
Tooth eruption and shedding
27
-
Upload
babukancha -
Category
Documents
-
view
161 -
download
14
Transcript of Tooth eruption and shedding


TOOTH ERUPTION AND SHEDDING
Presented by:Shiwani Gupta
Roll.no: 18BDS- 4th year, 1st batch
CONTENTS
• Defination• Pattern of tooth movement• Stages of tooth eruption• Phases of tooth eruption• Types of tooth eruption• Theories of tooth eruption• Teething• Shedding• Mechanism of resorption and shedding• Conclusion• References

ERUPTION• Defined as ‘the movement of tooth from its position within
the jaw to its functional position in an occlusal plane , in vertical/axial direction.
• MAURY MASSLER and SCHOUR(1941) defined eruption as
‘process whereby the forming tooth migrates from its intraosseous location in jaw to its functional position within oral cavity’.
• OSBORNE defined as ‘axial movement of tooth which brings the crown of tooth from its developmental position within bone of the jaw to its functional position in occlusal plane’.
• JAMES K AVERY defined as’ movement of teeth through the bone of the jaws and the overlying mucosa to appear and function in the oral cavity’.
Pattern of tooth movement
• Eruption movement begin with the onset of the root formation.
• Phases can be categorized in 3- phases: phase-1: pre-eruptive phase phase-2: eruptive phase phase-3: post-eruptive phase

Pre- eruptive phase:
• Preparatory to eruptive phase
• Movement of developing tooth germs within alveolar process
• Bodily movement of growing teeth
• Bone resorption and deposition occurs
• Eccentric movement occurs
• Permanent successors develop lingual and near to occlusal level of primary predecessor

Eruptive phase:• Begins with the initiation of root formation and
ends when teeth reach occlusal contact
• Anatomic stages of tooth eruption by NOYES and SCHOUR.
Stage-1: preparatory stage(opening of bony crypt)Stage-2: migration of tooth towards oral epitheliumStage-3: emergence of crown tip into oral
cavity(clinical eruption)Stage-4: first occlusal contactStage-5: full occlusal contactStage-6: continuous eruption

Stages of tooth eruption:Roots begins their formation as a result of proliferation of epithelial root
sheath and mesenchymal tissue of dental papillae and follicle
Erupting teeth moves through bone of crypt and connective tissue of oral mucosa
REE covering crown comes in contact with oral epithelium
REE of crown proliferates and forms a thin attachment with oral epithelium
Tip of crown enter the oral cavity by degenerating the membrane and breaking through center of double layered epithelium

CONT’
Crown erupts further and lateral boarder of oral mucosa now becomes the dentogingival junction
REE now surrounding like a cuff, becomes known as junctional epithelium
Erupting tooth continues to move occlusally as the result of active eruption, exposing more of the clinical crown
Seperation of junctional epithelium from the crown and resulting apical shift of juctional epithelium

Post-eruptive phase:
• Begins when teeth reach occlusion and continues for long as each tooth remains in oral cavity
• Alveolar process increases in height and roots continue to grow
• Occlusion is well established
• Alveolar bone density increases and principle fibers of PDL establish themselves
• Later in life, teeth erupt slightly to compensate for loss of tooth structure
Types of eruption
3- distinct phases:1. Continuously growing: eruptive velocity is rapid
under normal function, increases when wear rate increase or when antagonist is missing.
Eg: incisors of rodents and lyomorphs
2. Continuously extruding: teeth stop forming once root formation is complete. Have well defined crown and root and associated with moderate occlusal wear. Height of clinical crown is maintained by extrusion of tooth.
Eg: cheek teeth of cattle and sheep

3.Continuously invested teeth:• human teeth belong to this type of eruption• Teeth stop forming after a predictable amount of
root development has occurred

Theories of tooth eruption
• Crown are pushed into oral cavity by virtue of growth and elongation of roots
Root elongation theory
• Growth of root dentin and subsequent constriction of pulp causes sufficient pressure to move tooth occlusally
Pulpal constriction theory
• Pulling effect of connective tissue moves teeth in oral cavity
Periodontal growth theory
• Action of cheek and lip musculature upon alveolar process squeezes crown into oral cavity
Pressure from muscular action
• Resorption of alveolar exposes crown to oral cavity
Resorption of alveolar crest
• Hormones secreted by thyroid and pituitary gland governs eruption of teethHormonal theory
• Osmotic pressure and force due to cellular proliferation of pulp and surrounding tissues may account for the eruption of teeth
Cellular proliferation theory
• bony surrounding possess a very rich vascular supply which assist in tooth eruptionVascularity theory
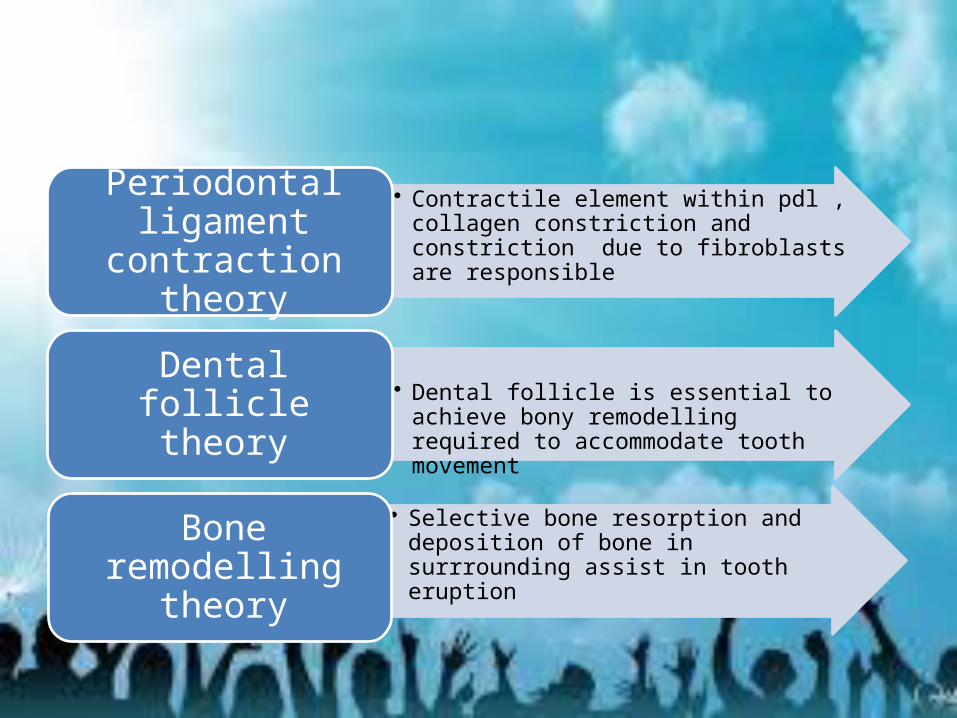
• Contractile element within pdl , collagen constriction and constriction due to fibroblasts are responsible
Periodontal ligament contraction theory
• Dental follicle is essential to achieve bony remodelling required to accommodate tooth movement
Dental follicle theory
• Selective bone resorption and deposition of bone in surrrounding assist in tooth eruptionBone remodelling
theory

Teething
• It is eruption of primary dentition• Local and systemic factors are associated• Begins at 4th-6th month of child’s life
C/F:1. local signs:• swelling of mucosa• Patches of erythema• flushing
2.Systemic signs:• General irritability and crying• Loss of apatite• Sleeplessness, restlessness• Increased salivation• Increased thrust3.Associated problems(systemic):• Fever• Convulsion• Diarrhea• Vomiting• Cholera • Infantile paralysis

Local:• Eruption hematoma• Eruption sequestrum• Ectopic eruption• Transmigration• TranspositionManagement :• Preventive measures• General measures• Medical management• Surgical management

SHEDDING/ERUPTION
• Defined as ‘physiologic process resulting in the elimination of deciduous dentition’.
Pattern of shedding: • Due to progressive resorption of roots of teeth and
their supporting structure.• Pressure due to erupting permanent teeth
Resorption of anterior teeth:• Position of permanent anterior tooth germ is
lingual to apical 1/3rd to root of primary tooth hence resorption is in occluso-labial direction.
• Later crown of permanent tooth lies directly apical to root of primary teeth which leads to horizontal resorption , which causes permanent teeth to erupt in place of primary teeth.

Resorption in posterior teeth:
• Since growing premolars initially are situated between roots of primary molars
• Initiated by resorption of inter-radicular bone followed by adjacent structure
• Alveolar process is growing to compensate for lengthening roots of permanent molars
• Premolars continue to erupt until primary molar roots are entirely resorbed and the teeth exfoliate.
Mechanism of resorption and shedding
• Exact mechanism not known • However 3 attributed reasons are: -loss of root -loss of bone -increased force• KRONFIELD suggest role of stellate reticulum and
dental follicle • Pressure due to growth of permanent teeth
induce differentiation of osteoclast and adontoclast
• Although resorption of teeth is multifocal, but pressure from erupting successional tooth plays key role as odontoclast differentiate at pressure site.
• Forces of mastication are also involved• EVLAMBIA HH demonstrates resorption
involves receptor activator ligand system(RANK), i.e. receptor activator nuclear factor of kappa-B, which stimulates osteoclast formation.
CONCLUSION
• Dental follicle is a loose connective layer that surrounds erupting tooth.
• Follicle is neccesary for tooth eruption.• Special cellular changes occur in and around the follicle
when a tooth erupts.• An eruption pathway is formed around when bone and
roots of deciduous teeth are resorbed.• Events initiated by dental follicle during eruption .• Because tooth eruption depends on dental follicle and
activities around it, studies of follicle may shed some light on eruption mechanism.

References
• TEXT BOOK OF PEDIATRIC DENTISTRY…..3RD EDITION…BY NIKHIL MARWAH
• TEXT BOOK OF PEFDODONTICS…..2ND EDITION…BY SHOBHA TANDON

THANK YOU


















