
TJC Infection Control Standards 2011 Supplement Resources.
113
TJC Infection Control Standards 2011 Supplement Resources
-
Upload
gerard-davidson -
Category
Documents
-
view
218 -
download
1
Transcript of TJC Infection Control Standards 2011 Supplement Resources.

TJC Infection Control Standards2011 Supplement
Resources

2
National Healthcare Safety Network (NHSN) NHSN was previously known as the National
Nosocomial Infection Surveillance System
It is a voluntary, web-based surveillance system by CDC Healthcare Quality Promotion
Goal to obtain national data on HAIs
Hospitals and ASCs may participate in the network
Available at www.cdc.gov/nhsn

3
Risk Assessment

Infection Preventionist Tools
4
www.infectionpreventiontools.com/home

5
TJC Surveyor
May look at both the infection control plan and your risk assessment 1
May look for local statistics and data, relationship with outside agencies and that you prioritized the risks
May look at your review of the last two years of interventions and program related to hand hygiene
May observe an OR cases and observe the processing of instruments in Central Supply
1 www.unc.edu/depts/spice/jcaho.html

6
Resources
TJC has Speak Up Initiatives including five things you can do to prevent infections
www.jointcommission.org/GeneralPublic/Speak+Up/about_speakup.htm
Options to Increase Isolation Surge Capacity www.jcrinc.com/common/PDFs/document_collection/
resources/collections/00032482/00032984-0001.pdf
Preparing for a Pandemic, EM Case Study, How the Health First Hospital Developed a Pandemic Influenza Plan
www.jcrinc.com/common/pdfs/qualityandsafety/preparing_for_a_pandemic_brevard_county_FL.pdf

7

8
9
www.unc.edu/depts/spice
Spice

10
TJC Crosswalk
http://www.jcrinc.com/common/pdfs/csr/forms%20and%20tools,%20newsletters/ic/CSR%20IC%20Self-Assessment%20June%20Update%20HAP%200709.doc

11

12
www.cdc.gov/nhsn/mdro_cdad.html

13

14

15

16
AORN Updated Surgical Attire
All hospitals should be aware of the updated AORN surgical attire recommended practice
Hospital must launder all scrubs
States wearing scrubs as street attire creates exposure to infectious pathogens in the community
Recommendations for safe footwear and wearing jewelry
Recommendation on cleaning of stethoscopes and ID badges
17

IV Spiking is 1 hour
IV should not spiked more than one hour before use
USP 797 requirement
APIC also has out a position paper that advices administering has soon as possible
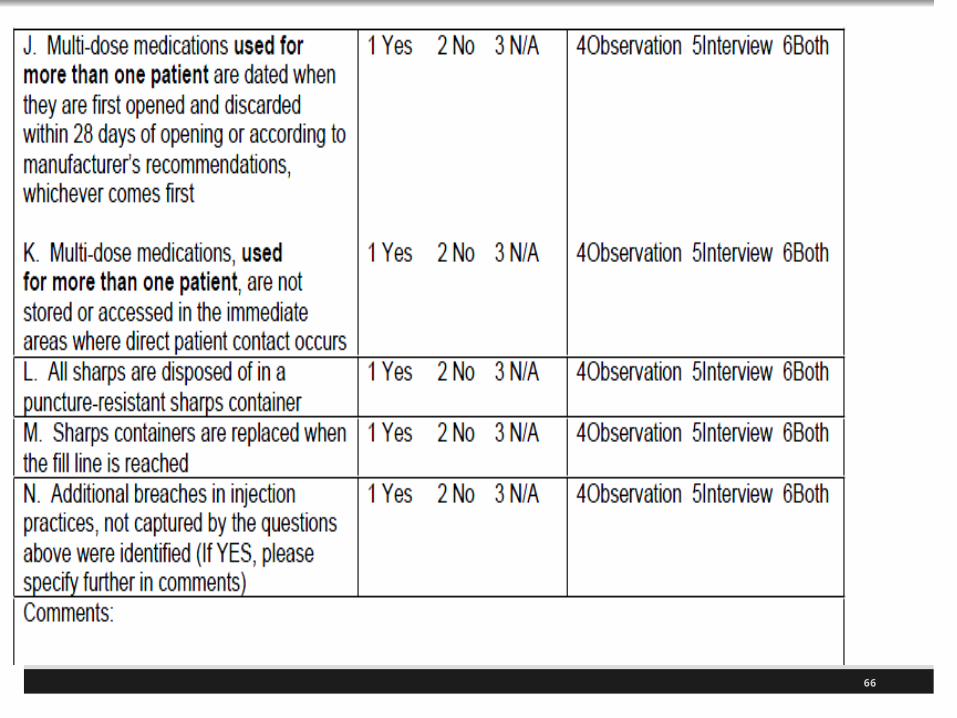
Hospitals should also have a safe injection practices policy
Hospitals should follow the 10 CDC guidelines found in the isolation standards
CMS also has an infection control sheet (15 pages) that all ASCs must complete by the surveyor
18
19

20
Reducing Surgical Site Infections
Land mark trial shows that chlorahexidine reduces surgical site infections instead of povidone-iodine
This changes the standard of care
Same edition of NEJM shows you can prevent surgical site infections by swabbing nasal site (rapid screen) and if staph aureus then decolonize
This can be done by rinse with chlorahexidine soap and use mupirocin nasal ointment
NEJM 362;18-26 January 7

21

22

Recent Issues June 2010 OSHA makes bold move to regulate
infection prevention and publishes in FR (new IC police) Issued May 6, 2010
June 2010 Environmental team at Mayo Clinic wipes out C-diff with bleach wipe program
June 2010 VA hospitals cut MRSA by 77% in ICUs with active surveillance
June 2010 SHEA and IDSA issues new C-diff guidelines
23
8 Things to Reduce Post-operative Pneumonia Researchers from VA Palo Alto Healthcare System
and Stanford University employed 8 things to reduce pneumonia on the surgery floor
1. Education of all surgical and ward nursing staff about their role in pneumonia prevention
2. Cough and deep-breathing exercises with incentive spirometer
3. Twice-daily oral hygiene with chlorhexidine swabs
4. Ambulation with good pain control24
5. Head-of-bed elevation to at least 30 degrees and sitting up for all meals ("up to eat")
6. Quarterly discussion of the progress of the program and results for nursing staff
7. Pneumonia bundle documentation in the nursing documentation
8. Computerized physician pneumonia prevention order set in the physician order entry system.
Wren SM, Martin M, Yoon JK, and Bech F. Postoperative Pneumonia-Prevention Program for the Inpatient Surgical Ward.J Am Coll Surg; April 2010, Vol. 210, Issue 4: 491-495
25
8 Things to Reduce Post-operative Pneumonia
/ 26
Institute for Healthcare Improvement

/ 27
Source: www.shea-online.org

/ 28
Source: www.his.org.uk

www.who.int/en
29
www.theific.org
30

/ 31
Source: www.idsociety.org

32

33

/ 34
PA Patient Safety Authority
Source: www.patientsafetyauthority.org/Pages/Default.aspx

35

36
/ 37
Recent cases of improperly sterilized equipment.
PA Safety Authority reports number of reported cases of contaminated equipment from prior surgery
Portland VA sent out 2,270 letters of TRUS guided prostate biopsy equipment
FDA alert July 2006 and 2009 on prostate biopsy equipment
Called bioburden
Old dried blood and tissue came out of tissue protector on drill, triple trocar full of dried blood, suture remained on tunneler, and particles of tissue found on cannulated instruments
Sterilized Equipment Issue

/ 38
Sterilized Equipment Issue (continued)
Adequate cleaning is required to remove all residual that remains, if not prevents sterilization
Many wipe instruments with wet lap or gauze sponge with sterile water during or after procedure
CMS and TJC issue information on flash sterilization so make sure you pay attention to this issue
Soaking instrument in enzymatic solution after procedure and follow manufacturers instructions Immediately soak all instruments
May need to use brushes to remove material

39
Cleaning of Medical Equipment

/ 40
MRDOs ResourcesCDC MRSA resources
www.cdc.gov/ncidod/dhqp/ar_mrsa.html
Includes fact sheet on MRSA, MRSA in healthcare setting 2007, educational material, data, lab testing and practices, etc.
Isolation precaution 2007 www.cdc.gov/ncidod/dhqp/gl_isolation.html
VRE resources www.cdc.gov/ncidod/dhqp/ ar_vre.html
Guidelines for Prevention of Surgical Site Infections
/ 41
Resources APIC resources at www.apic.org and see
standards and guidelines
Guidelines for Environmental Infection Control in Health Care Facilities
Guidelines for Prevention of Surgical-Site Infections
Recommendations for Preventing the Spread of VRE
Guidelines to Prevent Intravascular Catheter Related Infections

/ 42
/ 43
Many are on infection control
Implement best practices to prevent multiple drug resistant organisms MDROs
Educate staff and patients about MDRO and necessity for prevention
Measure MRSA and CDAD (C-diff associated disease)
Clean and disinfect equipment and patient care environment
TJC NPSGs

/ 44
IHI ICU Improvements VHA united with IHI to improve ICU care
Better control of blood sugars with glucose monitoring protocols1
Aggressive treatment of sepsis/blood stream infections (see central line bundle)
Prevention of ventilator associated pneumonia (see VAP bundle), surgical infections
Developed toolkits (order sets, protocols, daily goal sheets), report templates for monthly reporting of change
1 www.ihi.org

/ 45
Head of bed (HOB) elevation > 30 degrees
Deep venous thrombosis (DVT) prophylaxis
Peptic ulcer disease (PUD) prophylaxis
Daily sedation vacations
Assessment of readiness of wean
Oral care
Use a checklist and document each!
Ventilator Bundle

/ 46
Hand hygiene
Maximal barrier precautions upon insertion
Chlorhexidine skin antisepsis
Optimal catheter site selection with subclavian vein as the preferred site for non-tunneled catheters
Daily review of line necessity with prompt removal of unnecessary lines
Central Line Bundle

/ 47
/ 48
Over 750,000 patients a year develop sepsis or septic shock in the US
Severe sepsis will kill 30% of infected patients and another 20% will die within six months
Surviving sepsis campaign
Can listen to presentations
Sepsis bundle lists seven tasks to be done during first six hours
Sepsis Bundle

/ 49

/ 50

/ 51
If hypotension, give serum lactate >4 mmol/L (deliver initial minimum of 20 mL/kg of crystalloid and vasopressors for arterial pressure less 65 mm Hg)
Bundle 5 is for persistent hypotension achieve central venous pressure > 8mm Hg and venous oxygen sat of > 70%
Sepsis Resuscitation Bundle

/ 52
Administer low dose steroids with standardized ICU policy
Administer recombinant human activated protein C (rhAPC) in accordance with a standardized ICU policy. If not administered, document why the patient did not qualify for rhAPC.
Maintain glucose control >70, but <150 mg/dL.
Sepsis Management Bundle
/ 53
Surviving Sepsis Campaign website1
Sepsis bundle website2
Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Critical Care Medicine. 2004;32(3):858-873.
See IHI, Defeating Sepsis; 25% by 20093 1 www.survivingsepsis.org2 www.survivingsepsis.org/implement/bundles3 www.ihi.org/IHI/Topics/CriticalCare/Sepsis/ImprovementStories/
FSDefeatingSepsis25Percentby2009.htm
Sepsis Bundle

/ 54
Do not put in unless absolutely necessary
Make sure meticulous care is followed in inserting
Remove ASAP
Document everyday considerations as to whether foley can come out
Follow evidence based literature and CDC guidelines on preventing catheter associated UTI
Many UTIs can be prevented with proper management of the indwelling urethral catheter
Maintain sterile closed system CDC 2009 guidelines at
www.cdc.gov/ncidod/dhqp/dpac_uti_pc.html
Preventing UTI from Catheters
/ 55

56
Additional Resources
2011 CDC Guidelines for Prevention of Intravascular Catheter Related Infections, (pending)
CDC Guidelines for the Prevention of catheter-Induced Urinary Tract Infections, December 2009
www.cdc.gov/hicpac/cauti/002_cauti_toc.html
AHRQ toolkit
www.ahrq.gov/qual/haiflyer.htm

CA-UTI Resources
Pa Patient Safety has toolkit to prevent CA-UTIs http://patientsafetyauthority.org/EducationalTools/
PatientSafetyTools/cauti/Pages/home.aspx
APIC guidelines to eliminate catheter-associated UTI
AORN article Jan 2010 on new scip measure regarding urinary catheter removal www.aorn.org/News/Managers/November2009Issue/Catheter
57

CA-UTI Resources
IDSA as the Diagnosis, Prevention, & Treatment of Catheter-Associated Urinary Tract Infections in Adults: 2009 International Clinical Practice Guidelines from the Infectious Disease Society of America
http://cid.oxfordjournals.org/content/50/5/625.full
Iowa Healthcare Collaborative toolkit
www.ihi.org/IHI/Programs/ImprovementMap/PreventCatheterAssociatedUrinaryTractInfections.htm
58

Accreditation Connection, 6-28-2010
59

www.cdc.gov/ncidod/dhqp/dpac_uti_pc.html
60

Injection Safety CDC
61

62

63

64

65
66

67

68

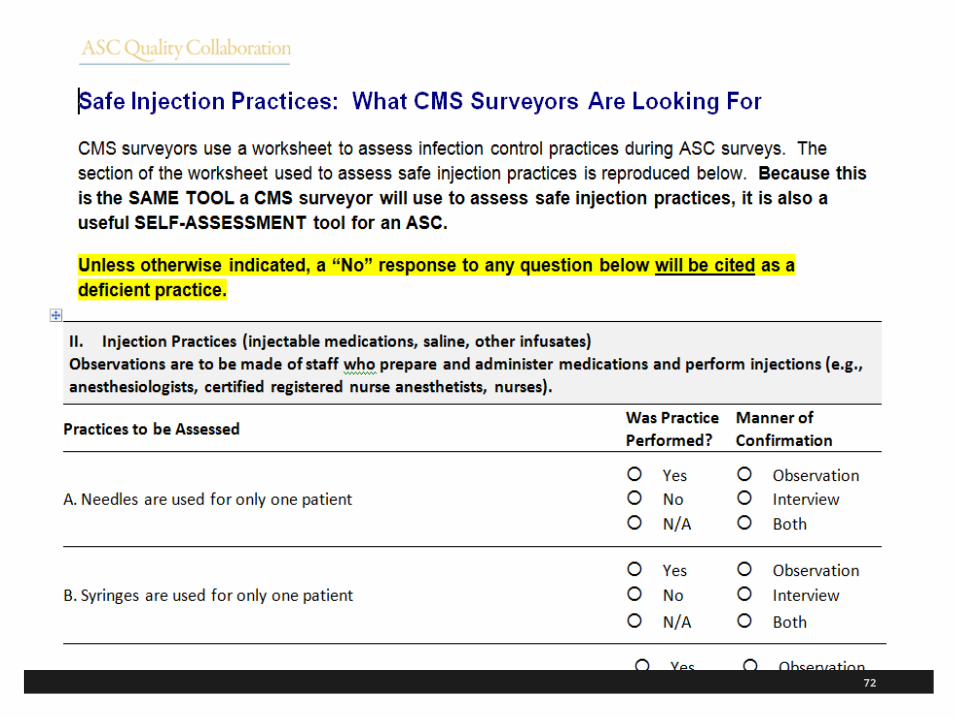
Advancing ASC Quality
ASC Quality Collaboration has ASC tool kit for infection prevention
Includes one on hand hygiene and safe injection practices
Includes a basic and expanded version of the toolkit
Available at www.ascquality.org/advancing_asc_quality.cfm
69

70

71
72

73

74

75
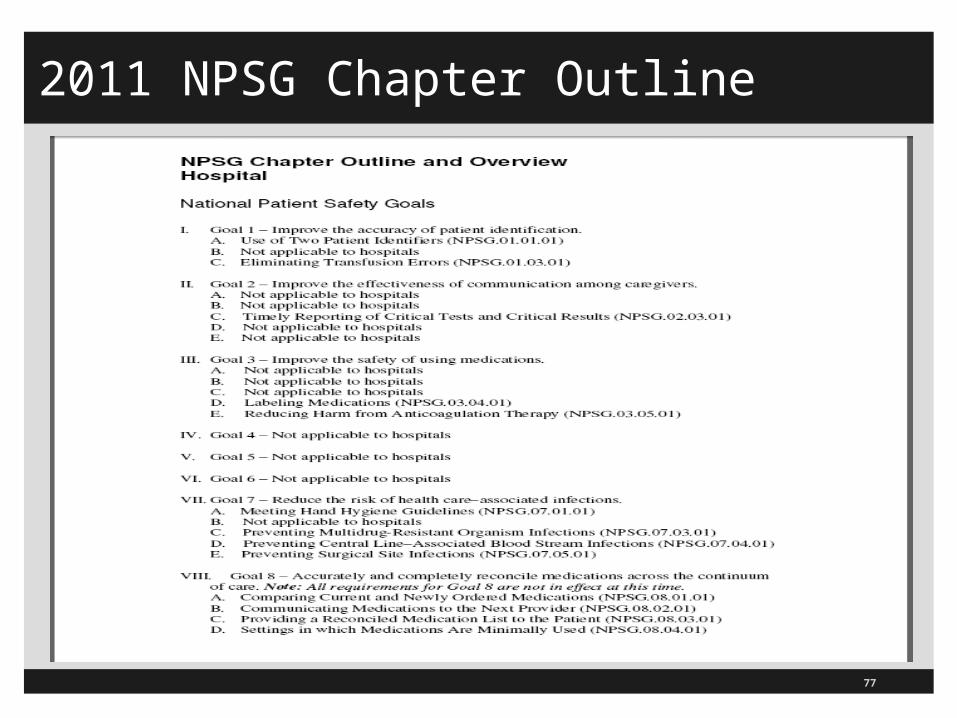
2011 NPSG Chapter Outline

Proposed for 2012 NPSG
TJC is seeking comments on NPSGs for 2012
Looking at two proposed additions
Ventilator-associated pneumonia (VAP)
–Has seven elements of performance
Catheter-associated urinary tract infections (CAUTI)
–Has four elements of performance
Comment period ended January 27, 2012
76
77
2011 NPSG Chapter Outline

78
Goal 7: Reduce the Risk of HAIGoal: Reduce the risk of HAI
4 of 5 sections remain in 2011
Deleted 7 B on HAI as a sentinel event
In August 2010 Perspective noted changes to NPSG 07.04.01 and 07.05.01
NPSG.07.04.01 EP11
Added to use an antiseptic for skin preparation during insertion of central line that is cited in the scientific literature
Removed “use chlorahexidine” even though currently the standard of care but in the event it changes

Reduce Risk of HAI InfectionsIn August 2010 Perspective changes to NPSG 07.05.01 EP7 & 8 on implementing evidenced based practices for preventing surgical site infections (SSI)
EP7 Administer antimicrobial agents for prophylaxis for a procedure or disease
Removed “evidenced based practices”
Added to do this according to methods cited in the scientific evidence or endorsed by professional organizations
Removed give antibiotics one hour before the surgery and discontinue within 24 hours or 48 for cardiothoracic patients
79

Reduce Risk of HAI Infections
EP8 Removed the section to “use clippers or depilatories” when hair is removed
Removed the note that shaving is an inappropriate hair removal method
Added to use a method that is cited in the scientific literature or endorsed by professional organizations
This is currently the standard of care
However, this new wording is flexible so if the new literature shows a new standard of care TJC does not have to go back and revise the standard
80
Reduce Risk of HAI InfectionsIn March 2010 Perspective change to NPSG.07.03.01
The word “prevention” was accidentally omitted from EP3 in the 2010 NPSG publication
Patients and families should be educated, when needed, who are colonized with MDRO about health-care associated infection prevention strategies
Retained hand hygiene, MDRO, reducing central line associated blood steam infections, and preventing surgical site infections
Good resource is the April 2010 updates to the NQF 34 Safe Practices for Better Healthcare
81
82
Hand Hygiene NPSG.07.01.01
Reduce the Risk of HAI: Comply with current CDC or WHO hand hygiene guidelines
Has 3 EPs
EP1 Implement a program that follows categories 1A, 1B, and 1C on one of the above
EP2 Set goals for improving compliance with hand hygiene guidelines
EP3 Improve compliance with hand hygiene guidelines based on established goals

83
Implement Evidenced-Based Practices Implement evidenced-based practices to prevent
HAI due to multi-drug resistant organisms (MDROs)
07.03.01 (7C)
9 EPs
Applies to, but not limited to, MRSA, VRE, C-Diff, and MDRO gram negative bacteria
Patients continue to acquire health care associated (HAI) infections at an alarming rate
Need prevention and control strategies

Increased focus on cleaning and disinfecting equipment appropriately (IC.02.02.01)
Proper use of flash sterilization
Making sure all scopes are cleaned according to the manufacturer
Cleaning the patient environment is also important
84
Implement Evidenced-Based Practices

85
Evidenced-Based HAI Prevention
1. Conduct periodic risk assessment for MDROs acquisition and transmission
In time frame set by hospital
See IC.01.03.01, EPs 1-5 that talks about identifying the risk of acquiring and transmitting infections
Following slides on this provided for reference
TJC infection control chapter very important and dovetails with these infection control NPSGs

86
Identify Risks for Transmitting Infections
IC.01.03.01 Hospital identifies risks for acquiring and transmitting infections
EP1 Hospital identifies risks based on geographic location, community, and population served
– NPSG.07.03.01 EP1 Conduct periodic risk assessments in time frames set by hospital for multidrug-resistent organisms (MDRO) acquisitions and transmission
– MDRO includes methicillin-resistant Staphylococcus Aureus (MRSA), Vancomycin-resistant Enterococcus (VRE), Klebsiella, and Acinetobacter
– CDC has free MDRO infection (and CDAD) surveillance and training on the National Healthcare Safety Network (NISN)
– 1 www.cdc.gov/nhsn/wc_MDRO_CDAD.html

87
Identify Risks for Transmitting Infections IC.01.03.01
EP2 Hospital identifies risk for acquiring and transmitting infections based on the care and treatment it provides (on MDRO)
EP3 Look at risk for acquiring or transmitting an infection by doing an analysis of surveillance activities and other infection control data (including MRDO and adverse tissue reactions)
EP4 Review and identify risks annually and when there is a significant change and get input from IP, MS, nursing, and leadership including MRDO
EP5 Prioritize these risks
88
Evidenced-Based HAI Prevention MDRO
2. Educate staff and LIPS about HAI, MDROs, and preventive strategies in orientation
At hire and annually
Use information from your risk assessment
Education must reflect their diverse roles
3. Educate patient and their families about HAI strategies who are infected or colonized with MRDO, as needed

4. Implement a MDRO surveillance program based on your risk assessment
Surveillance may be targeted rather than hospital-wide
CDC has MDRO surveillance training at www.cdc.gov/nhsn/wc_MDRO_CDAD.html
Has many resources including training videos on MDRO surveillance, slide sets, protocols, reporting plan, etc.
89
Evidenced-Based HAI Prevention MDRO

90
91

92
5. Measure and monitor MDRO prevention processes and outcomes including; MDRO infection rates using evidence based metrics, compliance with evidenced based practice, and evaluate education provided
6. Provide MRDO process and outcome data to key stakeholders, nurses, doctors, LIPs and other clinicians
7. Implement P&Ps to reduce transmission of MRDOs which meet CDC and other professional organization standards (APIC,SHEA,OSHA, AORN)
Evidenced-Based HAI Prevention MDRO

93
Evidenced-Based Practices MDRO
8. Implement a laboratory based alert system that identifies new patients with MDRO when indicated by the risk assessment
The alert system can be manual or electronic and can use faxes, pages, telephones etc.,
9. Implement an alert system that identifies readmitted or transferred MRDO positive patient when indicated by risk assessment
Alert system can be in a separate database or integrated and can manual or electronic

94
MRDOs Resources CDC Management of MRDOs in Healthcare Settings
2006, 74 pages, at www.cdc.gov/ncidod/dhqp/pdf/ar/mdroGuideline2006.pdf
Provides strategies and practices to prevent MRSA, VRE and other MDROs,
Includes gram neg bacilli (GNB), E. coli and Klebsiella pneumoniae, stenotrophomonas maltophilia, burkholderia cepacia, and ralstonia picketti

95
MRDOs Resources
CDC MRSA resources at www.cdc.gov/ncidod/dhqp/ar_mrsa.html
Includes fact sheet on MRSA, MRSA in healthcare setting 2007, educational material, data, lab testing and practices, etc.
Isolation precaution 2007 at www.cdc.gov/ncidod/dhqp/gl_isolation.html
VRE resources at www.cdc.gov/ncidod/dhqp/ar_vre.html
Guidelines for Prevention of Surgical Site Infections

96
Resources
APIC resources at www.apic.org and see standards and guidelines
Guidelines for Environmental Infection Control in Health Care Facilities
Guidelines for Prevention of Surgical Site Infections
Recommendations for Preventing the Spread of VRE
Guidelines to Prevent Intravascular Catheter Related Infections

97
Central Lines 07.04.01 (7D)
Implement best practices to prevent central line associated bloodstream infections,
13 EPs
IHI has how to guides and other resources at www.ihi.org (Keystone project)
EP1 Educate staff and LIPs involved in procedures about HAI, central line infection and importance of prevention
Must do education in orientation and annually and if procedure added to your job

Revised How-to Kit Central Lines
98

99

100
Central Lines
Note that under reform law hospitals with ICUs or NICU must report central lines infections on the CDC National Healthcare Safety Network (NHSN)
2. Educate patients and families before inserting central line about central line associated bloodstream infection prevention (BSI), as needed
3. Implement P&Ps to reduce risk of BSI that meet regulatory and evidenced based standards
Central Lines 07.04.01 P&P need to meet the regulatory requirements
Need to be aligned with the CDC requirements
And professional standards of care (APIC, AORN, SHEA, etc.)
4. Conduct periodic risk assessments for central line infection, measure BSI (blood stream infection) rate, and monitor compliance with best practices and how effective the prevention efforts are
Need to do risk assessment conducted in the time frames defined by the hospital
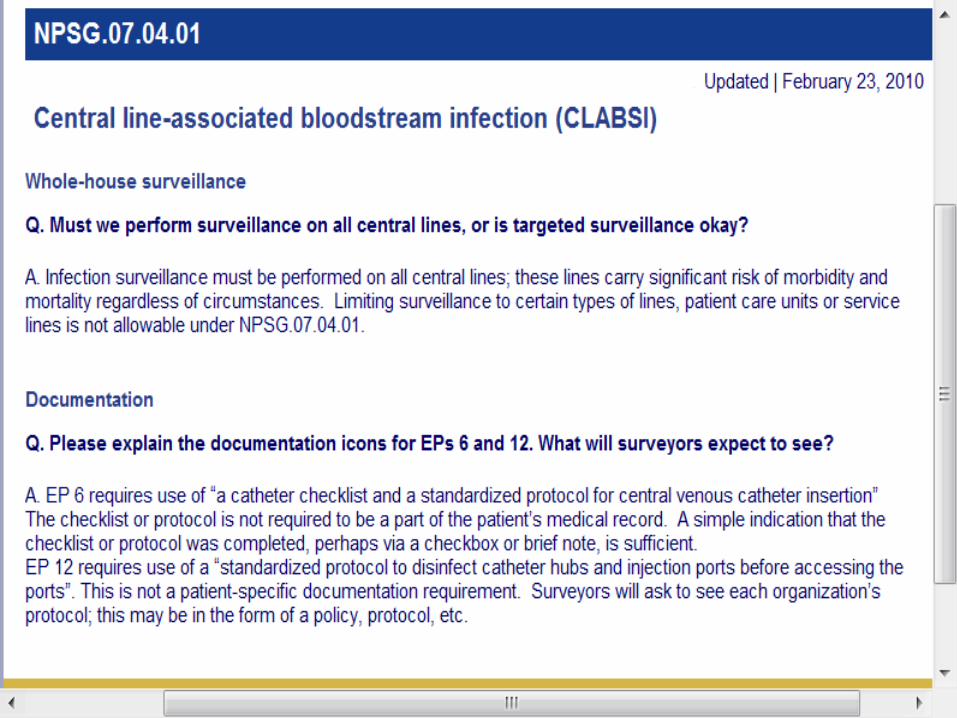
Surveillance is hospital wide and not targeted101
102
Central Lines
5. Provide CLAI (central line associated infection) rate data and prevention outcome measurement to staff and LIPs and clinicians
6. Use a catheter checklist and standard protocol for central line insertion
7. Perform hand hygiene before catheter insertion or manipulation
8. Do not put in femoral vein unless last resort for adult patients
9. Use standardized supply care or kit for central lines
103

104
Central Lines
10. Use standardized protocol for maximum sterile barrier precautions during insertion
11. Use antiseptic for skin prep in patients during insertion that is cited in the scientific literature or endorsed by professional organizations
12. Use standardized protocol to disinfect catheter hubs and injection ports before accessing
Such as wipe vigorously for 15 sections and let dry
Surveyor will ask to see the protocol or P&P
13. Evaluate all central lines routinely and remove none essential catheters

www.cdc.gov/ncidod/dhqp/dpac_uti_pc.html
105
106
Surgical Site Infections (SSI)
Implement best practices to prevent surgical site infections
There are 8 EPs
1. Educate hospital staff and LIPs involved in procedures about HAI, surgical site, and the importance of prevention
Educate during orientation, annually, and if added to your job

107
Surgical Site Infections
2. Educate patients and families, who are undergoing surgical procedures, about preventing surgical site infections (SSI)
3. Implement P&P to reduce SSI that meet regulations and evidenced based practice (such as the CDC and other professional organizations)
4. Conduct periodic risk assessments for SSI, select measures using best practices or evidence based guidelines and monitor compliance with them and how effective they are

108
Surgical Site Infections
5. Measure surgical site infection rates for the first 30 days following a procedure that does not involve inserting implantable devices
Measure for the first year procedures involving implantable devices
Need to follow evidence based guidelines
Surveillance may to targeted to certain procedures based on hospital risk assessment
6. Provide process and outcome data on SSI to stakeholders etc, such as the SS infection rate
109
Surgical Site Infections
7. Antimicrobial agents for prophylaxis are administered according to methods cited in the scientific literature or endorsed by professional organizations
Still want to be sure that prophylactic antibiotics are administered timely in the operating room and rebolused when indicated
8. When hair removal is necessary, use a method that is cited in the scientific literature or endorsed by professional organizations
www.cdc.gov/hicpac/CAUTI_fastFacts.html
110

www.cdc.gov/hicpac/Disinfection_Sterilization/acknowledg.html
111

www.cdc.gov/hicpac/pubs.html
112
113
The End Questions?
Sue Dill Calloway RN Esq. CPHRM
AD, BA, BSN, MSN, JD
Medical Legal Consultant
614 791-1468
5447 Fawnbrook Lane
Dublin, Ohio 43017















![[ njH ] [ gVd ] [ kLl ] [ TINk ] [ 'hxpI ] [ nau ] [ tJC ]](https://static.fdocuments.us/doc/165x107/56649e3f5503460f94b30286/-njh-gvd-kll-tink-hxpi-nau-tjc-.jpg)


