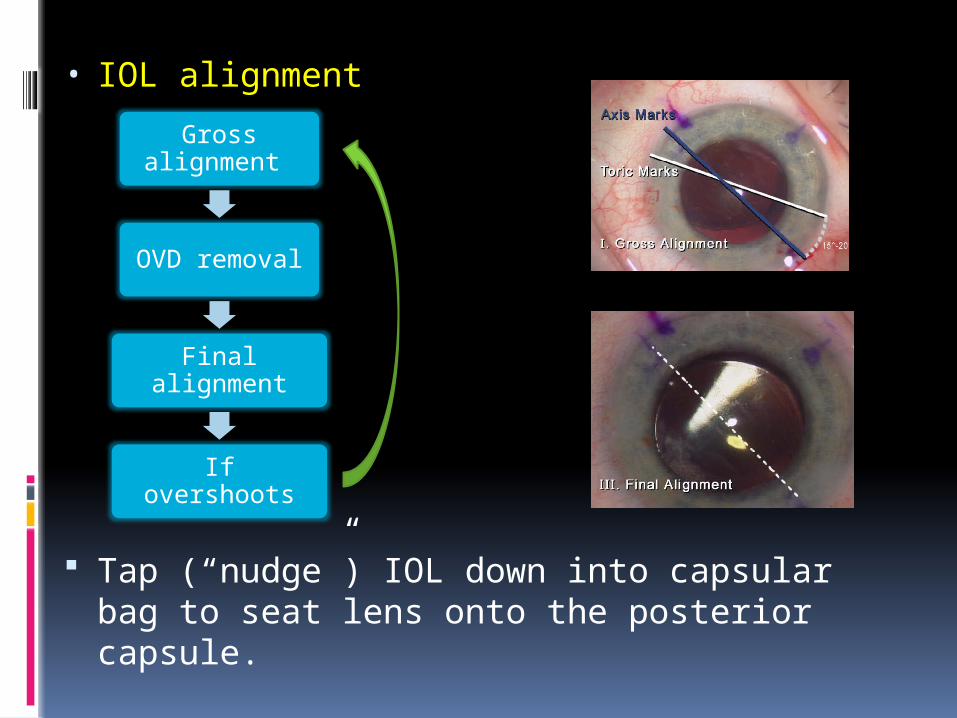
• IOL alignment
Tap (“nudge”) IOL down into capsular bag to seat lens onto the posterior capsule.
Gross alignment
OVD removal
Final alignment
If overshoots
If any compromise of zonular integrity or capsule occurs please switch to standard non toric IOL
Postoperative axis alignment :
Slit Lamp with dilated pupil
Wavefront aberrometry in undilated pupil
Realignment should be done in < 2 wks
22
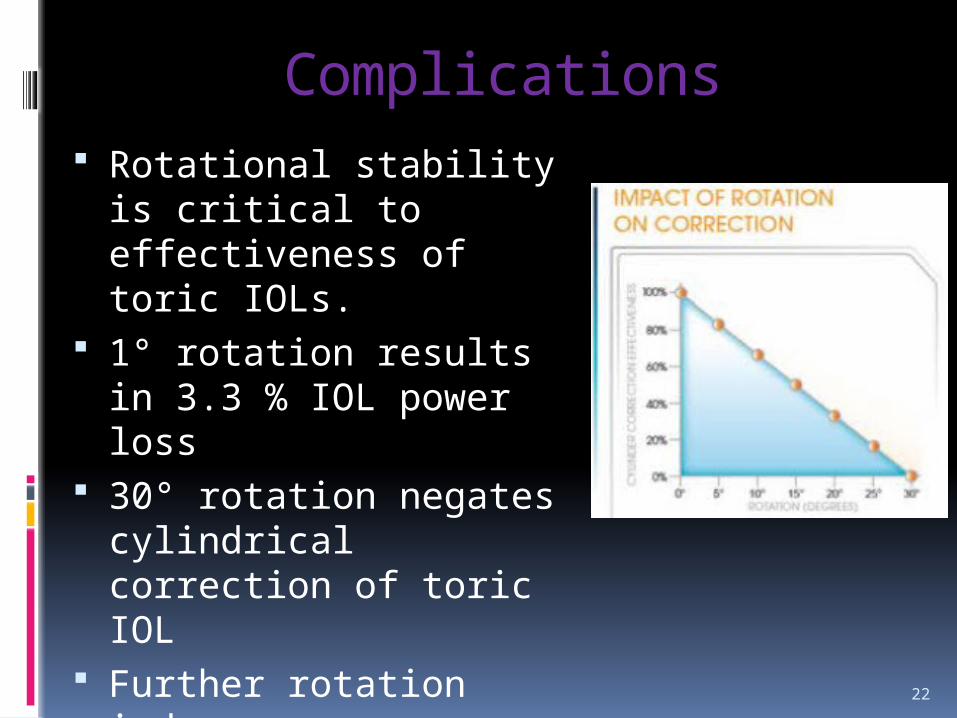
Complications Rotational stability is critical
to effectiveness of toric IOLs. 1° rotation results in 3.3 %
IOL power loss 30° rotation negates
cylindrical correction of toric IOL
Further rotation induces more astigmatism
Conclusion
Bilateral toric IOL implantation shows high percentage of spectacle independence for distance vision.



















