Tobacco Related Cancers Philip C. Nasca, MS, PhD, FACE State University of New York At Albany School...
35
Tobacco Related Cancers Philip C. Nasca, MS, PhD, FACE State University of New York At Albany School of Public Health
-
Upload
milton-garrison -
Category
Documents
-
view
216 -
download
1
Transcript of Tobacco Related Cancers Philip C. Nasca, MS, PhD, FACE State University of New York At Albany School...
Tobacco Related Cancers
Philip C. Nasca, MS, PhD, FACE
State University of New York At Albany
School of Public Health



Annual Deaths Attributable to Cigarette Smoking – United States, 200-2004



Assessing Causality
A. Strength of Associations: There are mathematical techniques for measuring how strongly two variables are associated, to be discussed later in the course. Strong associations are more likely to be causal than weak associations; but the fact that an association is weak does not rule out a causal association
B. Consistency: Repeated observation of an association in different populations, at different times, using different methodologies
C. Biologic Credibility (Plausibility):An assessment of how credible the inference is, based on available biologic evidence
Assessing Causality
D. Temporality (Time Sequence): The necessity that cause precede effect in time. This is a necessary part of causal inference, but sometimes temporal information is not available.
E. Biologic Gradient (Dose-Response Relationship): The observation of a gradient of risk associated with the degree of exposure.
F. Experimental Evidence: Strong, but such information is seldom available for human populations. Animal data are often used, e.g. to test if a particular substance may be carcinogenic and then these data are used by analogy, to support observational data that the substance is associated with cancer in humans.
Assessing Causality
G. Coherence: Agreement between the hypothesized cause and the known facts of the natural history and biology of the disease. Very similar to “biologic credibility”.
H. Analogy: A very weak criterion since an analogy with a different causal association may not pertain to the association in question. Good for hypothesis generation.
I. Specificity: Of historic and pedagogic interest only. This criterion states that one cause should lead to a dingle, not multiple effects. This has been advanced by many others (Koch-Henle postulates of infectious disease), but, even with reservations, it appears obvious that single events/causes/exposures can have many effects.
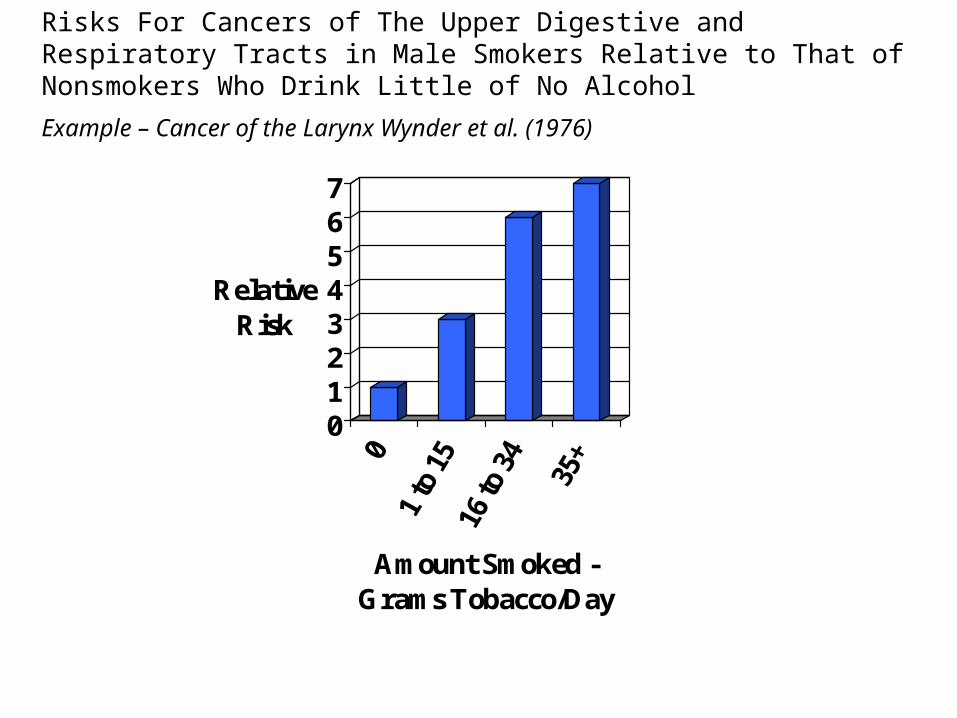
01234567
Relative Risk
Amount Smoked - Grams Tobacco/Day
Risks For Cancers of The Upper Digestive and Respiratory Tracts in Male Smokers Relative to That of Nonsmokers Who Drink Little of No Alcohol
Example – Cancer of the Larynx Wynder et al. (1976)

Risks For Cancer of the Pancreas in Cigarette Smokers Relative to That For Nonsmokers – Wynder et al. (1983)
0
0.5
1
1.5
2
2.5
3
Relative Risk
0 1 to 10 11 to 20 21 to 30 >/=31
Daily # Cigarettes
MalesFemales
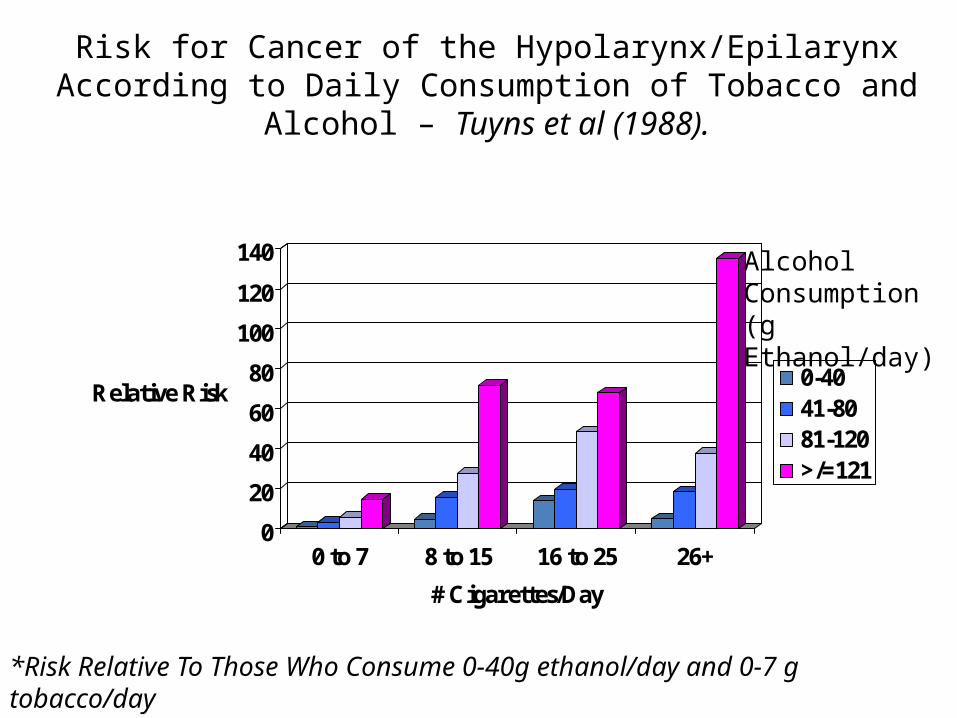
Risk for Cancer of the Hypolarynx/Epilarynx According to Daily Consumption of Tobacco and Alcohol – Tuyns et al (1988).
0
20
40
60
80
100
120
140
Relative Risk
0 to 7 8 to 15 16 to 25 26+
# Cigarettes/Day
0-4041-8081-120>/=121
Alcohol Consumption(g Ethanol/day)
*Risk Relative To Those Who Consume 0-40g ethanol/day and 0-7 g tobacco/day
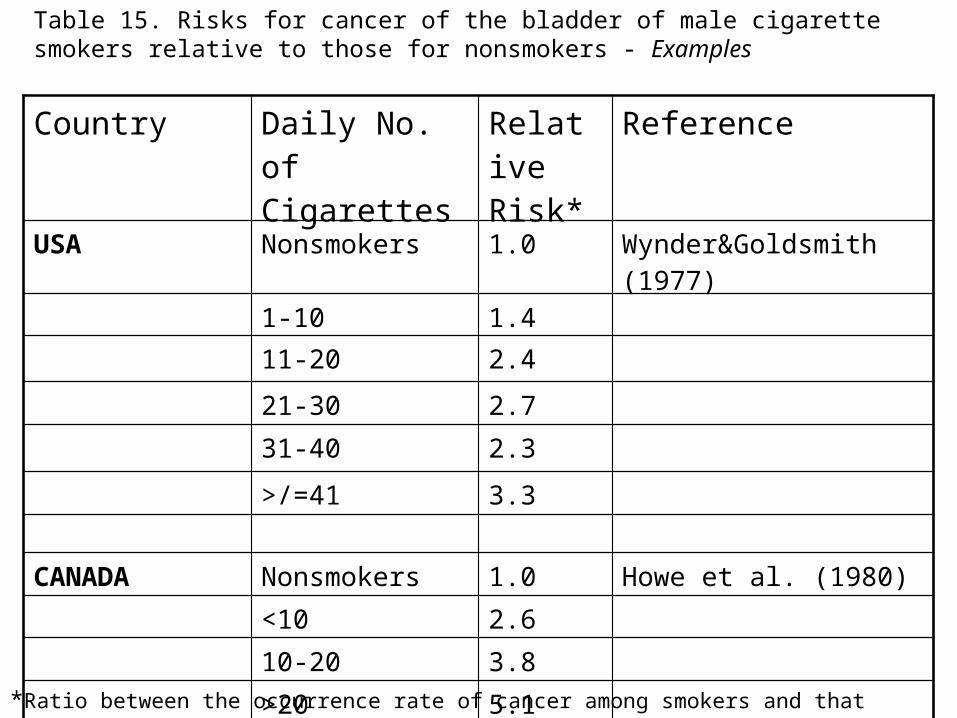
Table 15. Risks for cancer of the bladder of male cigarette smokers relative to those for nonsmokers - Examples
Country Daily No. of Cigarettes
Relative Risk*
Reference
USA Nonsmokers 1.0 Wynder&Goldsmith (1977)
1-10 1.4
11-20 2.4
21-30 2.7
31-40 2.3
>/=41 3.3
CANADA Nonsmokers 1.0 Howe et al. (1980)
<10 2.6
10-20 3.8
>20 5.1*Ratio between the occurrence rate of cancer among smokers and that among nonsmokers
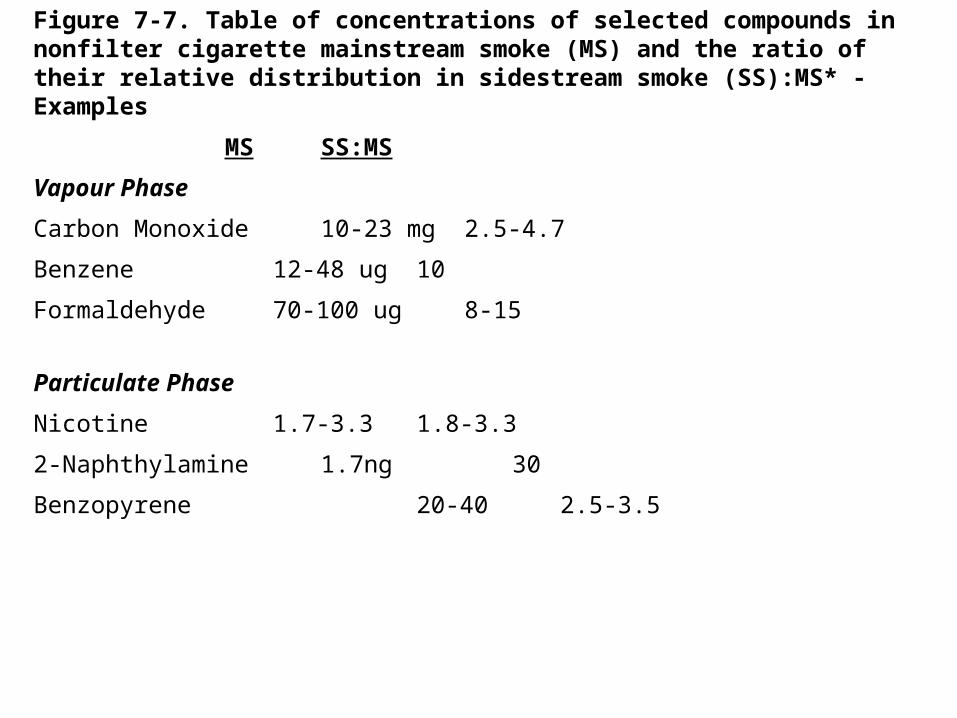
Figure 7-7. Table of concentrations of selected compounds in nonfilter cigarette mainstream smoke (MS) and the ratio of their relative distribution in sidestream smoke (SS):MS* - Examples
MS SS:MS
Vapour Phase
Carbon Monoxide 10-23 mg 2.5-4.7
Benzene 12-48 ug 10
Formaldehyde 70-100 ug 8-15
Particulate Phase
Nicotine 1.7-3.3 1.8-3.3
2-Naphthylamine 1.7ng 30
Benzopyrene 20-40 2.5-3.5

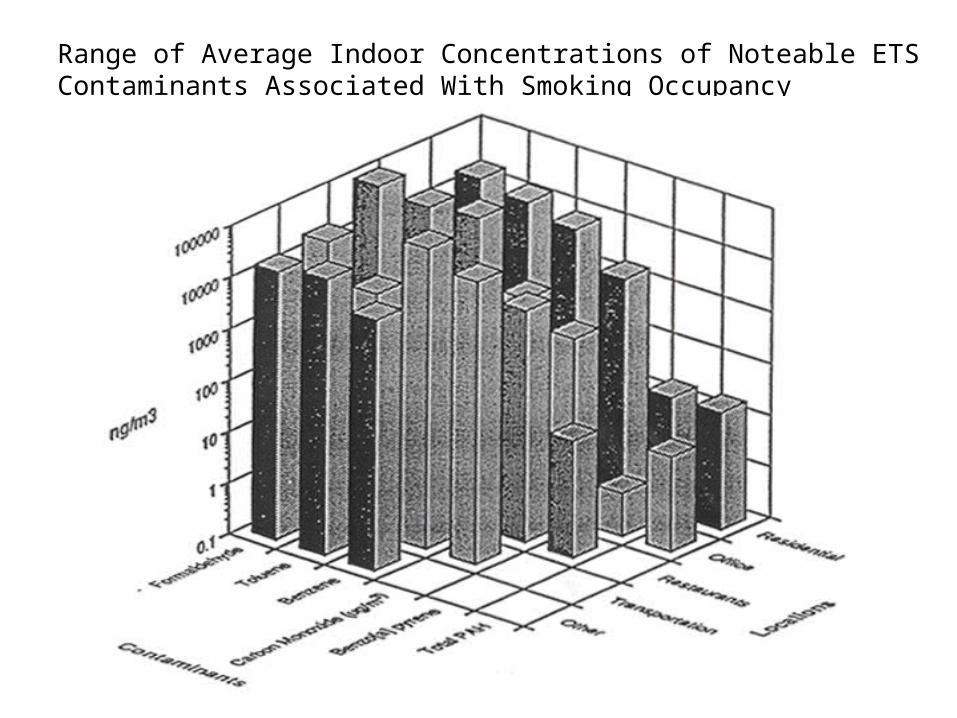
Range of Average Indoor Concentrations of Noteable ETS Contaminants Associated With Smoking Occupancy

0123456789
10111213141516
Cotinine (mg/ml)
Mean Cotinine(mg/ml)
Number of Exposures in the Past 4 Days
Figure 3-16. Urinary cotinine concentrations by number of reported exposures to tobacco smoke in the past 4 days among 663 nonsmokers, Buffalo, New York, 1986

Table 5-11. Exposure Response Trends For Females – Smoking By Spouse
Study Exposure RR* C.I
Font (Years) 0 1.0
1-15 1.33 (0.93, 1.89)
16-30 1.40 (0.96,2.05)
>30 1.43 (0.99, 2.09)
Font (Pack Years) 1.0
0<15 1.03 (0.73, 1.46)
15-39 1.26 (0.85, 1.87)
40-79 1.49 (0.98, 2.27)
>/=80 1.70 (0.82, 3.49)

Table 5-11. Exposure Response Trends For Females – Smoking By Spouse
Study Exposure RR* C.I
Geng (Cig./Day) 0 1.0
1-9 1.40 (1.1, 1.8)
10-19 1.97 (1.4, 2.7)
>/= 20 2.76 (1.9, 4.1)
Geng (Years) 0 1.0
<20 1.49 (1.15, 1.94)
20-39 2.23 (1.54, 3.22)
>/=40 3.32 (2.11, 5.22)
HISTORY OF SMOKELESS TOBACCO
Smokeless tobacco was used in the United States in the early 1600s when snuff made its way to the Jamestown Colony in Virginia through the efforts of John Rolfe in 1611 (1). Evidence of tobacco chewing, however, was not until a century later in 1704 (2).

A Chinese Law in 1683 Threatened That Anyone Possessing Tobacco Would Be Beheaded
HISTORY OF SMOKELESS TOBACCO
In the past, tobacco use was considered by some as beneficial.
•3500 B.C. tobacco an article of value – Mexico and Peru
•Alleviation of hunger pains
•Medicinal Uses: In Native Americans – to alleviate toothaches, disinfect cuts and relieve the effects of snake, spider, and insect bites
•19th and 20th centuries used to relieve toothache, to cure neuroglia, bleeding of gums, and scurvy
•To preserve and whiten teeth and prevent decay
CHEWING TOBACCO
•Looseleaf
•Plug
•Twist
SNUFF
•Moist
•Dry

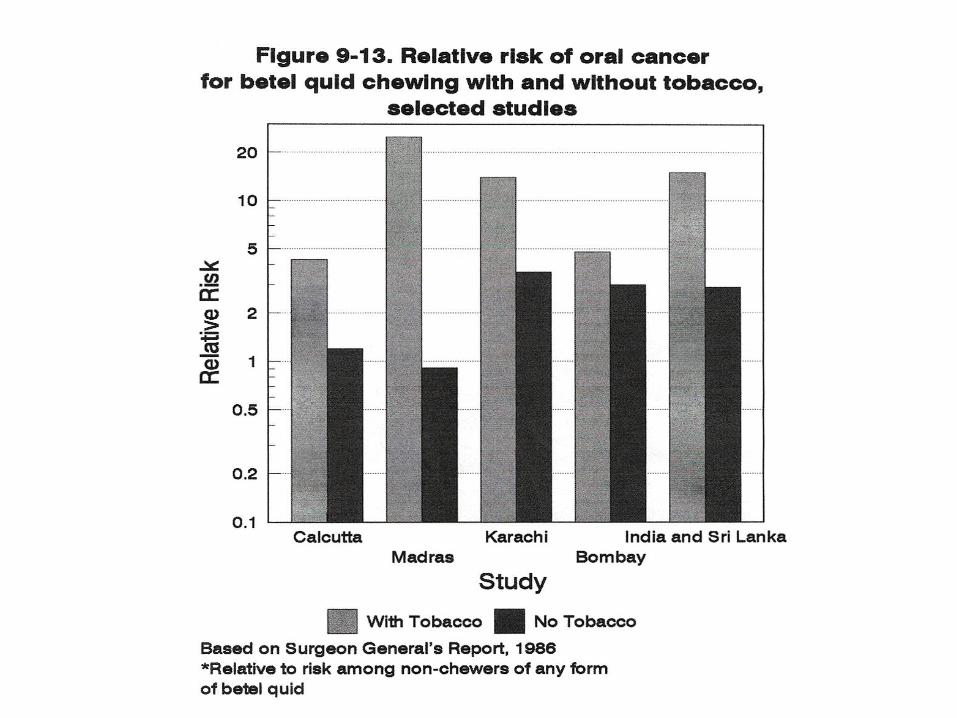
Does smokeless tobacco cause cancer?Smokeless tobacco is tobacco that is not burned. It includes chewing tobacco, dip, snuff, and betel quid*.
At least 28 chemicals in these products have been found to cause cancer, including:
• Esophageal cancer• Mouth cancer• Pancreatic cancer• Esophageal cancer• Lip cancer• Mouth cancer• Pharynx cancer• Tongue cancer
*Betel quid is a combination of betel leaf, areca nut, and slaked lime. In many countries, tobacco is added, and the product is known as gutka, ghutka, or gutkha. Like other smokeless tobacco products, betel quid and gutka are known to cause various cancers
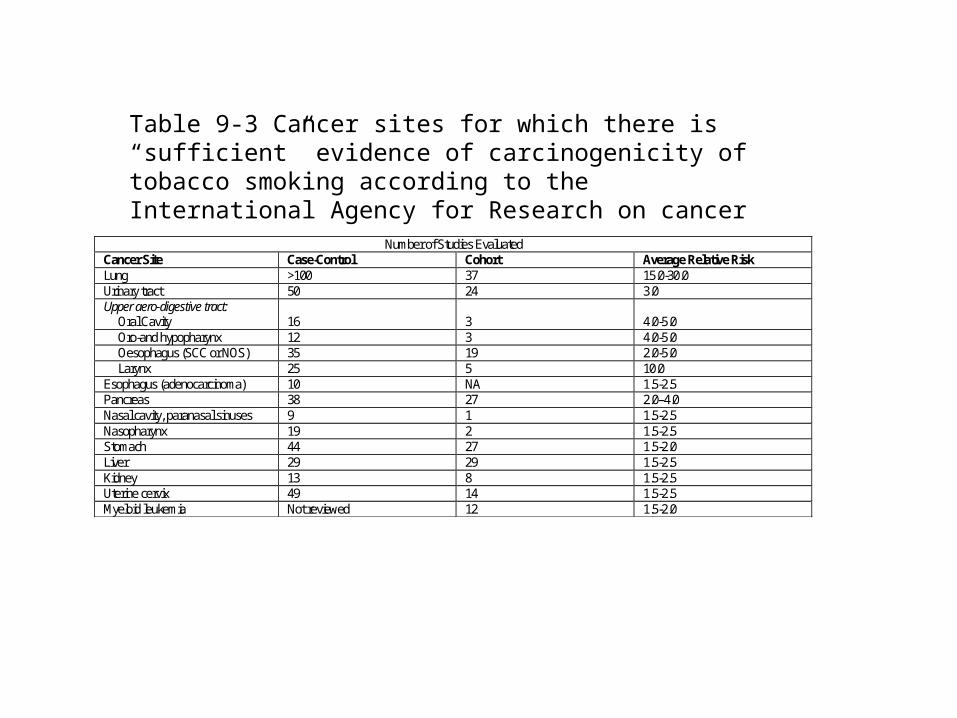
Number of Studies Evaluated
Cancer Site Case-Control Cohort Average Relative Risk Lung >100 37 15.0-30.0 Urinary tract 50 24 3.0 Upper aero-digestive tract: Oral Cavity
16
3
4.0-5.0
Oro-and hypopharynx 12 3 4.0-5.0 Oesophagus (SCC or NOS) 35 19 2.0-5.0 Larynx 25 5 10.0 Esophagus (adenocarcinoma) 10 NA 1.5-2.5 Pancreas 38 27 2.0–4.0 Nasal cavity, paranasal sinuses 9 1 1.5-2.5 Nasopharynx 19 2 1.5-2.5 Stomach 44 27 1.5-2.0 Liver 29 29 1.5-2.5 Kidney 13 8 1.5-2.5 Uterine cervix 49 14 1.5-2.5 Myeloid leukemia Not reviewed 12 1.5-2.0
Table 9-3 Cancer sites for which there is “sufficient” evidence of carcinogenicity of tobacco smoking according to the International Agency for Research on cancer
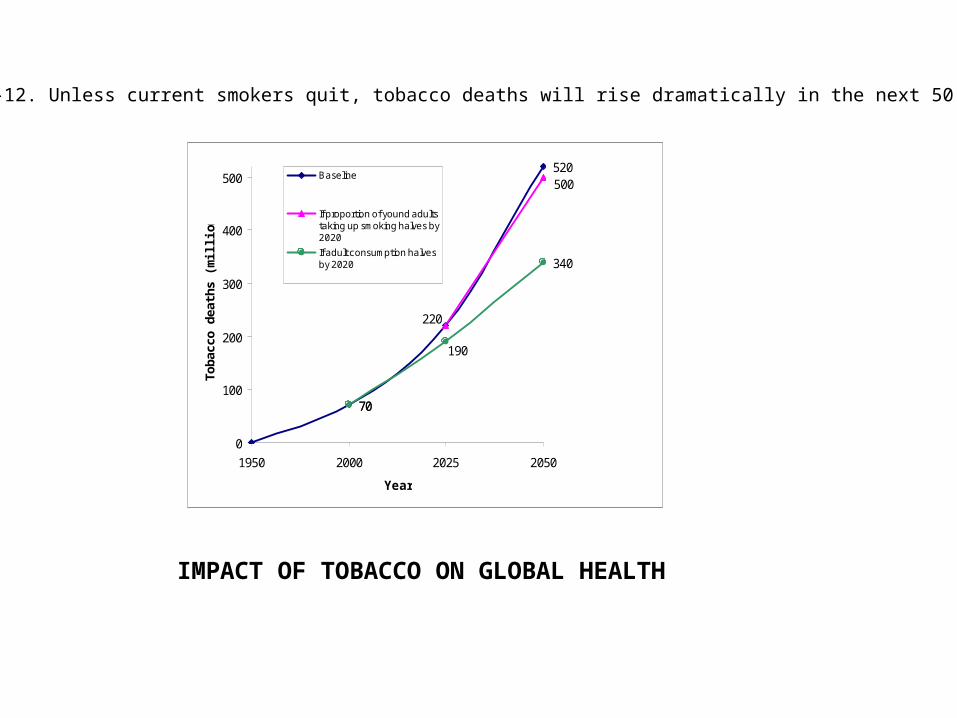
70
520
70
340
500
220
190
0
100
200
300
400
500
1950 2000 2025 2050
Year
Toba
cco
deat
hs (m
illio
n)
Baseline
If proportion of yound adultstaking up smoking halves by2020
If adult consumption halvesby 2020
Figure 9-12. Unless current smokers quit, tobacco deaths will rise dramatically in the next 50 years
IMPACT OF TOBACCO ON GLOBAL HEALTH