Top Dermatological Tips on diagnosing skin lesions for busy GPs! Louise Moss GP Moss Valley Medical...
65
Top Dermatological Tips on diagnosing skin lesions for busy GPs! Louise Moss GP Moss Valley Medical Practice, Eckington 28 th March 2012
-
Upload
iyanna-chessher -
Category
Documents
-
view
217 -
download
0
Transcript of Top Dermatological Tips on diagnosing skin lesions for busy GPs! Louise Moss GP Moss Valley Medical...

Top Dermatological Tips on diagnosing skin lesions
for busy GPs!
Louise MossGP Moss Valley Medical
Practice, Eckington 28th March 2012

Aim for today
To feel more confident about how to diagnose and treat some common skin lesions within general practice.
Remember,common things occur commonly!

So what do we need to cover?
• In 2009 I reviewed the sorts of skin conditions referred to my GPwSI clinic to see if this would help plan teaching for GPs, practice nurses & registrars.
• 229 patients were seen from 3 neighbouring practices in a GPwSI community clinic

Outcomes
DX rate 60%
FU Rate 16%
Referred to Hospital Dermatology service 24%

A rash lesion?
60% were lesions
60%
40%Lesion
Rashes

? S
kin
CA
for
surg
ery
Be
nig
n N
ae
vus
Se
bo
rrh
eic
wa
rt
Act
inic
Ke
rato
sis
Vira
l wa
rt
Ha
em
an
gio
ma
So
lar
len
tigo
Bo
we
ns
CD
NH
De
rma
tofib
rom
a
Ke
loid
Se
ba
ceo
us
cyst
Pyo
ge
nic
gra
nu
lom
a
Infla
mm
ato
ry le
sio
n
Ha
em
ato
ma
Pilo
ma
trix
om
a
Co
ng
en
ital l
esi
on
foo
t0
5
10
15
20
25
30
35
40
0%
20%
40%
60%
80%
100%
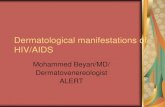
Frequency of lesions
FrequencyCumulative frequency %

Ecz
em
a
Acn
e
Pso
ria
sis
Ha
nd
ecz
em
a
Urt
ica
ria
Na
il d
ystr
op
hy
Ba
ct fo
llicu
litis
Sca
ly s
calp
s
Lic
he
n P
lan
us
P. v
ers
ico
lor
Ne
uro
de
rma
titis
Po
st in
flam
ato
ry h
ype
rpig
me
nt
Urt
ica
ria
pig
me
nto
sa
Dru
g e
rup
tion
DL
E
Tin
ea
inco
gn
ito
Vir
al e
xan
the
m
Act
inic
po
roke
rato
sis
LS
& A
Pe
rio
ral d
erm GA
P. r
ose
a
Tra
um
a
Ch
r p
aro
nyc
hia
Su
bu
ng
ua
l ha
em
ato
ma
K. p
ilan
s
Alo
pe
cia
Lip
lick
ing
ch
elit
is
Vo
n R
eck
ing
ha
nse
urs
café
au
lait
spo
ts
BX
O
Co
nta
ct a
llerg
ic d
erm
0
5
10
15
20
0%
20%
40%
60%
80%
100%
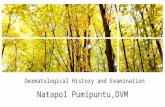
Rashes: Frequency of condition
Frequency
Cumulative frequency %

– Possible Skin cancer– Benign naevi– Seborrhoeic warts– Actinic Keratosis
• How can you increase your confidence?
80% of lesions referred include…

• The majority of these can be managed in primary care
• Benign Naevi• Actinic keratosis• Seborrhoeic Keratoses
• Also need to be able to identify common skin cancers

Top tips for lesion recognition
• Take a good history- sun exposure, pmh/fh• Have a careful look with good light &
magnification• Touch and feel- stretch the skin, if there’s a
crust what’s beneath?• Look elsewhere for other examples• Is there a pattern?

Make sure you look properly......

If there’s a crust take it off..........

What’s that?

DESCRIBING SKIN LESIONS
Site and size- record measurementColourSurface or TextureType of lesionBorder/shapeAttacehment to other structuresSingle or multiple/ arrangement of lesions
IF YOU LOOK CAREFULLY YOU WILL BE ABLE TO DIAGNOSE WITH MORE CONFIDENCE!

Macule < 1cm

Patch >1cm

Plaque

Papule <1 cm

Nodule >1cm

Pustule <1cm

Vesicle <1cm

Bulla >1cm

Types of skin cancer

Non melanoma skin cancer


Basal cell carcinoma
What to look for..........• Shine• Superficial telangectasia• Rolled edge• Spots of pigmentation• Ulceration
• A history of slow growth & bleeding on sun-damaged skin

Don’t forget there are different types……
• Nodular/cystic• Superficial• Morpheic• Pigmented



Stretch the skin and look from the side.............
• YOU NEED TO TOUCH!


Benign naevi?

Squamous cell carcinoma
• Rapidly growing• Tender• Indurated base• On sundamaged skin• ? Immunosupression• ? Worked in tropics


Solar (Actinic) Keratoses
• Common sun exposed sites in older people
UK >40yrs 15%men, 6%women• Forehead, face, back of hands, bald
scalp of men, and ladies legs• Rough, raised and irregular, like
stuck on cornflakes



Importance
• Marker of sun damaged skin (so BCC/SCC/Melanoma risks all raised)
• Malignant change MAY occur in AK– Quantitative evidence poor– Probably <1/1000– Some remit spontaneously

Treating Actinic Keratoses in primary care
• Why – very common • NICE IOG skin cancer 2006 : Patients with precancerous
lesions may be treated entirely by their GP
Exclusions: Diagnostic uncertainty Thick lesions Indurated or tender base – risk of scc
Lesions in immunosupressed patient

• Do nothing- age/life expectancy/thin lesions• Single or multiple scattered AKs
– Cryotherapy 5-10s FTC - – Curettage & cautery – useful if slight uncertainty/ensure base is
included in histology specimen
– Efudix – 5 flurouracil cream– Solareze – diclofenac 3% ( Bd for 3/12)– Excise if malignancy is suspected
• Thick/tender/indurated/rapid growth
• Multiple AKs/Field change – Efudix secondary care may use imiquimod ( Aldara)
Can use Solareze – less irritant/ less effective
Top up with Li N2 if needed for few residual lesion
AK- Treatment options


How to use Efudix.....
• Topical fluorouracil (5FU) is a topical cytostatic preparation that selectively destroys sun damaged skin cells with little injury to normal skin.
Useful for treating actinic keratoses that occur over a wide area and for Bowens Disease.
Not for very large or thick lesions with an infiltrated base:- refer these to exclude Squamous Cell Carcinoma.

Efudix treatment.......• Apply at night with a finger or cotton-bud.....
• Avoid the eyes, lips and nasolabial folds. Don’t do too much at once!
• Wash off the following morning....
• Apply daily for 2 weeks, unless the skin becomes tender and sore before then. If there is little or no change at 2 weeks then apply twice daily until ...
The skin becomes red, tender and a bit weepy. It may resemble a
superficial burn.
This signals effective treatment and should take 10-28 days. Stop & allow to heal. Review after 1 month.
Early redness with mild stinging is not a sufficient end point!


Treating AK in primary Care
• Look for other skin lesions• Advice re sun protection – 25% of lesions
may regress• Inform patients that they may develop more
lesions and which changes need to be reported
Resources: Efudix leafletsPCDS.org.uk
NED guideline

Solar (Actinic) Keratoses
ALWAYS EXCISE (or refer) IF THICK, INDURATED OR TENDER LESIONS.
• Be careful of causing a leg ulcer by excessive cryotherapy or Efudix on the lower leg
• CUTANEOUS HORNS are better excised or curretted off with a good chunk of base


Cutaneous horn
• Can arise from AK, keratoacanthoma,viral wart or SCC
• Need excising to get histology
• If no induration –could be curretted off with a good scoop of base for histology


Bowen’s disease
• Full thickness dysplasia
• 2-5% chance of developing SCC
• Common lower legs/ hands/ face
• Slow growing sharply demarcated scaly plaque




Treatment of Bowen’s
• Confirm diagnosis with biopsy –may not be necessary if patients have had a previous patch
• Treat efudix, currettage/ cautery• Follow up to check lesion has resolved
Remember if treating lower leg you can cause a leg ulcer

Benign skin lesions

Benign naevi
‘ happy families’

Benign naevi

Seborrheic warts

Dermoscopic appearance seborrhoeic keratosis

Thin seborrhoeic keratosis




Viral warts-use wart paint........

QUIZ
While I’m here Doctor......