Today's Dietitian August 2014
68
2014 DIABETES RESOURCE GUIDE The Top 10 Gluten-Free Fast Food Dairy’s Probiotic Prowess Build Your Career via Public Speaking Experts Review US News & World Report ’s Highest-Ranked Diets AADE CONFERENCE ISSUE www.TodaysDietitian.com August 2014 Vol. 16 No. 8 The Magazine for Nutrition Professionals
-
Upload
estee-chan -
Category
Documents
-
view
218 -
download
1
description
Â
Transcript of Today's Dietitian August 2014

2014DIABETES RESOURCE
GUIDE
The Top 10
The Top 10
The Top 10Gluten-Free Fast Food
Dairy’s Probiotic Prowess
Build Your Career via Public Speaking
Experts Review US News & World Report’s Highest-Ranked Diets
AADE CONFERENCE ISSUE
www.TodaysDietitian.com
August 2014
Vol. 16 No. 8
The Magazine for Nutrition Professionals

YUM
CHOLESTEROL FREE
NEWSCIENTIFIC STUDIES
8% DV FIBER PER 1-OZ. SERVING
NATURALLY GOOD FATS
Ex: AVOCADOId: HASSW: 232gLin: 1/1
Id:BRM/Lin:BRM3/Id:14372
w:1825 L:3244
Ex:2251897
The next time your clients need a fresh source of naturally good monounsaturated fats, recommend an avocado. Learn more about avocado nutrition and see the results of recent avocado studies at LoveOneToday.com.
naturally good fats cholesterol free© 2014 Hass Avocado Board. All rights reserved.
NATURALLY
DATE: 3.17.14 CLIENT: HASS TRIM SIZE: 8" x 10.5" APPROVAL INITIAL/DATE/TIME APPROVAL INITIAL/DATE/TIME
FILE NAME: HAB130410 PREPARED BY: Mollie LIVE SIZE: 7.25 x 10” 1 ART DIRECTOR 4 PROD. MGR
PUB/ISSUE: Today’s Dietitian April INTERNAL ROUND: R1 BLEED SIZE: +.25" 2 COPYWRITER 5 PROJ. MGR
FILE TYPE: INDD CS CLIENT ROUND: Final LASER SCALE: 100% 3 COPYEDITOR 6 ACCOUNT MGR
NOTES:
HAB140410_HealthProf_Ad_TodaysDietitian_Apr.indd 1 3/17/14 4:08 PM

Client: Domino Job #: DM2013-1253 Ad #: DOM-2171Media: Todays Dietitian Issue: Aug 14 Ad Size: live: 7.25x10; trim: 8x10.5; bleed: 8.5x11
THIS ADVERTISEMENT PREPARED BY enCore
©20
14 D
om
ino
Fo
od
s, In
c.
dominosugar.com/light | chsugar.com/light
Bake favorite recipes with fewercalories and carbohydrates.
Try packets for easy Sprinklingor to Stir into beverages.
Enjoy a delicious sweet taste andno artificial ingredients fromthe makers of Domino® Sugarand C&H® Sugar.
Combining two ofNature’s Sweeteners.
Real WaySweet!
theto do
TM
1253 Green Light_COMBO_2171_Spec 7/16/14 4:16 PM Page 1

Fonts » Archer (Book, Bold Italic, Medium, Bold), Chocolate Amargo (Regular)
Images » ItalianTomatoes_HerbedCottageCheese_Toast_InkLimit.psd (CMYK; 577 ppi; 51.93%),
GettyImages_Granola_121878340_Retouched.psd (CMYK; 784 ppi; 38.23%), GettyImag-
es_102374527_Flat_Large.psd (CMYK; 4310 ppi; 6.96%), 102518293_22_rev2Red_CMYK_In-
kLimit.psd (CMYK; 2834 ppi; 10.58%), Spinach_f.psd (CMYK; 2911 ppi; 10.31%), Tomatoes_f.
psd (CMYK; 2615 ppi; 11.47%), GettyImages_Walnuts_88257144_CMYK.psd (CMYK; 951
ppi; 31.54%), Correct Kiwi Image_Retouched.psd (CMYK; 1858 ppi; 16.14%), DaisyCC_
Duo_2per_16oz24oz_MixedBerries_R2.psd (CMYK; 2206 ppi; 13.59%)
Inks » 4C Cyan, Magenta, Yellow, Black
9468_Ad_TodaysDietation_April_RUN.indd R
JobClient
Media Type
BleedTrimLive
Publication
Creative DirectorDesigner
Account ManagerStudio Artist
Print ProductionProofreader
9468Daisy
None
8.5” x 11”8” x 10.5”7.25” x 10”
Today’s Dietition
Brad JunglesNoneRae Ann FischMichael SchultzNoneAll
Notes » None
JOB INFO FONTS & IMAGESAPPROVAL & NOTES
SAVED 3-18-2014 1:14 PM | BY Mike Schultz | PREVIOUSLY BY Mike Schultz | FILES SENT VIA None » Contact Rae Ann Fisch · (816) 423-6196 · [email protected] ROUND
References: 1. Leidy HJ, Armstrong CL, Tang M, Mattes RD, Campbell WW: The infl uence of higher protein intake and greater eating frequency on appetite control in overweight and obese men. Obesity (Silver Spring) 2010, 18:1725–1732.2. Purslow LR, et al. Energy intake at breakfast and weight change: Prospective study of 6,764 middle-aged men and women. American Journal of Epidemiology. 2008;167:1883. Kant AK, et al. Association of breakfast energy density with diet quality and body mass index in American adults: National Health and Nutrition Examination Surveys, 1999-2004. American Journal of Clinical Nutrition. 2008;88:1396.
to the healthy foods you already recommend.Add Daisy
DISCOVER THE BENEFITS THAT COME WITH NUTRITION AND TASTE.
Maximize Muscle SynthesisEncourage your patients and clients to make the most of their protein consumption. Studies show that consuming 20 to 30 grams of protein at each meal—instead of one large meal high in protein—can maximize muscle synthesis, which is critical for everyone.1
Stay On TrackResearch suggests that when people eat breakfast, they tend to eat a healthier overall diet, one that is more nutritious and lower in fat.2,3 Part of this means starting the day with a breakfast high in protein. Daisy Low Fat Cottage Cheese has 13 grams of satisfying protein and 4 grams of carbs per 90 calorie ½ cup serving. A meal high in protein and low in calories and carbohydrates will promote satiety and regulate blood sugar levels.
Variety – The Spice of LifeCottage cheese is so convenient and versatile; you can enjoy it for breakfast, lunch, dinner or a snack. Pair it with fruits, vegetables, nuts or whole grains, or use as an ingredient in favorite recipes, such as lasagna, for a healthier spin. Eating healthy doesn’t need to be complicated or boring.
Power the Day with Daisy
Better Ingredients: That’s the Daisy Di� erenceDaisy Low Fat Cottage Cheese is made with 4 high quality ingredients—no additives, thickeners or preservatives. Look for our new packaging with colored lids.
Add Daisy
S:7.25”S:10”
T:8”T:10.5”
B:8.5”B:11”

EDITOR’S SPOT
President & CEO Kathleen Czermanski
Vice President & COO Mara E. Honicker
EDITORIALEditor Judith Riddle
Editorial Director Jim Knaub Senior Production Editor Tracy Denninger
Editorial Assistants Heather Hogstrom, Leesha LentzContributing Editor Sharon Palmer, RD
Editorial Advisory Board Dina Aronson, RD; Jenna A. Bell, PhD, RD; Janet Bond Brill, PhD, RD, CSSD, LDN; Marlisa Brown, MS, RD, CDE, CDN;
Constance Brown-Riggs, MSEd, RD, CDE, CDN; Carol Meerschaert, MBA, RD; Sharon Palmer, RD;
Christin L. Seher, MS, RD, LD
ARTArt Director Charles Slack
Graphic Designer Erin ProsiniJunior Graphic Designer Victoria Tuturice
ADMINISTRATIONAdministrative Manager Helen Bommarito
Administrative Assistants Pat Plumley, Susan YanulevichExecutive Assistant Matt Czermanski
Systems Manager Jeff CzermanskiSystems Consultant Mike Davey
FINANCEDirector of Finance Jeff Czermanski
CONTINUING EDUCATIONDirector of Continuing Education Jack Graham
Continuing Education Editor Kate Jackson Continuing Education Coordinator Leara Angello
Continuing Education Assistant Susan Graver
CIRCULATIONCirculation Manager Nicole Hunchar
MARKETING AND ADVERTISINGPublisher Mara E. Honicker
Director of Marketing and Digital Media Jason Frenchman Web Designer/Marketing Assistant Jessica McGurk
Marketing Coordinator Leara AngelloSales Manager Brian Ohl
Associate Sales Manager Peter J. BurkeSenior Account Executives Sue Aldinger, Gigi Grillot,
Diana Kempster, Beth VanOstenbridgeAccount Executives Victor Ciervo, Dan Healey, Patricia McLaughlin
Sales Coordinator Joe Reilly
© 2014 Great Valley Publishing Company, Inc.
Phone: 610-948-9500 Fax: 610-948-7202Editorial e-mail: [email protected] Sales e-mail: [email protected]
Website: www.TodaysDietitian.com Subscription e-mail: [email protected]
Ad fax: 610-948-4202 Ad artwork e-mail: [email protected]
All articles contained in Today’s Dietitian, including letters to the editor, reviews, and editorials, represent the opinions of the authors, not those of Great Valley Publishing Company, Inc. or any organizations
with which the authors may be affiliated. Great Valley Publishing Company, Inc., its editors, and its editorial advisors do not assume
responsibility for opinions expressed by the authors or individuals quoted in the magazine, for the accuracy of material submitted by the authors, or for any injury to persons or property resulting from reference to ideas or
products discussed in the editorial copy or the advertisements.
Judy
CAN WE ALL GET ALONG? In June, the Centers for Medicare & Medicaid Services (CMS) issued a landmark ruling stating that qualified dietitians or nutrition professionals may order all patient diets, including therapeutic diets, in hospitals as authorized by the medical staff and in accordance with state law.
The ruling doesn’t specify which qualified nutrition professionals may provide the same hospital services as RDs. However, because the Board for Certification of Nutri-tion Specialists (BCNS) was instrumental in changing the draft language in the proposed rule to include all “qualified nutrition professionals,” including certified nutrition specialists (CNSs), RDs have begun scrutinizing the CNS credential.
When Today’s Dietitian posted the news about the ruling from the BCNS on its Facebook wall, comments poured in. A few RDs supported the ruling, stating that CNSs are just as qualified as they are. Others rejected the ruling, claiming it undermines and devalues the RD credential, that it renders the RD degree worth-less and dietetic internships purposeless. Some commenters feared for the future of RDs in hospitals.
To obtain the CNS credential, you must have at least a master of science or doctoral degree in the nutrition or clinical health field; complete coursework in nutrition, biochemistry, physiol-ogy or anatomy/physiology, and the clinical health sciences at an accredited university; complete 1,000 hours of supervised practical experience in nutrition; and pass an exam. For the RD credential, you must have at least a bachelor’s degree and com-plete a dietetic internship from an accredited university, com-plete 1,200 hours of supervised practice experience in nutrition, and pass an exam.
A CNS requires more education than an RD. However, many RDs have master’s and doctoral degrees plus other specialized certifications. To be sure, RDs have the right to question whether lesser-qualified nutrition professionals with fewer years of edu-cation and practice experience should offer the same hospital services, but should we argue about who’s more qualified and worry about job security or should we simply accept one another as colleagues and try to get along? Stay tuned for more in-depth coverage of this controversial ruling in an upcoming issue of Today’s Dietitian.
In light of the American Association of Diabetes Educators Annual Meeting and Exhibition, this month’s issue features special diabetes coverage on US News & World Report’s top 10 diets for patients and strategies for overcoming weight loss challenges. See you in Orlando!
Judith [email protected]
august 2014 www.todaysdietitian.com 5

FEATURES
22 The Top 10 Diabetes Meal Patterns Nutrition professionals review US News & World Report’s highest-ranked diets for clients and patients.
28 Gluten-Free Fast Food Many fast-food chains are offering gluten-free menus, but there are some important things clients and patients must know before chowing down.
32 Dairy’s Probiotic Power Here’s a review of the benefits of probiotics, the top sources, and what’s new in the dairy case.
38 Building a Career Through Public Speaking RDs discuss what it takes to get started, how to set goals, and the importance of choosing a specialty for long-term success.
42 CPE Monthly: Caring for Today’s Cancer Survivors This continuing education course focuses on cancer survivors’ nutrition-related issues following the conclusion of active cancer treatment.
DEPARTMENTS
5 Editor’s Spot
7 Reader Feedback
8 Ask the Expert
10 Health Matters
12 Conference Currents
14 Dynamics of Diabetes
17 Vegetarian Nutrition
20 Supplement Spotlight
49 Personal Computing
50 Focus on Fitness
52 Get to Know…�
54 Diabetes Resource Guide
55 News Bites
58 Bookshelf
60 Products + Services
62 Research Briefs
64 Summer Product Showcase
65 Datebook
66 Culinary Corner
CONTENTS AUGUST 2014
Today’s Dietitian (Print ISSN: 1540-4269, Online ISSN: 2169-7906) is published monthly by Great Valley Publishing Company, Inc., 3801 Schuylkill Road, Spring City, PA 19475. Periodicals postage paid at Spring City, PA, Post Office and other mailing offices. Permission to reprint may be obtained from the publisher. REPRINTS: The Reprint Outsource, Inc.: 877-394-7350 or e-mail [email protected] NOTE: For subscription changes of address, please write to Today’s Dietitian, 3801 Schuylkill Road, Spring City, PA 19475. Changes of address will not be accepted over the telephone. Allow six weeks for a change of address or new subscriptions. Please provide both new and old addresses as printed on last label. POSTMASTER: Send address changes to Today’s Dietitian, 3801 Schuylkill Road, Spring City, PA 19475. Subscription Rates — Domestic: $14.99 per year; Canada: $48 per year; Foreign: $95 per year; Single issue: $5. Today’s Dietitian Volume 16, Number 8.
Page 42
1432

READER FEEDBACK
From Our Twitter Page Popular Tweets, Retweets
June Issue
@nutrinotions: Got my new edition! Every article is spot on. Can’t wait to read more!
“Men in Dietetics”
@DropBarDarcy: As an RD, I appreciated the Men’s Health Month June edition. Male dietitians are on the up and coming!
“Athletes and Protein Intake”
@kimsteinRD: You need protein to build/repair muscle and carbs to fuel. Great article on protein intake.
@Eat_Pray_Run: Great article on the latest talk about protein.
“Exercise During Pregnancy” (Focus on Fitness)
@CuseSportsRD: So important yet so under- emphasized.
“Grilling Tips” (Ask the Expert)
@jenhaugen: Great grilling tips, Toby Amidor! Essential for a safe summer!
@BeefRD: Just in time for summer!
“Rising CO2 Poses Significant Threat to Human Nutrition” (Research Brief)
@EmmaJaneRD: Great to see impact of increased CO2 climate change on food production being raised by Today’s Dietitian; risk of micronutrient deficiencies.
From Our Facebook Wall
“A Pill for Celiac Disease Is Almost Here”www.huffingtonpost.com
Calli Leigh: I think it would help the accidental harm of gluten intake for people who have celiac disease. People who think they have a gluten intolerance might abuse it, though.Chelsea Johns: While I think it would be incredible for children with celiac disease to feel they can eat the “normal” food that everyone else is eating, I’m afraid it may authorize people who switched to eating nutrient-dense, gluten-free foods (fruits, veggies, etc) to go back to nutrient-poor foods like sugary breakfast cereal, prepackaged cookies, etc.
“8 Things Nutrition Experts Wish You Would Stop Saying About Food”www.huffingtonpost.com
Karl ’n Cheryl Flanagan: Yes! Although I do believe there’s a need for the label “bad foods,” but it should be given to bad foodlike substances.
“Growing Up on Raw Foods”www.nytimes.com
Susan Macfarlane: The first thing I would ask is why are you following a raw diet and what’s the message you’re trying to send? As a vegan myself, I completely support families who want to choose a vegan diet for ethical, environmental, health, or a combination of the three reasons. However, I think that only eating raw (which generally excludes all animal products by default) may lead to a distorted relationship with food, similar to orthorexia. I do see the benefits of consuming some foods in their raw form, since cooking does destroy heat-sensitive nutrients, however, cooking also can enhance the nutrition of the food, as is the case with cooked spinach. I also disagree that a diet that requires supplementation is inherently unhealthful. Here in Canada, it’s difficult to meet our vitamin D requirements, thus essentially all Canadians require supplementation. This doesn’t mean that whatever diet we’re following is necessarily unhealthful.
June 2014
Vol. 16 No. 6
The Magazine for Nutrition Professionals
CONFERENCE ISSUE
5 Summer Foodservice Programs for Kids
Dairy’s Value in Disease Prevention
MEN’S HEALTH MONTH
FEATURING
Men in Dietetics
Men’s Fitness
INSIDEGluten-Free Showcase
AthletesProtein Intake
and
Experts Discuss Whether the RDA Is Adequate
www.TodaysDietitian.com
august 2014 www.todaysdietitian.com 7

Scientifi c studies have shown that Almased® can help maintain healthy blood sugar levels as well as the equally important leptin level. It was also suggested
that Almased can help maintain healthy blood levels for body compounds such as cholesterol.
Almased® is an all-natural powder made from high-quality non-GMO soy, yogurt and enzyme-rich honey. It is made in a unique fermentation process, is gluten-free and rich in essential amino acids. The product does not contain artifi cial fi llers, fl avors, added sugars, preservatives or stim-ulants. Almased® has a low glycemic index (27) and extreme-ly low glycemic load (4) and is diabetic friendly. The renowned Joslin Diabetes Center suggests that a carb controlled diet consists of approximately 40% carbohydrates, 30% fat and 30% protein. The Almased® Diet provides this recommended mix of micronutrients.
The Weight Loss Phenomenon with scientifi c
results
Help your clients succeed with their weight loss goalAn all-natural weight loss system which also helps to maintain healthy blood sugar levels Catarsha
Atkins lost 75 lbs with Almased®!
before
Read Catarsha’s story and more at
www.almased.com.
Order these FREE brochures for you and your clients.
Download the Almased® Figure Plan and other brochures at www.fi gureplan.com.Enter Source Code TD1.
You can fi nd Almased® in health food stores and nationwide at GNC and the Vitamin Shoppe.
Ask our nutritionist
We off er comprehensive information packages for health care professionals and clients. In addition, our nutritionist Silke Ullmann, MPH, RD, is available to assist you and your clients with advice and more detailed information. Email her at [email protected].
Today’s Dietitian Aug ad_03.indd 1 23.06.14 09:41
TEXT MESSAGING FOR HEALTHBy Toby Amidor, MS, RD, CDN
Q:Has texting ever been shown to be an effective nutrition education tool?
A: In today’s society, cell phones are a mainstream way of communicating. As such, many are focusing their atten-
tion on the use of texting as a means of providing nutrition education. Several successful mobile information services have been designed to promote healthful eating through text messaging, including Text2BHealthy and Text4baby.
Text2BHealthyText2BHealthy was developed by the University of Maryland
Food Supplement Nutrition Education program and implemented this year in 19 schools across Maryland where more than 2,600 parents enrolled, reaching on average about 25% of the parent population at participating schools.
Text2BHealthy recognizes that parents play an important role in the development of their children’s eating patterns and physical activity. The program provides two targeted messages per week to parents that act as actionable “nudges” about how they can be positive role models by eating healthier foods and becoming more physically active. Parents also receive nutrition information that connects what their children have been learning in the classroom with tips and ideas on implementing healthful eating behaviors at home. A sample text message would read, “This week is MSA testing week at Barclay Elementary. Make sure your child eats breakfast. A healthy start to the day will help them do well in school.”
“We can educate the kids, but if we’re not educating their caregivers who provide for the kids, how likely will changes be made in the home?” says Joni Garcia, MS, RD, program integrity team lead at the USDA Food and Nutrition Service Mid-Atlantic Regional Office. “Text2BHealthy aims to reach this population and communicate with them in a way that meets the needs of their busy schedules. It meets them where they are.”
Results from the Text2BHealthy evaluation found that close to 40% of Text2BHealthy parents are eating fruits and
vegetables as snacks more often at the end of the year than they were at the beginning, and 74% of parents now are eating fruits and vegetables as snacks often or every day. Moreover, 52% of Text2BHealthy parents report eating two or more vegetables at their main meal often or every day, and 47% of parents say their child is doing the same.
Text4babyText4baby is a free service offered through National
Healthy Mothers, Healthy Babies Coalition and is supported and promoted by more than 1,200 health departments, academic institutions, health plans, businesses, and the federal government. Participants are sent more than 250 messages containing the most critical information that experts want pregnant women and moms with infants aged younger than 12 months to know. Messages address issues such as breast-feeding, nutrition, exercise, prenatal care, and oral health. A sample text message for pregnant women would read, “Morning sickness may be caused by a change in your hormones. Try eating crackers or dry cereal. Eat small meals often. Don’t go without eating.”
An evaluation of the Text4baby program found that 74% of total respondents said Text4baby messages informed them of medical warning signs they didn’t know.1
Future of Nutrition EducationWith texting and cell phones being the major means of
communication, nutrition professionals need to evolve their education techniques to meet with modern times. “Texting and other nontraditional ways of providing information, such as social media, is the future of communication and education,” Garcia says. “Nutrition professionals working with the public need to be exploring these avenues for providing information because that’s our future.”
— Toby Amidor, MS, RD, CDN, is the founder of Toby Amidor Nutrition
(http://tobyamidornutrition.com) and the author of the cookbook The Greek Yogurt Kitchen. She’s also a nutrition
expert for FoodNetwork.com and contributor to US News Eat + Run.
Reference1. Hoff A, Nunez-Alvarez A, Martinez KM, Lacoursiere DY.
Maternal and newborn health: Text4baby San Diego evaluation overview: October 2011-October 2012.
ASK THE EXPERT
Have questions about nutrition trends, patient care, and other dietetics issues you’d like to ask our expert?
Send your questions to Ask the Expert at [email protected] or send a tweet to @tobyamidor.
8 today’s dietitian august 2014

Scientifi c studies have shown that Almased® can help maintain healthy blood sugar levels as well as the equally important leptin level. It was also suggested
that Almased can help maintain healthy blood levels for body compounds such as cholesterol.
Almased® is an all-natural powder made from high-quality non-GMO soy, yogurt and enzyme-rich honey. It is made in a unique fermentation process, is gluten-free and rich in essential amino acids. The product does not contain artifi cial fi llers, fl avors, added sugars, preservatives or stim-ulants. Almased® has a low glycemic index (27) and extreme-ly low glycemic load (4) and is diabetic friendly. The renowned Joslin Diabetes Center suggests that a carb controlled diet consists of approximately 40% carbohydrates, 30% fat and 30% protein. The Almased® Diet provides this recommended mix of micronutrients.
The Weight Loss Phenomenon with scientifi c
results
Help your clients succeed with their weight loss goalAn all-natural weight loss system which also helps to maintain healthy blood sugar levels Catarsha
Atkins lost 75 lbs with Almased®!
before
Read Catarsha’s story and more at
www.almased.com.
Order these FREE brochures for you and your clients.
Download the Almased® Figure Plan and other brochures at www.fi gureplan.com.Enter Source Code TD1.
You can fi nd Almased® in health food stores and nationwide at GNC and the Vitamin Shoppe.
Ask our nutritionist
We off er comprehensive information packages for health care professionals and clients. In addition, our nutritionist Silke Ullmann, MPH, RD, is available to assist you and your clients with advice and more detailed information. Email her at [email protected].
Today’s Dietitian Aug ad_03.indd 1 23.06.14 09:41
Sponsored Content

Fish Oil May Benefit Those Who Abuse Alcohol
Omega-3 fish oil may help protect against alcohol-related neuro-damage and the risk of eventual dementia, according to a study pub-lished in PLOS ONE.
Many human studies have shown that long-term alcohol abuse causes brain damage and increases the risk of dementia. The new study found that in brain cells exposed to high levels of alcohol, a fish oil compound protected against inflammation and neuronal cell death.
The study was conducted by Michael A. Collins, PhD; Edward J. Neafsey, PhD; colleagues at Loyola University Chicago Stritch School of Medicine; and collaborators at the University of Kentucky and the National Institute on Alcohol Abuse and Alcoholism.
Collins and colleagues exposed cultures of adult rat brain cells over several days to concentrations of alcohol equivalent to about four times
the legal limit for driving—a concentration seen in chronic alcoholics. These brain cultures were compared with cultures exposed to the same high levels of alcohol, plus DHA. Researchers found there was up to 90% less neuroinflammation and neuronal death in the brain cells exposed to alcohol plus DHA than in the cells exposed to alcohol alone.
An earlier meta-analysis by Collins and Neafsey, which pooled the results of about 75 studies, found that moderate social drinking may have the opposite effect of reducing the risk of dementia and/or cognitive impairment during aging. (Moderate drinking is defined as a maximum of two drinks per day for men and one drink per day for women.)
It appears that limited amounts of alcohol may, in effect, make brain cells more fit. Alcohol in moderate amounts stresses cells and thus toughens them to cope with major stresses that could cause dementia. But too much alcohol overwhelms the cells, leading to neuroinflammation and cell death.
Further studies are needed to confirm whether fish oil protects against alcohol-related cognitive injury and dementia in adult rodent models. “Fish oil has the potential of helping preserve brain integrity in chronic alcohol abusers,” Collins says. “At the very least, it’s unlikely that it would hurt them.”
But he adds that the best way for an alcohol abuser to protect the brain is to cut back to low or moderate amounts or quit entirely. “We don’t want people to think it’s OK to take a few fish oil capsules and then continue to go on abusing alcohol,” he says.— SOURCE: LOYOLA UNIVERSITY HEALTH SYSTEM
HEALTH MATTERS
Having Fun While Exercising Decreases AppetiteIf you’re looking to lose weight, think of your next workout
as a fun activity or as a well-deserved break, not exercise, and you’ll eat less and lose more weight, according to a new study from Cornell University Food and Brand Lab.
Published in Marketing Letters, the new study analyzed the eating habits of people after walking 2 km (roughly 1.2 miles). One-half of the participants were told the walk was exercise, while the others were told it was a scenic walk. Researchers found that those who believed they com-pleted an exercise walk ate 35% more chocolate pudding for dessert than those who had been on a scenic walk. On a different occasion, those thinking they had taken an exercise walk ate 206 (124%) more calories than those
who had been told they were on a scenic walk.According to researchers, the study shows one reason
why people in new exercise programs often find themselves gaining weight: New exercisers have a tendency to reward themselves by overeating after their workout.
For beginning or veteran exercisers, the bottom line is to “do whatever you can to make your workout fun. Play music, watch a video, or simply be grateful that you’re working out instead of working in the office,” says Brian Wansink, PhD, director of the Cornell Food and Brand Lab. “Anything that brings a smile is likely to get you to eat less.”— SOURCE: CORNELL UNIVERSITY
10 today’s dietitian august 2014

Caffeine Intake May Worsen Menopausal Hot FlashesA new Mayo Clinic study, published online ahead of
print in Menopause, found an association between caffeine intake and more bothersome hot flashes and night sweats in postmenopausal women. The study also showed an association between caffeine intake and fewer problems with mood, memory, and concentration in perimenopausal women, possibly because caffeine is known to enhance arousal, mood, and attention.
For the study, researchers conducted a survey using the Menopause Health Questionnaire, a comprehensive assessment of menopause-related health information that includes personal habits and ratings of menopausal symptom presence and severity. Questionnaires were completed by 2,507 consecutive women who presented with menopausal concerns at the Women’s Health Clinic at Mayo Clinic in Rochester, Minnesota, between July 25, 2005, and July 25, 2011. Data from 1,806 women who met all inclusion criteria were analyzed. Menopausal symptom ratings were compared between caffeine users and nonusers.
Vasomotor symptoms (hot flashes and night sweats) are the most commonly reported menopausal symptoms, occurring in 79% of perimenopausal women and 65% of postmenopausal women. Although it has long been believed
that caffeine intake exacerbates vasomotor symptoms, research has challenged this assumption, as caffeine has been both positively and negatively linked to hot flashes.
“While these findings are preliminary, our study suggests that limiting caffeine intake may be useful for those post-menopausal women who have bothersome hot flashes and night sweats,” says Stephanie Faubion, MD, director of the Women’s Health Clinic. “Menopause symptoms can be chal-lenging, but there are many management strategies to try.”
Faubion recommends the following strategies:• Be aware of triggers such as spicy foods and hot beverages. • In addition to caffeine, limit alcohol and tobacco.•Dress in layers, so you can remove a layer when
you’re warm.•Consider products to stay cool at night, such as wicking
sheets and sleepwear, fans, and cooling pillows.•Try stress management strategies such as meditation,
yoga, tai chi, acupuncture, and massage. •Maintain a healthy weight and exercise regularly.•Talk with your provider about hormone therapy and
nonhormonal prescription medications to alleviate symptoms.
— SOURCE: MAYO CLINIC
Vitamin D Deficiency Raises Risk of Schizophrenia DiagnosisVitamin D–deficient individuals are twice as likely to be
diagnosed with schizophrenia as people who have sufficient levels of the vitamin, according to a study published in the Journal of Clinical Endocrinology & Metabolism.
Vitamin D helps the body absorb calcium and is needed for bone and muscle health. The skin naturally produces this vitamin after exposure to sunlight. People also obtain smaller amounts of the vitamin through foods, such as milk fortified with vitamin D. More than 1 billion people worldwide are estimated to have deficient levels of vitamin D due to limited sunshine exposure.
Schizophrenia is a mental illness with symptoms that can include delusions and hallucinations. Since schizophrenia is more prevalent in high latitudes and cold climates, researchers have theorized vitamin D may be connected to the disorder.
“This is the first comprehensive meta-analysis to study the relationship between the two conditions,” says study author Ahmad Esmaillzadeh, PhD, of the Isfahan University of Medical Sciences in Iran. “When we examined the findings of several observational studies on vitamin D and schizophrenia, we found people with schizophrenia have lower vitamin D levels than healthy people. Vitamin D deficiency is quite common among people with schizophrenia.”
The researchers reviewed the findings of 19 observational studies that assessed the link between vitamin D and schizo-phrenia. Combined, the studies looked at vitamin D levels and the mental health of 2,804 adult participants. The studies used blood tests to determine each participant’s vitamin D levels.
The meta-analysis found that people with schizophrenia had significantly lower levels of vitamin D in the blood compared with the control groups. The average difference in vitamin D levels between schizophrenic patients and control participants was -5.91 ng/mL. People with vitamin D deficiency were 2.16 times more likely to have schizophrenia than those with sufficient vitamin D in their bloodstreams. In addition, 65% of the participants who had schizophrenia also were vitamin D deficient.
“There’s a growing trend in the nutrition science field to consider vitamin D and its relationship to conditions such as diabetes, cancer, heart disease, and depression,” Esmaillzadeh says. “Our findings support the theory that vitamin D may have a significant impact on psychiatric health. More research is needed to determine how the growing problem of vitamin D deficiency may be affecting our overall health.”— SOURCE: ENDOCRINE SOCIETY
august 2014 www.todaysdietitian.com 11

SOLVING FOOD INSECURITYBy Beth W. OrensteinDietitians have the resources to end hunger and obesity in their communities.
How can children be both hungry and overweight? Not only is this possible, but it’s happening all too frequently in America, Glenna McCollum, DMOL, MPH, RDN, now past president of the Academy of Nutrition and Dietetics, told members of the Pennsylvania Academy at their annual meeting in Bethlehem, Pennsylvania, in April. “In our country, far too many children and families are struggling with food insecurity,” she said in delivering the Anna DePlanter Bowes Lecture.
The USDA defines food insecurity as lack of access to enough food for an active, healthful life and indicates that, as of 2012, 49 million Americans suffer from it. Of those, 16 million are children under the age of 18. At the same time, 23 million chil-dren are overweight or obese.
Food insecurity is the highest among minority households, as members of black and Hispanic households are twice as likely as those in white households to be food insecure, McCollum said. Location also plays a role, with food insecurity being high-est in the South (16%) and West (15.8%). Though the rates are slightly lower in the Northeast and Midwest (13.5%), the figure still is high, she said.
And while food insecurity hasn’t gotten much worse in recent years, it hasn’t gotten much better, either, McCollum continued.
Poor Eating Habits Children can be both hungry and over-
weight or obese because they lack access to foods that are nutrient dense—foods that dietitians would recommend children eat. “Healthy foods can be more expensive than calorie-dense foods,” McCollum explained. “Research shows that food-insecure par-ents report that the price of fruits and vegetables are too high.”
Also, food-insecure parents have less access to quality food in their neighborhoods. “They may also lack transportation to make more affordable food purchases at larger grocery stores,” McCollum said. Their readily available food choices in corner markets may leave them and their children at risk of being overweight or obese.
Additionally, when home pantries are full, children may have regular and healthful
diets, McCollum said, but when pantries are empty, often at the end of the month when food dollars are stretched, diets may be lacking or meals may be skipped. This inconsistency in eating patterns can cause changes in metabolism that promote fat storage and weight gain, she said.
Children and parents in food-insecure homes also have high levels of stress related to issues such as finances, employment, health care, and housing. The stress, anxiety, and depression can result in poor food choices and lead to weight gain, McCollum said, noting that obesity needs to be addressed in childhood. Studies have shown that few school-age children can outgrow their weight problems. “The probability that an overweight school-age child will become an obese adult is over 50%,” she said. “An overweight adolescent has a 70% chance of becoming overweight or obese as an adult, and obesity leads to more morbidity and mortality.”
What’s more, children who are food insecure have more difficulty in school. Kids who are hungry in kindergarten are significantly behind their peers in math and reading by the third grade, and sometimes never catch up, McCollum said. And adolescents from food-insecure homes are more likely to have difficulty getting along with others, she said. “They’re seven times more likely to get in fights with their peers and four times more likely than their peers to require mental health counseling.”
CONFERENCE CURRENTS
12 today’s dietitian august 2014

What Are the Solutions?The good news is that solutions to decrease food insecurity
and improve kids’ diet quality exist, McCollum said. Examples include increasing participation in school meals and expanding meal programs before, during, and after school and over the summer. Other examples are increasing participation in the Supplemental Nutrition Assistance Program for those who are eligible, advocating for healthier foods and more nutrition edu-cation in food banks, and enlisting the assistance of dietitians.
Food insecurity demands the attention of all segments of society, McCollum said. “Registered dietitian nutritionists are a key to the solution, but it takes collaboration with hunger relief professionals, health care and education sectors, and strong public/private partnerships.” All Academy members need to become champions for kids and get involved in their schools and communities to educate parents and leaders about food insecurity and its consequences, she said.
There are plenty of opportunities for Academy members to get involved even if their region or local area isn’t among the hardest hit, McCollum said. RDs need to educate parents and communities about the consequences of kids going hungry and how to combat the problem.
What You Can DoMcCollum suggested RDs do the following:•Get involved. Access suggested hunger action programs,
including the Hunger In Our Community: What We Can Do Toolkit at www.kidseatright.org/volunteer. Also, share the Nourish to Flourish infographic explaining the hungry and overweight paradox, which is available at www.eatright.org/Public/content.aspx?id=6442478348.
•Learn more. A series of eight webinars on food insecurity topics are available on the Academy Foundation’s website at www.eatright.org/Foundation/content.aspx?id=6442478708. RDs can find quality resources targeting food-insecure popu-lations at www.healthyfoodbankhub.org, a website developed as part of the Future of Food collaboration with the Academy Foundation, Feeding America, and the National Dairy Council.
•Volunteer at a local food bank. Volunteers are needed to sort, box, and repack donated food and direct it to where it’s needed most. Volunteers also are needed to transport food to charitable agencies and provide clerical help. You can find food
banks in your area at FeedingAmerica.org. See if your local food bank operates a Kids Café program. The program provides meals to kids and a safe place where they can get involved in educational, recreational, and social activities. Kids Café pro-grams also offer nutrition education during the school year.
•Advocate for school breakfasts. Studies show that kids who eat school breakfast boost their scores on math, reading, and other tests that require speed, memory, and cognition. For more information about federal food/nutrition programs, visit the Food Research and Action Center at www.frac.org.
•Thank your grocer. Some grocery stores are starting to position products differently and put healthier choices on the more visible end caps. When you shop and see retailers making such changes, show your appreciation, McCollum suggested. Tell them who you are, and “let them know you applaud them and that it doesn’t have to be all candy bars at the front counter.”
•Participate in Kids Eat Right. The Academy and its foundation launched the Kids Eat Right initiative in 2010 to support the efforts of First Lady Michelle Obama and the White House to end the childhood obesity epidemic within a generation. You can get involved in Kids Eat Right in several ways. One is to educate families on strategies for providing healthful meals each day. Offer them shopping ideas, cooking strategies, and recipes through social media. Another is to get involved in parent empowerment, encouraging and helping them to be healthier role models for themselves and their families. You can find many toolkits with ready-made presentations on a variety of healthful eating topics at www.kidseatright.org/volunteer.
RDs don’t have to start from scratch, McCollum said. “You can utilize the tools that are available to you through the Academy and other resources.”
Remember, collaboration is key to success and reducing food insecurity nationwide, McCollum concluded. “We know we have to work together. We can’t do it alone.” She said she has no doubt that RDs can meet the challenges and make a big impact on the health of the nation’s children.
— Beth W. Orenstein is a freelance health writer living in Northampton, Pennsylvania.
We offer relief, recovery and support to anyone who wants to stop eating compulsively.
Compulsive Client?
®no fees • oa.org
august 2014 www.todaysdietitian.com 13

DYNAMICS OF DIABETES
HELP PATIENTS LOSE WEIGHTBy Jill Weisenberger, MS, RDN, CDE, FANDMaking adjustments to medications in accordance with eating and exercise habits is key.
Jack, a middle-aged man with type 1 diabetes, started a low-carbohydrate diet to lose weight. In the first few days of his new diet, he experienced the shaking, sweating, and mild confusion that frequently accompanies hypoglycemia, which is typically defined as blood glucose levels less than 70 mg/dL. Jack didn’t know that by consuming less carbohydrate than usual, he’d need to take less insulin.
Maura, a woman in her early 30s with type 2 diabetes, takes glyburide to control her blood glucose levels. She began an exercise program to lose weight in preparation for her sister’s wedding. Three weeks into the program, she started experiencing hypoglycemia. To avoid this, she began eating a carbohydrate-containing snack before and after each workout. The calories from her snacks, however, exceeded the calories burned during exercise, so her weight slowly increased. She considered giving up exercise.
Maura’s friend Lisa also has type 2 diabetes but controls her blood glucose with metformin. Maura advised Lisa to eat a large carbohydrate-containing snack before exercise, so she did.
Weight-Loss ConcernsLosing weight and keeping it off is
difficult for most people, but those with diabetes of any type have additional challenges. They need to consider how changing their eating and activity habits may affect their blood glucose levels, explains Patti Urbanski, MEd, RD, LD, CDE, one of the authors of the recent American Diabetes
Association nutrition position statement and a diabetes educator on the Fond du Lac Reservation in Cloquet, Minnesota.
Insulin and medications that increase insulin levels in the blood raise the risk of hypoglycemia (see table below). There-fore, individuals taking these medications may need to mea-sure their blood glucose more frequently, Urbanski says. In addition, they may need medication adjustments when they lose weight, increase physical activity, or change their diets, and they will need to know the signs and symptoms of hypo-glycemia and its appropriate treatment. Not all blood glucose–lowering medications promote hypoglycemia when used as monotherapy. In fact, rarely do medications not listed in the accompanying table cause hypoglycemia.
Ideally, patients, guided by a health care team member, should be able to proactively reduce medications as necessary to avoid hypoglycemia. Keeping food, activity, and blood glucose records can provide the necessary information to make sound decisions about treatment changes, says Linda Delahanty, MS, RDN, chief dietitian and director of nutrition and behavioral research at Massachusetts General Hospital Diabetes Center in Boston.
For instance, Jack worked with his health care team to reduce his mealtime insulin to better match his carbohydrate intake. Maura’s health care provider also reduced her glucose-lowering medications. Maura worked with a certified diabetes educator and RD to learn about appropriate snack choices and ideal timing of meals and snacks. Lisa was surprised to learn that taking metformin put her at low risk of hypoglycemia, and that she probably didn’t need a snack immediately before exercise.
To ensure safety, dietitians should advise people at risk of hypoglycemia to carry a carbohydrate source and, if possible, their blood glucose meter while exercising. Dietitians also should tell patients about typical hypoglycemia symptoms, including shaking, nervousness, irritability, sweating, chills, and dizziness.1 Appropriate treatment for mild to moderate hypoglycemia involves consuming a measured amount of glucose (see “The Rule of 15” sidebar on page 16). In addition, patients should wear a medical ID bracelet or carry identification stating they have diabetes.
Hypoglycemia can occur several hours or even a day after exercising, so additional blood glucose monitoring is indicated. Conversely, some people experience hyperglycemia after intense bouts of activity, says New
Blood Glucose–Lowering Medications Likely to Cause HypoglycemiaClass of Medication Generic Name (Brand Name)
Sulfonylureas Glimepiride (Amaryl), glipizide (Glucotrol), glyburide (Diabeta, Micronase, Glynase)
Meglitinides Repaglinide (Prandin), nateglinide (Starlix)
Insulin All types
— SOURCE: GARBER AJ, ABRAHAMSON MJ, BARZILAY JI, ET AL. AACE COMPREHENSIVE DIABETES MANAGEMENT ALGORITHM 2013. ENDOCR PRACT. 2013;19(2):327-336.
14 today’s dietitian august 2014

York-based dietitian Susan Weiner, MS, RDN, CDE, CDN, author of The Complete Diabetes Organizer.
People with diabetes also may have other health concerns, such as comorbidities or complications that contraindicate certain types of physical activity or require specific modifications. For example, patients with proliferative retinopathy or moderate or severe nonproliferative retinopathy may need to avoid lifting weights and placing their heads below the level of their hearts to prevent intraocular bleeding, retinal tears, or retinal detachment. It’s prudent to have patients seek clearance from their health care providers before they begin an exercise program, Delahanty says.
In general, adults with diabetes are encouraged to perform at least 150 minutes of moderate-intensity aerobic activity each week, spread over at least three days with no more than two consecutive days without exercise.2 In the absence of contraindications, adults with type 2 diabetes also should perform resistance training at least twice weekly.
Weight-Loss BenefitsDietitians can assure overweight and obese patients that
losing even a few pounds can result in meaningful improvements in blood glucose and other health parameters. In fact, losing as little as 2% of body weight can benefit glycemic control,
Delahanty says. Losses of 5% to 10% of body weight are associated with significant improvements in blood glucose, blood pressure, and lipids with fewer medications needed to treat these cardiovascular risk factors. Other benefits include improvements in sleep apnea, knee pain, physical functioning and mobility, urinary incontinence, depression, and quality of life, she adds.
Diabetes RemissionIn some patients, weight loss and increased physical
activity can induce either partial or complete remission of type 2 diabetes, Delahanty says. In the Look AHEAD study that examined more than 5,000 overweight or obese people with type 2 diabetes, 11.5% of participants in the intensive lifestyle intervention arm achieved complete remission, defined as normal blood glucose levels with no medications, or partial remission, defined as blood glucose levels in the prediabetes range with no medications.3 Remission rates were higher in those who achieved the greatest weight loss and fitness improvements, had diabetes for a shorter time, had lower initial body weight, had better initial glycemic control, and didn’t take insulin, Delahanty says.
Though weight loss has potential benefits at any time, “It appears that weight loss has the biggest impact on glycemic control when the person is still in the early stages of type 2
THE BENEFITS OF BARLEYWhen talking to your clients about a healthy diet, Go Barley! This ancient grain is versatile, tasty and has been shown to:
• Lower cholesterol
• Moderate glucose response
• Stimulate satiety
For more information, visit www.GoBarley.com
august 2014 www.todaysdietitian.com 15

diabetes,” Urbanski says. In a retrospective study of 2,574 patients, losing weight shortly after their type 2 diabetes diagnosis predicted improved blood pressure and glycemic control despite weight regain.4
An important take-home message is that “losing weight has many other health benefits even if it doesn’t make the diabetes go away,” Urbanski says. “And if people adopt healthier eating habits and increase their activity while they’re trying to lose weight, they very likely will see improved blood glucose even if they don’t lose weight.”
Patients need to know that type 1 diabetes won’t go away with weight loss. Type 1 diabetes is an autoimmune disease, Weiner says, and currently there’s no cure. However, if patients with type 1 diabetes are overweight or obese, weight loss may reduce the amount of insulin they need for blood glucose control.
Is There an Ideal Weight-Loss Diet?Patients with diabetes may ask whether there’s a special
diet they can try to help them lose weight. However, a review of the evidence suggests there’s no single ideal weight-loss
diet for people with diabetes. In interventional studies lasting at least one year and targeting weight loss in individuals with type 2 diabetes, weight loss ranged from an average of 1.9 to 8.4 kg (4.2 to 18.5 lbs) at the one-year mark.5
The two studies reporting the greatest weight loss at one year used different approaches. The Look AHEAD trial reported an average weight loss of 8.6% of initial body weight and used a calorie-controlled plan, meal replacements, and physical activity.3 A study using a Mediterranean-style eating pattern with no more than 50% of calories from complex carbohydrates reported losses averaging 6.2 kg (13.7 lbs).6 “The ideal eating pattern for achieving weight loss is one that’s reduced in calories and considers each individual’s typical eating patterns, food preferences, and metabolic goals, and at the same time is a sustainable way of eating rather than a short-term diet that relies on willpower,” Delahanty says.
By paying special attention to the risk of hypoglycemia and other concerns unique to people with diabetes, dietitians can individualize care to help them lose weight and live healthier lives.
— Jill Weisenberger, MS, RDN, CDE, FAND, is a freelance writer and a nutrition and diabetes consultant to the food industry, including Daisy Brand Cottage Cheese and Good Fats 101. She has
a private practice in Newport News, Virginia, and is the author of Diabetes Weight Loss — Week by Week and the forthcoming
The Overworked Person’s Guide to Better Nutrition.
References1. Hypoglycemia (low blood glucose). American Diabetes
Association website. http://www.diabetes.org/living-with-diabetes/treatment-and-care/blood-glucose-control/hypoglycemia-low-blood.html. Updated May 20, 2014. Accessed May 23, 2014.
2. American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2014;37(1):S14-S80.
3. Delahanty LM. The Look AHEAD study: implications for clinical practice go beyond the headlines. J Acad Nutr Diet. 2014;114(4):537-542.
4. Feldstein AC, Nichols GA, Smith DH, et al. Weight change in diabetes and glycemic and blood pressure control. Diabetes Care. 2008;31(10):1960-1965.
5. Evert AB, Boucher JL, Cypress M, et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care. 2013;36(11):3821-3842.
6. Esposito K, Maiorino MI, Ciotola M, et al. Effects of a Mediterranean-style diet on the need for antihyperglycemic drug therapy in patients with newly diagnosed type 2 diabetes: a randomized trial. Ann Intern Med. 2009;151(5):306-314.
THE RULE OF 151
Both losing weight and becoming more active improve insulin action, which increases the risk of hypoglycemia in some people with diabetes. Dietitians can share the following treatment guidelines with patients who experience blood glucose levels below 70 mg/dL:
Consume 15 g of carbohydrate. It’s best to use pure glucose in the form of tablets, gel, or liquid because it works more quickly and contains a min-imum of calories. The following are some good choices that also include food:
•twotofiveglucosetablets(checkthelabelfor the proper dosage);
•onetubeofglucosegel;
•2Traisins;
•4ozregularsodaorfruitjuice;
•1Tsugarorhoney;or
•1cupnonfatorlow-fatmilk.
Wait 15 minutes after treating before eating anything else or resuming activity. Consume an additional 15 g of carbohydrate if blood glucose remains low. Continue this procedure until blood glucose normalizes.
16 today’s dietitian august 2014

VEGETARIAN NUTRITION
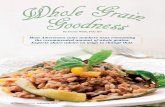
INDIAN CUISINE Foods That Hold a Special Place in Plant-Based Food TraditionsBy Sharon Palmer, RDN
Most vegetarians agree: Indian food is one of the tastiest plant-based cuisines. With fragrant curry, dal, and korma dishes lending their aromatic, flavorful qualities to the plate, who needs meat? Indeed, Indian food culture has a long history of dishing up delicious vegetarian food. Data show that 42% of households in India are vegetarian (don’t eat fish, meat, or eggs), and 58% are less strict vegetarians or nonvegetarians.1
Gita Patel, MS, RDN, CDE, LD, CLT, author of Blending Science With Spices, explains that Indian culture leans toward vegetarianism due to Hinduism, which hosts a central theme of nonviolence, including animals. “A profound respect for all life is a common Hindu belief that supports vegetarian eating styles,” adds Vandana Sheth, RDN, CDE, a spokesperson for the Academy of Nutrition and Dietetics.
However, British colonial influences and Western food trends, such as the emergence of fast-food restaurants, have brought more animal foods into India, Patel says. “With the globalization of the world and technology, some of the urban lifestyle changes have significantly affected traditional food practices in India,” Sheth adds, listing as evidence the increasing number of fast-food restaurants and premade foods replacing traditional meals in India.
Traditional Eating Patterns“A lot of people are drawn to Indian cuisine. People like
the flavors, herbs, and spices,” Patel says, noting that home cooking is vastly different from what you’re likely to sample in an Indian restaurant.
“The traditional eating pattern is very balanced,” Patel says. She describes typical meals consisting of dal (a legume dish), rice, roti (bread), vegetable, salad, fruit, and a yogurt or butter-milk drink, which may vary slightly depending on the region.
Indeed, there’s scientific consensus that a disease-protective diet is based on a variety of whole plant foods, which sums up the traditional Indian eating pattern. “The traditional Indian vegetarian diet is one that’s rich in a wide variety of grains, beans, lentils, vegetables, fruits, nuts, seeds, spices, and herbs. Research has found that vegetarians have a lower risk of heart disease and some types of cancer,” Sheth says. The National Cancer Institute reports that cancer rates are lower in India than in Western countries, and that diet characteristics such as a high intake of fruits, vegetables, spices, and tea may be responsible for protecting Indians against certain forms of cancer.2
Chana Dal Stew
Makes 6 servings (about 1 cup each)
Ingredients8 oz (227 g or 11⁄4 cups) dried chana dal 5 cups (711 ml) water2 medium carrots, sliced1 medium red bell pepper, chopped1 medium onion, chopped2 small red potatoes, unpeeled, chopped2 small tomatoes, chopped1 tsp garam masala 1⁄2 tsp turmeric1⁄2 tsp grated fresh ginger2 medium garlic cloves, minced1⁄4 tsp crushed red pepper 1 T unsalted creamy peanut butter
Directions1. Place all ingredients in a large pot, stir well, cover, and bring to a simmer.2. Cook for about 50 minutes until the vegetables and chana dal are tender.
Nutrient Analysis per servingCalories: 215; Total fat: 1 g; Sat fat: 0 g; Sodium:
34 mg; Total carbohydrate: 40 g; Fiber: 14 g; Sugars: 4 g; Protein: 12 g
— RECIPE COURTESY OF SHARON PALMER, RD, FROM PLANT-POWERED FOR LIFE (THE EXPERIMENT, 2014)
Chana Dal Stew—
PH
OTO
CO
UR
TES
Y O
F H
EA
THE
R P
OIR
E
august 2014 www.todaysdietitian.com 17

Key Components While the specific dishes may vary according to dif-
ferent regions of India, the key ingredients basically are the same and include the following:
• Vegetables: “Vegetables are grown all over the country due to the climate,” Patel says, adding that many vegetables are unique to India, such as specific types of gourds, radishes, beans, and greens. However, other dishes are based on more familiar vegetables, such as beets, Brussels sprouts, cabbage, carrots, cauliflower, celery, cucumber, corn, eggplant, green beans, various greens, okra, onions, peas, peppers, potatoes, radishes, spinach, squash, and tomatoes. In addition, fermented foods such as pickled vegetables are a regular feature in Indian cuisine.
• Grains: Rice and wheat are staples in India and used in flatbreads (eg, dosa, roti, chapati), doughs (eg, samosa, kachori), and side dishes (rice) to accompany meals.
• Legumes: Indian cuisine relies on the regular and flavorful use of legumes, such as black-eyed peas, chickpeas, lentils, and beans. In addition to dal, many legumes are sprouted or used as flour in breads.
• Fruits: Apples, apricots, bananas, figs, grapes, guavas, lychees, loquats, mangoes, oranges, papa-yas, passion fruit, and sweet limes are common fruits in India.
• Dairy: From milk and buttermilk to yogurt and paneer (fresh cheese), dairy products are regular features of the Indian diet. Patel reports that most Indian households receive fresh milk, which is then used for beverages and cooking. Households make their own ghee (clarified butter) from the milk fat, and leftover milk is made into fresh yogurt every day.
• Vegetable oils: Most oils used in traditional cook-ing are unrefined vegetable oils, such as peanut or sesame. However, Patel reports an increase in the use of refined oils, such as soybean oil, in modern cooking.
Sprouted Moong Bean Salad
Makes 6 servings
Ingredients
Dressing1 T oil (olive or canola)1⁄2 to 1 tsp salt (optional)1 tsp freshly roasted and ground cumin1 T lemon juice
Beans2 cups sprouted moong (also known as mung) beans Salt, to taste1 cup chopped tomatoes1 cup chopped cucumber1⁄2 to 1 cup shredded cabbage1 seeded and diced green chili (optional)1 tsp minced ginger (optional)1⁄4 cup chopped cilantro
Directions1. Mix all of the dressing ingredients and set aside.2. Heat 1⁄4 cup of water in a pan with sprouts and salt. When it comes to a boil, turn the stove off, and leave it covered for 4 to 5 minutes.3. Mix the sprouted beans with all of the ingredients, stir in the dressing, and top with cilantro.
Nutrient Analysis per servingCalories: 111; Total fat: 3 g; Sat fat: 0 g; Sodium: 8 mg;
Total carbohydrate: 17 g; Fiber: 6 g; Sugars: 2 g; Protein: 6 g
— RECIPE COURTESY OF VANDANA SHETH, RDN, CDE
Indian cuisine relies on the regular and flavorful use of legumes, such
as black-eyed peas, chickpeas, lentils, and beans. In addition to dal, many legumes are sprouted
or used as flour in breads.
18 today’s dietitian august 2014

• Herbs and spices: At the heart of Indian food is a long list of culinary herbs and spices that have been used for centuries, many of which are proven to have antioxidant, anti-inflammatory, antimicrobial, and anticancer effects. Indian spices include amchur (made from mangoes), aniseed, asafetida (a pungent, onionlike flavor), bay leaf, black pepper, cardamom, chilies, cinnamon, cloves, coconut, coriander, cumin, dill, fennel, fenugreek, garam masala (a spice blend), garlic, ginger, mango powder, mint, mustard, nutmeg, onion seeds, parsley, pomegranate seeds, poppy seeds, saffron, sesame seeds, tamarind, and turmeric.
Tips to Get CookingThe following are some tips when cooking Indian
vegetarian food:•Fortrueflavor,useIndianspices.Don’tjustrelyoncurry
powder for every dish; stock your kitchen with the basics, such as cumin seeds, cayenne pepper, ground coriander, turmeric, brown mustard seeds, and the spice blend garam masala.
•Don’tbeafraidtotryanIndianrecipe.Manyrecipesusestandard cooking utensils you may have at home and take only minutes to prepare.
•Don’tfeelyouhavetoprepareafullIndianmealwithawide variety of dishes you may see at a typical restaurant. Keep it simple with one legume dish that can be served with rice and a salad.
— Sharon Palmer, RDN, is a contributing editor to Today’s Dietitian and the author of
The Plant-Powered Diet and Plant-Powered for Life.
References1. Growth and concentration in India. Food and Agriculture
Organization of the United Nations website. http://www.fao.org/wairdocs/lead/x6170e/x6170e09.htm#fn6. Accessed May 25, 2014.
2. Sinha R, Anderson DE, McDonald SS, Greenwald P. Cancer risk and diet in India. J Postgrad Med. 2003;49(3):222-228.
Stir-Fried Vegetables With Edamame
Makes 6 servings
Ingredients1 tsp cumin seeds2 T olive oil1 T sesame seeds3 cloves garlic, chopped1⁄2 jalapeño pepper, sliced in half (or use cayenne
or black pepper to taste)11⁄2 cups fresh or frozen corn 1⁄4 tsp turmeric
1⁄4 tsp salt (or to taste)1 cup frozen edamame, thawed3 cups zucchini, sliced1 cup sweet red bell pepper, sliced1 cup chopped (with tender stems) cilantro Juice of 1⁄2 lemon1⁄2 tsp lemon zestCooked rice, millet, or quinoa
Directions1. Heat a 2- to 3-qt skillet or pan on medium-high heat and add cumin seeds.2. When the seeds begin to change color and give an aroma, add olive oil, sesame seeds, and chopped garlic and turn heat to medium.3. Fry the garlic for a minute and add jalapeño, corn, tur-meric, and salt. Stir then cook covered for 2 to 3 minutes.4. Add edamame, zucchini, and red pepper. Stir then cook covered for 3 to 4 minutes.5. Before serving, add chopped cilantro, fresh lemon juice, and lemon zest. Stir to mix all the ingredients.6. Serve the vegetables over rice, quinoa, or millet. Enjoy leftovers for lunch in a pita pocket.
Nutrient Analysis per servingCalories: 121; Total fat: 7 g; Sat fat: 1 g; Sodium: 10 mg;
Total carbohydrate: 14 g; Fiber: 4 g; Sugars: 5 g; Protein: 4 g
— RECIPE AND PHOTO COURTESY OF GITA PATEL, MS, RDN, CDE, LD, CLT
august 2014 www.todaysdietitian.com 19

VITAMIN B12 By Amelia R. SherryResearch suggests deficiencies in this vitamin are more common than we may think.
Dietitians are well aware that vitamin B12 is one of the key nutrients in which vegetarians and vegans are deficient, and that they need guidance on how to increase their intake. But can more be done to protect these clients against this nutrient shortfall and its severe consequences?
According to one researcher, the answer is yes. “Registered dietitian nutritionists should recommend that all vegetarians, including even semivegetarians, be tested for B12,” says Roman Pawlak, PhD, RD, an associate professor in the department of nutrition science at East Carolina University in Greenville, North Carolina.
It’s long been accepted that a vegan diet poses a high risk of vitamin B12 deficiency, but the notion that less restrictive vegetarians should be closely monitored for shortfalls remains controversial. Pawlak bases his recommendation for testing in part on a 2013 literature review he coauthored, in which 18 articles were examined that assessed the vitamin B12 status of vegetarians, including lacto-ovo-vegetarians, lacto-vegetarians, vegans, and those following a macrobiotic diet. The results showed that 62% of pregnant women, 25% to almost 86% of young children, 21% to 41% of adolescents, and 11% to 90% of elderly subjects were deficient in vitamin B12.1
Accurate MeasuresPrevious studies that have identified B12 deficiency among
vegetarians have shown significantly lower prevalence rates than Pawlak’s 2013 literature review.2-4 Pawlak argues that his 2013 study paints a more realistic picture of the prevalence of B12 deficiency because he and his colleagues limited their
research to studies assessing B12 status using only serum or urinary methylmalonic acid (MMA), holo-transcobalamin-II (holo-TCII), or both, which are considered more specific and accurate measures of vitamin B12 depletion and deficiency com-pared with the more commonly used serum B12 test.5,6 Notably, MMA and holo-TCII are the two tests, along with homocysteine, that the Academy of Nutrition and Dietetics (the Academy) cur-rently recommends for determining B12 status in vegetarians.7
In fact, the widely used serum B12 test has been characterized as an unreliable measure of deficiency because the cutoff point for determining a deficiency is most often defined as 200 pg/mL or lower, which often is considered too low.8 In other words, researchers who use 200 pg/mL as the cutoff point are exclud-ing a significant number of deficient patients with levels falling between 200 pg/mL and 350 pg/mL. “Symptoms of B12 deficiency have been noted up to a concentration of 350 pg/mL,” explains Katherine L. Tucker, PhD, a professor of nutritional epidemiol-ogy in the department of clinical laboratory and nutritional sciences at the University of Massachusetts Lowell.
Indeed, low serum B12 is considered a late indicator of defi-ciency in that by the time blood levels fall, clinical symptoms such as irreversible peripheral neuropathy already may be present. And serum B12 measures the total amount of B12 cir-culating in the blood, up to 80% of which may be inactive analogues, which can block B12 absorption.9 Holo-TCII, by com-parison, is considered more sensitive because it measures just the active form of B12. MMA also is considered more sensitive because cobalamin is required to convert methylmalonyl coen-zyme A to succinyl coenzyme A; therefore, rising MMA levels are an early indicator that active B12 has fallen.10
Jumping the Gun on Testing?Despite the current research, not all dietitians are convinced
that Pawlak’s 2013 review proves that all vegetarians should be tested for vitamin B12 deficiency. “The research studies that are available to be included in this review are limited, particularly with regard to Western countries in which B12-fortified foods are commonly consumed, though it’s not the fault of the review that the studies are limited; there just aren’t many out there,” says Reed Mangels, PhD, RD, LDN, an adjunct professor of nutrition at the University of Massachusetts Amherst and the nutrition advisor for the Vegetarian Resource Group.
“The only study on pregnant women was conducted in Ethiopia where a diet primarily composed of maize was eaten, for example. Also, while the studies spanned 22 years, very few recent studies, such as those conducted in the past 10 years, were available and included. In recent years, more vegetarians seem to be aware of the need to include reliable sources of B12 in their diets,” Mangels says, adding that she considers the evidence for across-the-board testing, which can be very costly, to be “shaky at best.”
Another weakness of the literature review: While MMA and holo-TCII are considered more accurate measures than serum B12, neither test, nor homocysteine, on its own is considered
SUPPLEMENT SPOTLIGHT
20 today’s dietitian august 2014

a gold standard diagnostic tool for identifying deficiency.10 For example, serum MMA may be elevated because of intestinal bacterial overgrowth, while urinary MMA may be high due to impaired kidney function. Holo-TCII levels may dip temporarily due to drug interactions or be affected by pregnancy, oral con-traceptives, folate disorders, and alcoholism, plus folate, renal dysfunction, and vitamin B6 deficiency can impact homocys-teine levels.10,11 For these reasons, it has been recommended that abnormal results of two or more tests be used to confirm a deficiency.10 In Pawlak’s 2013 literature review, only three of the 18 studies required two tests to establish a vitamin B12 defi-ciency. However, those studies that used two tests still revealed that deficiencies existed in 55% to 69% of vegetarians.
What’s more, because no universally established criteria exists for defining a vitamin B12 deficiency, the cutoff points for determining shortfalls differed among the studies examined. However, Pawlak believes that if uniform measures were used, prevalence would be even higher. “I am convinced that if authors of the published studies used appropriate B12 deficiency criteria, virtually all of their participants would have been diagnosed with a deficiency,” he says.
Stages of Deficiency While across-the-board testing is expensive and remains con-
troversial, understanding the usefulness of sensitive diagnostic tests is helpful for dietitians who suspect a client or patient may have a vitamin B12 deficiency. Mangels agrees that detecting B12 depletion before it becomes a deficiency is important. “You don’t want to wait until symptoms appear because by that time, there could be irreversible damage,” she says.
The early stages of B12 deficiency, also referred to as B12 depletion, often involves a fairly latent condition characterized by vague or no symptoms (eg, fatigue, forgetfulness), which can go unnoticed for months or years.8,12 Then suddenly, depletion can progress to later stages without warning and in as little as two months, lead to permanent peripheral neuropathy and cognitive damage.13
Sensitive tests can help a clinician detect B12 depletion (or a subclinical deficiency ) before it progresses. Specifically, the holo-TCII test can identify B12 depletion (also known as stages I and II of B12 deficiency), which is defined as having a negative balance of B12, or simply when the amount absorbed falls below the amount lost daily since it measures only the active amount of B12 circulating in the blood.4 Elevated MMA and homocysteine levels indicate a functional deficiency of B12, which is stage III. Total serum B12, which includes inactive and active forms, usually doesn’t fall until stage IV when more obvious clinical manifestations are apparent.
Counseling and ProtectionWhen working with vegetarian and vegan clients, the first
step for dietitians is to assess their B12 intake from foods and supplements to determine whether they’re meeting the Recommended Dietary Allowance (RDA), which is 2.4 mcg/day
for adults and elders and 2.6 and 2.8 mcg/day for pregnant and lactating women, respectively. “This should include serving sizes, frequency, and sources,” Mangels says. “For example, taking a large supplemental dose once weekly may be fine, but eating eggs once or twice a week is not.”
Dietitians can recommend testing once a dietary assess-ment reveals a low intake. “I would especially recommend it for any client who is reluctant to supplement or eat fortified foods. If they feel they don’t need it, a test such as MMA, holo-TCII, or homocysteine can help prove to them otherwise,” Mangels says.
If these three, more sensitive tests aren’t available, “practi-tioners can use serum B12, but they should be aware that many lab values consider serum concentration even slightly below 200 as normal. So, in such a case, the dietitian needs to under-stand how to interpret the results rather than just accept the description from the lab,” Pawlak says.
For clients who resist testing altogether, RDs should stress the profound risks associated with vitamin B12 depletion and elevated MMA and homocysteine, such as anemia, Alzheimer’s and cardiovascular diseases, dementia, depression, and nerve degeneration, which may help change their minds.
When providing nutrition counseling to vegan and vegetarian clients, dietitians should recommend they eat foods fortified with vitamin B12 or suggest they take a supplemental amount that meets the RDA, says Toby Smithson, MSNW, RDN, LDN, CDE, a spokesperson for the Academy. However, controversy exists over whether the RDA is enough, since research has shown that anywhere between 4 and 10 mcg may be needed to raise B12 to appropriate levels in healthy subjects.14,15 For those who already have a deficiency or serum blood level below 350 pg/mL, some experts recommend amounts 40 to 100 times higher than the RDA.
Vegetarian elders also should eat fortified foods or take a supplement since the naturally occurring B12 found in food sources often is bound to protein. Atrophic gastritis, a condition affecting up to 30% of older adults, reduces the secretion of hydrochloric acid and thereby limits protein-bound vitamin B12 absorption. “Having a list handy of reliable sources of fortified foods, including plant milks, meat substitutes, breakfast cere-als, some energy bars, and supplements, also can be helpful for all clients,” Mangels says.
Moreover, dietitians should be vigilant about discussing the importance of vitamin B12 supplementation when counseling pregnant and lactating women and children since the risks of deficiency, such as neurological damage and developmental delay, in these groups can be especially devastating.
— Amelia R. Sherry is a freelance writer, a dietetic intern at CUNY Hunter College School of Public Health in New York City,
and the founder of the blog FeedingIsla.com.
For references, view this article on our website at www.TodaysDietitian.com.
august 2014 www.todaysdietitian.com 21

Diabetes MealThe Top 10
BY CONSTANCE BROWN-RIGGS, MSEd, RD, CDE, CDN

It’s been two decades since the American Diabetes Association (ADA) announced there was no longer a universal diet for people with diabetes. This message was reemphasized in 2013 when the ADA issued a new position statement, “Nutrition Therapy Recommendations for the Management of Adults With Diabetes.” Moreover, the ADA moved away from using the word “diet,” opting to focus on meal patterns or dietary patterns instead.
“The word ‘diet’ gives people the notion that there’s an on and off,” says Hope Warshaw, MMSc, RD, CDE, BC-ADM, owner of Hope Warshaw Associates in Alexandria, Virginia. “Reality is that this can’t be the case if one is going to be successful at achieving diabetes control and/or weight management long term.”
Because the media often promotes various fad diets for weight loss and other health conditions, encouraging clients and patients and other health care providers to move away from the notion of following a particular diet can be difficult.
Recently, US News & World Report ranked what it called 10 diets as the most effective for managing diabetes. This article will discuss each of them and the research regarding their effectiveness, strengths, and weaknesses.
Best Eating Plans for DiabetesEvery year since 2010, US News & World Report has ranked the year’s
most popular diets. Using a panel of experts, including RDs and physicians specializing in diabetes, heart health, and weight loss, diets are ranked in eight categories, such as diabetes and heart disease prevention and control, as well as easiness to follow and likelihood of weight loss.
According to the 2013 ADA nutrition recommendations, there are several meal patterns that have shown good results in people with diabetes. Many of these meal patterns, such as the Mediterranean, vegetarian, vegan, and DASH dietary plans, can be found among the US News & World Report list of best diets for people with diabetes. The Biggest Loser and DASH approaches tied for first place, while the Engine 2, flexitarian, Mayo Clinic, Ornish, and vegan approaches tied for second place. Tying for third place were the anti-Inflammatory, Mediterranean, and vegetarian diets.
Biggest Loser“The Biggest Loser uses the 4-3-2-1 Biggest
Loser Pyramid for the nutritional choices,” says Amy Jamieson-Petonic, MEd, RD, CSSD, LD, LMT, a Cleveland-based spokesperson for the Academy of Nutrition and Dietetics (the Acad-emy). The diet suggests consuming four serv-ings of fruits and vegetables per day, three servings of protein foods, two servings of whole grains, and no more than 200 kcal from the extras category at the top of the pyramid.
Can it prevent or control diabetes? “The diet can help control blood sugar. Eating less refined carbohydrates and more dietary fiber, fruits, and vegetables, along with physical activity, can improve insulin resistance and improve glucose levels in people with diabetes,” Jamieson-Petonic says.
The Diabetes Prevention Program provides evidence that people at risk of type 2 diabetes can delay or avoid developing the disease by losing weight through regular physical activity and a diet low in fat and calories. Data from The Biggest Loser show some contestants no longer had indications of the metabolic syndrome, reducing the risk of type 2 diabetes.1
In a retrospective analysis of 35 Biggest Loser contestants, those with prediabetes experienced decreased hemoglobin A1c levels, from 5.6% to 5.1% at week 29. The drop also was significant for those with type 2 diabetes, who saw A1c reduced from 6.9% to 5.2%. Participants who had been taking metformin discontinued it during week 1. Reductions also were observed in fasting glucose, fasting insulin, and insulin resistance index.2
Strengths and weakness: “It’s a solid nutri-tion program that offers a well-balanced, high-fiber diet full of whole grains, lean proteins, fruits, and vegetables as well as adequate water,” Jamieson-Petonic says.
Supplements aren’t recommended as part of the diet, but Jamieson-Petonic says a supple-ment is warranted because the lowest calorie range suggested in the plan is 1,050. “A multivi-tamin should be recommended for people con-suming less than 1,200 kcal per day,” she says.
DASH In 1995, the National Heart, Lung, and Blood
Institute funded the landmark diet and blood pressure study called the Dietary Approaches
PatternsDiabetes MealNutrition professionals review US News & World Report’s highest-ranked diets for clients and patients.
FIRST PLACE WINNERS1
august 2014 www.todaysdietitian.com 23

to Stop Hypertension (DASH) trial. “The study was remarkable, illustrating for the first time that dietary intervention alone significantly lowers systolic and diastolic blood pressure in hypertensives and nonhypertensives,” says Janet Bond Brill, PhD, RDN, LDN, FAND, author of Prevent a Second Heart Attack: 8 Foods, 8 Weeks to Reverse Heart Disease and two other books.
Can it prevent or control diabetes? “The DASH diet is excellent for pre-venting and controlling diabetes,” Brill says. Most research on the DASH diet has been in people without diabetes, but there was a small study pub-lished January 2011 in Diabetes Care that examined people with type 2 dia-betes. The participants, who were randomly assigned to a control diet or the DASH eating plan with a sodium restriction of 2,300 mg/day, experi-enced reduced body weight and improved fasting blood glucose, A1c, blood pressure, and other cardiovascular risk factors.
Being overweight is one of the biggest risk factors for developing type 2 diabetes, and combining the DASH eating pattern with calorie restriction has been found to help people shed pounds and reduce other risk factors, such as the metabolic syndrome.
Strengths and weaknesses: The DASH eating plan has been shown to help control high blood pressure, which is prevalent in people with diabe-tes. From 2005 to 2008, 67% of adults aged 20 and older with self-reported diabetes had blood pressure greater than or equal to 140/90 mm Hg or used prescription medications to control their hypertension.3
The DASH diet is an exchange-based meal plan with various calorie levels, which Brill considers a strength. “It has a specific daily level of minerals and calories to strive for, plus it restricts sodium intake,” she says. The biggest weakness: “There isn’t as much clinical research backing effectiveness for diabetes management,” she says.
Engine 2 Firefighter Rip Esselstyn created the Engine 2 diet, and his father’s
landmark research on the prevention and reversal of heart disease through a plant-based diet is what inspired him to develop the eating plan.4 “The author puts readers on a plant-based diet consisting of whole grains, vegetables, fruits, soy products, tofu, and legumes and steers clear of animal-based products and refined foods,” explains Jim White, RDN, ACSM HFS, owner of Jim White Fitness & Nutrition Studios in Virginia Beach, Virginia, and a spokesperson for the Academy.
Can it prevent or control diabetes? “According to Esselstyn, the Engine 2 diet will help people with diabetes get off their medications,” White says.
The diet provides two options: the firefighter, which requires a complete and immediate life-style change, avoiding all animal products, pro-cessed foods, and vegetable oils; and the fire cadet, which allows for a more gradual change to ultimately eat a vegan diet. “Weight loss is inevitable with either approach,” White says, and that’s good news.
“If one is overweight with prediabetes and early-onset type 2 diabetes, then a small amount of weight loss—7%—can help the person improve their glycemia, lipids, and blood pressure,” Warshaw says. After reviewing six low-fat vegan studies in individuals with type 2 diabetes, the writers of the 2013 ADA position statement found that the research consistently showed improvement in glycemic control and cardiovascular risk factors but only when sub-jects lost weight.
Strengths and weaknesses: The Engine 2 diet is low in fat, which leads to weight loss, and that’s a strength, White says. However, the diet requires a complete lifestyle change with considerable meal planning and preparation,4 which will take a strong commitment to carry out, he says. Instead, “I’d recommend this diet for current vegetarians looking for a resource for new recipes or vegetarians looking to prog-ress to a vegan diet.”
Flexitarian “The flexitarian diet is a vegetarian diet
with flexibility to include occasional meat and poultry,” explains Dawn Jackson Blatner, RD, a certified specialist in sports dietetics and the author of The Flexitarian Diet. Unlike many vegetarian eating plans that eliminate meat, “The flexitarian diet philosophy is proplants, not antimeat,” Blatner says. She believes, and evidence supports, that people who eat more plants tend to consume fewer calories and more nutrients, such as fiber, and a wide variety of disease-fighting phytonutrients that are available only in plants.
Can it prevent or control diabetes? The 2013 ADA nutrition recommendations for preventing and controlling diabetes include weight loss and eating high-fiber foods such as fruits, vegeta-bles, whole grains, and legumes.
Individuals following an energy-restricted, plant-based diet such as the Mediterranean or vegetarian eating patterns have been shown to experience improved glycemic control.5 “Flexi-tarian eating can lead to weight loss, and weight
The Mayo Clinic diet mirrors the 2013 ADA nutrition recommendations. There are heart-healthy food choices and recommendations for portion control, exercise, and limiting excess fat, sugar, alcohol, and calories.
— Melissa Joy Dobbins, MS, RDN, CDE
SECOND PLACE WINNERS2
24 today’s dietitian august 2014

The Diabetes Prevention Program provides evidence on the benefits of weight loss, and the 2013 ADA nutrition recommendations state that there isn’t an ideal eating pattern for everyone, and that total energy intake is important. “Anyone with prediabetes, diabetes, or a family history of dia-betes can benefit from this diet plan,” Dobbins says. “However, people with diabetes should talk with their health care provider about whether carb counting also should be a part of their individualized plan.”
Strengths and weaknesses: The Mayo Clinic diet mirrors the 2013 ADA nutrition recommendations. There are heart-healthy food choices and rec-ommendations for portion control, exercise, and limiting excess fat, sugar, alcohol, and calories, Dobbins says.
The 2013 ADA nutrition recommendations show that the quantity and type of carbohydrate in food impacts blood glucose levels, and the total amount of carbohydrate eaten is the primary predictor of glycemic response. One weakness of the Mayo Clinic diet is the absence of carb counting. “Even ‘healthy’ carbs in healthy amounts may raise blood sugar in people with diabetes,” Dobbins says.
US News & World Report experts thought the Mayo Clinic diet was mod-erately easy to follow. However, Dobbins suggests that individuals with dia-betes may find the diet and activity recommendations daunting to follow on their own. “I strongly recommend talking with a certified diabetes educator to help create a personal, step-by-step action plan that takes into account the individuals lifestyle and supports behavior change,” she says.
OrnishDean Ornish, MD, ranked foods from most to least healthful. No
foods are forbidden, and there’s no all-or-nothing approach. Results depend on the degree to which an individual limits the least healthful foods. “For example, his recommendations to reverse heart disease
loss can help prevent and manage diseases such as diabetes,” Blatner says.
Strengths and weaknesses: “Because the diet is balanced and flexible, it can be used by anyone, but portions matter as much as food choice,” Blatner says. “It’s important for anyone following a plant-based diet to understand the right portions for their body, lifestyle, and activ-ity level to achieve their best blood sugar levels.”
Mayo ClinicThe Mayo Clinic diet has two phases to help
people transition to healthier food and physi-cal activity choices. The first phase, “Lose It,” is about changing key habits, not calorie count-ing. The second phase, “Live It,” focuses more on food groups and portion sizes. “Overall, it’s a well-balanced, healthful diet that incorpo-rates nutrient-rich foods from all food groups and reduces or eliminates excess fat, sugar, and calorie intake [from less nutritious foods],” says Melissa Joy Dobbins, MS, RDN, CDE, CEO of Sound Bites in Chicago.
Can it prevent or control diabetes? The Mayo Clinic diet wasn’t designed specifically to prevent or control diabetes. However, the majority of the US News & World Report experts considered the diet’s approach to be better than other diets for this purpose.5
august 2014 www.todaysdietitian.com 25

require less than 10% of calories from fat—no oils, seeds, nuts, avocados, or olives; no more than 10 mg of cholesterol per day; meat, poultry, and fish are to be eliminated; less than 2 T, or 24 g, of sugar per day; no caffeine except green tea; low salt; no more than one alcoholic drink per day; and include one full-fat serving of soy per day,” says Jessica Crandall, RDN, CDE, a dietitian at Sodexo’s Denver Wellness and Nutrition program.
Can it prevent or control diabetes? “The majority of research on the Ornish diet has been conducted by Dr Ornish or by his team, therefore it’s difficult to know the validity,” Crandall says. “In addition, the research has been focused on heart disease as opposed to diabetes.”
However, there was a study published in the American Journal of Health Promotion in which Ornish dieters decreased their A1c levels by 0.4 per-centage points after one year. Study participants with diabetes followed the Ornish program and showed the same improvements in coronary risk fac-tors and quality of life as those without diabetes. Participants also reduced their diabetes medication.6
Strengths and weaknesses: “The diet is rich in healthful foods such as fruits, vegetables, and whole grains, but it’s also extremely low in fat, going against the recommendations for Americans,” Crandall says. The best candidate for the Ornish diet is “someone who can maintain an extreme diet with limited food options and can afford to purchase that food,” she says.
Anti-Inflammatory The anti-inflammatory diet was developed by Andrew Weil, MD, best-
selling author, speaker, and integrative medicine specialist, and is based on the Mediterranean diet. It follows the same nutrition guidelines as the 2010 Dietary Guidelines for Americans and the American Heart Association. “Consume low–glycemic-load meals, lean protein, healthy fats—balancing omega-3 and omega-6—and fresh produce,” says Toby Smithson, MSNW, RDN, LDN, CDE, author of Diabetes Meal Planning and Nutrition for Dummies. The diet also recommends eating fewer white potatoes, bread, crackers, chips, and pastries as well as sugar-sweetened beverages. “These carbohydrate foods also contribute to inflammation,” Smithson says.
Can it prevent or control diabetes? Smithson agrees with the US News & World Report experts and says, “The guidelines fall in line with the poten-tial to prevent and control diabetes since the overall recommendations are healthful eating guidelines.” However, she says the best method of reducing inflammation is through weight reduction and increased physi-cal activity.
Strengths and weaknesses: The anti-inflammatory diet doesn’t prom-ise or focus on weight loss. The recommended daily calorie range is from 2,000 to 3,000, depending on sex, size, and activity level. “People with pre-diabetes and type 2 diabetes typically require weight loss, and the anti-inflammatory diet won’t guarantee weight loss with 2,000 to 3,000 kcal/day and limited focus on physical activity,” Smithson says, also pointing to the diet’s high sodium content. A sample menu contained more than 3,000 mg of sodium, which is twice as much sodium as recommended for people with diabetes, she says.
Moreover, Smithson says the lack of discus-sion on physical activity is another weakness of the diet. “This eating plan is an overall health-ful eating plan with inclusion of lean protein, healthful fats, fresh fruits and vegetables, and whole grain carbohydrates,” she says.
MediterraneanIn 1993, the nonprofit organization Oldways,
the Harvard School of Public Health, and the European Office of the World Health Organiza-tion introduced the Mediterranean diet along with the Mediterranean Diet Pyramid graphic. “The Mediterranean diet is a largely plant-based eating pattern based on the traditional foods and drinks of countries surrounding the Mediterra-nean,” says Sara Baer-Sinnott, president of Old-ways. The diet features fruits, vegetables, fish, beans, nuts, and whole grains as well as other ingredients such as olive oil and wine that have been shown to promote good health.
Can it prevent or control diabetes? Accord-ing to Baer-Sinnott, the diet has been studied and noted by many leading scientists as one of the healthiest in the world. In the last year, 10 studies have been published that document the relationship between diabetes and the Mediter-ranean diet.
In a large study published in the August 2013 issue of Diabetologia, researchers analyzed data from more than 22,000 participants followed for 11 years in the Greek cohort of the European Prospective Investigation Into Cancer and Nutri-tion study to explore the relationship among the Mediterranean diet, glycemic load, and occur-rence of type 2 diabetes. Researchers found that people who consumed foods with a low glycemic load that adhere to the principles of the Medi-terranean diet have a 20% reduced risk of type 2 diabetes.7
The ADA 2013 nutrition recommendations suggest further research is needed to deter-mine whether these study results and others conducted in the Mediterranean region can be generalized to other populations and whether similar levels of adherence to the eating pattern can be achieved.
Strengths and weaknesses: “The Mediterra-nean diet is easy to follow, affordable, and deli-cious, and can be enjoyed by the entire family,” Baer-Sinnott says. “It’s filled with quality nutri-ent-dense foods.” Research has shown that eating foods such as olive oil, nuts, and legumes contribute to satiety, helping people feel full
THIRD PLACE WINNERS3
26 today’s dietitian august 2014

Crunchmaster.comFor recipe ideas and coupons, please visit us at:
plan. Results show these vegetarians have a lower rate of type 2 diabetes than nonvegetarians. “In this study, eating vegetarian also has been asso-ciated with lower risk of overweight, insulin resistance, and metabolic syn-drome, a precursor to type 2,” she says. The research also shows that the closer someone follows a vegan diet along the vegetarian spectrum, the more health benefits he or she will experience.
Strengths and weaknesses: According to Warshaw, following a veg-etarian diet is easier today than ever before, but it still has its challenges. People need to understand the challenges of following a vegetarian or vegan diet up front, such as the shopping, cooking, and eating meals out, she says.
No One-Size-Fits-All Pattern“There’s no magic to any eating plan or pattern for diabetes,” Warshaw
notes. The best meal plan for diabetes is one that’s individualized based on health goals, personal and cultural preferences, access to healthful choices, and a readiness, willingness, and ability to change.
— Constance Brown-Riggs, MSEd, RD, CDE, CDN, is past national spokesperson for the Academy of Nutrition and Dietetics, specializing in
African American nutrition, and author of the African American Guide to Living Well With Diabetes and Eating Soulfully and Healthfully With Diabetes.
longer. “We know that eating too much of any-thing isn’t healthful, so portion size and balance are still key,” she says.
Conversely, Brill says, “No standard definition of the Mediterranean diet exists, making it difficult for many to follow. There are no suggested daily intake guidelines or calorie-controlled options and no recommended daily maximum sodium level.” To address this problem, Brill developed the 10 Point Mediterranean Lifestyle Key Component Checklist, which helps her patients determine minimum and maximum amounts of foods for this eating pattern.8
Vegetarian“Vegetarianism is a broad term for an
increasingly or decreasingly rigid list of allowed foods, with vegan the most narrow,” Warshaw says. The vegan diet excludes eggs, dairy, and all other animal products. The flexitarian, Ornish, and Engine 2 diets are all part of the spectrum of vegetarianism.
Can it prevent or control diabetes? Warshaw points to the ongoing 1974 Adventist Health Study of nearly 100,000 Seventh-day Adventists as evidence of the benefits of a vegetarian meal
For references, view this article on our website at www.TodaysDietitian.com.

Gluten-Free

In an effort to stay abreast of the latest trends, some of the nation’s fast-food chains have introduced gluten-free menus or menu items to cater to cus-tomers. Like the large numbers of sit-down res-taurants that offer gluten-free foods, fast-food chains are finding that the demand for such fare
continues to rise, and they’re attempting to deliver. But there are some important things clients and patients must know if they plan to eat gluten-free fast food.
Burgeoning TrendAs the general population and the medical community
become more educated about celiac disease, an increasing number of people are being diagnosed. That’s driving a trend of increased demand for gluten-free food options. “Restau-rants are getting on board with this trend because of the fact that one out of 133 Americans [1% of the population] is esti-mated to have celiac disease,” says Jim White, RDN, ACSM HFS, owner and president of Jim White Fitness & Nutrition Studios in Virginia Beach, Virginia, and a spokesperson for the Academy of Nutrition and Dietetics (the Academy).
Joy Dubost, RD, PhD, CSSD, an experienced food scientist and the director of nutrition and healthy living at the National Restaurant Association, says there’s no question the demand is there. “Eating a gluten-free diet has become very popular for many reasons. People think they can lose weight or feel healthier, and restaurants are in the business of providing what customers want,” she says.
White agrees that celiac disease isn’t the only reason many Americans have chosen the gluten-free route; weight loss and overall health are two motivators. “Diet trends including Paleo, low carb, and antiwheat have all driven the trend of gluten-free dining at restaurants,” he says.
For many, it’s become a lifestyle choice. Unfortunately, that choice sometimes is based on misinformation. “As much as 30% of the population reports eating gluten-free,” says Rachel Begun, MS, RDN, CDN, a food and nutrition consultant and the author of The Gluten Free RD blog. “Of this 30%, more are eating gluten-free for nonmedical rea-sons than those who have to eat gluten-free due to celiac disease or nonceliac gluten sensitivity. I attribute this to the health-halo effect.”
Begun says that because celebrities and professional ath-letes have endorsed a gluten-free diet for everything from weight loss to improving athletic performance and even overall health, the trend has really taken off. But she says there’s no evidence to prove that removing gluten from the diet helps with any of this, and those who jump on the glu-ten-free bandwagon for one of these reasons alone may not be eating a healthier diet at all. The whole health-halo effect of the term “gluten-free” often misleads people to assume they’re eating a healthful diet when they’re not, Begun says. “Just because it’s gluten-free, doesn’t mean it’s healthful,” she adds.
And that’s certainly the case for fast food. Although fast-food restaurants now are touting more gluten-free choices, it doesn’t mean the food is healthful. But many consumers are duped into thinking that’s the case simply because of the association between gluten-free and the idea of good health. This is an important area in which dietitians can educate cli-ents and patients.
In addition, there are safety concerns of which clients need to be aware. There’s always a risk of cross-contact when restaurants are handling both gluten-free and gluten-containing foods.
Safe EatingMaintaining a strict, gluten-free diet isn’t always easy for
clients, particularly if someone else prepares their food. “If you’re eating gluten-free for a medical reason, such as celiac disease, you have to be very careful any time you dine out,” says Marlisa Brown, MS, RD, CDE, CDN, president of Total Wellness in Bay Shore, New York, and author of Gluten-Free Hassle-Free and Easy Gluten-Free. “A salad might be adver-tised as gluten-free, but what if the person who handled your salad forgot to change his or her gloves after handling a sandwich [that contained gluten]?”
White agrees there’s always the risk of cross-contact or cross-contamination when dining out. But in fast-food res-taurants, it might be an even higher risk. Factors such as a large amount of employee turnover and the hiring of younger, less experienced food handlers can prevent consistency in food preparation. “In fast-food restaurants, it’s likely that the workers haven’t had training on how to avoid contamination,”
BY LINDSEY GETZGluten-Free Fast Food May I Take Your Order Please?
august 2014 www.todaysdietitian.com 29

he says. “My best advice would be to keep the order simple and be very explicit in your instructions.”
Brown says that when it comes to fast-food dining, she advises against the drive-thru and urges individuals with celiac disease to go inside the restaurant and order their food. The drive-thru poses more possibility for cross-con-tamination to go unnoticed. “With fast food, you often can watch it being prepared because you can see the kitchen, and you can ask questions face to face,” she says. “But that’s only if you go inside. Obviously that takes away a little from the convenience factor, but it’s important to protect yourself.”
Going inside the restaurant also allows clients to use common sense. “If you go through the drive-thru, you never get a look at the inside of the place,” Brown says. “But if you walk inside, and the restaurant is very poorly kept and you can see that the kitchen
area is a wreck, common sense dictates that they’re probably not going to do the best job taking all the precautions with your food. That would be a good time to choose a different restaurant.”
In addition to scrutinizing the prep area, Brown says it’s important for people to communicate their needs with restau-rant staff members in advance and not wait for them to make a mistake before speaking up. “Explain that you will become ill with the smallest amount of gluten, and ask that the food han-dler change his gloves,” she advises. “Actually speaking to someone in person is going to be your best chance of having a safe experience. Trying to talk to someone through a drive-thru window isn’t good enough.”
Dubost agrees that communication is key any time clients dine out. “Go inside and talk to a manager or server to ensure they’re fully aware of your needs,” she says. “But also have a
Gluten-Free Offerings at Fast-Food ChainsBurger KingFour years ago, Burger King revealed a gluten-sensitive list as part of its BK Positive Steps campaign to provide more nutrition information on the chain’s menu items. The com-pany also switched ingredients to make its fries gluten-free. Although celiac disease patients have several choices, rang-ing from the Whopper patty to the Tendergrill chicken filet, the chain does note that fried items may still be fried with gluten-containing ingredients. Clients can find the full list at www.bk.com/cms/en/us/cms_out/digital_assets/files/pages/MenuGlutenFree.pdf.
Chick-fil-AChick-fil-A has provided information about allergens and its gluten-free offerings on its website (www.chick-fil-a.com/Food/Allergen-Gluten-Diabetic). Gluten-free diners can choose the Chargrilled chicken filet (no bun) or nuggets and several sides to avoid eating gluten. However, the chain makes it clear that it doesn’t have a gluten-free prep area in its kitchens.
KFCKnown for its fried chicken, individuals with celiac disease and nonceliac gluten sensitivity will find it difficult to eat at KFC because all of the fried chicken items and the sandwiches con-tain gluten. Diners may be able to choose from the side dishes or salads. The information is available online at www.kfc.com/nutrition/pdf/kfc_allergens.pdf.
McDonald’sMcDonald’s doesn’t offer a gluten-free menu nor does the chain list gluten-free menu items. The chain encourages customers to visit its website and review all ingredients, since they change periodically. McDonald’s also urges customers to seek physician guidance due to the “individualized nature of food allergies and food sensitivities.” Ingredient information can be found at www.mcdonalds.com.
Taco BellTaco Bell has information listed on its website under the “Food Allergens & Sensitivities” tab (www.tacobell.com/nutrition/allergens). A few of the gluten-free choices are the Cantina Bowls and sides. Like other chains, Taco Bell warns that gluten-free food may be prepared on the same equipment as gluten-containing food.
Wendy’sWendy’s publishes a link to its gluten-free menu on its website (www.wendys.com/redesign/wendys/pdf/en_US_gluten_free_list.pdf). Its signature sides such as chili and the baked potato both are on the list as well as several salads and meats.
— LG
30 today’s dietitian august 2014

plan before you even get there. Look at their menu online and know what gluten-free options are available.”
Although reading menus ahead of time and going inside the restaurant vs. using the drive-thru seem to defeat the purpose of fast food, these are important steps for clients to ensure safety. Brown says doing advanced planning is easier than ever before with advances in technology and the many gluten-free menus available online. “There are now apps available that can help you find restaurants with gluten-free options even when you’re out and about,” she says. “An app allows you to look things up quickly and still get the convenience factor of eating on the go. It’s not like you have to do your research at home. Smartphones make it a lot easier to eat gluten-free on the road.”
Consumers who eat fast food need to remember that even if they did their homework about a restaurant in the past, they’ll need to do it again because menus are subject to frequent changes. This is why some fast-food restaurants don’t commit to offering gluten-free food. “Some restaurants such as McDon-ald’s don’t have a gluten-free menu because they frequently change their ingredients,” White says. “It’s always a good idea to check the websites the day you’re going somewhere in order to make sure that what you’re selecting truly is gluten-free.”
Cindy Goody, PhD, MBA, RDN, LDN, senior director of the nutrition/menu innovation team for McDonald’s USA, says the chain always encourages diners to visit its website for the most current information available, particularly since ingredients periodically change. At this time, Goody says the chain doesn’t offer a gluten-free menu or list of items but does encourage customers to do their own research. “By accessing the ingredient statement listing on our website, individuals can determine if there are any ingredients or food allergens to which they’re personally sensitive,” she says. “But we also want you to know that despite taking precautions, normal kitchen operations may involve some shared cooking and preparation equipment, areas, and utensils, and the possibility exists for food and beverage items to come into contact with other food products, including allergens.”
Choosing a RestaurantThe potential for cross-contamination is a common sce-
nario. Begun says that many restaurants offer gluten-free items on their menu but aren’t taking the extra steps needed to separate gluten-free food preparation areas from the gen-eral preparation areas. However, there are some restaurants that take serving gluten-free foods seriously. They go the extra mile to train employees about preventing cross-contact in the kitchen and front of house. The fact that a restaurant trains its employees in this regard may not be advertised, but according to Begun, it’s easy to determine. “To the person that has to avoid even the smallest amount of gluten, it’s usu-ally pretty obvious if the restaurant associates have been trained,” she says.
Which restaurants have the best employee training pro-grams varies, but in general, Angela Lemond, RDN, CSP, LD, a wellness coach in Plano, Texas, and spokesperson for the Academy, says specialty restaurants may know more about their ingredients if they make foods from scratch because they know exactly what’s in them. Of course, that’s not the case with fast-food restaurants. “In general, chain restaurants have a tendency to have more premarinated or preseasoned foods that just need to be heated up, and those foods will have many more questionable ingredients,” she says.
However, one positive about fast-food menus is the consistency of ingredients from chain to chain. “Chains may have more of a uni-versal ingredient menu produced from a national headquarters, which is helpful in determining what’s in a menu item,” she adds.
Of course, Lemond notes that it ultimately comes down to the people working at a particular restaurant, as they deter-mine whether individuals who must avoid gluten can safely eat there. “The bottom line is that having a successful din-ing-out experience is largely impacted by the individuals will-ing to work with you at the specific restaurant you go to,” she says. “They need to have the knowledge to decipher their own menu’s ingredients.”
Some fast-food restaurants do a better job of promoting their gluten-free message than others and therefore are more popu-lar with people who have celiac disease or nonceliac gluten sen-sitivity. But even that doesn’t always mean they’re doing a better job of preparing gluten-free items. Diners who must eat gluten-free still need to do their homework and ask the right questions.
White says that Wendy’s appears to be a popular choice for gluten-free dining, and the chain has done a good job promoting their gluten-free items. “According to Wendy’s, their trademark baked potato is gluten-free as well as their chili and the popular chocolate and vanilla Frostys,” White says. “The salads can be ordered without the croutons, although for true celiac patients this may not be good enough. Most of their salad dressings are also gluten-free.”
What Lies AheadWhile the gluten-free food trend is booming, Dubost says
when the FDA begins enforcing regulations surrounding the definition of gluten-free this month, the number of restau-rants boasting these options may decrease. “They will have to comply with strict regulatory definitions, and for some, that simply may not be worth the risk,” she says. “It’s not easy for restaurants to ensure a gluten-free dining expe-rience. They can work with their suppliers and their ingre-dients, but there’s also prep and handling to worry about. Those that continue to offer gluten-free options are going to be those that are truly committed.”
— Lindsey Getz is a freelance writer based in Royersford, Pennsylvania.
august 2014 www.todaysdietitian.com 31

A Review of the Benefits of Probiotics, the Top Sources, and What’s New in the Dairy Case
By JULIANN SCHAEFFER
Dairy’s Probiotic Power

t any given time, hundreds of species of bacteria—both potentially harmful and potentially helpful—inhabit the human digestive tract. Probiotics are the “friendly” types that help to ferment, decompose, and digest the foods we consume.
Thus far, research has suggested that there’s potential in how certain probiotic strains may help aid certain ailments. “Research has shown that certain strains of bacteria may help promote good digestion (eg, lactobacillus and bifidobacterium), boost the immune system (eg, Bifidobacterium bifidum and Streptococcus thermophilus prevented rotavirus infection), and fight infections (eg, Lactobacillus GG to treat Clostridium difficile),” says Sherry Coleman Collins, MS, RDN, LD, owner of Southern Fried Nutrition Services in suburban Atlanta.
What’s more, research is examining probiotics’ potential effects on digestive disorders such as irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD) as well as how a certain strain of the beneficial bugs even may help lower cholesterol. “Probiotics have a very good safety record and have been successfully used with patients suffering from a variety of illnesses and compromised immune systems,” Collins says, adding that she still recommends that all clients who are interested in starting a regular probiotics regimen to treat disease first consult their physician.
Though Collins notes that the current evidence may support probiotic consumption for many different health benefits, she cautions that the research has yet to confirm these findings “since there aren’t studies looking at ‘deficiencies’ among those who don’t consume probiotics,” she says.
Joanne Slavin, PhD, RD, a professor at the University of Minnesota and a nutrition researcher, agrees: “We don’t have great intake data on probiotics, so it’s difficult to show rela-tionships between intake of probiotics and health outcomes.” Since there are no universally accepted methods to measure probiotic intake, she says this also makes it difficult to rank or compare products.
Nevertheless, it’s well known that dairy is one of the main healthful sources of probiotics, with yogurt being the most pop-ular among consumers. And if probiotic curiosity leads more people to include yogurt in their diet, Slavin says that isn’t bad. Here, dietitians discuss dairy’s probiotic prowess, which prod-ucts are the best sources, and what’s new in the dairy case.
Dairy’s BenefitsDairy is one of the most regularly accessible and acceptable
food categories that contain probiotics, Collins says. That, with its overall nutrient profile, makes it a great form in which to consume probiotics. “When working with clients, I always try to encourage them to choose foods that are nutritionally dense, and dairy is one of those foods,” she says.
“In addition, there’s some evidence that foods that provide probiotics and prebiotics [nondigestible parts of foods that
become fuel for probiotics] may enhance mineral absorption,” she adds. “Therefore, eating yogurt and other probiotic dairy foods may help ensure that calcium and other minerals in dairy yogurt are absorbed.”
Yogurt also is a great vehicle for getting probiotics, Collins says, because of the nutrient profile of cow’s milk. And for people, particularly kids, who don’t like milk, yogurt provides another way to get the vitamins and minerals in cow’s milk into their system. “While many things [such as sauerkraut, miso, and tempeh] can be fermented to produce healthful live active cultures, cow’s milk packs a powerful vitamin and mineral profile along with the gut-restoring probiotics,” says Christa Byrd, MA, RD, a clinical dietitian at Beaumont Health System in Royal Oak, Michigan. “[But] yogurt is better tolerated by people who are lactose intolerant because the bacteria digest the lactose or milk sugar while fermenting the milk, which produces increased lactic acid and decreased lactose.” According to Slavin, yogurt is particularly beneficial for children who don’t like the taste of cow’s milk because yogurt provides high-quality protein, vitamin D, and calcium.
According to Kristin Kirkpatrick, MS, RD, LD, manager of wellness nutrition services at the Cleveland Clinic, yogurt’s accessibility and familiarity make it a great starting point for most people looking for probiotics, and many varieties offer a big probiotic punch. “Yogurt and kefir will have the most probiotics,” she says.
Because heat kills the bacteria in yogurt, Kirkpatrick recommends researching whether a particular brand has been heated after production or just look for the “live and active cultures” seal to ensure there’s enough probiotics to provide any potential benefit. “Yogurt and most probiotic-containing drinks aren’t heated before serving, so they’ll be the most reliable sources,” she says.
What’s New on Store ShelvesAs the media spotlight continues to shine its healthy halo on
the probiotic buzzword, food companies continue to offer con-sumers new ways to get their daily dose of the beneficial bugs. New yogurt flavors, single-shot probiotic drinks, and frozen kefir bars are just a few of the new forms probiotics are taking at the grocery store today. Dietitians speak out on the latest probiotic dairy trends as well as provide tips on how to recom-mend clients incorporate these bugs into their daily meals.
Yogurt“Because yogurt is available in every supermarket and
many convenience stores and even fast-food restaurants, Americans have easy access to probiotics via this favorite food,” Collins says.
By far, yogurt also offers the most flavor and texture options. Even so, she says it’s important to consider quality when surveying for probiotic content. “While yogurt may be available almost everywhere, the practitioner should know
A
august 2014 www.todaysdietitian.com 33

that good-quality yogurt with multiple strains of bacteria and live, active cultures must be eaten to get the best benefit,” Collins says. “Bacteria in foods is sensitive to time and tem-perature, so if it’s improperly stored, the bacteria may not be alive or in adequate amounts to be of benefit.”
Yes, yogurt generally has the greatest amount of probiotic content, says Janet Colson, PhD, RD, a professor of nutrition and food science at Middle Tennessee State University in Murfreesboro, but bacteria strains and numbers will vary by brand, so she recommends clients know their yogurt before purchasing. “The ingredient label indicates the strain but not the number of bacteria,” she notes.
In general, Colson says the number of live bacteria likely will decrease as the yogurt sits in the refrigerator, so fresh is best. “In some cases, the bacterial content increases [as yogurt sits], which depends on the strain of bacteria,” she says, noting that this isn’t the case for the majority of probiotic-containing yogurts. The bacteria Lactobacillus rhamnosus (found mainly in Stonyfield yogurt varieties) tends to be more stable during storage than other bacteria.
Colson says the leading yogurt trend she’s seen lately is the increased types of bacteria that food companies are offering in yogurt varieties as well as additional flavor options. “Lacto-bacillus bulgaricus and Streptococcus thermophilus are the only two cultures required by law to be present in yogurt. However, many yogurts have more than these two,” she says.
Greek yogurt continues to increase in popularity, so it’s no surprise that many of the latest product innovations are coming from Greek (or similar) varieties. According to Byrd, Greek yogurt is her go-to patient recommendation, particularly for wound healing. “When dealing with underweight patients in the clinical setting who have increased protein needs for wound healing, yogurt is my No. 1 supplement recommenda-tion, especially Greek yogurt, which packs a powerful 13 g of protein per 100-kcal serving,” she says.
“Yogurt is a great option because pressure sores and unintended weight loss are commonly seen in the elderly, who also are more likely to be lactose intolerant,” she adds. “The low-lactose profile of yogurt makes it helpful and easy to digest. Yogurt also is a low-cost supplement, which is easy to find in a variety of flavors that patients can easily continue [to consume] at home.”
In addition to the starter cultures, Stonyfield products con-tain three other probiotic cultures: Lactobacillus acidophilus, Bifidus, and Lactobacillus casei. Stonyfield, which recently introduced a creamier texture to its line of organic Greek yogurt, now offers two new flavors: Black Cherry and Café Latte. Cobranded with Happy Family, Stonyfield also recently launched yogurt pouches for the younger set under the pre-existing brand names YoBaby, YoTots, and YoKids, all of which contain the same probiotic strains as its other yogurt products.
YoBaby pouches offer whole-milk yogurt in four varieties, including Blueberry and Mango, with fish oil–sourced DHA and
EPA omega-3 fatty acids. YoTots offers a similar yogurt for-mulation with slightly more adventurous veggie-fruit options, such as Pear Spinach Mango, meant to introduce toddlers to new flavors. And YoKids pouches feature low-fat yogurt in Blueberry, Strawberry, and Strawberry Banana flavors.
Three Happy Cows, another Greek yogurt company that uses a blend of probiotic strains, recently launched Strawberry, Blueberry, Caramel, and Vanilla Bean flavors, with 11 to 12 g of sugar and 15 g of protein in each serving.
Greek yogurt manufacturer Chobani, which includes three strains of probiotics in all of its products, introduced a range of new options this summer. In addition to a dessertlike full-fat line called Chobani Indulgent, the company is offering a new line called Chobani Greek Yogurt Oats, made with real fruit and whole grain steel-cut oats for added fiber.
For weight-conscious consumers, Chobani Simply 100 Greek Yogurt offers 100-kcal varieties in Key Lime and Pine-apple Coconut, and Chobani Kids offers kids a low-fat, low-sugar Greek yogurt line with flavors such as Grape and Watermelon. Chobani’s Seasonal line, with Watermelon and Pink Grapefruit highlighting the summer’s freshest flavors, also is new, as is its 4% whole milk Chobani Kitchen, which is touted as perfect for baking.
A relative newcomer to the yogurt section, Noosa Yoghurt describes itself as an Aussie-style yogurt that’s plenty thick and paired with fresh fruit purées and honey in addition to a blend of probiotics. Its yogurts contain a blend of five cultures (the same strains Stonyfield products offer) and new flavors include Pineapple and Coconut as well as a Plain variety.
For clients who can’t (or choose not to) eat dairy, Kirkpatrick says there are soy- and coconut-based yogurts that also provide probiotics. Byrd likes Trader Joe’s Coconut Yogurt for people with a milk protein allergy. “It’s a good fermented snack with active cultures, although it contains a little less protein than other yogurts,” she says.
With so many new brands and product lines filling the yogurt case, where should clients look for the most benefit? According to Colson, the most important thing is to guide clients toward live, active cultures first and low sugar next. “I personally only select plain fat-free yogurt and use it in place of sour cream on vegetables or a casserole and for whipped topping on fruits,” she says.
Research has yet to determine which probiotic strains can elicit specific benefits, but Colson says when it comes to look-ing at ingredient labels, the more bacteria strains a yogurt contains, the better. (Both Stonyfield and Noosa yogurts con-tain five strains, whereas many varieties offer two to three.)
“I would avoid selecting a yogurt that has too many added sugars, candy, or cookies—basically, the dessert type,” she adds. “People can easily gain an excessive amount of weight by eating yogurt for the health benefits and end up having so much added sugar and fat that the detriments outweigh any possible health benefits.”
2014 NASPGHAN Nutrition SymposiumSaturday, October 25, 2014 • Hilton Atlanta, Atlanta, GA
Explore our resources for you, your patients and families:www.GIKIDs.org
We are pleased to announce the launch of
The NASPGHAN Council for
Pediatric Nutrition Professionals
JOIN:
www.naspghan.org/nutritionpros
Join by 9/15/2014, for $25 and
receive $50 off your registration for the
2014 NASPGHAN Nutrition Symposium
REGISTRATION: www.naspghan.org
The North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) presents:
TDad_2014b.indd 1 6/25/14 4:19 PM
34 today’s dietitian august 2014

It’s also easy for clients to spend more cash than they intended when looking for new yogurt options, but Kirkpatrick says a steady eye can solve that problem. She tells clients to “read the ingredients. Buying an off-brand yogurt containing the same species of probiotics as the name brand will still provide the same benefit.” She also notes that yogurt can be the most cost-effective way to get their daily probiotics, if consumers shop carefully.
Collins agrees: “There are some store brands that are as robust in the strains of bacteria as the more expensive name brands. Looking for sales and coupons is always a good tip for saving bucks at the grocery store.”
Probiotic Dairy DrinksWhile not as widely known or loved as yogurt, the yogurt-
like probiotic drink kefir is gaining in popularity. Collins says kefir is available in most supermarkets and specialty nutrition stores, and with far more strains of bacteria than yogurt, she says kefir is a delicious drinkable dose of probiotics. “Kefir typically contains 10 different strains of bacteria,” she says.
Lifeway, which makes a range of kefir products that all offer its blend of 12 probiotic cultures, has introduced a few ways for people to enjoy its probiotic drinks. Veggie Kefir is a savory alternative to fruit-flavored kefirs. A new blend of vegetable juices and kefir, it delivers one full serving of
vegetables as well as the full nutritional kick of kefir per 8-oz glass. It comes in Tomato, Cucumber, and Beet varieties.
Lifeway’s Kefir With Oats provides consumers with 1.5 g of soluble oat powder mixed with kefir. With a smooth texture and a hint of oat flavor, Kefir With Oats offers 11 g of complete protein in breakfast-friendly flavors such as Blueberry Maple, Cinnamon Apple, and Vanilla Plum. For clients watching their sugar intake, Lifeway offers Perfect 12 Kefir, which is sweetened with stevia and has no added sugar and only 12 g of carbs.
In addition to kefirs, there are drinkable yogurts available that offer probiotics as well. California-based GlenOaks Farms, which debuted the first drinkable yogurt in the 1980s, recently introduced GlenOaks Drinkable GREEK STYLE Yogurt, offering more protein in addition to its live and active cultures in Peach, Raspberry, and Strawberry flavors.
Collins also has seen a trend in drinkable yogurt products specifically designed to be probiotic “shots” that pack lots of probiotics into small quantities. One such option is Bio-K+, a liquid probiotic that uses dairy, soy, and rice to make its formula of 50 billion bacteria, which it packs into a single-serving shot of sorts. The bottle is more akin to the size of a small yogurt container and can be consumed in one serving. Or individuals can consume one-quarter to one-half of the drink at a time and still reap the probiotic benefits.
2014 NASPGHAN Nutrition SymposiumSaturday, October 25, 2014 • Hilton Atlanta, Atlanta, GA
Explore our resources for you, your patients and families:www.GIKIDs.org
We are pleased to announce the launch of
The NASPGHAN Council for
Pediatric Nutrition Professionals
JOIN:
www.naspghan.org/nutritionpros
Join by 9/15/2014, for $25 and
receive $50 off your registration for the
2014 NASPGHAN Nutrition Symposium
REGISTRATION: www.naspghan.org
The North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) presents:
TDad_2014b.indd 1 6/25/14 4:19 PM

Cheeses and SpreadsEven though all cheese (except processed) is fermented,
Byrd says, that doesn’t mean all varieties contain probiotics, and those that do may not survive conditions in the gastroin-testinal tract. Because of this, she says it’s just as important for clients to check the labels for live and active cultures on any product they believe has probiotic cultures.
A relatively new player in the probiotic category, and a potentially new way to entice clients to consume probiotics, are yogurt and cream cheese spreads. Sonya Angelone, MS, RDN, CLT, a spokesperson for the Academy of Nutrition and Dietet-ics, likes the cream cheese and yogurt spread from Green Mountain Farms, which comes in individual 1-oz containers for convenience. “Although a bit more expensive than buying one large container and portioning out a serving, it may make the difference between eating it and not eating it,” she says.
Angelone likes suggesting clients try the spread on bagels, wraps, sandwiches, celery sticks, and even in smoothies. Whereas regular cream cheese provides about 10 g of fat and 1 g of protein with 100 kcal/oz (with no probiotics), Green Mountain spread has “4 g of protein, 3.5 g of fat, and 60 kcal/oz with live and active cultures,” she says.
For fruit aficionados, discount retailer Aldi recently rolled out a Greek yogurt fruit dip that blends Greek yogurt and cream cheese and contains live and active cultures. In two flavors, Strawberry and Vanilla Bean, each serving provides 4 g of fat, 2 g of protein, and 70 kcal.
Karoun Dairies also introduced its healthier alternative to cream cheese called Blue Isle Mediterranean Yogurt Spreads. Similar in consistency to cream cheese, the spreads contain
6 g of fat, 1 g of protein, and 60 to 70 kcal in addition to its pro-biotic blend. Blue Isle spreads come in five varieties: Blue-berry, French Onion, Honey, Original, and Spicy Vegetable.
Karoun Dairies also offers a line of flavored soft yogurt cheeses called Karoun Labne. This line of Mediterranean-style spreadable cheese also contains live and active cultures and comes in Creamy Ranch, French Onion, and Spicy Garden Vegetables.
Frozen OfferingsThe frozen foods aisle also contains probiotic-containing
dairy products. “Frozen Greek yogurt has become very popular, and frozen kefir is now available,” Kirkpatrick says. Various companies, including Lifeway, are offering frozen kefir bars/ice creams, but Kirkpatrick cautions clients and patients who may want to consume such tasty-sounding products as the main source of their probiotics.
While noting that frozen products still can have the live and active cultures seal if they contain enough viable bacteria per gram at the time of production, she urges clients to see such ice cream–like options for what they are: dessert. “I wouldn’t recommend these as a main source of probiotics. They’re desserts and should be consumed in moderation,” she says.
Counseling TakeawayWhether clients seek to get their probiotics from a single-
serving shot, a spoonable yogurt, or even a spread on their morning bagel, Byrd says her advice to clients is similar: Look to include fermented foods in your diet three times per week, and avoid added sugars whenever possible. “Use caution with products containing increased sugar, as this may not only add empty calories, but it may negate some of the healthful gastrointestinal benefits,” she says. “Excessive sugar intake also can disrupt the balance of healthful bacteria that works to breakdown and digest the foods we eat by increasing the gas-producing [bloating] fungal inhabitants.”
In general, Collins recommends most clients consume 6 to 8 oz of plain yogurt or 4 oz of kefir per day to maintain good digestion, upping that recommendation to twice per day if a client seeks to prevent antibiotic-induced diarrhea, for example.
“I recommend my clients choose a yogurt with the most different strains of bacteria—five or more—since different bacteria seem to have different positive health benefits,” she says. “Buying the freshest yogurt available helps ensure live and active cultures, and avoid those with added stabilizers and gelatin, since quality yogurt doesn’t need those added ingredients to be thick and creamy.”
— Juliann Schaeffer is a freelance writer and editor based in Alburtis, Pennsylvania,
and a frequent contributor to Today’s Dietitian.
36 today’s dietitian august 2014

Do you wish to begin or renew your subscription to Today’s Dietitian?❑ YES, please begin/renew my subscription. ❑ No thanks.
Signature______________________________________________________________________ Date________________Signature and date required for processing. Incomplete forms will not be processed.
Name_____________________________________________________________________________________________
Phone_____________________________________________________________________________________________
Facility_____________________________________________________________________________________________
Address_____________________________________________________________________________________________
City____________________________________________________ State__________________ Zip_________________
E-mail*____________________________________________________________________________________________
*E-mail address will primarily be used for renewals, e-newsletters, and digital editions.
❑ 1 Year - $14.99 (12 issues) ❑ 2 Years - $28.50 (24 issues) ❑ 3 Years - $39.99 (36 issues)For print subscriptions in Canada or other locations outside the U.S., please e-mail or call for pricing. Subscriptions are nonrefundable.
Payment Options (select one): ❑ Check made out to Today’s Dietitian ❑ Money Order ❑ Visa ❑ MasterCard ❑ AMEX
Credit Card No.____________________________________ Security Code_______________ Exp.Date___________________
SUBSCRIBE or RENEW Now and SAVE!
Today’s Dietitian contains practical articles loaded with
information that every nutrition professional needs to know
PLUS the opportunity to earn 2 CE credits by reading the
CPE Monthly article and taking a short online exam.
CHOOSE THE DESIGNATION THAT BEST DESCRIBES YOUR CREDENTIALS:
❑ RD❑ RDE❑ DTR❑ LD❑ CDM❑ CDE❑ Other____________________
CHOOSE THE TITLE THAT BEST DESCRIBES YOU:
❑ Foodservice Manager❑ Clinical Nutrition Manager❑ Consultant Dietitian❑ Dietetic Technician❑ Educator❑ Dietitian in Private Practice❑ Clinical Dietitian❑ Food and Culinary Professional❑ Director❑ Student❑ Other____________________
CHOOSE YOUR WORK SETTING:
❑ Hospital❑ Nursing Home/Long-Term Care Facility❑ State Dept. of Public Health❑ HMO❑ College/University/School District❑ Government Agency❑ Food Company❑ Pharmaceutical Company❑ Nutrition-Related Company❑ Hotel❑ Correctional Facility❑ Other____________________
INCOMPLETE FORMS WILL NOT BE PROCESSED. CODE: 072814
THREE EASY WAYS TO SUBSCRIBE OR RENEW:Online at www.TodaysDietitian.com • Fax this form to 610-819-1214 • Mail form and payment to
Today’s Dietitian, 3801 Schuylkill Road, Spring City, PA 19475
SILENT CELIAC DISEASE
Atypical Signs and Symptoms
Often Delay Proper Diagnosis
and Treatment
INSIDE
Gluten-Free Resource
Guide
Experts Decipher
the Farm Bill’s Impact
Can Overweight RDs
Still Be Effective?
Spring Symposium Issue
www.TodaysDietitian.com
May 2014
Vol. 16 No. 5
The Magazine for Nutrition Professionals
May 2014y
Vol. 16 No. 5
Thee MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaagggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaazzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzziiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiinnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnneeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeee ffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffoooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooorrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrr NNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuutttttttttttttttttttttttttttttttttttttttttttttttttttttttttttrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrition Professionals
Th
National Celiac Disease Awareness Month
TTT AASSASESSSSE
ssee
TTTEAs s
Diseas
June 2014
Vol. 16 No. 6
The Magazine for Nutrition Professionals
CONFERENCE ISSUE
5 Summer Foodservice Programs for Kids
Dairy’s Value in Disease Prevention
MEN’S HEALTH MONTHFEATURING
Men in Dietetics
Men’s Fitness
INSIDEGluten-Free Showcase
AthletesProtein Intake
and
Experts Discuss Whether the RDA Is Adequate
www.TodaysDietitian.com
Men in Dietetics
Men’s Fitnessakes
DA
an.comwww.TodaysDietitia
Substituting Palm OilTrans FatIs Palm Oil a Good Alternative
for Human Health and the Environment?
for
Spring SymposiumHighlights
Diabetes andCardiovascular DamageTips for Adding More
Veggies at BreakfastRDs Debate the FDA’s
Proposed Nutrition Facts Label
July 2014
Vol. 16 No. 7
The Magazine for Nutrition Professionals
CONFERENCE ISSUE
www.TodaysDietitian.com
Phone: 800-278-4400 • E-mail: [email protected]
www.TodaysDietitian.comwww.TodaysDietitian.com
TD_2014_Subform.indd 1 7/22/14 10:11 AM

Learn What It Takes to Get Started and Become Successful
By LORI ZANTESON
Building a Career Through
Public Speaking

sk nutrition professionals today how they’re pro-moting their businesses and brands and spread-ing nutrition messages, and most will probably tell you they’re doing this through social media outlets such as Facebook, Twitter, and Pinterest;
websites; blogs; videos; and even writing books. Others will say they’re taking advantage of public speaking opportunities as well to further expand their professional influence, boost their income, and take their careers to a higher level.
Many dietitians start small by speaking at venues such as local and regional conferences, neighborhood hospitals, non-profit organizations, schools, local chambers of commerce, community education events, and faith-based organizations. Many participate in public seminars, webinars, and corporate speaking and eventually go on to deliver keynote addresses and presentations at national meetings.
Today’s Dietitian interviewed RDs with public speaking experi-ence who discuss what it takes to get started, how to set goals, and the importance of choosing a specialty for long-term success.
Taking the First StepBecause there are many different public speaking paths
dietitians can take to complement their business, including becoming a consultant or coach, it’s best to determine what you want to accomplish and set business goals. “Do you want to get more clients, diversify your revenue, increase exposure?” asks Stacy Tetschner, CAE, CEO of the National Speakers Association in Tempe, Arizona.
According to Michelle May, MD, CSP, a Phoenix-based motivational wellness speaker, the founder of Am I Hungry? Mindful Eating Programs and Training, and the author of Eat What You Love, Love What You Eat: How to Break Your Eat-Repent-Repeat Cycle, dietitians need to ask themselves why they want to do public speaking. “Everyone always has to start with why. You have to know why because that helps find your audience,” she says.
For example, if a dietitian’s goal is to build her practice, she can look locally for prospective clients at community events, mothers’ groups, support groups, or corporate lunch and learns. “A dietitian is well qualified to speak at these [venues]. Being a dietitian is the perfect segue into a variety of topics,” May says.
A retired family physician, May had a medical practice for 16 years. When she started the mindful eating program Am I Hungry? in 1999, she gradually transitioned to become a full-time entrepreneur, helping others run mindful eating pro-grams. She started speaking publicly to health professionals in 2000 to share information about mindful eating and how it could help their patients and clients as well as at community and corporate wellness events and at many other programs to help individuals. “We also train dietitians in mindful eating, so I speak at RD events. They might follow up with our facilitator training program or have patients or clients to refer to our programs or books,” she says.
As a member of the Arizona Academy of Family Physicians, May spoke at local chapter events, where she received valuable feedback while honing her speaking skills. She eventually applied to speak at the national convention, where she’d speak for the next 10 years. May recommends RDs turn to the Academy of Nutrition and Dietetics (the Academy) to get public speaking experience, starting with the local chapter and moving up to the state and eventually the national level.
Find Your NicheOnce dietitians have established why they’d like to do
public speaking, it’s important to develop a specialty for which they’d like to be known. Academy members can participate in the Speakers and Media specialty group, which is part of the Nutrition Entrepreneurs Dietetic Practice Group (DPG) composed of dietitians looking for support and mentoring from colleagues who are doing the same thing. (The speakers group has a mailing list, publishes newsletters, and provides networking opportunities with other practice groups at the Food & Nutrition Conference & Expo [FNCE].)
Karen Collins, MS, RDN, CDN, FAND, a speaker, writer, and consultant and the nutrition advisor for the American Institute for Cancer Research (AICR), joined this group early in her career. In fact, it was during one of the speakers’ meetings at FNCE that Collins was encouraged to specialize in a certain aspect of nutrition. “At first I wanted to be broad, but in order to be a speaker, [you should] be an expert on something, a subject matter such as weight control or a group like the elderly, kids, or people in business. I think it’s valuable to have a niche,” she says. Eventually, Collins specialized in cancer.
Early in her career, Collins spoke at group classes and hospital events and as a clinical instructor at Cornell Univer-sity, all of which helped build her confidence. Becoming the nutrition advisor for the AICR transitioned her from small to much larger conferences and audiences. “It’s a great way to reach out to people,” she says.
Over the years, as health professionals and cancer sur-vivors heard Collins speak publicly about the disease, she established herself as an expert and built a good reputation. “You have to have that expertise and speak on what you already know,” she says. “There’s something that’s very genuine. The audience can sense that your expertise comes from research and practical experience.”
Now that Collins is well established in her career and as a presenter, people approach her with speaking opportuni-ties. Even if she presented the topic before, Collins says she always customizes it to meet the needs of the audience. “You have to research the group, look on their website, and talk to people in the group to assess what they need and want to know about a topic,” she explains. “It takes a lot of time to craft a good proposal—before you even get the job—and then more time shaping a presentation that each particular audi-ence will find truly memorable.”
A
august 2014 www.todaysdietitian.com 39

Getting PaidWhen dietitians are hired to speak, it’s important for them
to determine how much they’re worth. “I spend enormous amounts of time” preparing for presentations, Collins says, including research and figuring out how to condense it, the take-home message, and the PowerPoint slides.
Tetschner suggests dietitians consider what they earn annually as an RD, determine how much time they’d have to give up to speak, then figure out how many times per year they’ll need to speak at a particular rate to net the amount of money they want to earn in one year.
However, dietitians shouldn’t expect to get paid for public speaking when they’re just starting out. In fact, many RDs begin speaking for free. “A person should never do paid [speaking] until he or she has done a ton of free [engage-ments]. Your reputation as a speaker is only as good as your last speech. Get really good and comfortable on the platform. No one will pay good fees for a so-so speech,” May says.
David Grotto, MS, RDN, LDN, president and founder of Nutrition Housecall in Chicago and author of The Best Things You Can Eat, 101 Foods That Could Save Your Life, and 101 Optimal Life Foods, agrees that speaking in front of as many audiences as one can is the most valuable way to get experience. “I did a lot of freebies in the beginning,” he says. “Early on, I’d speak for food—a meal provided with the event—in the hopes of drumming up my private practice. It can be a great public relations tool that may pay off in client referrals down the line.”
Unpaid speaking also can be lucrative in other ways. Grotto has experienced his audience members looking for dynamic speakers, which has led to more speaking opportunities. He’d ask these audience members to provide testimonials and make referrals that he’d use as marketing tools to get hired for other speaking events. “It’s worth its weight in gold—better than a PR company,” he says.
Another way to capitalize on free public speaking is to have a book to sell at the event, otherwise known as back-of-the-room sales. During speaking engagements, many dietitians sell books they’ve written and do well. “I found that my first book became a living, breathing business card for me,” Grotto says. “Being an author has huge appeal when people are looking for a speaker,” adding that he’s seen self-published books bring in six figures from back-of-the-room sales.
For authors who have publishers, arrangements can be made to allow the group or organization to buy several books at the wholesale price (typically 50% less than retail), and sales at the event would go toward supporting the organization. “It’s a win-win. You get credit for book sales, and you’re helping the event,” Grotto says.
Speaking for free often is easier to accept when you feel honored for being invited, says Barbara Ruhs, MS, RD, LDN, a retail food and health marketing communications specialist and former supermarket dietitian who currently operates the consulting business NeighborhoodNutrition.com. The event administrators may waive your conference fee and offer other perks, she says. “It’s always been about education and opportunities. I’ve been a leader in creating education opportunities for other supermarket dietitians. Others know this and seek me out,” she says.
In fact, Ruhs once received an all-expenses-paid trip to Japan to learn about probiotics and an invitation to tour behind the scenes at Grimmway Farms to see how they harvested carrots. “They know I’m vocal in this area and talk to lots of dietitians,” she says.
Resources for SpeakersOrganizations Supporting the Public Speaking Business •NationalSpeakersAssociation(www.nsaspeaker.org):Provides resources and education designed to advance the skills, integrity, and value of its members and the speaking profession. There are state and regional chapters throughout the United States.
•NutritionEntrepreneursDieteticPracticeGroup (http://nedpg.org/about), speakers and media specialty group: Represented in all 50 states, this group provides colleague support in the business of speaking profes-sionally on wellness and nutrition topics.
Training •ToastmastersInternational(www.toastmasters.org): Members improve their speaking and leadership skills by attending one of the more than 14,000 clubs worldwide.
•Publicspeakingclassesatyourlocaluniversityorcommunity college
Books •Power Speak by Dorothy Leeds
•Made to Stick by Chip Heath and Dan Heath
Websites •SixMinutes:SpeakingandPresentationSkills (http://sixminutes.dlugan.com): This site provides tips and strategies for developing presentation skills and becoming an effective and confident public speaker.
•TJWalker(www.tjwalker.com):Walkeristhehostof the top-rated YouTube channel devoted to public speaking and media training improvement. This site features helpful videos that address various aspects of public speaking skills.
40 today’s dietitian august 2014

As a coordinator for the Nutrition Education and Training Program, which is under the Child Nutrition Act, it was part of Ruhs’ job to teach school foodservice professionals how to comply with the National School Lunch Program nutrition guidelines. She has hosted conferences for dietitians and has had many television and print media opportunities. “In public health, you’re always looking for ways to maximize your impact. Media is a way to reach a lot of people,” she says.
When Ruhs became a supermarket dietitian 14 years ago, it was a natural fit. The media reached out to her as a local voice, and it was good marketing for both Ruhs and the supermarket for which she worked.
She says the most important part of public speaking is sharing what she’s learned with others. When she started her career as a supermarket dietitian, she saw a need for resources that would help supermarket dietitians do their jobs in the communities they served to the best of their abili-ties. She saw the opportunity to specialize in a particular niche, became the expert she was seeking, and now people seek her as a public speaker for supermarket dietitians.
While becoming an expert helps garner more speaking engagements, there’s much more to public speaking than meets the eye. “You build up a reputation, but you have to be relevant; you have to be front of mind,” Grotto says. In other words, you need to market yourself.
Grotto was busy completing his master’s degree program last year and noted the decrease in speaking engagements compared with the year before when he was actively promot-ing himself and doing more public speaking. “You never stop pitching. You have to get out there,” he says.
Honing the CraftWhile speaking in front of audiences comes naturally for some
dietitians, it doesn’t for others. Fortunately, there are plenty of resources to fine-tune and master the skill of public speaking. Toastmasters International, a world leader in communication and leadership development, helps professionals develop speak-ing skills and gives them practice in front of an audience.
Of course, there’s no better teacher than getting experience speaking in real life situations. “Ninety percent is the way you say it, 10% is what you say,” Grotto says. “The thing that seems to work the best is repetition. You’ll develop your style,” adding that he recommends nutrition professionals watch other speakers and note what they do that audiences enjoy.
In addition to the Nutrition Entrepreneurs DPG, the National Speakers Association can show professionals how to use speaking to make a living. “We help people gain the tools—the education and the professional community—they need,” Tetschner says, noting that people don’t have to do this on their own. There are 3,000 members of the organization who make speaking a full-time business. Those just starting out can find out who’s doing what they’d like to do and learn from their experiences, he says.
“Dietitians have expertise that people are interested in,” May says. “Speaking is a great way to help people, build your busi-ness, and help serve.” Dietitians need to set business goals, determine the ideal audience for their niche topic, and pitch it, she says. Start small and speak for free to get the experience and keep at it. Public speaking can give dietitians higher pro-files that can open doors and opportunities that not only can build their business and brand but elevate their careers.
— Lori Zanteson is a food, nutrition, and health writer based in Southern California.
Venues for Speaking Opportunities
Michelle May, MD, CSP, a Phoenix-based motivational wellness speaker, offers these suggestions:
• Adult education programs
• Businesses, small and large, local and national (or international)
• Chambers of commerce
• Charity fundraisers
• City visitors’ bureaus, meetings, and conventions listings
• Clubs (eg, women’s, business, special interest)
• Colleges and universities
• Community education
• Conferences and conventions
• Continuing education
• Corporate training programs
• Corporations
• Cruise ships
• Employee wellness programs
• Faith-based organizations
• Governments
• Hospitals
• Lunch and learns
• Nonprofits
• Professional or industry associations (Check out the Gale Encyclopedia of Associations which includes listings such as annual budget; upcoming state, regional, and national conferences; publications; and contact information.)
• Public seminars and workshops
• Schools, for kids, parents, teachers, and the administration
• Service groups
• Sponsored speeches at conferences and conventions
• Trade shows
• Youth/children’s organizations
august 2014 www.todaysdietitian.com 41

CARING FOR TODAY’S CANCER SURVIVORSBy Karen Collins, MS, RDN, CDN, FANDAppropriate nutrition and physical activity recommendations can enhance their long-term health and quality of life.
Many dietitians likely will work with cancer survivors at some point in their careers.1,2 As a result of multiple factors, includ-ing earlier detection and more effective treatments, 65.8% of cancer survivors today have passed the classic five-year sur-vival marker,3 and 40% have survived 10 years or more.2
These survivors face myriad nutrition-related challenges, including those caused by an increased risk of cancer recur-rence or the development of a second cancer, cardiovascu-lar disease (CVD), or other chronic diseases. Many experience long-lasting side effects of the cancer or its treatment or they develop late effects that begin months or years after initial treatment. According to the National Cancer Institute, individu-als are considered cancer survivors from the time of diagnosis through the balance of their lives.
This continuing education course focuses on cancer survivors’ nutrition-related issues following the conclusion of active cancer treatment. It reviews current diet, weight, and physical activity recommendations for cancer survivors. Nutrition-related challenges and questions survivors face after cancer treatment also are discussed, including how to support long-term health.
Recommendations for SurvivorsResearch on how nutrition, physical activity, and body com-
position affect cancer recurrence, the development of second primary cancers, and overall survival for cancer survivors still is limited. Nonetheless, evidence has accumulated that supports recommendations to enhance recovery and promote long-term health and quality of life. Among US survivors, approximately 50% had breast, prostate, or colorectal cancer,1 so these groups have been most widely studied. The attention to breast cancer survivors in this review reflects the availabil-ity of applicable research findings.
American Institute for Cancer Research (AICR) recommenda-tions state that after treatment, if possible and unless otherwise advised, survivors should aim to follow the organization’s cancer prevention recommendations for diet, physical activity, and healthy weight maintenance.4,5 As part of the Continuous Update Project, in which the AICR partners with the World Cancer Research Fund, systematic review and evidence-based recom-mendations for breast cancer survivors are in progress.
The American Cancer Society (ACS) issued guidelines on nutrition and physical activity specific to cancer survivors in 2012. The guidelines address survivors in general, although the journal article in which the guidelines are presented discusses issues unique to specific types of cancer.6
An American College of Sports Medicine roundtable of experts developed exercise guidelines for cancer survivors, published in 2010.7 Based on these guidelines, survivors are encouraged to follow the federal physical activity guidelines for all Americans, though in some cases certain modifications are necessary. All survivors are advised to avoid inactivity.
Sources providing more background on these recommen-dations and patient education materials to explain them are
CPE MONTHLY
COURSE CREDIT: 2 CPEUs
LEARNING OBJECTIVESAfter completing this continuing education course, nutrition professionals should be better able to:
1. Use current evidence-based diet, weight, and physical activity recommendations for cancer survivors to prioritize goals for their nutritional care.
2. Evaluate how changes in body fat and lean body mass may affect cancer survivors’ prognosis and how these changes may be addressed.
3. Use current research to address questions cancer survivors commonly pose regarding supplements and dietary choices said to be cancer protective.
Suggested CDR Learning Codes 3020, 4040, 5150; Level 2
42 today’s dietitian august 2014

provided in the resources list created as a companion to this article and available in the version of this article posted on the Today’s Dietitian website.
Protective Eating Pattern Vegetables, fruits, whole grains, and legumes form the core
of a diet that reduces the risk of cancer and heart disease. Plant foods that aren’t highly processed or refined provide a wide range of nutrients and phytochemicals that may act protec-tively throughout cancer development, influencing DNA repair, inflammation, cell proliferation, and cancer progression.4 Diets built around foods low in calorie density are recommended to avoid weight gain and support intentional weight loss.4,8
However, neither observational nor interventional studies have demonstrated a strong link between vegetable and fruit consumption and reduced cancer recurrence or mortality.6 The effects of a diet high in vegetables and fruits likely are influenced by personal characteristics such as hormonal status, genetics, gut microbiota, and medical treatment as well as how the diet is implemented, including the choice and preparation of vegetables and fruits, total calorie intake, and overall diet and lifestyle qual-ity.9-11 Studies examining the associations of vegetable and fruit consumption with health outcomes generally adjust for BMI, thus addressing benefits beyond a role in weight management.
The Women’s Healthy Eating & Living Study of early-stage breast cancer survivors found no difference in breast cancer recurrence or death between a control group and an inter-vention group eating a low-fat diet very high in vegetables and fruits.12 Within the control group, neither the consump-tion of five vegetables and fruits daily nor moderate physical activity alone was associated with lower mortality. However, compared with women who met neither standard, those who met both dietary and activity standards experienced almost 50% lower mortality.13
A link between higher dietary fat intake and cancer risk once suggested by observational data hasn’t held up with closer study,4 and associations with breast cancer outcomes generally disappear when results are adjusted for calorie intake, weight, or weight change.14,15
Limited studies on this topic among men diagnosed with prostate cancer show inconsistent results. Dietary recommen-dations from the AICR and the ACS don’t address fat consump-tion except to call for avoiding very high levels that contribute to obesity.4,6 The ACS recommends limiting saturated fat for heart health, noting limited data linking saturated fat with cancer risk or recurrence.6
The strongest evidence from observational studies regarding diet relates to the overall dietary patterns of cancer survivors. Among those with stage III colorectal cancer, a more Western diet, characterized by a high intake of meat, fat, refined grains, and desserts, has been linked with more than double the overall mortality and a nearly threefold increase in cancer recurrence or death.16 Among breast cancer survivors, no link to breast
cancer mortality or recurrence was seen, but those with the highest Western or unhealthful diet scores had more than two or three times the mortality from other causes than those with lowest scores.17,18 In the Nurses’ Health Study cohort, the major-ity of these other deaths were due to other cancers or CVD.17
Although a Western diet is associated with worse outcomes among colorectal cancer survivors, a prudent diet, characterized by a high intake of fruits, vegetables, poultry, and fish, hasn’t been linked to better cancer-specific outcomes or overall mortality.16
Among breast cancer survivors, higher scores for a healthy dietary pattern are inconsistent in association with lower breast cancer recurrence or mortality but are associated with a 28% to 46% reduction in other causes of mortality, which includes deaths from other cancers, CVD, and additional causes.17-19
Among a cohort of older female survivors of all cancer types, compared with lower scores, the highest scores for adherence to the dietary portion of the AICR recommendations to reduce cancer risk weren’t associated with decreased cancer mortality but were associated with 20% lower all-cause mortality.20
Weight and Body Composition Traditionally, nutritional care for cancer survivors has
focused on preventing and treating malnutrition and on regaining lost weight, and that remains true for some of them. However, many survivors today are overweight or obese at the time of their diagnosis and remain so following treatment. This reflects both the increased prevalence of obesity and its association with cancer risk and improvements in treatment and early diagnosis reducing unplanned weight loss.
Mounting evidence indicates that among cancer survivors, prediagnosis obesity increases the risk of cancer recurrence, cancer mortality, and all-cause mortality. These associations are most strongly documented for breast cancer,21-23 though overweight and obesity also are associated with a worse prognosis for colorectal and prostate cancer survivors.24-29 Obesity doesn’t increase the risk of prostate cancer, but higher BMI and adult weight gain increase the risk of aggressive forms of prostate cancer and related mortality.30
Summer SpecialCreate your own summer session schedule by selecting three or more 2-credit courses from the CE Learning Library course
catalog and applying coupon code SUMMER14 at checkout to receive a 20% discount. You do not have to complete all courses in one sitting. Courses will remain available in your account until
their expiration date. Coupon is valid until August 31, 2014.
Visit CE.TodaysDietitian.com.
august 2014 www.todaysdietitian.com 43

Obesity’s link to poor prognosis for cancer patients may relate to several mechanisms, including increased inflamma-tion and elevated levels of insulin and growth factors such as IGF-1 that promote cancer cell growth.24,31,32 Excess body fat increases adipose production of estrogen in postmenopausal women, raising levels that promote the growth of estrogen-sensitive cancers. Obesity also is associated with the risk of developing CVD, the primary cause of death among many cancer survivors.
People at a healthy weight when they’re diagnosed with cancer may gain weight during treatment and in the years that follow. Fatigue, depression, and insomnia can lead to decreased physical activity or increased calorie intake from using food to cope with these problems, which can result in weight gain. Some chemotherapy, hormone, and steroid medications also can cause undesirable weight gain.
One analysis showed that about 35% of breast cancer survivors experienced a 5% or larger weight gain two years after diagnosis.33 Yet in a review with a longer time horizon, about 70% gained weight during and after treatment, including those whose weight was stable during treatment.34 Weight gain now averages 8 to 10 lbs, which is less than in decades past, but larger gains aren’t unusual. Weight gain is linked with increased mortality from breast cancer, CVD, and all causes.33,35 Researchers generally conclude that avoiding weight gain is an appropriate evidence-based goal for all breast cancer survivors.33,35
Research is less clear about the value of promoting weight loss in cancer survivors. One study has linked modest weight loss by breast cancer survivors with reduced cancer recurrence,14 while another trial of breast cancer survivors showed that weight loss of 5% or more decreased insulin and bioavailable estrogen levels.36 Several studies have linked elevated insulin, insulin resistance, the metabolic syndrome, and abdominal obesity to more aggressive breast cancers and a greater risk of recurrence and death in breast cancer survivors.37,38
The ACS guidelines for cancer survivors encourage those who are overweight to achieve and maintain a healthy weight, if only for noncancer health benefits.6 Despite many reasons for overweight or obese cancer survivors to expect benefits from weight loss, little documentation of outcomes is available. An analysis of four prospective cohort studies of breast cancer survivors showed the lowest mortality rates in those who maintained a steady weight in the first few years following their diagnosis.33 Although breast cancer mortality wasn’t affected by weight gain or loss of 10% or more, overall mortality increased, apparently related to heart attack and stroke.33
It’s important for the health care team, including RDs, to differentiate between unintentional weight loss caused by deteriorating health or malnutrition vs. intentional, gradual weight loss. In the pooled analysis of breast cancer survivors, increased mortality among overweight and obese subjects
with a 10% or greater weight loss was limited to those with a history of smoking and occurred primarily in those with other chronic diseases. The study authors hypothesized that increased mortality was related to substantial loss of lean body mass, which is associated with negative cancer and cardiovascular outcomes.33
While RDs await the outcomes of more than two dozen intentional weight-loss intervention studies in cancer survivors now under way, they need to consider overall health and prognosis when assessing the weight and body composition of individual cancer survivors. Evidence supports advising cancer survivors to avoid undesirable weight gain.4,6 For those already overweight or obese, adopting healthful lifestyle habits to facilitate intentional weight loss after treatment may be a worthwhile goal, if not medically contraindicated and if efforts are made to retain or improve lean body mass through a gradual rate of weight loss and the inclusion of physical activity.5,6,39 Evidence suggests that beneficial effects on important biomarkers, such as insulin level, insulin resistance, markers of inflammation, and bioavailable estrogen, can be achieved with weight loss of 5% to 10%.6,40
Physical Activity Survivorship care has changed dramatically in its empha-
sis on physical activity. The strongest evidence involves breast cancer survivors, including several observational studies that link greater postdiagnosis physical activity with reduced all-cause mortality.41 Most studies find that, compared with less activity, moderate exercise such as brisk walking for 2.5 to six hours per week is linked with 25% to 50% reduced breast cancer mortality and possibly decreased recurrence.41-43
Physical activity also is associated with increased progres-sion-free survival and reduced recurrence, cancer mortality, and all-cause mortality in colorectal and prostate cancer survivors.41,44-46 Among survivors of all types of cancer in the Iowa Women’s Health Study cohort, adherence to the AICR’s physical activity recommendation was tied to lower all-cause, CVD, and cancer mortality.20
Interventions promoting physical activity consistently have demonstrated improved fitness, strength, and quality of life and decreased fatigue and sleep disturbances among survivors of various cancer types.47,48 An analysis of six interventional trials showed that early-stage cancer survivors who weren’t assigned to exercise experienced decreased fitness levels, while those in supervised exercise programs following treatment experienced improvements.49 Interventional trials of breast cancer survivors have demonstrated increased lean body mass, decreased body fat, and reduced levels of insulin and IGF-1.50-52 This is important since elevated insulin levels are linked to cell proliferation and cancer risk as well as the metabolic syndrome and cardiovascular risk.
44 today’s dietitian august 2014

An American College of Sports Medicine roundtable con-cluded that although physical activity’s effects on mortality and cancer recurrence are unclear, cancer survivors still should be advised to avoid inactivity since strong evidence supports benefits to functioning and quality of life.7 It’s within RDs’ scope of practice to discuss with patients general steps to increase physical activ-ity if they’re medically cleared to exercise.53 Referral to a certified cancer exercise trainer for detailed plans also can prove helpful.
Exercise goals and plans need to be tailored to each cancer survivor.54 Some survivors face issues that require modify-ing the type or amount of exercise that’s safe for them, such as anemia, compromised immune function, neuropathy, balance problems, an ostomy or indwelling catheter, cardiac comor-bidities, the presence of or risk factors for lymphedema, bone metastases, and decreased bone density as a result of hor-monal treatments.6,7,54
Common Challenges
Loss of Weight and Lean Body Mass Those who have survived cancers of the head, neck, and
lung are among those more likely to be malnourished and underweight when diagnosed and at risk of further weight loss. Loss of weight and lean body mass may result from disease, aggressive treatment, and side effects that limit patients’ ability to consume adequate calories. For these cancer survivors, nutrition care should aim for positive energy balance and adequate protein to preserve or rebuild lean body mass. Physical activity also is important to increase strength and endurance and, when tailored to individual needs, may help improve eating by enhancing appetite.
Weight alone doesn’t adequately reflect changes in lean body mass, which can dramatically decrease with aging and during cancer treatment. Low lean body mass, especially as part of sarcopenic obesity, is associated with poor health outcomes.55-57 Androgen deprivation therapy for prostate cancer promotes sarcopenic obesity. In one meta-analysis, body fat increased by an average of 7.7% and lean body mass decreased an average of 2.8% in conjunction with this therapy.58
Loss of lean body mass often is also seen in survivors of colon, breast, and childhood cancers. In the Health, Eating, Activity & Lifestyle Study of breast cancer survivors, sarcope-nia was associated with an almost threefold increase in overall mortality independent of treatment type, comorbidities, waist circumference, and total body fat.59
Physical activity, including resistance training, may help protect against the loss of lean body mass.60 More research is needed to clarify the optimal diet to support lean body mass among cancer survivors. Adequate protein and calories are essential, and research is under way regarding the potential for omega-3 fatty acids to help reduce muscle catabolism and the appropriate choices among protein sources to support muscle growth.61-63
Fatigue Among the most common and debilitating problems
cancer survivors face, cancer-related fatigue is a persistent tiredness not proportional to recent activity that interferes with usual functioning and isn’t alleviated with rest. Some survivors experience this fatigue even years after treatment is completed. Although it may appear without a clear cause, cancer-related fatigue can occur because of new or ongoing and potentially treatable medical problems such as thyroid, pulmonary, cardiac, or liver disorders; anemia; depression; poor appetite; and medications. Survivors are urged to discuss fatigue with their physicians.
Family members and friends often urge survivors with can-cer-related fatigue to rest more. While adequate sleep and rest are important, research strongly supports engaging in physi-cal activity to reduce cancer-related fatigue, and it’s one of the few evidence-based treatments currently available.64-66 Other research shows that additional, potentially helpful nonpharma-ceutical interventions include yoga, cognitive behavioral ther-apy, counseling, and relaxation techniques.
Nutrition consultation also is included in National Compre-hensive Cancer Network clinical practice guidelines for assess-ing and addressing cancer-related fatigue.67 The guidelines highlight the management of nutritional deficiencies that devel-oped during cancer treatment, adequate hydration, and electro-lyte balance to prevent and treat fatigue.
Few published trials have tested nutrition interventions for cancer-related fatigue, though. Dietary adjustments beyond those in the National Comprehensive Cancer Network guide-lines that also may help include consuming five or six mini meals, distributing calories evenly through the day, or consum-ing larger amounts of calories earlier in the day. Education is vital to reinforce that mini meals aren’t snacks but nutritionally balanced meals that provide complex carbohydrates, a small amount of heart-healthy fat, and a protein source.
Although research is lacking, anecdotal data from dietitians working with cancer survivors suggest that high-fiber, whole-food carbohydrate choices distributed throughout the day can help survivors maintain their energy level and avoid fatigue related to blood sugar swings. These data also are consistent with guidelines to promote overall health.
Other Posttreatment Challenges Cancer survivors typically recover from the acute effects of
their treatment within weeks or months after treatment ends. In some cases, however, side effects of treatment persist, such as taste changes, odynophagia (painful swallowing), dysphagia (difficulty swallowing), xerostomia (dry mouth caused by a lack of saliva), enteritis, diarrhea, constipation, and other concerns that can challenge nutritional status. The websites of the National Cancer Institute (www.cancer.gov), the ACS (www.cancer.org), the AICR (www.aicr.org), the American Society of Clinical Oncology (www.cancer.net), and the Oncology Nutrition
august 2014 www.todaysdietitian.com 45

Dietetic Practice Group of the Academy of Nutrition and Dietetics (www.oncologynutrition.org/erfc) provide practical tips for handling such problems. In addition, dietitians who are board-certified oncology nutrition specialists (those with the CSO credential) have special expertise in this area and are excellent resources.
Questions About Supplement Use Supplements are more widely used among cancer
survivors than by the general public.68,69 However, currently there’s no consistent evidence indicating that dietary supplements reduce the risk of cancer recurrence or improve a person’s odds of survival.4,6 Nevertheless, supplements can help reduce nutrient inadequacies, though research is identifying U-shaped curves for an increasing number of nutrients, meaning that inadequacy and excess both may pose risks. The risks vary depending on the nutrient but may include increased risk of various cancer types, diabetes, and all-cause mortality.
Emerging data suggest certain supplements may help sur-vivors deal with the side effects of cancer or its treatment. Research in this area is ongoing, though, and updated informa-tion is accessible through online sources such as those in the accompanying resources list (available in the version of this article on the Today’s Dietitian website).
Multivitamin/mineral supplements often have been recommended for cancer patients following treatment as nutritional “insurance.” Data now suggest that these supplements can help achieve adequate nutrient intake in survivors whose diets are limited but don’t offer support for improving cancer outcomes or preventing mortality.6,70-72 Some observational evidence raises concerns that high levels of multivitamins may accelerate prostate cancer progression and increase fatality.72,73
The following are some supplements of particular interest for cancer survivors:
•Vitamin D seems to have antiproliferative effects that may be especially beneficial for decreasing cancer progression and enhancing survival, at least based on animal studies.72,74 Low circulating 25-hydroxy vitamin D [25(OH)D], the recommended biomarker of vitamin D status, is linked to an increased risk of several cancers.72,74 Observational studies tie higher 25(OH)D levels to improved outcomes among colorectal cancer survi-vors75 and possibly breast cancer survivors.76,77 But even when low circulating 25(OH)D is associated with worse outcomes in observational studies, it isn’t clear whether supplementation changes prognosis.72,78
It’s unclear whether the Institute of Medicine’s 25(OH)D recommendation of 600 to 800 IU daily based on bone health are adequate for bone or overall health among cancer survivors. Some researchers propose targeting serum 25(OH)D levels of at least 30 ng/mL or 40 to 80 ng/mL in the survivor population, with an intake of 1,000 to 2,000 IU of
vitamin D commonly recommended to reach those levels but still not established as optimal.72,74
Especially a concern among breast and prostate cancer survivors is the risk of osteoporosis secondary to surgical, chemotherapy, or hormonal therapies that decrease estrogen or testosterone levels, respectively, or following long-term corticosteroid use.79,80 While aiming for bone- and cancer-protective benefits, researchers emphasize that evidence is lacking regarding the safety of high blood levels of vitamin D.
•Glutamine is an essential amino acid of interest for its potential to aid mouth sores and other symptoms of mucosi-tis and to improve peripheral neuropathy that develops as a side effect of chemotherapy.74 It supports gastrointestinal cell growth and regeneration, and it may reduce the production of inflammatory cytokines. Significant side effects are uncommon with oral glutamine supplementation. More research on its use is needed, but caution is advised among patients with hepatic or renal insufficiency because, since it’s an amino acid, the liver and kidneys must metabolize glutamine. In patients with liver or renal insufficiency on protein restriction, glutamine supple-mentation should be avoided so as not to burden these organs.
Glutamine is used in clinical practice as a powder mixed into oral solution, generally “swished” before swallowing for muco-sitis benefit.
•Melatonin, a hormone secreted by the pineal gland, holds dual interest for cancer survivors. For those who have difficulty falling asleep, doses of 0.5 to 3 mg at bedtime may be help-ful.74,81 Emerging evidence suggests that melatonin may provide cancer-protective effects by upregulating antioxidant enzymes and suppressing factors that promote cancer development. Limited data show some improvement in mortality rates when used at higher doses as an accompaniment to conventional cancer therapy.74,81,82
Since melatonin can alter estrogen levels and may interact with drugs metabolized through certain pathways, those con-sidering use should consult their physicians.81
Moving Into Survivorship Living
Survivorship in the Big Picture Even after successful cancer treatment, some cancer cells
may persist and ultimately develop into a detectable cancer recurrence. Cancer survivors also face a modestly increased risk of developing a second primary cancer independent of the first, though for some cancers that risk is roughly double.1 Increased risk of second primary cancers reflects several factors, including late effects of radiation or other cancer treatments, genetic susceptibility, and lifestyle risk factors (eg, tobacco, excessive alcohol intake, obesity, inactivity).83
Although cancer survivors may worry most about cancer recurrence, for some of the most common cancers, heart disease is the predominant cause of death. This reflects shared risk factors and cardiotoxic effects of certain chemotherapies
46 today’s dietitian august 2014

and radiation cancer treatments, which may begin immediately or many years later.84,85 Most common is heart muscle damage causing heart failure, but ischemia, hypertension, arrhythmias, and other cardiac events also may occur. Cardiovascular deconditioning and weight gain, common during some cancer treatments and often not reversed later, also elevate risk.
Therefore, as cancer survivors move beyond treatment, research supports health professionals in encouraging sur-vivors to create lifestyles that help them maintain long-term health, including steps aimed to decrease the risk of recurrent or new cancers and the risk of heart disease.
Addressing Common Questions • Is soy safe for breast cancer survivors? The classifica-
tion of soy’s isoflavone compounds as phytoestrogens often raises questions about soy and breast cancer risk, espe-cially for women who had estrogen receptor–positive cancer. However, animal studies suggesting such a risk don’t accu-rately represent human metabolism of isoflavones. Multiple population studies now have concluded that among estro-gen receptor–positive breast cancer survivors (with or without tamoxifen use), there’s either no effect, a decreased recur-rence, or decreased deaths related to moderate soyfood consumption.86-91
Observational studies have reported a modestly lower risk of breast cancer in women who consume moderate amounts of soy starting early in life, and moderate consumption does appear safe for survivors.6 A moderate amount is considered to be one to two standard servings of soyfoods daily (eg, 1⁄2 cup of tofu or edamame or 1 cup of soymilk as one serving). The safety of amounts above three servings daily is unclear, and evidence isn’t available regarding the effects of isofla-vone supplements.
• Does sugar “feed” cancer? All the cells in the body use sugar for fuel, and cancer cells seem to take up blood sugar more rapidly than do healthy cells. However, dietary sugar, other carbohydrate, and gluconeogenesis from protein all produce blood sugar. Both the AICR and the ACS have concluded that the current evidence is too sparse and inconsistent to support a link between sugar intake and the risk or progression of cancer.4,6 Hyperinsulinemia may promote cancer cell growth, though.92
For cancer protection, research supports maintaining healthy blood sugar and insulin levels with weight control, regular exercise, a high-fiber diet, and avoiding large loads of refined carbohydrate. Limiting foods and beverages high in added sugar is recommended, but that’s because of their general lack of nutrients and substantial calorie load that promotes weight gain, which is linked with worse cancer outcomes.
• Is an alkaline diet cancer protective? Survivors may ask about claims that an acidic body pH promotes cancer cell growth, while an alkaline environment is protective. However, no solid research supports such claims.93,94
There’s no single measure of so-called body pH. Food choices may affect urine pH, though research isn’t consis-tent on that. Intricate body systems maintain pH within a rela-tively narrow range. The alkaline diet is plant based, so it does offer protective nutrients, phytochemicals, and fiber. However, it imposes unfounded restrictions, discouraging not only pro-cessed foods, white sugar, white flour, caffeine, and meat but also fish, poultry, and dairy products.
Optimizing Survivorship Care The Institute of Medicine identifies four essential compo-
nents of cancer survivorship care and recommends that every cancer patient receive an individualized survivorship care plan for monitoring and maintaining health.95
A growing number of cancer treatment centers and hospi-tals are establishing survivorship programs. Sometimes called cancer prehabilitation (pretreatment care) and rehabilitation programs, these may include pain management, smoking ces-sation, exercise, and nutrition components.96 Programs often offer support groups and cognitive-behavioral therapy target-ing stress management, relaxation training, and coping skills.
For a successful survivorship program, all stakeholders should participate in planning, which should be based on evi-dence-based effectiveness, program sustainability, and identi-fied outcomes for program evaluation.97
The Bottom Line Cancer survivors stand to benefit in many ways from a
healthful lifestyle. Unfortunately, for some, a cancer diagno-sis doesn’t always lead to health-protective changes.20,98,99 In a cross-sectional study of adult cancer survivors, most did meet the recommendation to avoid smoking, but only 30% to 47% met the physical activity recommendation, and about 15% to 19% met the five-a-day minimum vegetable and fruit target.98
Dietitians play a vital role in enhancing cancer survivors’ health and quality of life. Assessing survivors’ nutritional status and dietary intake can identify areas in which they’re nutritionally lacking and also areas of potential excess. Guidance can help survivors meet nutritional needs and improve outcomes relevant to cancer, cardiovascular, and bone health. Survivors have wide-ranging needs for help in evaluating information from many sources and making evidence-based behavior changes that support recovery and long-term health, and dietitians can assist them in addressing these needs.
— Karen Collins, MS, RDN, CDN, FAND, is a speaker, writer, and consultant who serves as the nutrition advisor for
the American Institute for Cancer Research.
For references, resources, and a patient handout view this article on our website at www.TodaysDietitian.com.
august 2014 www.todaysdietitian.com 47

CPE Monthly Examination1. Approximately what percentage of Americans diagnosed with cancer currently live more than five years?a. 25b. 45c. 65d. 85
2. Based on recommendations from the American Institute for Cancer Research (AICR) and the American Cancer Society (ACS) regarding physi-cal activity, cancer survivors should do which of the following? a. Talk with their physicians or a fitness professional trained to work with cancer survivors about how to safely incorporate strength training to restore or minimize the loss of lean body mass.b. Attempt to return to the level of exercise in which they engaged before their cancer diagnosis, since cancer treatment doesn’t affect the choice of physical activity upon completion.c. Engage in gentle exercise such as walking, but avoid strength training because of cardiac and lymphedema risks.d. Engage in physical activity every day or nearly every day, though it will likely improve only sleep patterns and quality of life.
3. What does current research say about overweight and obesity in cancer survivors? a. Among cancer survivors today, overweight and obesity are more common than underweight.b. Most people who were obese when diagnosed with cancer are normal weight or underweight by the time they complete treatment.c. Prediagnosis obesity is associated with a greater risk of cancer but is unrelated to cancer outcomes.d. Research hasn’t identified any mechanisms connecting obesity with cancer outcomes, so any link seen likely is due to a mutual association with lifestyle habits.
4. Which of the following statements best describes the issue of lean body mass loss for cancer survivors? a. Loss of lean body mass occurs as a later stage of excess weight loss.b. Loss of lean body mass primarily is seen in association with mouth, esophageal, and lung cancers.c. Loss of lean body mass frequently is seen in survivors of colon, breast, and childhood cancers.d. Androgen deprivation therapy generally protects against the loss of lean body mass often seen in prostate cancer.
5. What advice for overweight or obese cancer survivors is best sup-ported by overall current research? a. Aim for modest weight loss through changes in eating and physical activity after confirming with your health care provider that you have no medical contraindications, including low lean body mass.b. Since cancer survivors have an increased risk of developing a second cancer and heart disease, both of which increase with obesity, shed excess weight as soon as possible.c. Especially if there’s excess weight around the abdomen, aim for at least a 10% weight loss by reducing calorie intake, but don’t chance the cardio-vascular risk of increased physical activity.d. Avoid weight gain, but don’t attempt to lose weight because mortality data suggest doing so poses significant risk.
6. Evidence-based dietary recommendations suggest that cancer survi-vors should do which of the following? a. Focus on plant foods providing nutrients and compounds that can influence DNA repair, inflammation, cell proliferation, and cancer progression.b. Aim for no more than 20% of calories from fat.c. Include red meat at least once per day to provide bioavailable iron that can thwart survivors’ tendency to develop anemia.d. Exclude refined grains and all forms of sugar from their diet so as not to promote the growth of any remaining micrometastases.
7. Which of these statements about cancer survivors’ soyfood consump-tion is best supported by current research? a. Women who start consuming soyfoods after a breast cancer diagnosis can reduce the risk of recurrence.b. Consuming one or two standard servings of soyfoods daily appears safe for cancer survivors.c. Daily soyfood consumption is safe for most cancer survivors, but those who had estrogen receptor–positive breast cancers should avoid it.d. Soyfoods contain phytoestrogens called isoflavones that increase the risk of breast, uterine, and prostate cancers.
8. Which of the following statements about vitamin D and cancer survi-vors is best supported by current evidence? a. Laboratory studies show that vitamin D may play a role in slowing down the early stages of cancer development, but it’s unlikely to affect pro-gression or survival.b. Observational studies have linked higher vitamin D status with better outcomes in colorectal cancer survivors and possibly breast cancer survivors.c. Current evidence shows a straight-line relationship in which the higher cancer survivors’ blood levels of vitamin D, the lower their risk of mortality.d. Because of an increased need for vitamin D among cancer survivors, an intake of 5,000 IU/day now is recommended for survivors unless there are medical contraindications.
9. When working with cancer survivors who suffer from cancer-related fatigue, RDs should do which of the following?a. Encourage them to rest more and cut back on activities.b. Suggest saving the majority of their calorie intake for evenings, when there’s more time and energy to prepare a balanced meal.c. Help them plan mini meals that provide high-fiber carbohydrate, pro-tein, and healthful fat yet require minimal energy for preparation.d. Suggest they consult a psychologist or mental health counselor since the fatigue likely reflects depression.
10. Which of the following best meets published recommendations for cancer survivorship programs?a. Activities begin either as soon as treatment ends or in later months when a survivor feels ready.b. Each survivor is plugged into one of a few generic survivorship care templates that meet the needs of most survivors.c. Programs focus mostly on decreasing risk of cancer recurrence, since for most survivors that poses the greatest threat to quality of life and mortality.d. Dietitians play a vital role in helping survivors improve outcomes related to cancer, cardiovascular, and bone health.
For more information, call our continuing education division toll-free at 877-925-CELL (2355) M-F 9 am to 5 pm ET or e-mail [email protected].
Register or log in on CE.TodaysDietitian.com to purchase access to complete the online exam and earn your credit certificate for 2 CPEUs on our CE Learning Library.
48 today’s dietitian august 2014

PERSONAL COMPUTING
FACEBOOK, WHERE TO?By Reid Goldsborough
Facebook, the world’s largest social networking site, recently celebrated its 10th anniversary, which calls for a look backward and forward.
Founded in 2004 by Mark Zuckerberg and four of his Har-vard University classmates, Facebook initially was limited to Harvard students before first expanding to other colleges in the Boston area then other Ivy League colleges followed by other colleges, high schools, and anyone in the world who claims to be at least 13 years old.
Today, Facebook contends it has more than 1 billion active users, about one-seventh of the world’s population, though this number likely is exaggerated. Still, Facebook’s reach is undeniable, as Zuckerberg’s goal is to “connect the world.” Part of his recently announced 10-year plan is helping users “answer interesting questions or solve problems.”
People use Facebook to keep up with news about friends and family, write public and private messages, post photographs and videos, find people from their past, and join common-interest groups organized by workplace, school, hobby, or other characteristics.
Myspace (at the time stylized as MySpace) was the first widely popular social networking site, launched in 2003 just six months before Facebook. It took Facebook until 2008 to over-take Myspace in popularity.
Over the years, Facebook has received its share of criticism—and it still does. It changes its interface too often for many users, forcing them to learn new ways to use it. It has a loosey-goosey approach to privacy, collecting data on users and
bombarding them with ads. Despite the criticism, Facebook’s advertising revenue has grown exponentially.
But if you’re not careful, as with several other online activities, you can get scammed or otherwise harmed through Facebook. One scam involves Facebook’s Like option, its thumbs-up button. Likes can generate ad revenue for the business or individual behind the particular Facebook page. Any attempt to sell users Likes is a scam, and Facebook’s policies prohibit this practice. According to Facebook’s help system, “Certain websites promise to provide large numbers of likes for your Page if you sign up and give them money. These websites typically use deceptive practices or are scams.”
Another scam involves a “You gotta see this!” or simi-lar message. When you click on it, you’re asked through a pop-up window to download a media player. Only the down-load is malware that steals your data, identity, or money. The Facebook section of Hoax-Slayer (www.hoax-slayer.com/facebook-related.html) has more detailed information about Facebook-related scams and hoaxes.
Facebook isn’t the only current social networking site, though. The most prominent competing services include Twitter, Google+, and LinkedIn.
Twitter specializes in letting you send and read “tweets,” which are text messages of up to 140 characters. You can update your followers with news ranging from your recent job promotion or upcoming marriage to your thoughts about the movie you just saw or what you had for dinner.
Google+ attempts to leverage Google’s other services, from search and online storage to e-mail and cloud software. LinkedIn is targeted for professional networking, helping companies and business people make new contacts and keep in touch with previous coworkers, affiliates, and clients.
The social media world is constantly in flux. In February, Twitter began testing an experimental interface with a select group of users that’s a cross between Facebook and Google+.
Today, Facebook is arguably the second most prominent online presence, behind Google’s search engine. In the ever-changing online world, it’s an open question whether this will remain the case.
— Reid Goldsborough is a syndicated columnist and author of the book Straight Talk About the Information Superhighway. He can
be reached at [email protected] or reidgold.com.
august 2014 www.todaysdietitian.com 49

FOCUS ON FITNESS
‘WEIRD’ WORKOUTSFun Activities Way Beyond the ConventionalBy Jennifer Van Pelt, MA
Over the course of my 25 years teaching fitness classes and writing about fitness, I’ve seen many fitness fads come and go. Within the last few years, I’ve noticed a new overall fad: the increasing number of “weird” workouts.
We all have different perceptions of what weird is, and what may be weird for some may be normal for others. For example, many exercisers think workouts performed at 4:30 am are weird because they prefer exercising at a different time. Exercise previously considered weird may evolve into a “normal” and popular activity. For instance, in the 1970s, only “hippies” did yoga, but now millions of Americans practice different styles of yoga every day.
The workouts discussed here recently have been deemed weird by major fitness organizations, popular health magazines and websites, and/or social media. Most are available only in urban areas with large gyms or at specialized facilities, such as health resorts, sports training centers, and boutique fitness studios. For each weird workout, I’ve provided a brief description, the potential benefits or disadvantages, and the types of clients who may find it appealing. I’ve also commented on whether a
particular weird workout may evolve into a popular and widespread fitness activity in the future, such as yoga did.
Indulge Your Inner Child •Hula hooping: This workout uses a standard or weighted
hula hoop to perform various movements designed to tone the hips, thighs, and abdominal muscles. Hoopnotica, a branded hula hoop workout, recently has emerged, offering instructor certifications and DVDs. According to WebMD, hula hooping can burn as many calories as a step aerobics or boot camp class and is a viable workout option.1
Benefits: Calorie burning and toning in a fun workout. Downside: The workout could become frustrating, and the
movements may not be suitable for those with hip or knee joint issues or low back pain.
Hula hooping may appeal to clients who want to exercise with their children or who are looking for a fun alternative to core conditioning classes.
•Circus workouts: Offered at large gyms and special circus training centers, these workouts involve learning about and using the trapeze and acrobatic equipment used by circus performers. Trapeze workouts are available on high trapezes with a safety net or very low stationary trapezes in a room.
Inspired by Cirque de Soleil, companies specializing in circus fitness for adults and children have emerged, primarily in major cities such as New York, Philadelphia, and Atlanta. In fact, Reebok and Cirque de Soleil recently partnered to create Jukari Fit to Fly, a trapeze class that uses a special bar that can be affixed to a gym’s fitness classroom ceiling. Some yoga studios now are offering aerial or “floating” yoga. Yoga poses are performed in silk hammocks suspended from the ceiling. The silks resemble those used by many acrobatic circus performers.
Benefits: Strength and flexibility. Downside: Expensive and limited access. Trapeze workouts will appeal to clients who want a challenge
and anyone who ever dreamed of joining the circus when they were younger. Aerial yoga may interest those looking for a new yoga challenge.
•Trampolining: Small trampolines known as rebounders or mini-trampolines hit the market in the late 1970s and 1980s. Occasionally, fitness infomercials for rebounders still can be seen on TV and online. I have one of my own, and I find that the bouncy surface is easy on the joints. Rebounding has been pro-posed as beneficial for the immune system because it’s sup-posed to help with lymphatic drainage.2 No studies have been published on this proposed benefit, but two recent studies reported significant benefits for stroke rehabilitation and fall prevention for the elderly.3,4
Due to the popularity of larger trampolines for home yards, trampoline fitness centers recently have been built in some areas. Fitness classes for adults, children, and families are offered.
Benefits: Cardiovascular and toning without the impact of exercise on hard surfaces.
50 today’s dietitian august 2014

Downside: Larger trampolines have the potential for spinal injuries due to improper landing.
Clients looking for a fun home exercise alternative that’s easier on the joints than a treadmill should investigate the inex-pensive mini-trampoline. DVDs are available for home workout guidance. Families looking for a fun exercise alternative should check out local trampoline fitness centers, but they should make sure that all bouncing is supervised.
Release Your Inner Rock Star•Karaoke cycling: Add a microphone and karaoke machine
to an indoor cycling room and let the party begin. Crunch Fit-ness gyms offer this workout that mixes traditional faster cycling music with slower karaoke song favorites. Participants can opt whether to sing while cycling.
Benefits: Cardio benefits of cycling combined with some fun. Being able to sing karaoke does allow participants to judge their level of exertion; they will know they’ve recovered from the hard cycling interval that left them gasping for air.
Downside: How many individuals are comfortable singing in front of others? And, in my experience, cycling classes are well attended because of the variety of music. Do they really want to hear the person next to them, who may or may not have any vocal talent, singing a Maroon 5 song when they can hear the original in a standard cycling class?
• Punk rock aerobics: Originating in Boston about 15 years ago, punk rock aerobics classes were held during the day in rock clubs, often with guest DJs supplying punk rock classics from groups such as the Ramones. These classes appeal to anyone who dislikes the conventional gym setting. According to major news magazines such as Rolling Stone and Newsweek, the punk rock workout attracts “anarchists” under age 30 and older “rockers” looking to get in shape and enjoy wearing what-ever they want. According to its website, Punk Rock Aerobics is about empowerment, stating, “We aim to inspire, empower, and have a good time.” The company now offers rock camps for young girls with the intention of building self-esteem and improving fitness.
Benefits: Cardiovascular and strength conditioning to music that rocks.
Downside: The music won’t appeal to everyone, and access currently is limited to areas where the company offers classes.
Clients of any age who like punk rock music and prefer to wear knee socks and funky shorts, rather than designer yoga pants, may find this workout appealing.
•Drumming workout: Drumming-based workouts use drumsticks and upper body movements combined with other aerobic movements to provide a cardiovascular workout that focuses on upper body strength. In some classes, regular drumsticks are used to drum on stability exercise balls.
A new branded workout called POUND uses proprietary RipStix (lightly weighted drumsticks) and combinations of cardio, Pilates, isometrics, and plyometrics in a 45-minute
class set to rock, rap, dubstep, and other music styles with strong beats. Classes are offered at gyms listed on the web-site (www.poundfit.com/the-workout), and a DVD for home exercise also is available.
Benefits: Cardiovascular, core, and upper body conditioning to fun music.
Downside: Drumsticks or RipStix must be purchased for home use. Weighted drumsticks may aggravate shoulder joints.
Clients who want an alternative full-body workout set to music will like this workout.
Adding Variety and FunThe list of weird workouts is too long to include all of them
here. Some that I haven’t summarized but recommend avoiding due to safety issues include the stiletto workout (working out in high heels) and treadmill dancing, both of which have a high risk of injury due to falling.
Of those I have summarized, I believe trampoline workouts have the greatest potential for growth and longevity. Even though numerous injuries associated with trampolining have been reported, these have occurred mostly in children left unsupervised on home backyard equipment. The introduc-tion of trampoline sport centers offering supervised classes or bouncing time will minimize the risk of injury. Trampolin-ing became an Olympic sport in 2000, which has helped fuel interest as well. Mini-trampolines are an inexpensive alter-native to expensive home exercise equipment, and they carry little risk of injury.
If you have clients who are bored with conventional fitness activities, suggest they investigate a safe weird workout to add variety and fun to their exercise program.
— Jennifer Van Pelt, MA, is a certified group fitness instructor and health care research analyst/consultant
in the Reading, Pennsylvania, area.
References1. Goodman B. Hula hoop workouts burn calories.
WebMD website. http://www.webmd.com/fitness-exercise/news/20110210/hula-hoop-workouts-burn-calories. February 11, 2011.
2. Scrivens D. Rebounding: good for the lymph system. WellBeing Journal website. http://www.wellbeingjournal.com/rebounding-good-for-the-lymph-system.
3. Miklitsch C, Krewer C, Freivogel S, Steube D. Effects of a predefined mini-trampoline training programme on balance, mobility and activities of daily living after stroke: a randomized controlled pilot study. Clin Rehabil. 2013;27(10):939-947.
4. Aragão FA, Karamanidis K, Vaz MA, Arampatzis A. Mini-trampoline exercise related to mechanisms of dynamic stability improves the ability to regain balance in elderly. J Electromyogr Kinesiol. 2011;21(3):512-518.
august 2014 www.todaysdietitian.com 51

GET TO KNOW…�
JOANNE SLAVINConducting Research and Inspiring the Next Generation of Nutrition PioneersBy Juliann Schaeffer
As a professor at the University of Minnesota and a leading nutrition researcher for the past three decades, Joanne Slavin, PhD, RD, has published more than 200 scientific articles, helped 55 graduate students discern their own food and nutri-tion path, and likely inspired countless others who happened upon her lecture classes in one way or another.
Writing hundreds of scientific articles doesn’t happen without being involved in several research studies. Whether it’s assist-ing in a student research project on what causes heart disease or directing her own study on how various types of fiber affect the body, Slavin knows her way around a research lab (and fecal samples, as you’ll see later), though she didn’t get to this place without years of honing her nutrition knowledge base first.
Growing up on a Wisconsin dairy farm, Slavin says 4-H was an important aspect of life in her community, and she showed an affinity for food and nutrition, especially baking, pretty early. “But I was actually more interested in sports and wanted to be a gym teacher,” she says. That changed when she gave a speech about calories in college, and soon after she switched her edu-cation focus to nutrition. She didn’t know it then, but she’d spend the next decade as a student—and calories were just the tip of what she’d learn.
At the University of Wisconsin-Madison, Slavin earned not just a bachelor of science degree but then an RD credential followed by a master’s degree and doctorate, all with a focus in nutritional sciences. After all that time spent in a class-room, one may think Slavin would grow tired of that environ-ment but not so, she says. Though various speaking and other
engagements take her away for a time, to this day her home base continues to be a college classroom.
What led her to pursue this path? According to Slavin, she had way too much fun learning to ever contemplate leaving the university life. “Living in Madison and hanging out with other graduate students was much more fun than working for a living, so it was an easy choice to continue in graduate school,” she says. “I decided that university professors had about the best job I had ever heard about, so I wanted to be able to work at a university.”
Though her doctorate may have afforded her some great professional opportunities, she says it’s her RD credential that has proved the most valuable. “I always used my RD skills,” she says, whether in making wedding cakes, working in foodser-vice, or giving talks on sports nutrition. “I always tell my stu-dents that I would give up my PhD before my RD, since my RD has helped me pay the rent my entire working life.” Today’s Dietitian (TD): What do you enjoy most about your job?Slavin: Working with students. Food and nutrition is an amaz-ing field with so many routes to a successful life. Some of my best students ever have decided to be full-time parents, a place where their amazing skills can have a huge impact. TD: You worked on the Dietary Guidelines Advisory Committee (DGAC). What input did you have in crafting the 2010 version of the guidelines, and how did those guidelines come to be?Slavin: I was honored to be a member of the 2010 DGAC. The DGAC is the scientific support for the guidelines. I chaired the carbohydrate and protein committees and also worked on the energy balance and nutrient adequacy subcommittees. After the scientific report is issued, the government writes the Dietary Guidelines for Americans. The DGAC doesn’t see the guidelines before they’re released to the public, so if you have any complaints about the Dietary Guidelines for Americans, please send them up the government channels.
TD: In what ways do you think the 2010 Dietary Guidelines improved on the previous version?Slavin: I’m particularly proud that protein was added to the guidelines. The role of whole foods such as vegetables, whole grains, fruits, and dairy products also was a strength of the Dietary Guidelines for Americans.
TD: Were there any downsides about the process or any 2010 guidelines you wish you could modify or change completely?Slavin: Because of such a broad scope, it’s difficult to cover all the topics of interest to Americans. Usual topics such as fat, sugar, and salt never go away, but new topics emerge (eg, gluten, prebiotics, GMOs). It’s hard to cover all these issues with an evidence-based approach.
52 today’s dietitian august 2014

TD: How have your personal experiences changed or molded your outlook on life and on eating?Slavin: I’ve traveled a lot and seen that other cultures take more care in eating and appreciate the importance of eating in life. I worked in Switzerland, and every day it was required that you check out for one hour for lunch. The lunch was shared with your coworkers, and great conversations were part of those lunches. [Here in the United States,] we’ve lost the connection with food and family that I had as a child grow-ing up on the farm.
TD: If you could offer clients only one piece of advice, what would it be?Slavin: Make peace with your diet; don’t obsess about grams of added sugar or solid fat. It’s counterproductive to health.
TD: What has been the most exciting or significant finding you’ve uncovered in your research thus far in your career?Slavin: That all fibers are different. Choose psyllium or wheat bran if you want a larger stool, and go with oat bran or guar gum if you want to lower serum lipids.
TD: What’s the most exciting research that you’re working on right now, either one that has come out recently or is still ongoing?Slavin: Like everyone else on the planet, we’re interested in changes in microbiota with different diets, except unlike every-one else on the planet, we were interested in this area long before it became cool.
TD: Do you have any favorite stories from your research studies that have stuck with you?Slavin: Since we collect fecal samples for a living, most of my favorite stories would be in the potty humor area, including cases of stolen fecal samples.
TD: What has been the biggest professional obstacle you’ve faced, and how did you overcome it?Slavin: I didn’t get a dietetic internship. I later found out that my advisor never got around to sending off any of the letters I needed. So I did a traineeship after earning my MS to get the experiences needed to sit for the RD exam. It’s quite likely that if I had gotten an internship, I would be working as a dietitian in southern Wisconsin and would never have gone to graduate school and become a professor.
TD: What foods do you crave?Slavin: Bacon, ice cream, and fresh baked bread with butter.
TD: What’s one food with an unhealthful stigma that’s actually pretty good for people?
Slavin: Potatoes: They’re high in vitamin C, potassium, fiber, and high-quality protein.
TD: Conversely, what’s one food that gets a good rap but shouldn’t?Slavin: Fruit: It generally only contains carbohydrate and not that much fiber. Many consumers don’t understand that fruit contains no protein.
TD: What’s the biggest step people can take today to decrease their risk of diet-related disease in the future? Slavin: Enjoy life and understand that fat doesn’t cause heart disease. Dietary patterns are linked to disease outcomes, but eating dinner as a family and enjoying food are more important than obsessing about every gram of fat or milligram of sodium. Consumers feel cheated when they develop colon cancer, for example, even when they have been on a high-fiber diet their entire lives.
Physical activity is likely more important than diet in the prevention of diseases such as heart disease, cancer, and diabetes. But routine physical activity—walking the dog, gardening, and playing softball with friends—is the type of physical activity we need everyone to enjoy; there’s no need to run marathons or join expensive gyms.
TD: What food or exercise items are on your bucket list?Slavin: My bucket list is all checked off. I never let an opportu-nity pass me by, a lesson I learned from my mom.
TD: What’s something most people may be surprised to learn about you?Slavin: I play a mean accordion, so call me if you need some polka background music at your next event.
— Juliann Schaeffer is a freelance writer and editor based in Alburtis, Pennsylvania, and a regular contributor to Today’s Dietitian.
Physical activity is likely more important than diet in the prevention of diseases such as heart disease, cancer, and diabetes. But routine physical activity is the type of physical activity we need everyone to enjoy; there’s no need to run marathons or join expensive gyms.
august 2014 www.todaysdietitian.com 53

Diabetes Resource Guide2014
Cabot, maker of the world’s best cheddar, including all-natural, light cheddar cheese, offers support for your nutrition education
programs. Visit our online Health Professional Resource Center to fi nd
out more about our sampling programs, coupons, recipes, and more.
Cabot Creamery CooperativeE-mail: [email protected]
www.cabotcheese.coop/healthprofessionals
Cascade Ice is a zero-calorie, sparkling fl avored water that is free of sodium, gluten
and sugar. Cascade Ice waters have a delightful fi zz combined with natural juices
and are available in over 21 delicious fl avors! Visit CascadeIceWater.com to check out
retailer availability.
Cascade IceP.O. Box 2246, Everett, WA 98213-0246
Phone: (425) 267-0959Fax: (425) 353-5600
E-mail: [email protected]
Daisy Low Fat Cottage Cheese has 13 grams of satisfying protein and
4 grams of carbs per 90 calorie ½ cup serving. Plus, it’s made with only 4 ingredients
and no additives or preservatives.
Visit DaisyBrandHealth.com for product information, patient education materials, healthy recipes and pairings!
Daisy Low Fat Cottage Cheese has Daisy Low Fat Cottage Cheese has
Diabetes Sentry is an FDA approved, non-invasive, wearable medical device designed to prevent the catastrophic consequences of nocturnal hypoglycemia by monitoring changes in external body chemistry—skin temperature changes and/or changes in levels of perspiration.
Diabetes Sentry952-221-0506
* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure or prevent any disease.
www.EssentialFormulas.com
• Contains both LIVE probiotics and their prebiotic food supply.• Allows the cultivation of an individual’s unique personalized fl ora• Supports superior digestion and optimal whole health.*
Discover the Dr. Ohhira Difference!™
JOIN THE CHIA REVOLUTION
• More Omega-3 than fi sh or fl ax oil!• Plant derived Omega-3• Sustainable and non-GMO
* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure or prevent any disease.
www.EssentialFormulas.com
™
Diabetic-Friendly Skinny Shirataki Noodles are made from the root of the Konnyaku plant. • Low Carb
• Low Calorie
• Gluten Free
• Good Source of Dietary Fiber (3-4g per serving)
• All Natural and Vegan
• Made in the USA
Just rinse, drain and heat pre-cooked Skinny Noodles.
A diabetic-friendly alternative for all your favorite pasta dishes.
AVAILABLE ONLINE:www.getskinnynoodles.com
LC Foods Company is dedicated to providing quality, blood sugar stable foods for diabetics and health conscious people.
Our products are low in carbohydrates and free of sugar, artifi cial sweeteners,
soy and GMOs. Visit our online store today at www.HoldtheCarbs.com.
Contact UsPhone: 919-510-6688
E-mail: [email protected]
54 today’s dietitian august 2014

Potassium Supplements May Increase Survival in Patients Taking Diuretics
Researchers from the Perelman School of Medicine at the University of Pennsylvania found that patients taking prescription potassium supplements together with loop diuretics for heart failure have better survival rates than patients taking diuretics without potassium. Moreover, the degree of benefit increases with higher diuretic doses. The team, including senior author Sean Hennessy, PharmD, PhD, an associate professor of epidemiology in Penn’s Center for Clinical Epidemiology and Biostatistics, reported its findings in a study published online in PLOS ONE.
Loop diuretics, which are one type of diuretic or water pill named after the part of the kidney acted on, are commonly used in the treatment of heart failure (and associated lower-limb edema or swelling) to help push out extra fluid that can accumulate when the heart isn’t working properly. However, they also flush out needed potassium, causing many physicians to prescribe potassium supplements. But its survival benefit has never been studied, and because of this lack of evidence, there’s controversy about whether potassium should be prescribed to all patients receiving loop diuretics.
In a retrospective study, the researchers examined existing health care data from Medicaid between 1999 and 2007 to study approximately 180,000 new starters of loop diuretics who were prescribed supplemental potassium and an equal number of people who started a loop diuretic without the potassium supplement. The researchers found that in patients receiving at least 40 mg/day of furosemide (one form of loop diuretic), adding supplemental potassium appeared to reduce mortality by 16%, a large and statistically significant reduction.
“Our findings provide evidence that adding potassium supplementation may increase survival rates among patients taking loop diuretics,” says the study’s lead author, Charles E. Leonard, PharmD, MSCE, a senior research investigator in the Center for Clinical Epidemiology and Biostatistics and the senior manager of the Ambulatory Drug Use & Effects Program at Penn. “Nonetheless, because this is the first such study of this question, we hope that others confirm these results in independent studies.”
The researchers also found that in patients receiving less than 40 mg/day of furosemide, potassium appeared to reduce the mortality rate by 7%, a suggestive but statistically nonsignificant finding. (The overall mortality rate was about 9% per year in the population under examination.)
The use of potassium supplementation under investigation was preventive as opposed to being prescribed to patients who already had measured reductions in potassium. Only patients receiving supplemental potassium in solid (not liquid) form were studied, the latter possibly indicating an inability to swallow and therefore a marker for a possibly complicating corollary medical impairment.
These results appear to support the common practice of using potas-sium together with loop diuretics. Today, nearly 5.8 million Americans suffer from heart failure.
“Using potassium supplementation for patients receiving loop diuretic therapy may be a relatively inexpensive way to save lives,” Hennessy says. “In today’s climate of seeking cost-effective measures to keep patients healthy, this is a therapy that certainly merits additional consideration.”— SOURCE: PERELMAN SCHOOL OF MEDICINE AT THE UNIVERSITY OF PENNSYLVANIA
NEWS BITES
We offer relief, recovery and support to anyone
who wants to stop eating compulsively.
®
Compulsive Client?
no fees • oa.org
Since 1979, UP4 Probiotics by UAS LifeSciences has delivered the highest
quality, science-backed probiotics to the natural marketplace. Strictly dedicated to probiotics, UP4 iscommitted to designing
innovative and effective formulations based on L. acidophilus DDS®-1, a strain
that has been researched and tested rigorously for decades.
WWW.UP4PROBIOTICS.COM
UP4 PROBIOTICS™
No Calories, Sugar, Carbs, Fat or Gluten. Walden Farms makes more than 60 Calorie Free
Specialties. Chocolate Dip, Caramel Dip, Marshmallow Dip, Chocolate Syrup, Pancake Syrup, Caramel
Syrup, Fruit Syrups, Peanut Spread, Jam & Jelly Fruit Spreads, Salad Dressings, BBQ Sauces, Miracle Mayo, Flavored Mayos, Ketchup, Seafood Sauce,
Pasta Sauces, Veggie & Chip Dips.
1209 W St. Georges Avenue • Linden, NJ 07036Phone: 1.800.229.1706 • E-mail: [email protected]
www.waldenfarms.com
august 2014 www.todaysdietitian.com 55

NEWS BITES
Quality, More Than Quantity, Matters in Exercise, Diet
If the goal is losing weight and maintaining optimal health and fitness, the quality of the exercise and diet regimen mat-ters more than the quantity, says Paul Arciero, DPE, a pro-fessor in the health and exercise sciences department at Skidmore College in Saratoga Springs, New York.
In a paper published by The Journal of Applied Physiology, Arciero and several colleagues reported the clear benefits of a multidimensional exercise regimen that includes resistance exercise, interval sprint exercise, stretching (including yoga or pilates), and endurance exercise. If people add moderate amounts of protein regularly throughout the day, they’ll be on their way to decreasing total and abdominal fat, increasing lean body mass, and achieving optimal levels for blood pressure, blood glucose, and insulin.
A member of the advisory board of the American Heart Association and a fellow of both the American College of Sports Medicine and the Obesity Society, Arciero is familiar with the exercise and diet recommendations issued by these and other governing health organizations. “They’re well intended, but they’re complex, and they’re not being com-municated in a way that’s easy for the public to understand
and incorporate in their daily life-style,” he says. “I wanted to test an exercise protocol with a nutritional component that’s simple and under-standable for people.”
To conduct the study, Arciero enlisted 36 female and 21 male volunteers between the ages of 35 and 57 who could be described as out of shape. They exercised fewer than 60 minutes per week, had done no resistance training within the last 10 years, and could be described as obese or overweight, with an average BMI of 28.6 and average body fat percentage of 36.6.
Dividing his subjects randomly into three groups, Arciero conducted a 16-week trial in which all subjects consumed the same amount of whey protein (60 g/day) but exercised dif-ferently. One group was sedentary, another performed intense resistance training four times per week, and the third followed a multidimensional regimen that included resistance exercise, interval sprint exercise, stretching led by a yoga instructor, and endurance exercise.
When the trial ended, Arciero found that those who had followed the multidimensional regimen showed the greatest health improvements, including the greatest reductions in body weight, total and abdominal fat mass, waist circumfer-ence, and blood glucose. In addition, this group experienced the greatest increase in percentage of lean body mass.
Interestingly, all groups showed improvements, even those who maintained a sedentary lifestyle during the period and simply ate the assigned daily regimen of 60 g of whey protein. That finding supports an earlier study by Arciero’s team that found increasing the amount of protein in the diet to as much as 35% may decrease total and abdominal fat.
Overall, the study supports a rethinking of current assumptions about exercise, which Arciero believes place too much focus on the quantity of exercise people do rather than the quality of that exercise. “It’s very difficult to just lift weights or only do the treadmill or the elliptical machine and be healthy,” he says. “Your exercise regimen needs to encompass as much of what makes you a fully integrated living person as possible.
“It’s not about simply doing more exercise,” he continues. “It’s about doing the appropriate range of exercises and activities that most effectively promote health and fitness.”— SOURCE: SKIDMORE COLLEGE
56 today’s dietitian august 2014

Poor Health, Lifestyle Factors Linked to Memory ComplaintsIf you’re depressed, don’t get enough exercise, or have
high blood pressure, you may find yourself complaining more about memory problems, even if you’re a young adult, according to a new UCLA study.
UCLA researchers and the Gallup organization polled more than 18,000 people about their memory and a vari-ety of lifestyle and health factors previously shown to increase the risk of Alzheimer’s disease and dementia. They found that many of these risk factors increased the likelihood of self-perceived memory complaints across all adult age groups. The findings, published in PLOS ONE, may help scientists better identify how early lifestyle and health choices impact memory later in life. Examin-ing these potential relation-ships, researchers say, also could help to pinpoint inter-ventions aimed at lowering the risk of memory issues.
The 18,552 individuals polled ranged in age from 18 to 99. The known risk factors the researchers focused on included depression, lower education levels, physical inactivity, high blood pressure, diabetes, obesity, and smoking. They were surprised by the prevalence of memory issues among younger adults, says the study’s senior author Gary Small, MD, UCLA’s Parlow–Solomon Professor on Aging and director of the UCLA Longevity Center. “In this study, for the first time, we determined these risk factors may also be indicative of early memory complaints, which are often precursors to more significant memory decline later in life,” says Small, who also is a professor of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience and Human Behavior at UCLA.
Depression, low levels of education, physical inactiv-ity, and high blood pressure increased the likelihood of memory complaints in younger adults (ages 18 to 39), mid-dle-aged adults (40 to 59), and older adults (60 to 99), the researchers found. Depression was the strongest single risk factor for memory complaints in all age groups.
Having just one risk factor significantly increased the frequency of memory complaints, regardless of age, according to researchers. Memory complaints rose when
the number of risk factors increased.Overall, 20% of those polled had memory complaints,
including 14% of younger adults, 22% of middle-aged adults, and 26% of older adults.
The researchers noted that, in general, memory issues in younger people may be different from those that plague older individuals. For younger adults, stress may play more of a role, and the ubiquity of technology, including the Internet and wireless devices, which often can result in constant multitasking, may impact their attention span, making it harder to focus and remember.
Small notes that previous studies have shown that edu-cation is a key element of cog-nitive reserve, the ability to compensate for progressive brain pathology. These results suggest that pursuing educa-tional activities at any stage of life may be helpful.
“We hope that our findings will raise awareness among researchers, health care providers, and the general public about the importance of lowering these risk factors at any age, such as getting screened and treated for depression and high blood pressure, exercising more,
and furthering one’s education,” says Stephen Chen, MD, an associate clinical professor of psychiatry and biobehavioral sciences at the Semel Institute and the first author of the study.
“We’re planning to use these results as a basis for future studies to better understand how reducing these risk factors may possibly lower the frequency of memory complaints,” says author Fernando Torres-Gil, PhD, a professor at UCLA’s Luskin School of Public Affairs and the associate director of UCLA’s Longevity Center.
The Gallup poll used in the study took place between December 2011 and January 2012 and was part of the Gallup–Healthways Well-Being Index, which includes health- and lifestyle-related polling questions. Pollsters conducted landline and cell phone interviews that cap-tured a representative 90% of the US population, accord-ing to the researchers.— SOURCE: UCLA HEALTH SCIENCES
august 2014 www.todaysdietitian.com 57

Eat What You Love — EverydayBy Marlene Koch2014, Running PressHardcover, 352 pages, $26.50
With 200 new recipes, Marlene Koch offers plenty of delicious options, all modified with healthful eating in mind.
The first section of the book contains healthful eating tips, an explanation of ingredients used in her recipes (I love that she used everyday ingredients for the everyday cook), meal planning suggestions, and general information for diabetes patients on how to use her book.
Koch’s concept of “eat what you love” is right on target. As dietitians, we know that sustaining healthful eating habits requires good-tasting food. Koch’s recipes make that task easy, and she often does “dare to compare” so consumers can compare the nutrition facts of a familiar dish with her modification.
The book’s food photography is exquisite, which likely will motivate readers to try her recipes. I decided to try the Oven Fried Mozzarella Sticks With Marinara Sauce. This recipe caught my interest because the item is frequently ordered in restaurants or purchased from the freezer section of the grocery store, but restaurant or store-bought fried cheese sticks are loaded with fat, carbohydrates, and calories. Koch’s recipe contained only 3 g of carbohydrates, 4.5 g of fat, and 80 kcal for two pieces. The recipe turned out perfectly and was a delicious comfort food. My only recommendation is to swap out the garlic salt for garlic powder to help lower the sodium level. People with diabetes, for example, need to limit their sodium intake, and I thought this swap made sense with the cheese being a higher-sodium food to start.
Throughout the book, there are strategies on cooking or nutrition information worth mentioning, which are located in the “Marlene Says” section. Kudos to Koch for adding carbohydrate choice as part of the nutrition information for
each recipe, one of the many ways she speaks directly to diabetes patients in this book.
One of the last sections of the book, “Menus for Every Day, Every Occasion, and Everyone,” is helpful for the average consumer. This section offers a little extra help to put together delicious, nutritious menus and provides different menu options by combining delectable recipes from the book.
I have a confession to make. As someone who manages type 1 diabetes, I was captivated some time ago by Koch’s 90 Calorie Chocolate Cupcakes from a previous book. Now I’m staring at the photo of her Molten Chocolate Lava Cakes, weighing in at only 21 g of carbohydrates. I love this book and Koch’s recipes, but in fairness, I must acknowledge that I may be under the influence of chocolate.
— Toby Smithson, MSNW, RDN, LDN, CDE, is a spokesperson for the Academy of Nutrition and Dietetics and the author of
Diabetes Meal Planning and Nutrition for Dummies.
Fresh From the Farm: A Year of Recipes and StoriesBy Susie Middleton2014, Taunton PressHardcover, 256 pages, $28
Author Susie Middleton’s fantasy became reality when she started her own full-working farm shortly after leaving her job as editor-in-chief of Fine Cooking magazine. Fresh From the Farm captures Middleton’s experience in her rural world growing vegetables, raising chickens, and enjoying the fruits of her labor.
The book not only includes 125 delicious recipes but also tells a story of how a farmer came to be. Middleton’s captivating stories of life on the farm, woven through the pages of her delicious recipes, truly give the reader a sense of escape and an appreciation for the simpler life. Its
BOOKSHELF

accompanying photos take the reader on a journey from the farm to the prepared meals on the dinner table.
Divided into three categories by growing seasons—Late Spring and Early Summer, High Summer, and Indian Summer and Early Fall—this is a book focused on fresh, simple dishes both cooks and aspiring gardeners or farmers can learn from. I particularly like Middleton’s focus on basic food preparation tips for fruits and vegetables, such as those showcased in her recipes for Slow-Roasted Beefsteak Tomatoes and Roasted Carrot “Fries” With Roadhouse Dipping Sauce.
Interjections of “Cook’s Tips” throughout the book offer additional advice for novice to experienced cooks, ranging from tips for properly preparing wheat berries to serving perfectly warm French toast to shelling fava beans. The appendix offers advice for individuals aspiring to start their own garden market or simply wanting to try their hand at a small-scale backyard farm.
The Roasted Butternut Squash Risotto With Thyme, Parmigiano and Toasted Pine Nuts was a personal favorite recipe, as was the one for the Chocolate-Chocolate Chip Zucchini and Raspberry Muffins; they were among the best muffins/cupcakes I’ve ever made, and I had multiple friends and family members begging for the recipe.
This certainly is a book that both RDs and food lovers can embrace, as it showcases healthful, nutrient-rich foods in all their glory. Middleton’s approachable style welcomes the reader in and shows them how delicious simple foods grown straight from the land truly can be.
— McKenzie Hall, RD, is a cofounder of Nourish RDs, a nutrition communications and consulting business based in Los Angeles.
Whole-Grain Mornings: New Breakfast Recipes to Span the SeasonsBy Megan Gordon2014, Ten Speed PressHardcover, 184 pages, $22
Finding time in the morning to make a breakfast complete with whole grains and natural, seasonal foods can be a chal-lenge, and you may find yourself reaching for prepared cere-als or other fast but not-so-healthful choices.
Megan Gordon aims to help you start your day right with a collection of 65 wholesome and innovative breakfast recipes.
Seasonal recipes, such as Greens and Grains Scramble and Strawberry Rhubarb Quick Jam, complement breakfast staples such as Whole-Grain Pancake Mix and The Very Best Oatmeal.
The book begins with a peek inside Gordon’s cupboard. Stocking up on some basics, such as certain spices, herbs, oils, and natural sweeteners, will be helpful in making Gordon’s recipes. She also provides an overview of whole grain flours plus how to store and cook them. Packed with fiber, protein, and amino acids, whole grains provide ample energy and keep you feeling fuller longer.
Each chapter features a “Seasonal Spotlight” on different fruits and veggies. You’ll get tips on how to select, store, and prepare them. “Make It Your Own” recipe suggestions encourage both novice and experienced chefs to get creative in the kitchen.
Keep in mind that while some of the recipes may be fairly easy and quick to make, you may have to plan ahead and pur-chase some of the ingredients or even refrigerate prepared ingredients overnight. Helpful “Make Ahead” tips easily will guide you with this. Cooking times may be longer than you can allot on a busy morning as well. However, Gordon is careful to include how to properly store your creations in the fridge or freezer and how long they will last.
The book, which features many colorful, mouth-watering photos, goes beyond the kitchen, too. Gordon delightfully shares her personal journey of successfully founding a busi-ness—Marge Granola—and relocating from San Francisco to Seattle to be with a newfound love.
So whether you’re making it fresh or you’re grabbing it on the go from the fridge, make your mornings nourishing with these tried-and-true recipes. Clients seeking nourishing breakfast ideas are sure to enjoy them, too.
— Karen Appold is a freelance medical writer and editor based in Pennsylvania’s Lehigh Valley.

PRODUCTS + SERVICES
Real McCoy’s Rice Chips and Puffs Bear Whole Grains Stamp
Real McCoy’s Snacks offers a line of all-natural, gluten-free rice chips and puffs made with whole grain, non-GMO ingredients.
Handcrafted with organic whole grain kernels of brown rice, these snacks are free of trans fats and bear the Whole Grains Stamp of approval from the Whole Grains Council.
Real McCoy’s Rice Chip flavors include Sweet & Spicy, Worces-ter & Chives, and Sea Salt. Real McCoy’s Rice Puffs flavors include Vermont White Cheddar, Jalapeño Cheddar, and Hatch Chile.
For more information, visit http://realmccoysnax.com.
Primal Essence Releases Teas, Coconut Oil Products
Primal Essence, an organic and natural extracts producer, is showcasing its own brand of certified organic, all-natural Organic Super Teas and Infused Coconut Oils.
In Classic Chai, Ginger Zing, Lemon Ginger, Peppermint Splash, Turmeric Tulsi, and Vanilla Chai varieties, Primal Essence’s Organic Super Teas come in 45-mL pump bottles that are loaded with natural phytonutrients and antioxidants. With just two or three squirts, the teas can be used in water, juice, and coffee.
With just a spoonful of Infused Coconut Oil, which comes in Garlic Onion, Indian Curry, Italian Herb, Lemon Pepper, Smoked Chili, and Thai Curry varieties, dishes exude natural flavors from whole-food extracts with all the benefits of coconut oil.
For more information, visit www.primalessence.com.
PowerICE Debuts New Flavors of Frozen Bars
PowerICE has announced that its frozen hydration bars, designed to enhance performance in athletes by cooling the core body temperature while replenishing lost electrolytes, are now made with 100% all-natural ingredients.
The company also has doubled the number of flavors in its lineup, introducing Pomegranate Raspberry Rip and Grape Score to accompany original flavors Lime Kicker and Orange Blast.
For more information, visit www.powerice.com.
GloryBee Adds New Raw Honey Varieties
GloryBee, a family-owned and -operated provider of all-natural honey, sweeteners, spices, dried fruits, nuts, and oils, has rolled out five new raw honey flavors: Raw California Orange Blossom, Raw Mountain Wildflower, Raw Organic Tropical Blossom, Raw Pacific Northwest Clover, and Raw Pacific Northwest Raspberry.
GloryBee’s new honey flavors are raw, meaning the honey hasn’t been heated above 115˚F, pasteurized, or processed in any way, allowing the honey to retain a more creamy texture. Raw honey contains bee pollen, vitamins, enzymes, antioxidants, and other important natural nutrients.
For more information, visit http://glorybee.com.
Xlear Introduces Spry Gems Mints
Xlear (pronounced “clear”) has developed a new line of mints called Spry Gems. Consuming too much sugar can lead to various dental issues, including damage to the teeth, gums, and oral tissues. Spry Gems give candy lovers the best of both worlds by delivering treats that taste great and promote good oral health.
Available in Peppermint, Berry, Spearmint, and Cinnamon flavors, Spry Gems contain xylitol, a natural sweetener, and are formulated with all-natural ingredients. In addition, their pH-balanced formula helps protect and preserve oral health, and Spry Gems provide calcium for increased tooth enamel remineralization.
For more information, visit www.xlear.com.
Pitcher Filters Water at the Speed of Your Faucet
CamelBak has introduced Relay, the first water filtration pitcher to filter water at the speed of your faucet. It relies on a unique, pleated double-filter technology system that filters water twice, once as the pitcher is filled and again as water is poured. The Relay Fresh Filter lasts for four months with regular usage. Independent test results have shown Relay removes 97% of chlorine, taste, and odor.
Now available nationwide, CamelBak Relay is BPA-free and dishwasher safe.
For more information, visit www.camelbak.com.
60 today’s dietitian august 2014

Bump Water Packs in Folic Acid for Pregnant Women
Developed by two moms who saw a need for a prenatal vitamin-infused water, Bump Water is a functional, all-natural beverage designed to ensure women get enough folic acid to help their developing baby. Bump Water contains 100% of the Recommended Dietary Allowance of folic acid; vitamins A, D, B6, and B12; niacin; biotin; zinc; and magnesium.
Bump Water comes in four flavors, including Sparkling Lemonade and Sparkling Cranberry Ginger.
For more information, visit www.bumpwater.com.
Corazonas Expands Line of Heart-Healthy Oatmeal Squares
Corazonas Foods, maker of snacks infused with choles-terol-lowering plant sterols, has added Chocolate Coconut Macaroon and Orange Cranberry Oatmeal Squares to its line of heart-healthy snacks.
The bars join the brand‘s classic Oatmeal Squares lineup, which includes seven different options, from Peanut Butter and Blueberry to Chocolate Brownie & Almonds. Like the existing flavors, the new bars have 15 to 16 g of whole grain oats, 6 g of protein, and 5 g of fiber with no trans fat. They’re the only bars proven to lower LDL cholesterol and have no wheat, flour, or high-fructose corn syrup. Each bar is made with oats, apple juice–infused fruits, and fruit purée.
For more information, visit http://corazonas.com.
KIND Releases Savory Snack Line
KIND Healthy Snacks has released STRONG & KIND, the brand’s first savory snack line. STRONG & KIND has 10 g of natural protein (soy- and whey-free) from ingre-dients such as whole almonds, seeds, and legumes that, when combined, pack all nine essential amino acids. The new line features five flavors: Honey Smoked BBQ, Honey Mustard, Roasted Jalapeño, Hickory Smoked, and Thai Sweet Chili.
As with other KIND products, STRONG & KIND is gluten-free, non-GMO, low sodium, and contains no MSG.
For more information, visit www.kindsnacks.com.
Seapoint Farms Adds Dry Roasted Black Edamame Snack
Seapoint Farms is debuting its new snack: Dry Roasted Premium Black Edamame With Sea Salt.
Black edamame is made from a unique variety of black soy-bean that’s distinctly sweet and prized in Japan. It’s high in nutritional value due to the levels of omega-3 fatty acids, iron, vitamin K, and anthocyanins.
The product joins Seapoint Farms’ other black edamame snack, Crunchy Coated Premium Black Edamame. Like all of Seapoint Farms edamame, it’s gluten-free, heart healthy, and non-GMO. It has 14 g of complete protein per serving, is a good source of fiber, is cholesterol-free, and has just 130 kcal per serving.
For more information, visit www.seapointfarms.com.
Cluck ’n Moo Cuts the Fat, Seals in the Flavor
Cluck ’n Moo Burger is a proprietary crafted blend of humanely raised antibiotic- and hormone-free, grass-fed beef and humanely raised antibiotic- and hormone-free chicken. The hybrid burger is Certified Gluten Free and has 52% less fat, 34% fewer calories, and 57% less saturated fat than a typical grass-fed beef burger. The company’s Smashed Burger production method allows the burgers to cook quickly by sealing in the juices and keeping them moist.
For more information, visit http://clucknmoo.net.
Welch’s New 100% Juice Line Hits Stores Nationwide
Welch’s brings the Farmer’s Pick line of 100% juices to the juice aisle. Available in Concord Grape, Mango, and Blackberry flavors, Farmer’s Pick contains no preservatives, artificial flavors, synthetic colors, or ingredients. Unlike most 100% fruit juices in the shelf-stable juice aisle, Welch’s new line contains unfiltered juice.
In addition to using unfiltered juice, Welch’s uses cold-kettle batching to bring the fresh-picked fruit flavors of Farmer’s Pick to life. When batching the juice, Welch’s keeps the kettles cool to help preserve the delicate flavor and aroma of the fruits used to make the juice.
For more information, visit www.welchs.com.
august 2014 www.todaysdietitian.com 61

RESEARCH BRIEFS
Study Confirms Diet Beverages Aid Weight Loss
A new study published in Obesity confirms that drinking diet beverages helps people lose weight.
“This study clearly demonstrates that diet beverages can in fact help people lose weight, directly countering myths in recent years that suggest the opposite effect: weight gain,” says James O. Hill, PhD, executive director of the Univer-sity of Colorado Anschutz Health and Wellness Center and a study coauthor. “In fact, those who drank diet beverages lost more weight and reported feeling significantly less hungry than those who drank water alone. This reinforces that if you’re trying to shed pounds, you can enjoy diet beverages.”
The 12-week clinical study of 303 participants is the first prospective, randomized clinical trial to directly compare the effects of water and diet beverages on weight loss within a behavioral weight-loss program. Conducted simultaneously by researchers at the University of Colorado Anschutz Center for Health and Wellness in Aurora and Temple University’s Center for Obesity Research and Education in Philadelphia, the study shows that subjects who consumed diet beverages lost an average of 13 lbs—44% more than the control group, which lost an average of 9 lbs.
More than one-half of the participants in the diet beverage group (64%) lost at least 5% of their body weight, compared with only 43% in the control group. Losing just 5% of body weight has been shown to significantly improve health, including lowering the risk of heart disease, high blood pressure, and type 2 diabetes.
“There’s so much misinformation about diet beverages that isn’t based on studies designed to test cause and effect,
especially on the Internet,” says John C. Peters, PhD, a study coauthor and the chief strategy officer of the Anschutz Health and Wellness Center. “This research allows dieters to feel confident that low- and no-calorie sweetened beverages can play an important and helpful role as part of an effective and comprehensive weight loss strategy.”
Study participants were randomly assigned to one of two groups: those who were allowed to drink diet beverages, such as diet sodas, teas, and flavored waters, or those who were in a control group that drank only water. With the exception of beverage options, both groups followed an identical diet and exercise program for the duration of the study.
In addition to losing 44% more weight than the control group, the diet beverage group also reported feeling signifi-cantly less hungry, showed significantly greater improve-ments in serum levels of total and LDL cholesterol, and saw a significant reduction in serum triglycerides. Both diet soda and water groups saw reductions in waist circumference and blood pressure.
This latest study adds to the body of research demon-strating that diet beverages don’t hinder, but in fact help, with weight loss. In particular, two studies published in the American Journal of Clinical Nutrition in 2012 and 2013 by researchers from the University of North Carolina randomly assigned nondieting participants to drink either water or diet beverages. While both groups cut their food intake sig-nificantly, after six months, the diet beverage group had a greater likelihood of reaching a meaningful (5%) amount of weight loss compared with the control group. The diet beverage group also experienced a greater reduction in dessert consumption than the water group. Overall, the findings suggest that diet beverages don’t fuel a preference for sweet foods and drinks.
Additional research published in 2009 on weight-loss maintenance, drawn from the National Weight Control Registry, found that successful weight-loss maintainers drank three times more diet beverages than those who had never lost weight.— SOURCE: UNIVERSITY OF COLORADO DENVER ANSCHUTZ MEDICAL CAMPUS
“ This study clearly demonstrates that diet beverages can in fact help people lose weight, directly countering myths in recent years that suggest the opposite effect: weight gain.”
— James O. Hill, PhD
62 today’s dietitian august 2014

Lewes, Delaware • beebehealthcare.org
Part Time position to cover operational hours of 8am - 5pm, Monday-Friday. BSN required. State of Delaware RN license or Compact State. Must have current BLS through American Heart Association. Provides individual and group education to persons with Diabetes, their families, and appropriate support systems about diabetes self-management and related issues. Addresses educational needs of other health care professionals who do not specialize in diabetes, and the public. Performs basic foot and nail care to individuals with diabetes. Administers diabetes health management education to children, pregnant women, adults, and elderly individuals within the Beebe Medical Center inpatient or community populations.
PLEASE VISIT OUR WEBSITE FOR COMPLETE JOB DESCRIPTIONS [email protected] 302-645-3336EOE | 424 Savannah Rd, Lewes, DE 19958 www.facebook.com/beebecareers
Beebe Healthcare, located in Lewes, DE, offers you a unique Work/Life balance set in a beautiful, tranquil setting with exceptional leadership and an award winning staff of professionals. What do you want to Be?
RN-Certified Diabetes Educator/ Diabetes Management - Part Time
Be InspiredAre you looking for a patient-centered, team-oriented work environment where you will make a difference in patient lives?
Community Hospice has the position for you where you’ll be able to practice in a truly interdisciplinary supportive team environment. Dietitian will perform the coordination of all phases of diet therapy, including nutrition assessment, nutrition care planning, patient monitoring, and patient and family education. Full time, part time, or per diem positions available. Pay range is $32.00-$37.00/hr. Qualifi ed candidates must possess current registration with the Commission on Dietetic Registration and a B.S. in Nutrition, Dietetics, or related fi eld.
To apply, please send résumé via e-mail:[email protected] or apply online at
http://careers.hospiceheart.org/careers. EOE
Registered Dietitian
www.hospiceheart.org
TD_CA_CommHospice.indd 1 7/18/14 5:19 PM
FT Experienced Dietitian needed to support communityhealth needs. Duties include outpatient & inpatient diabetes and nutrition education with coverage of inpatient care, including screening, assessment, andnutrition support. Other duties may include coverage to outreach clinics and community education events as needed. RD required. Two years of experience in a hospital clinical setting is required. CDE certificationrequired within 6 months of hire. Our 176-bed accreditedregional acute care medical center is located in a 60,000rural population community at the base of the beautifulCascade Mts., all-season recreation, 280 days of sunshine each year, and friendly atmosphere.Competitive salary/benefits, including interview andrelocation assistance.
For more information about our facility/communityand to apply for this vacancy, visit our website at
www.skylakes.org.
SUCCESSin Your Allied Health Search
The KEY to
Bakery On Main introduces 12 new ways to put a smile on those gluten-free tastebuds: three as-good-for-you-as-they-taste flavors of Soft & Chewy bars packed with whole grains; six exotic flavors of Truebars, an honest-to-goodness line of fruit and nut bars that say “I’ve got nothing to hide”; and three irresistible bakeshop Instant Oatmeal flavors pumped up with chia, flax, amaranth, and quinoa.
For more information visit www.bakeryonmain.com or contact [email protected] to request a sample.
Sponsored Content
Product PreviewADVERTISER INDEXFor advertising information, please call 800-278-4400 or visit our website at www.TodaysDietitian.com.
Alberta Barley Commission, http://gobarley.com ......................................... 15
Almased, www.almased.com ............................................................................ 9
Bakery On Main, www.bakeryonmain.com ..................................................... 63
CherryFlex, www.cherryflex.com ................................................................... 65
Daisy Brand Cottage Cheese, www.daisybrand.com/cottagecheese ............. 4
Domino Foods, www.dominosugar.com/light www.chsugar.com/light .................................................................................... 3
Hass Avocado Board, www.loveonetoday.com/hpresources .......................... 2
Merisant US Inc., www.equal.com .................................................................. 64
Merisant US Inc., www.purevia.com............................................................... 64
NASPGHAN, www.naspghan.org .................................................................... 35
Overeaters Anonymous, www.oa.org ............................................................. 13
Purity Foods, www.natureslegacyforlife.com................................................. 64
Rosalind Franklin, www.rosalindfranklin.edu/chp/nutrition.aspx ................. 64
TH Foods, www.thfoods.com .......................................................................... 27
Vitatech/Cinsulin, www.cinsulin.com ............................................................ 68
Wisdom/Sweetleaf, www.sweetleaf.com ....................................................... 67
This index is a service to our readers. The publisher assumes no liability for errors or omissions.
august 2014 www.todaysdietitian.com 63
DE • O
R • CA

Sponsored Content
ShowcaseSummer
Made from the pure, sweet extract of the stevia leaf, Pure Via® is a natural alternative to sugar and artificial sweeteners. Pure Via® sweetener is zero calorie and is an ideal product for people who want to make healthier lifestyle choices. We are proud that Pure Via’s ingredients are simple, all natural and sourced from Non-GMO plants (not the product of bioengineering). Pure Via®’s secret? The great taste!
www.Purevia.com Please visit us at AADE booth number 937.
Pure Via is a registered trademark of Whole Earth Sweetener Co. LLC © 2014 Whole Earth Sweetener Co. LLC.
Equal® Original 0-Calorie sweetener has been your trusted sweetener for over 30 years. This sweetener is great for anyone reducing their sugar intake, especially those seeking healthier lifestyles, including individuals with diabetes. Equal has launched a new natural sweetener, also 0 calories, “Naturals™.” It is a delicious blend of Monk Fruit and Stevia extract. Please stop by our booth at the AADE Tradeshow and sample treats made with Equal and Naturals™.
www.equal.com • www.naturalssweetener.com Please visit us at AADE booth number 937.
©2014 Merisant Company. Equal is a registered trademark and Naturals is a trademark of Merisant Company.
0 calorie sweetener
NO NEED TO COMPROMISE!100% Whole grain goodness100% Delectable taste100% Silky smooth texture
To try it for yourself, call: Purity Foods, Inc. Hudson, MI 49247
1-800-99-SPELT (1-800-997-7358)
UNDENIABLY DELICIOUS
As natural as it gets!
Move Forward in Your Career Nutrition and Health Promotion
Flexible Online Degree Programs
• Master of Science in Clinical Nutrition
• Master of Science in Nutrition Education
• Master of Science in Prevention, Health Promotion and Wellness
• Innovative curriculum highlight current health problems, interventions and related professional skills
• Teamwork and leadership themes
• University focus on health sciences
• Experienced expert faculty
• No on-campus requirement
Department of Nutrition – College of Health Professions www.rosalindfranklin.edu/chp/nutrition.aspx
64 today’s dietitian august 2014

SEPTEMBER 2-5, 201414TH INTERNATIONAL NUTRITION & DIAGNOSTICS CONFERENCEPrague, Czech Republicwww.indc.cz/en
SEPTEMBER 8-10, 2014NATIONAL WIC ASSOCIATION NUTRITION EDUCATION AND BREASTFEEDING CONFERENCE & EXHIBITSAtlanta, Georgiawww.nwica.org
SEPTEMBER 12, 2014COLORADO SOCIETY FOR PARENTERAL AND ENTERAL NUTRITION 29TH ANNUAL NUTRITION SUPPORT SYMPOSIUMAurora, Coloradowww.nutritioncare.org
SEPTEMBER 12, 2014OKLAHOMA ACADEMY OF NUTRITION AND DIETETICS FALL SYMPOSIUMEdmond, Oklahomahttp://oknutrition.org
OCTOBER 11, 2014AMERICAN DIABETES ASSOCIATION DIABETES EXPOMinneapolis, Minnesotawww.diabetes.org
OCTOBER 24, 2014FOOD DAYA nationwide celebration and
movement for healthful, affordable, and sustainable food
www.foodday.org
OCTOBER 29-31, 2014AMERICAN INSTITUTE FOR CANCER RESEARCH ANNUAL RESEARCH CONFERENCE ON FOOD, NUTRITION, PHYSICAL ACTIVITY, AND CANCERWashington, D.C.www.aicr.org
NOVEMBER 5-6, 2014IOWA ACADEMY OF NUTRITION AND DIETETICS ANNUAL MEETINGWest Des Moines, Iowawww.eatrightiowa.org
NOVEMBER 8, 2014AMERICAN DIABETES ASSOCIATION DIABETES EXPOPittsburgh, Pennsylvaniawww.diabetes.org
NOVEMBER 21, 2014CHILDREN’S HOSPITAL OF PHILADELPHIA EMERGING TOPICS IN PEDIATRIC NUTRITION: A PRACTICAL APPROACHPhiladelphia, Pennsylvaniawww.chop.edu/cme
NOVEMBER 22, 2014AMERICAN DIABETES ASSOCIATION DIABETES EXPOAtlanta, Georgia, and Portland, Oregonwww.diabetes.org
DECEMBER 4-6, 2014AMERICAN SOCIETY FOR NUTRITION ADVANCES AND CONTROVERSIES IN CLINICAL NUTRITIONWashington, D.C.www.nutrition.org
MARKETPLACEDATEBOOK
BEGINNING AUGUST 1, 2014REGISTRATION NOW OPEN FOR THE 2014 RENFREW CENTER FOUNDATION EATING DISORDERS CONFERENCE FOR PROFESSIONALS — “FEMINIST RELATIONAL PERSPECTIVES AND BEYOND: THE ‘PRACTICE’ OF PEOPLE”November 14-16, 2014Philadelphia, PennsylvaniaFeaturing specialized workshops
for dietitians and nutrition therapists
17.5 continuing education credits available
Contact: Debbie LuckerPhone: 877-367-3383E-mail: [email protected]
SEPTEMBER 26, 2014ENHANCING HEALTH WITH PLANT-BASED NUTRITION PROFESSIONAL MEDICAL CONFERENCEOregon Convention Center,
Oregon Ballroom777 NE MLK Jr BlvdPortland, Oregonhttp://nwveg.org/health_
conference
Datebook listings are offered to all nonprofit organizations and associations for their meetings. Paid listings are guaranteed inclusion. All for-profit organizations are paid listings. Call for rates and availability.
Call 610.948.9500
Fax 610.948.7202
E-mail [email protected]
Send Write with your listing two months before publication of issue.
august 2014 www.todaysdietitian.com 65

SWEET CORNIt’s What’s for BreakfastBy Grace Dickinson
As a child, I would have told you that corn should be eaten solely on the cob. A quarter of its kernels should be smeared across your face and hands, and if you were lucky, you’d look like a Dalmatian pup because of the char marks left on your face from the grilled kernels.
Some of my fondest summertime childhood memories stem from corn on the cob. I remember helping my dad lug large buck-ets of ice water up the grassy hill near our charcoal grill. He’d soak the ears of corn then throw them on the hot grates, letting me play basketball while they cooked. As the corncobs steamed in their husks, I’d either beg my dad to join me in a game of hoops or ask him every two minutes how much longer did I have to wait until dinner was ready. I was a typical impatient kid with an atypical appetite for corn on the cob.
Inherently sweet, corn is the veggie version of candy, from the kernels down to the sugary cob, on which I often found myself chewing. At dinnertime, I’d frequently eat five cobs of corn served alongside nothing else but a pat of butter and salt.
I cherish these childhood memories, but I’m all grown up now and would rather not have a bunch of kernels lodged in my teeth and smeared across my face. Now I even conjure up ways to go beyond single-ingredient meals and have a desire to use corn’s sweetness to compliment other flavors in a recipe. These days, I find myself using seasonal ingredients for inspiration to create a complete meal.
The following breakfast taco recipe is a good example of this and has become an annual summertime favorite. Keeping it rela-tively simple, fiber-filled corn teams up with buttery squash, a bit of feta, and vine-ripened tomatoes. All the ingredients take corn’s sweetness to another level, and with the help of a few fluffy eggs, this dish becomes a well-balanced meal.
For added flavor, grill your corn ahead of time, and add it in with the first tomato. If you’re like me, you’ll end up munching on a cob for old time’s sake while you prepare the meal.
— Grace Dickinson is a photo enthusiast, food blogger, and recipe developer for FoodFitnessFreshAir.com.
CULINARY CORNER
Summer Squash and Corn Breakfast Tacos
These breakfast tacos are perfect for all meals. If you don’t have a gas stove, warm the tortillas by placing them in a dry (no oil) stainless steel skillet over medium heat for about 30 seconds on each side.
Serves 4
Ingredients2 T extra-virgin olive oil1 medium white onion, diced1 serrano pepper, minced2 small summer yellow squash, julienned into
2-inch strips2 ears of corn, kernels sliced from the cobSalt and pepper, to taste2 medium tomatoes, diced6 large eggs2 T milk8 (6-inch) soft white corn tortillas5 oz feta cheese, crumbled1/2 cup cilantro, choppedHot sauce, optional
Directions1. In a large sauté pan, heat oil over medium-high heat. Add onion and serrano pepper, and sauté for 2 minutes. Stir in yellow squash and corn, and sauté for another 3 minutes. Season with salt and pepper. Add one tomato and continue to cook until onion and squash are tender, stirring regularly, about 5 minutes.2. In a small bowl, whisk eggs with milk and a dash of salt and pepper. Pour them into the pan with the vegetable mixture. Cook, stirring occasionally, until eggs are fluffy and cooked through, 2 to 4 minutes.3. Using tongs, place corn tortillas over a gas flame for 30 seconds on each side to slightly char the outside. Place on a plate and top each tortilla with a spoonful of the egg mixture. Crumble feta on top, and sprinkle with cilantro and the remain-ing chopped tomato. Serve, with a side of hot sauce, if desired.
Nutrient Analysis per servingCalories: 420; Total fat: 10 g; Sat fat: 4 g; Trans
fat: 0 g; Cholesterol: 300 mg; Sodium: 415 mg; Total carbohydrate: 30 g; Dietary fiber: 5 g; Sugar: 5 g; Protein: 9 g
66 today’s dietitian august 2014

®
Enhance the fl avor of your water, naturally and guilt free
Experts say drinking water throughout the day is the best and easiest way to get or stay healthy.
With more than 20 irresistible fl avors, SweetLeaf® Liquid Stevia Sweet Drops™ sweeteners can turn that glass or bottle of boring water into pure pleasure. Better hydration leads to healthier and clearer skin, helps in weight management and improves mental function.
Have water the way you want it with SweetLeaf Sweet Drops!
NO calories NO carbsNO sugar NO glycemic response
BUY: www.ShopSweetLeaf.com and in your natural foods or grocery store
RECIPES & MORE: SWEETLEAF.COM
The only stevia brand consistently winning international awards for taste and innovation.
016371_WNB_Todays Dietitian_Aug 2014.indd 1 7/21/14 11:04 AM

Roses are red, violets are blue, Maintaining healthy blood sugar is what Cinnamon can do.†*
New Veggie Caps!Gluten Free!
† within the normal range*This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
cinsulin.com
.com
. . . And the only water extract of cinnamon ingredient that’s patented and clinically studied to support healthy
blood sugar levels, safely and naturally, is CinSulin®. †*
CinSulin is di�erent from ordinary cinnamon. Its patented water extraction process ensures you’re getting only the
healthy components of the cinnamon plant. It’s concentrated, too, so just two capsules equal 10
ordinary cinnamon capsules.
The amount of sugar in your blood can be a�ected by weight, diet, exercise, smoking, blood
pressure, family history and stress. If any of these factors describes you, it’s
time to try CinSulin.