Tooth-Implant and Implant Supported Fixed Partial Dentures: A 10
7
Tooth-Implant and Implant Supported Fixed Partial Dentures: A 10-Year Report foban Gunne, LDS, Odont Dt^ Per Ástrand, LDS, Odont Dr'' Tomas Lindb, LDS^ Kennetij Borg, LDS'^ Morgan Olsson, LDS' Purpose: The use of implants for prosthetic rehabilitation of partially edentulous patients is increasing. Ftowever, the possibilities of placing implants in the posterior part of the mandible are often limited. The purpose of thi5 longitudinal study with 10 years of follow-up was to evaluate the use of short implants supporting fixed partial dentures (FPD) in the posterior part of the mandible, and to compare implant supported FPDs to tooth-implant supported FPDs, Materials and Methods: The patient material comprised 23 patients with residual mandibular anierior teeth, and each patient received FPDs unilaterally. On one side the FPD was supported by two implants, and on the other side by one implant and one looth, thus permitting intraindividual comparison. The distribution of the two types of FPDs in each jaw was randomized. Implant success rates, marginal bone changes, and mechanical complications were studied. Results: The tooth- implant connection did not demonstrate any negative influences on the overall success rates for the 10-year period, nor were the shorter implants found to be less favorable. Conclusion: It is suggested that a prosthetic construction supported by hoth a tooth and an implant may be recommended as a predictable and reliable treatment alternative in the posterior mandible, int¡ Prosthodont 1999;!2:216-221. I n the rehabilitation of partially edentulous jaws, implants may be used in two different ways: implant supported fixed partial dentures [FPDl or tooth-im- plant supported FPDs, Implant supported FPDs have 'Professor, Dspartment of ProstbetiQ Oenthtry, Faculty of Odomohgy, Umei University, Unieá, Sweden. ''Head/Chairman, Department oí Oral and Maxiiloiacia! Surgery, UniversiSy Hospital, Linköping, Sweden. ^Asiistam Prolessor, Department of Prosthetic Dentistry, UmeS University, Umei, Sweden. ''Assistant Professor, Department of Oral and Maxilhfacial Surgery, Central Hospital, Skövde, Sweden. Reprint requests: Prof lohan Cunne, Department of Prosthetic Dentiitry, Faculty of Odontoiogy, Umeà University, SÍ-901 87 Umeê, Sweden. Fax: + 46 90 77 .44 60. e-mail: ¡ohan.gunr<[email protected]!rtu.ss been advocated by some authors,'"^ while tooth- implant supported FPDs have been reported to func- tion well by others.**"^ The possible effects on the pe- riodontal membrane of splinting teeth to implants have been elucidated*"'^ and found to have no impact on the abutment teeth. In vitro and in vivo studies have shown that vertical loads applied to tooth- implant supported FPDs can be shared between the tooth and the implant.^"" The risk of stress concen- tration around the implant neck when the implant is connected to teeth has been discussed, but no ad- verse effects of this phenomenon have been docu- mented in clinical studies.^^''^ With the increasing use of implants for prosthetic re- habilitation of partially edentulous patients, place- ment of implants in tbe posterior mandible has become The International loiirral of Proslliodontii 216 Volumelî, Number 3,1999
Transcript of Tooth-Implant and Implant Supported Fixed Partial Dentures: A 10

Tooth-Implant and ImplantSupported Fixed Partial Dentures:
A 10-Year Report
foban Gunne, LDS, Odont Dt^Per Ástrand, LDS, Odont Dr''Tomas Lindb, LDS^Kennetij Borg, LDS'^Morgan Olsson, LDS'
Purpose: The use of implants for prosthetic rehabilitation of partially edentulous patientsis increasing. Ftowever, the possibilities of placing implants in the posterior part of themandible are often limited. The purpose of thi5 longitudinal study with 10 years offollow-up was to evaluate the use of short implants supporting fixed partial dentures(FPD) in the posterior part of the mandible, and to compare implant supported FPDs totooth-implant supported FPDs, Materials and Methods: The patient material comprised23 patients with residual mandibular anierior teeth, and each patient received FPDsunilaterally. On one side the FPD was supported by two implants, and on the other sideby one implant and one looth, thus permitting intraindividual comparison. Thedistribution of the two types of FPDs in each jaw was randomized. Implant success rates,marginal bone changes, and mechanical complications were studied. Results: The tooth-implant connection did not demonstrate any negative influences on the overall successrates for the 10-year period, nor were the shorter implants found to be less favorable.Conclusion: It is suggested that a prosthetic construction supported by hoth a tooth andan implant may be recommended as a predictable and reliable treatment alternative inthe posterior mandible, int¡ Prosthodont 1999;!2:216-221.
In the rehabilitation of partially edentulous jaws,implants may be used in two different ways: implant
supported fixed partial dentures [FPDl or tooth-im-plant supported FPDs, Implant supported FPDs have
'Professor, Dspartment of ProstbetiQ Oenthtry, Faculty ofOdomohgy, Umei University, Unieá, Sweden.''Head/Chairman, Department oí Oral and Maxiiloiacia! Surgery,UniversiSy Hospital, Linköping, Sweden.^Asiistam Prolessor, Department of Prosthetic Dentistry, UmeSUniversity, Umei, Sweden.''Assistant Professor, Department of Oral and Maxilhfacial Surgery,Central Hospital, Skövde, Sweden.
Reprint requests: Prof lohan Cunne, Department of ProstheticDentiitry, Faculty of Odontoiogy, Umeà University, SÍ-901 87Umeê, Sweden. Fax: + 46 90 77 .44 60.e-mail: ¡ohan.gunr<[email protected]!rtu.ss
been advocated by some authors,'"^ while tooth-implant supported FPDs have been reported to func-tion well by others.**"^ The possible effects on the pe-riodontal membrane of splinting teeth to implantshave been elucidated*"'^ and found to have no impacton the abutment teeth. In vitro and in vivo studieshave shown that vertical loads applied to tooth-implant supported FPDs can be shared between thetooth and the implant.^"" The risk of stress concen-tration around the implant neck when the implant isconnected to teeth has been discussed, but no ad-verse effects of this phenomenon have been docu-mented in clinical studies.^^''^
With the increasing use of implants for prosthetic re-habilitation of partially edentulous patients, place-ment of implants in tbe posterior mandible has become
The International loiirral of Proslliodontii 216 Volumelî, Number 3,1999

Gunne et al Tooth-Implant vs Implant Supported Partial Dentures
of interest. The prosthetic alternative in many of thesecases is a removable partial denture, which may be dif-ficult for many patients to accept. The possibility forplacing implants in the posterior part of the mandible,however, is often limited. This means that in most ofthese cases only a few short implants can be used, sug-gesting that a combination of teeth and implants as FPDabutments may be valuable. The possibility of usingtooth-implant connections compared to implant sup-ported FPDs has been studied by the authors.'"^"' Thesame patient pool was used in the present study, whichaimed to evaluate this kind of treatment after 10 yearsof function and to perform this evaluation with specialregard to;
1. Impiant supported versus tooth- implantsupported FPDs
2. Changes in the marginal bone level3. The use of short implants in the posterior part of
the mandible
Materials and Methods
The patient material comprised 23 patients withApplegate-Kennedy Class I residual dentition in themandible and complete maxillary dentures. The pa-tients and the surgical and prosthetic techniqueswere previously presented in detail.'"* The patientswere provided with 2 Brânemark implants (NobelBiocarel in each mandibular quadrant. Because ofthe résorption of the alveolar process and the ioca-tion of the mandibular canal, short implants wereoften used (Table 1). Abutments were connectedafter 4 to 5 months. Each patient was provided with2 types of FPD. On one side the FPD was supportedby 2 implants (FPD type 1) and on the other side bythemostposterior implant and the most distal toothof the residual dentition (FPD type II). The tooth wasprovided with a gold alloy complete crown andwith an acrylic veneer. The other implant on thisside was left as a "sleeping" implant, ie, it was un-connected. The choice of side for the 2 types ofFPDs was randomized, with 4 exceptions. In onecase the potential tooth was root filled and thereforenot considered a suitable abutment, and in 3 casesit was not possible to place more than one implanton one side. The frameworks of the type II FPDswere constructed in 2 parts and connected with aprecision attachment (McCollum T-Attachment,Cendres et Métaux). This attachment was locked andrigidly connected with a horizontal gold screw, andthe construction permitted removal of the FPDs forindividual examinations of both tooth and implantmobility.
Table 1 Implants Placed and Frequency ot Failuresin Type I and II FPDs
Lengtti (mm)
71013Total
No. placed
37293
69
No.
FPD type r
32
6
lost
FPD type II
2
2
%rost
11
14
12"One implant was lost before loading.
At. the 10-year follow-up both clinical and radi-ographie examinations were performed and the fol-lowing variables were recorded:• fPOstaM/fywas defined as lack of clinically de-
tectable mobility and was checked by rocking theFPD back and forth.
• Impiant stabiiity was examined with the FPDs re-moved. In 4 cases where itwas not possible tore-move the FPD, the stability of the implants was es-timated by the stability of the FPD, the conditionof the periimpiant mucosa, and the radiographs.
• Supporting tooth mobility and contralateral toothmobility was estimated with a 4-grade scale thatis commonly used in periodontai registration. Ascore of 0 denoted normal physiologic mobility.
• Bieeding on probing was assessed by pressingthe tip of a probe against the marginal periimpiantmucosa or marginal gingiva at 4 surfaces aroundthe implants or teeth.
• Tightness of gold screws and abutment screwswasexamined by attempting to tighten the screws; therotation of the screwdriver was rated according toKallus and Bessing.''
• Sensory function of the mentai region was as-sessed in patients whtD had previously experi-enced a sensory disturbance. The affected areawas checked by the patient's ability to distinguishbetween a sharp and a blunt instrument.
• Margina/bone/eve/was measured on intraoral ra-diographs, which were exposed using a long conetechnique. The bone level was measured as the dis-tance from a reference point on tbe implant (Fig 1|to the point where tbe marginal bone met the im-plant surface. The measurements were indepen-dently performed by 2 of the authors. If the sepa-rate readings differed, the following procedure wasused to determine a value; if the discrepancy was<0.4 mm, the average of the 2 measurements wasused; if the discrepancy was > 0.5 mm the site wasreviewed again by both observers and consensuswas sought. The differences in marginal bone lossbetween the 2 types of FPDs were tested with theStudent's (test (P< 0.05).
2,Nuniber3, 1999 2 1 7 Ttie Intemational lournal of Pmstfiodontics

Toot il-Implant vs Implan! Supported Partial Dentures Cunne et al
Observation time (y)
1 2 5 10
FPD type IFPD type 11
Table 2 Lifetable Showing Success Rales from 1 to 10 Years
intervai (y)
No otimpiants at
beginning otintervai
No. ottaiied implants
No. ot Success ratewiltidrawn within intervaiimplants (%)
Fig 1 Reference point (arrow)used tor measurements andmarginai bone changes adja-cent to the supporting implantsthroughout the 10-year obser-vation period for Ihe 2 types ofFPDs.
Cumuiativesuccess rate
Betöre loading0-11-22-33-44-55-6e-77-88-99-10
6968646158585852525252
143
98,694.195.3
100100100100100100100100
98.692.888.4 -•88.488.488.48S.488 488.488.488.4
Results
Of the 23 patients, 20 patients attended the 10-yearfollow-up. Two patients had died and one patient,who lived farawayfrom the university clinic, did notwant to participate. Of those patients in whom it hadbeen possible to maintain continuous FPD stability,ail but one were very sati'ified with the treatment. Theexception was a patient who had lost one of the im-plants and also had slight paresthesia in the left men-tal region.
FPD Stability
Because of the implant losses, 4 type I FPDs and 2type II FPDs had been lost at the 5-year examination.The abutment tooth of one of the tooth-implantsupported FPDs had been lost at the 10-year exami-nation because of caries and endodontic complica-tions. The implant, however, was still osseointegratedand gave—with the sleeping implant—support for anewFPD, The FPD stability at the 10-year follow-upwas 80% for type I FPDs and 85% for type II FPDs.
Implant Stability
The initial 2."ï patients had 69 implants placed andloaded. At the 5-year follow-up a total of 8 implantshad been lost. One implant was lost before loading,4 were lost within 6 months after loading, and 3 im-plants were lost between 18 and 24 months afterloading (Table 1). At the 10-year examination no fur-ther losses had occurred and all remaining implantswere found to be stable. In those cases where it wasnot possible to remove the FPDs (3 type I FPDs andone type II FPD), the clinical as well as the radi-ographie examination indicated full stability, givinga cumulative success rate'^ of 88% (Table 2).
Tooth Mobility
In all cases but one the teeth acting as abutment sup-port in the tooth-implant supported FPDs had onlyphysiologicmobility. Asimilar result was found at theexamination of their contralaterals.
The iniern-Hionai Joucriai oí Prosthodoniii 218 Voliiiiie 12, Numbe
Toolti-lmplanI vs Impiant Suppcrted Partial Dentures
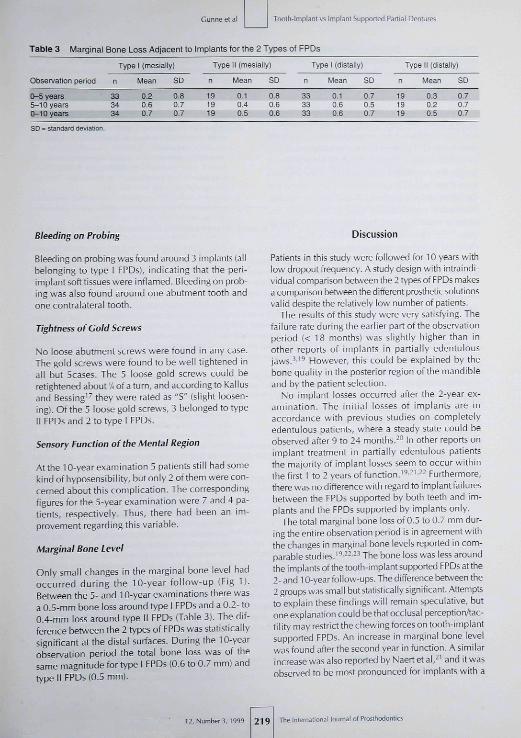
Table 3 Marginal Bone Loss Adjacent to Implants for the 2 Types of FPDs
Observation period
0-5 years5-10 years0-10 years
Type 1 (mesially)
n
333434
Mean
0.20.60.7
SD
0.8070.7
Type
n
191919
11 (mesially)
Mean
0.1040.5
SD
0.80.60.6
n
333333
Type 1 (distally)
Mean
0.10.60.6
SD
0.70.50.7
n
191919
Type II (distally)
Mean
0.30.20.5
SD
0.7070,7
Substandard deviation.
Bleeding on Probing
Bleeding on probing was found around 3 impiants (aiibeionging to type I FPDs), indicating that the peri-impiant soft tissues were infiamed. Bleeding on prob-ing was aiso found around one abutment tooth andone contraiaterai tooth.
Tightness of Cold Screws
No ioose abutment screws were found in any case.The gold screws were found to be weli tightened inaii but 5cases. The 5 ioose goid screws couid beretightened about v; of a turn, and according to Kailusand Bessing'" they were rated as "S" (siight ioosen-¡ng). Of the 5 loose goid screws, 3 belonged to typeii FPDs and 2 to type I FPDs,
Sensory Function of the Mental Region
Atthe 10-year examination 5 patients stiii had somekind of hyposensibiiity, but oniy 2 of them were con-cerned about this compiication. The correspondingfigures for the 5-year examination were 7 and 4 pa-tients, respectiveiy. Thus, there had been an im-provement regarding this variable.
Marginal Bone Level
Only small changes in the marginal bone ievel hadoccurred during the 10-year foliow-up (Fig 1].Between the 5- and 10-year examinations there wasa 0.5-mm bone ioss around type i FPDs and a 0,2- to0.4-mm ioss around type il FPDs (Tabie 3), The dif-ference between the 2 types of FPDs was statisticaiiysignificant at the distai surfaces. During the 10-yearobservation period the totai bone loss was of thesame magnitude for type I FPDs (0,6 to 0.7 mm) andtype II FPDs (0.5 mm).
Discussion
Patients in this study were followed for 10 years withlow dropout frequency, A study design with intraindi-viduai comparison be^veen the 2 types of FPDs makesa comparison between the different prosthetic solutionsvaiid despite the relativeiy iow number of patients.
The resuits of this study were very satisfying, Tbefaiiure rateduring the earlier part of the observationperiod (< 18 months) was siightiy higher than inother reports of impiants in partialiy edentuiousjaws,'-'^ However, this couid be explained by thebone quality in the posterior region of the mandibleand by the patient seiection.
No impiant iosses occurred after the 2-year ex-amination. The initiai iosses of implants are inaccordance with previous studies on compieteiyedentuious patients, where a steady state couid beobser\'ed after 9 to 24 months.-" In other reports onimpiant treatment in partiaiiy edentulous patientsthe majority of impiant iosses seem to occur withinthe first 1 to 2 years of function,' ' '- '-- Furthermore,there was no difference with regard to impiant failuresbetween the FPDs supported by both teeth and im-piants and the FPDs supported by impiants oniy.
The total marginai bone loss of 0.5 to 0.7 mm dur-ing the entire obser\'ation period is in agreement withthe changes in marginai bone levéis reported in com-parable studies.̂ ̂ ---^ The bone ioss was iess aroundthe impiants ofthetooth-implant supported FPDs atthe2- and 10-year foiiow-ups. The difference behveen the2 groups was small but statisticaiiy significant. Attemptsto expiain these findings wiii remain speculative, butoneexpianation couid be that occiusai perceptionAac-tiiity may restrict the chewing forces on tooth-impiantsupported FPDs, An increase in marginai bone ievelwas found after the second year in function, A similarincreasewas also reported by Naert et al,-' and it wasobserved to be most pronounced for implants with a
12, Ngirber3,1999 2 1 9 The Inleiraiional loumal of Prosthodontics

Tooth-implünt vs Impiant Supported Partial Dentures Cunne et al
rigid connection to the natural abutment. From a clin-ical point of view the differences between the 2 typesof FPDsare insignificant. The results indicate that thereis no disadvantage to connecting implants to teeth ina clinical situation like tbe one in the present study.
Short implants have previously been demonstratedto give lower survival rateî than longer implants,^^and 7-mm implants have sometimes been considereddoubtful for FPD abutments. It is interesting to note thatthe success rates reported in this study were achieveddespite the use of short implants (54% of the implantswere 7 mm and 42% were 10 mm; Table 1 ), and thatthefailureratewassimilarfor 7-and 10-mm implants.Mechanical complications, such as fractures of im-plants or retaining screws, have been noted in other re-ports.'̂ -̂ -̂̂ ^ However, in the present study no such me-chanical problems were encountered, with theexception of a few loose gold screws. The problem ofgold screws loosening that are reported elsewhere'''•'^were not experienced in this study. This is interestingbecause the mobility of the teeth could contribute toscrew loosening. The earlier removing and retighten-ing of the gold screws at the 3- and 5-year follow-upsmay have compensated for this.
It has been recommended that at least 3 implants withatripodplacementshould be used to reduce the stresstransferred to the surrounding bone.^•'The lack of fail-ures in this study after the 2-year examination does notsupportthis recommendation because all of the implantsupported FPDs were supported by only 2 implants, andin most cases with a mesial cantilever pontic.
The frequency of persisting disturbances of sensi-bility after 10 years is rather low. Nevertheless, tberisk of this damage to the mental nerve could becompletely avoided by placing only one implant an-terior to the mental foramen and by the use of atooth-implant supported FPD.
Conclusion
After 10 years of function no differences could bedemonstrated between implant supported FPDs andtooth-implant supported FPDs regarding failure ratesor marginal bone level changes. No negative influ-ences on the abutment tooth were observed. Thus,the connection between one implant and one tootbmay be recommended as a predictable and reliabletreatment In addition, this treatment is favorablefrom a cost-benefit point of view and may be supe-riorto an FPD supported by implants alone in someclinical situations.
Acknowledgment
The authors would iike to acknowledge the assistance of Ms EllenLund, Göteborg, Sweden, in the preparation of the manuscript.
References
1. Sullivan DY. Prosthetic considerations for the utilization of os-seointegrated fixtures in the partiaiiy edentulous arch, IntJ OralMaxiilofac Impiants 1986;! :39-45.
2. Naert IE. Prosthetic aspects of implant-supported prostheses. In:Naert I, van Steenberghe D, Worthington P (eds). Osseo.integration in Oral Rehabilitation. Ar Introductory Tei:tbook.Chicago: Quiniessence, 1993:106-122.
3. Schmitt A, Zarb GA.The longitudinal clinical effectiveness of os-seointegrated dental implants in posterior partially edentulouspatients, int j Prosthodont 1993;6:189-196.
4. Ericsson I, Lekhoim U, Brinemark P-I, Lindhe j , Glantz PO,Nyman S. A ciinicai evaluation of fixed-bridge restorations sup-ported by the combination of teeth and osseointegrated titaniumimplants. J Clin Periodontol 198b;13:307-312.
5. Kramer A. Clinical and roentgenological findings and octlusalmeasurements at implants in the free end situation. Oral SurgOral Diag1990;1:11-16.
6. Cavicchia F, Bravi F. Free-starding vs tooth-conneded implant-supported fixed partial restorations: A comparative retrospectiveclinical study of the prosthetic results. Int J Oral MaxillofacImpiant5i994;9:711-7ie,
7. O'Leary TJ, Dykema RW, Kafrawy AH. Spiinting osseointegratedfixtures to teeth with normal periodontjums. In: Laney WR, ToimanDE (edsl. Tissue Integration in Oral, Orthopedic, and ManillofacialReconstruction. Chicago: Quintessence, 1992:48-57.
8. Biancu S, Ericsson I, Lindhe J.The periodontal ligament of teethconnected to osseointegrated implants. An experimental studyin the beagie dog. 1 Clin Periodontoi 1995;22:362-370.
9. Rangert B, Gunne |, Suliivan DV. Mechanical aspects of aBrànemark implant connected to a natural tooth: An in vitrostudy. Int I Oral Maxillofac Implants 1991 ;6:177-186.
10. Rangert B,CunneJ, Giant! PO, Svensson A. Vertical load distri-bution on a three-unit prosthesis supported by a natural tooth anda single Brànemark implant. An in vivo study. Clin Oral Implants
11. Cunne |, Rangert B, Giant; PO, Svensson A. Functional loadson freestanding and connected implants in three-unit mandibu-lar prostheses opposing complete dentures: An in vivo study. IntJOral Maxillofac Implants 1997;12:335-341.
12. Gross M, Laufer BZ. Splinting osseointegrated implants and nat-ural teeth in rehabilitation of partially edentulous patients. Parti:Laboratory and clinical studies. J Oral Rehabil 1997;24:863-870.
13. Laufer BZ, Gross M. Splinting osseointegrated implants and nat-ural teeth in rehabilitation of partially edentulous patients. Parti l : Pnnciples and applications, ] Oral Rehabii 1998;25:69-80.
14. Âstrand P, Borg K, Gunne J, Olsson M. Combination of natural teethand osseointegrated implantsasprosthesibabutments:A2-yearlon-gitudinai study. Int ] Oral Maxillofac Implants 1991 ;6:305-312.
15. CunneJ, Ästrand P, Ahlen K, Borg K, Olsson M, Implants in par-tially edentulous patients: A longitudinal study of bridges sup-ported by both implants and natural teeth. Clin Oral ImplantsResl992;3:49-56.
16. OlssonM,CunneJ, Âstrand P, Borg K. Bridges supported by free-standing implants versus bridges supported by tooth and implant.A five-year prospective study, Clir Oral Implants Res 1995;6:114-121,
The International lournal of Prosthodontic 220 Volume 12, Number 3, 1999

Cunne et al
17. KallusT, BessingC. Loose goW screws frequently occur in full-arch fined prostheîes supported by osseointegrated implantsafter 5 years. Int | Oral Maxiilofac Implants 1994^9:169-178,
18. AlbrektssonT, Zarb GA, Worthington P, Erilisson AR. The long-termefficacy of cunently used dental implants: A review and pnjposedcriteria of success. Int [Oral Maxillofac Implants 1986;1:11-25.
19. Lekholm U, van Steenberghe D, Herrmann I, BolenderC, FolmerT, Cunne ), et al. Osseointegrated implants in the treatment ofpartially edentulous jaws: A prospective 5-year nulticenterstudy. Int ] Oral Masillofac Implants 1994:9:627-635,
20. Adell R, Lekholm U, Rockier B, Brânemark P-l, A 15-year studyof O55eointegrated implants in the treatment of the edentulousja\v, [nt | Oral Surg 1981:10:387-416.
Toolh-lmplant vs Implant Supported Partial Dentures
21. Naeit I, Quirynen M, van Steenberghe D, Darius P. A 5ix-yearpfosthodontic study of 509 coniecutively inserted implants for thetreatmentofpartialedenlulism.lPnjsthetDent 1992:67:236-J45.
22. Quirynen M, Naert I, van Steenberghe D, Dekeyser C, CaltensA. Periodontal aspects of osseointegrated fixtures supporting apartial bridge. An up to 6-years retrospective study. J ClinPeriodontol 1992:19:118-126.
23. JemtT, Lekholm U.Oral implanttreatment in posterior partiallyedentulous jaws: A 5-year follow-up report Int | Oral MaxillofacImplants 1993;8:63 5-640.
34. Rangert B, Krogh P, Lange' B, Van Roekel N. Bending overloadand implant fraCTure: A retrospective clinical analysis. Int J OralMa^illofac Implants 1995,10:326-334.
Literature Abstracts-
Clinlcal outcome of ScrewVent implants. A 7-year prospective follow-up study.
Tfiis study followed up on 31 patents who received 85 ScrewVent implants (Paragon). The iirvplant results were evaluated as proposed by Albrektsson and Zarb using the following classifi-cation: success, survival, unaccounted for, or failure. The implant success rate was 43.5% inthe maxilla and 65,2% in tfie mandible. Implant failures were not related to implant lengths,smoking habits, prosthetic quality, or oral hygiene level. The success witti prosttieses was 18out of 25 in the maxilla and 12 out of 13 in the mandible. From 24 patients witfi 60 implants, ra-diographs were available for marginal bone loss analyses. TTie mean tione loss after 7 yearswas 2,92 mm. Eighteen of the implants (30%) stiowed bone loss beyond the acceptable limit forsuccess (2,7 mm) It was concluded that the ScrewVent implant system does not meet the suc-cess criteria set by the EunDpean Association for Peri odontology. The ongoing bone less mayincrease the risk for future implant failures as well as pedimplant diseases.
De Bruyn H, Collaert B, Linden U. Jofiansson C, Altirektsson T, Clin Ora] Implants Res1999:10:139-148, References: 19. Reprints: Dr Hjgo De ßnjyn. Center tor Perodontology andImpiartology Brüssels, Basilieklaan 373/14,1081 Brüssels, Belgium—SP
Comparison of biting force in different age and sex groups: A study of bKingefficiency with mobile and non-mobile teeth.
It IS generally believeö that a mobile tooth with penodontal disease causes masticatory disad-vantages, Tfiese authors say that it is not clear whether the presence of mobile teeth reducesfuncton; therefore, they conducted this study 11) to investigate tfie influences of sex, age, andnumber of teeth on bitmg pressure, biting force, and occlusal contact area in a descriptive sur-vey, and (2) to compare these 3 variables between the subjects with and without moûile teethin a case-controlled study. A total of 687 volunteers participated (mean age 43 years, range15-99 years), fwlatching procedures with sex, age, and number of teeth were perfomied be-tween 30 subjects with at least one mobile tooth and 30 subjects without any mobile teeth.Results from the descriptive study showed that the biting force and the occlusal contact area inthe males were greater than those in the females. TTie biting pressure increased in subjectswith less than 20 teeth. The brting foroe and the occlusal contact area in subjects with 22 to 23teeUi were halt ot those in the subjects with 28 teeth. Results from fhe case-controlled studyrevealed that the group with mobile teeth had an average of 5 mobile teeth- However, therewere no differences in biting pressure, biting force, and occlusal contact area between thegroups. The conclusion was that the number ot teeth is most important in maintaining bitingability, and mobile teeth do not always reduce it,
Mlyaura K, Matsuka Y, Morllam M. Watanabe T, J OrsI Rehsbin9S9:26.223-227. Relerences: 15.Reprints: Prof Tatsuo Waianatw, Department of Preventive Dentistry, Okayama University Dental ScliOOl,2-5-1 SWkata-cho, Okayama 700-8525, Japan—/IW
H 2 , Number 3,1999 221 The International nal of Prosthodontii