Title page - Einsteinapps.einstein.br/revista/arquivos/correcaotraducao/3719... · Web view2...
73
AO-3719_ VERSÃO ORIGINAL EM INGLÊS_PREPRINT FRAN Interictal abnormal fMRI activation of visual areas during a motor task cued by visual stimuli in migraine Ativação interictal anormal de áreas visuais por ressonância magnética funcional durante uma tarefa visomotora em indivíduos com enxaqueca Short title: Adriana Bastos Conforto 1 , Khallil Taverna Chaim 2 , Mario Fernando Prieto Peres 1 , André Leite Gonçalves 1 , Inara Laurindo Siqueira 1 , Maria Ângela Maramaldo Barreiros 1 , Edson Amaro Junior 2 1 Hospital Israelita Albert Einstein, São Paulo, SP, Brazil. 2 Instituto Israelita de Ensino e Pesquisa Albert Einstein, Hospital Israelita Albert Einstein, São Paulo, SP, Brazil. Corresponding author: Adriana Bastos Conforto - Avenida Albert Einstein 627/701 - Building A1 - room 403 - Morumbi - Zip code: 05652-900 - São Paulo, SP, Brazil - Phone: (55 11) 2151- 9205 - E-mail: [email protected]
Transcript of Title page - Einsteinapps.einstein.br/revista/arquivos/correcaotraducao/3719... · Web view2...

AO-3719_ VERSÃO ORIGINAL EM INGLÊS_PREPRINT FRAN
Interictal abnormal fMRI activation of visual areas during a motor task cued by
visual stimuli in migraine
Ativação interictal anormal de áreas visuais por ressonância magnética funcional
durante uma tarefa visomotora em indivíduos com enxaqueca
Short title:
Adriana Bastos Conforto1, Khallil Taverna Chaim2, Mario Fernando Prieto Peres1, André
Leite Gonçalves1, Inara Laurindo Siqueira1, Maria Ângela Maramaldo Barreiros1, Edson
Amaro Junior2
1 Hospital Israelita Albert Einstein, São Paulo, SP, Brazil.
2 Instituto Israelita de Ensino e Pesquisa Albert Einstein, Hospital Israelita Albert
Einstein, São Paulo, SP, Brazil.
Corresponding author: Adriana Bastos Conforto - Avenida Albert Einstein 627/701 -
Building A1 - room 403 - Morumbi - Zip code: 05652-900 - São Paulo, SP, Brazil -
Phone: (55 11) 2151- 9205 - E-mail: [email protected]
Received on: May 27, 2016 - Accepted on: Jan 5, 2017
Conflict of interest: none.
DOI:******

ABSTRACT
Objective: To assess changes in blood-oxygen-level-dependent activity after light
deprivation compared to regular light exposure in subjects with migraine in the interictal
state and in controls. Methods: Ten subjects with migraine and ten controls participated
in two sessions of functional magnetic resonance imaging. In each session, they
performed a finger-tapping task with the right hand, cued by visual stimuli. They were
scanned before and after 30 minutes of light deprivation or light exposure. In subjects
with migraine, functional magnetic resonance imaging was performed interictally.
Analysis of variance was made with the factors time (before or after), session (light
deprivation or exposure), and group (migraine or control). Results: There were
significant “group” effects in a cluster in the bilateral cuneus encompassing the superior
border of the calcarine sulcus and extrastriate cortex. There were no significant effects
of “time”, “session”, or interactions between these factors. Conclusion: The main result
of this study is consistent with aberrant interictal processing of visual information in
migraine. Light deprivation did not modulate functional magnetic resonance imaging
activity in subjects with or without migraine.
Keywords: Visual cortex; Migraine disorders; Brain mapping; Cerebral cortex; Light
RESUMO
Objetivo: Avaliar mudanças na atividade dependente de níveis de sangue e oxigênio
cerebral através de ressonância magnética funcional após privação luminosa,
comparada à exposição a luz, em indivíduos com enxaqueca no estado interictal e em
controles. Métodos: Dez indivíduos com enxaqueca e dez controles participaram em
duas sessões de ressonância magnética funcional. Em cada sessão, realizaram uma
adriana.conforto, 26/01/17,
Em Português, não se traduz o termo “blood-oxygen-level-dependent activity”

tarefa motora com a mão direita guiada por estímulos visuais. Foram colhidas imagens
antes e após 30 minutos de privação luminosa ou exposição a luz. Em indivíduos com
enxaqueca, a ressonância funcional foi realizada no período interictal. Foi feita a
análise de variância com fatores tempo (antes ou depois), sessão (privação ou
exposição à luz) e grupo (enxaqueca ou controle). Resultados: Houve efeitos
significativos de “grupo” em uma área no cúneo bilateral, incluindo a borda superior do
sulco calcarino e o córtex extra-estriado. Não houve efeitos significativos de “tempo”,
“sessão” ou interações entre esses fatores. Conclusão: O principal resultado deste
estudo sugere um processamento interictal anormal das informações visuais em
indivíduos com enxaqueca. A privação luminosa não modulou a atividade na
ressonância magnética funcional em indivíduos com ou sem enxaqueca.
Descritores: Córtex visual; Transtornos de enxaqueca; Mapeamento encefálico;
Córtex cerebral; Luz
INTRODUCTION
Migraine is a common neurologic condition, with a mean prevalence of 12% in adults. (1)
A widespread concept is that migraine is a disorder of the brain characterized by
paroxysmal aberrant sensory processing.(2) Abnormal visual processing in particular has
been observed in migraineurs in behavioral, neurophysiologic, and imaging studies.
The interest on the relation between migraine pathogenesis and visual function
was boosted by similarities found between migraine attacks and the cortical spreading
depression (CSD) phenomenon. Initially described in animals, CSD starts in visual
areas of the brain. A wave of neuronal depression spreads from the occipital lobe to
anterior regions and is paralleled by an initial brief decrease, followed by an increase,
and finally, a long-lasting decrease in cerebral blood flow. Similar changes in blood

flood were reported in the visual cortex during the attack in patients with migraine with
or without aura.(3,4)Importantly, there is evidence that functional changes in areas related
to visual processing are not only temporarily associated to the visual aura during a
migraine attack, but may also be observed interictally.
Between attacks, increased amplitudes and lack of habituation of visual evoked
potential responses can be observed in subjects with migraine, with or without aura. (5) In
migraine with aura, interictal transcranial magnetic stimulation (TMS) studies indicate
increased visual cortical excitability evaluated by phosphene thresholds after stimulation
of V1.(6) Decreased phosphene thresholds obtained after stimulation of V5,(7) as well as
responsiveness to transcranial direct current stimulation of V5,(8) suggest
hyperexcitability of this non-primary visual area in migraine with or without aura. Another
evidence in favor of abnormal secondary visual processing is the observation that
motion perception is impaired in migraineurs compared to controls.(9)
Furthermore, aberrant responsiveness to sensory stimuli has been documented
by decreased preactivation and lack of habituation to afferent input,(5) as well as by
discomfort elicited by visual stimuli, such as stripes or checkerboard patterns(10) in
subjects with migraine. Increased sensitivity to light in migraineurs and improvement of
migraine attacks provided by resting in a dark room are also widely known.(11)
Light deprivation (LD) can modulate the functional magnetic resonance imaging
(fMRI) hemodynamic response in the primary visual cortex when compared to light
exposure.(12) In subjects with migraine, interictal or ictal abnormalities can be captured in
primary and secondary visual areas when visual stimuli are presented in fMRI
paradigms.(13)In addition, LD may increase excitability of the primary motor cortex to
TMS in healthy subjects.(14) Whether modulation of the fMRI hemodynamic response by
LD or light exposure (LE) is also abnormal, remains to be determined.

OBJECTIVE
Our goal in this hypothesis-generating study was to preliminarily compare differences
between hemodynamic responses evaluated by functional magnetic resonance
imaging, in patients with episodic migraine in the interictal state and in controls, before
and after light deprivation or light exposure, during performance of an one-hand motor
task guided by visual instructions. We hypothesized that effects of light deprivation on
the blood-oxygenation-level dependent signal would differ in patients with migraine and
in controls.
METHODS
Subjects
Subjects with or without migraine underwent two fMRI sessions on separate days. In
one session, fMRI was performed before and after LD, while in the other session, before
and after LE. The protocol was approved by our institution´s Ethics Committee protocol
number 06/473, CAAE: 0095.0.028.000-06 and complied to the ethical standards
described in the Declaration of Helsinki. All subjects provided Informed Consent to
participate.
Subjects who wished to participate after receiving information about the protocol
from announcements published in local media, from their physicians, or from the
researchers, were evaluated by a neurologist. The inclusion criteria for subjects were
diagnosis of migraine (with aura, without aura, or chronic) made by a neurologist,
according to the International Headache Society (IHS) criteria,(15) and at least one
migraine attack in the month before the experiments. Exclusion criteria for all subjects
were: left-handedness according to the Oldfield inventory;(16) contraindications to MRI;

psychiatric conditions other than anxiety or depression; neurological conditions; use of
prophylactic migraine drugs in the previous four weeks (beta-blockers, calcium channel
blockers, antidepressants, or antiepileptic drugs); abnormal brain magnetic resonance
imaging: vascular anomalies associated with changes in brain perfusion, compression
of venous structures, areas of recent ischemia; contraindications to MRI [N.T.
informação repetida]. Potential control subjects were excluded if they had a history of
any headache during their lifetime that fulfilled criteria for a migraine attack according to
IHS criteria, any primary headache other than episodic tension-type headache, or any
headache during the month before the experiments. All patients with migraine were
women; therefore, the male sex was an exclusion criterion for controls in order to avoid
differences in sex composition between the groups.
Functional magnetic resonance imaging
Image acquisition
Functional magnetic resonance imaging was performed on a 3T MR scanner (Tim Trio,
Siemens, Germany), equipped with a 12-channel head coil. Whole-brain sagittal
structural 3D T1 MPRAGE (TR= 25 s, TE= 3.45 ms, FA 7o, 1-mm isotropic voxels) and
axial FLAIR (TR= 9000 ms, TE=81 ms, IR=2500 ms, FA 150o, matrix 256 x 239, FOV=
220 mm, slice thickness 6 mm) were performed in all subjects. Two sets of 150
functional images (EPI GRE T2* –BOLD; TR 2000 ms, TE 30 ms, FA 90o, 3.3-mm
isotropic voxels) were acquired in each subject before and after 30 minutes of LD or LE
(Figure 1).

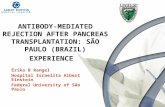
Figure 1. Experimental paradigm. In the motor paradigm cued by visual stimuli, right
hand finger tapping at 1 and 2 Hz was alternated with rest every 20s in a blocked
design. Total run time was 300 s, during which five epochs of each condition were
sampled. Subjects were instructed to remain with eyes open, fixating the center of a
screen, and to keep the right hand at rest with slight wrist flexion. Directions to oppose
each finger to the thumb following a specific order were provided visually via well-fitted
light-proof goggles. A figure of a hand was presented and subjects had to move fingers
colored in green. During the rest condition, all fingers were highlighted. In the visual
paradigm, a flickering checkerboard (frequency, 8 Hz) was presented to the left hemi-
field for 20 seconds, and to the right hemi-field for 20 seconds. A central fixation point
was then presented for 20 seconds. The order of the visuomotor paradigm and of the
visual paradigm was randomized across subjects.
REVISÃO DA FIGURA 1
adriana.conforto, 26/01/17,
Recebi um e-mail dizendo que as figuras estavam adequadas. Falta algo?
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17) Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

Image acquisition
STRUCTURAL MRI
LD or LE
Light-proof goggles were mounted on the head before starting the experiment
and were positioned on the eyes during LD. During LE, subjects were only exposed to
standard room lighting conditions (530 lux). Subjects listened to standard songs during
the 30 minutes of LD or LE, and were instructed to remain awake during the
experiment. The order of LD and LE sessions was randomized and counterbalanced
across subjects.
Visual stimuli were presented binocularly via goggles (NNL, Norway) with a
dedicated algorithm (E-prime, Psylab, USA), synchronizing image acquisition with
stimulus presentation. In order to minimize head movement, headbands were used. All
subjects trained the motor task for up to twenty minutes before entering the scanner.
Paradigm
In the motor paradigm guided by visual stimuli, right hand finger tapping at 1 and 2 Hz
was alternated with rest at every 20 s in a blocked design (Figure 1). Total run time was
300 s, during which five epochs of each condition were sampled. Subjects were
instructed to remain with eyes open, fixating the center of a screen, and to keep the
right hand at rest with slight wrist flexion. Directions to oppose each finger to the thumb,
following a specific order, were provided visually via well-fitted light-proof goggles. A
figure of a hand was presented in white (encompassing 10.6°/7.2° of the visual field –
corresponding to 90/61% of the foveal field; 100% contrast with the background) and
subjects had to move fingers colored in green (Figure 1). On average, each finger was

projected in 2.7°/1.3° of the visual field – corresponding to 23/11% of the foveal field;
53% contrast against the background in the foveal region.
The finger that should touch the thumb was highlighted at frequencies of 1 and
2 Hz. During the rest condition, all fingers were highlighted, alternating the right and
left hand representations (right/left hand visual field difference was 11.9/6.5; 94%
contrast against the background in the foveal region). We will show results obtained
during finger-tapping at 2 Hz, compared to rest; 1 Hz, compared to rest.
In addition, blocks of visual stimuli were presented before and after light
deprivation. Visual stimuli consisted of a checkerboard pattern at a frequency of 8 Hz,
presented to the left hemifield for 20 seconds, to the right hemifield for 20 seconds, and
to a central fixation point for 20 seconds. These conditions were randomized across
subjects. The order of presentation of visual and visuomotor stimuli was also
randomized.
Image analysis
Image processing and data analysis were performed using the FMRIB software library
package FSL (Analysis group, FMRIB, Oxford, UK, http://www.fmrib.ox.ac.uk/fsl/ ).
Standard pre-processing was done with Motion Correction FMRIB's Linear Image
Registration Tool (MCFLIRT) – slice time correction/motion correction, Brain Extraction
Tool (BET) – brain extraction, time-series pre-whitening, registration and spatial
normalization to the Montreal Neurological Institute (MNI) high-resolution 152-T1 2mm
template. Images were resampled into this space with 2-mm isotropic voxels. A
smoothed filter was applied with a Gaussian kernel of full-width at half-maximum
(FWHM=5 mm) to minimize noise and residual differences in gyral anatomy. A high-
pass filter (40 sec) was used to remove high frequency noise. Statistical inferences

were based on the theory of random Gaussian fields, and changes relative to the
paradigms were modeled by convolution of single trial epochs with the canonical
Hemodynamic Response Function to approximate the activation patterns with the
FMRIB’s improved linear model (FILM). Using multiple regression analysis, statistical
maps representing the association between the observed time series (e.g., BOLD
signal) and a linear combination of regressors for each subject were constructed.
Results of the motor paradigm will be presented in this manuscript. Results of the
visual paradigm will be present elsewhere.
Group analysis was performed using the higher level FEAT analysis tool to yield
statistical parameter maps (SPMs) in which all subsequent analyses were performed.
ANOVA analysis with factors TIME (before or after), SESSION (LD or LE), and GROUP
(patients with migraine or controls) was implemented using the Design Matrix feature
with the contrasts finger-tapping and rest, and SPMs were thresholded on a voxel-wise
basis at Z=2.3, and a (corrected) cluster significance threshold of p=0.05. The
maximum change in BOLD signal was collected in the “local maxima” of areas in which
significant effects or interactions were identified in the ANOVA, for post-hoc analysis.
MRI3DXv. 7.63 –was used for visual analysis and 3D rendering.
Because this was a hypothesis-generating study, the sample size was not
formally determined. Results of this study may be used to plan larger studies in the
future.
RESULTS
Subjects
Twenty women participated in the study: 10 subjects with migraine (mean age
±standard deviation, 34.8±7.7 years) and 10 controls (33.9±12.8 years). All subjects

were right-handed. Oldfield Inventory scores for patients ranged from 58 to 100, and for
controls, from 50 to 100.
Six patients had migraine without aura, and four, with aura. Migraine history
averaged (±standard deviation) 20.6±9.4 years, and the mean number of days with pain
was 10.4 ±9.4 per month. Median MIDAS (Migraine Disability Assessment Score) was
33.5 (1-80). MIDAS scores higher than 20 indicate severe disability. The average
intervals between the last migraine attack and fMRI sessions were 6.15.1 days (light
exposure session) and 8.67.4 days (light deprivation session).
Functional magnetic resonance imaging
Table 1 and Figure 2 show significant ANOVARM effects or interactions at 2 Hz and 1 Hz.
There were significant “Group” effects in a cluster in the bilateral cuneus encompassing
the superior border of the calcarine sulcus (V1, BA 17) and extra-striate cortex (V2, BA
18). There were no significant effects of “Time”, “Session”, or interactions between
these factors. Figure 3 shows the results of post-hoc analysis.
Table 1. Summary of the significant effects in functional magnetic resonance
imaging activation for the motor paradigm, at finger-tapping frequencies of 1Hz and
2Hz. Areas, Z scores, volumes (in mm3), and coordinates of the local maximal of
activation are shown.
Francislaine Soriani, 01/26/17,
Simbolo caiu
Francislaine Soriani, 01/26/17,
Símbolo caiu

Condition Area (Side) Z score mm3 x y z
Group effect
1 Hz Lingual gyrus (L) 4.17 5372-14 -92 -6
Superior temporal gyrus (R) 3.92 4210 52 -12 -8
Paracentral lobule (L) 3.76 1770 -14 -24 58
Inferior occipital gyrus (R) 3.11 729 42 -72 -8
Group effect
2 Hz Left cuneus 4.24 4006-1 -90 24


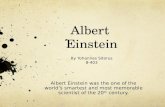
Figure 2. Brain regions with significant differences for the contrast (2 Hz finger-tapping cued by visual stimuli > rest) in subjects
with and without migraine: the cluster in the bilateral cuneus encompasses the superior border of the calcarine sulcus (V1, BA 17)
and extrastriate cortex (V2, BA 18). SPMs were thresholded on a voxel-wise basis at Z=2.3 and a (corrected) cluster significance
threshold of p=0.05
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17). Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

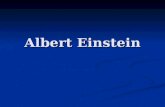
Figure 3. Variation in BOLD signal (%, contrast between finger-tapping, and rest) in patients with migraine (left) and controls (right)
before and after light exposure and light deprivation, during finger tapping at 1 Hz (A) and 2 Hz (B). Mean percentage is shown by
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17). Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

each bar. Error bar = standard deviation of the mean. Measurements were made in the local maxima of the region encompassing
the superior border of the calcarine sulcus (V1, BA 17) and extrastriate cortex (V2, BA 18). x=0 y=-90 z=24

DISCUSSION
The main finding of this study was the significant difference between migraineurs in the
interictal state and controls in fMRI activation in primary and extrastriate visual cortex
during a finger-tapping task cued by visual stimuli, compared to rest. This finding is
consistent with evidence of interictal aberrant processing of visual information in
migraineurs. Our hypothesis of differential modulation of the BOLD signal in the visual
cortex by light deprivation was not confirmed. However, due to the relatively small
sample size we cannot completely exclude this assumption.
Most interictal functional neuroimaging studies in migraine evaluated responses
to painful stimuli.(17) Our paradigm did not involve presentation of painful stimuli and our
results showed, for the first time, interictal abnormal activity in striate and extrastriate
areas in subjects with migraine during a motor task cued by visual stimuli. Enhanced
activity in another area, the peristriate visual cortex, has been reported in subjects with
migraine with aura in an fMRI block paradigm in which incongruent lines were visually
presented.(18)Also, in patients with fixed-side migraine aura, interictal fMRI showed
enhanced BOLD responses in the symptomatic hemispheres during visual stimulation.
(19)
Abnormal interictal activity in brain areas may be specific to paradigms employed
to address particular aspects of visual processing. For instance, no interictal H215O PET
changes were observed in patients with migraine in the interictal state, compared to
controls, in response to photostimulation, while increased activation was described
during attacks.(4) Photostimulation is a robust paradigm to elicit changes of the
hemodynamic response in the visual cortex, but may not capture differences in
operation of specific networks between migraineurs and controls.

We found no significant changes in fMRI activation in sensorimotor areas.
Enhanced activation of the contralateral sensorimotor cortex in subjects with migraine
without aura, compared to controls, has been reported when a hand motor paradigm is
used in a block design.(20) The specificities of the paradigm may explain this
discrepancy: Rocca et al.(20) chose a motor task consisting of 1-Hz flexion and extension
of the last four digits of the right hand, alternated with rest. In contrast with the visual
presentation of the stimulus in our paradigm, auditory cueing was applied with a
metronome to pace movement frequency, and fMRI was performed in a 1.5 T scanner.
Interictal fMRI connectivity studies point to an interictal network disorder in migraine,
rather than to dysfunction restricted to primary and secondary sensory areas.(2, 17, 21-28)
Auditory or visual cues may engage different networks, and hence have distinct abilities
to show anomalous activation in visual or sensorimotor areas, in a condition as complex
as migraine.
“Increased” or “decreased” activation of visual areas may be an oversimplification
of subtle mechanisms of deviations from normality in the brains of patients with
migraine. In the present study, the changes in activity were different in migraineurs and
controls in fMRI measurements, when performed twice within an experimental session.
Changes in activation or responsiveness over time may be a more robust endpoint for
comparisons between subjects with or without migraine, than evaluation of these
parameters at a particular point in time.
An example of different responsiveness over time in subjects with or without
migraine is the phenomenon of lack of habituation. For instance, when paired face
stimuli are presented to healthy subjects, a decrease in hemodynamic response can be
observed, compared to when a single face is shown in an event-related design.
Interictal, event-related fMRI with paired visual stimuli revealed a defective pattern of

habituation of the hemodynamic response in migraineurs,(28) in line with the previously
described absence of habituation of visual evoked responses reported in subjects with
migraine with or without aura, between attacks.(5) In addition, changes in resting motor
thresholds to TMS during a period of rest were reported over time in patients with
migraine, whereas no significant changes were observed in control subjects.(27)
Our fMRI results, obtained by using a non-painful motor paradigm cued by visual
stimuli, support the concept of interictal abnormal visual function in migraine. It is
believed that migraine attacks are generated by changes in the brain, including
abnormal cortical excitability.(5,27) Possibly, abnormal processing in visual or other
sensory areas could lead to activation of the “pain matrix” involving the thalamus, insula,
anterior cingulate cortex, prefrontal cortex, primary and secondary sensory cortex, and
the cerebellum.
Light deprivation, when compared with light exposure, did not lead to changes in
fMRI activation in subjects with or without migraine. A duration of 60 minutes of light
deprivation increased fMRI activation of the visual cortex and decreased phosphene
thresholds measured with TMS in healthy subjects.(12) The choice of a 30-minute
duration in the present study was based on a report of increased corticomotor
excitability to TMS, after 30 minutes of light deprivation, compared to baseline.(14)
However, TMS experiments performed in parallel to the present fMRI study failed to
show changes in corticomotor excitability after 30 minutes of light deprivation relative to
baseline, when compared to changes after light exposure relative to baseline, in
migraineurs or controls.(28) Considering that rest influences baseline activity in the brain,
the 30-minute period of relative rest during light deprivation or exposure may have
exceeded possible effects of light modulation on fMRI activation or on excitability to

TMS. Thus, any differences in effects of light deprivation, when compared to light
exposure, may have been obscured.
The main limitation of this study is the sample size. It was not possible to
perform subgroup analysis in order to address possible differences in results between
patients with migraine with or without aura, or whether there is a correlation with the
frequency of attacks, extent of disability from migraine, and abnormal sensory
processing. Further studies are necessary to clarify these points and to investigate
whether the fMRI results can predict risk of headache chronification or responsiveness
to specific treatments.
CONCLUSION
Interictal abnormal function and subtle structural abnormalities in the visual cortex may
reflect plastic processes related to repeated migraine attacks, as well as associated
modifications in blood flow or metabolism. Alternatively, increased thickness or
aberrant interictal activity in cortical sensory areas may reflect a common mechanism
with a likely strong genetic component, leading to migraine and to aberrant sensory
processing. Prospective studies are necessary to determine if structural and functional
findings are already present before the first migraine attack occurs, or if they develop
after repeated attacks throughout the life span.
ACKNOWLEDGEMENTS
We would like to thank André Amorim, Lais Lois, Mariana S. Moraes, and Marta O. S.
de Freitas for patient recruitment. This project was supported by the Instituto Israelita
de Ensino e Pesquisa Albert Einstein / Arthur Goldlust [grant number 143-06].

REFERENCES
1. Stewart WF, Wood C, Reed ML, Roy J, Lipton RB; AMPP Advisory Group.
Cumulative lifetime migraine incidence in women and men. Cephalalgia.
2008;28(11):28:1170-8.
2. Niazi AK, Andelova M, Sprenger T. Is the migrainous brain normal outside of
acute attacks? Lessons learned from psychophysical, neurochemical and functional
neuroimaging studies. Expert Rev Neurother. 2013;13(9):1061-7.
3. Schwedt TJ, Dodick DW. Advanced neuroimaging of migraine. Lancet Neurol.
2009;8(6):560-8. Review.
4. Denuelle M, Boulloche N, Payoux P, Fabre N, Trotter Y, Géraud G. A PET study
of photophobia during spontaneous migraine attacks. Neurology. 2011;76(3):213-8.
5. Ambrosini A, Magis D, Schoenen J. Migraine - - clinical neurophysiology.
HandbClinNeurol. 2010;97:275-93.
6. Brigo F, Storti M, Tezzon F, Manganotti P, Nardone R. Primary visual cortex
excitability in migraine: a systematic review with meta-analysis. NeurolSci.
2013;34(6):819-30. Review.
7. Battelli L, Black KR, Wray SH. Transcranial magnetic stimulation of visual area
V5 in migraine. Neurology. 2002;58(7):1066-9.
8. Chadaide Z, Arlt S, Antal A, Nitsche MA, Lang N, Paulus W. Transcranial direct
current stimulation reveals inhibitory deficiency in migraine. Cephalalgia.
2007;27(7):833-9.
9. Antal A, Temme J, Nitsche MA, Varga ET, Lang N, Paulus W. Altered motion
perception in migraineurs: evidence for interictal cortical hyperexcitability. Cephalalgia.
2005;25(10):788-94.

10. Conforto AB, Lois LA, Amaro E, Paes AT, Ecker C, Young WB, et al. Migraine and
motion sickness independently contribute to visual discomfort. Cephalalgia.
2010;30(2):161-9.
11. Main A, Dowson A, Gross M. Photophobia and phonophobia in migraineurs
between attacks. Headache. 1997;37(8):492-5.
12. Boroojerdi B, Bushara KO, Corwell B, Immisch I, Battaglia F, Muellbacher W, et al.
Enhanced excitability of the human visual cortex induced by short-term light deprivation.
CerebCortex. 2000;10(5):529-34.
13. Bramanti P, Grugno R, Vitetta A, Marino S, Di Bella P, Nappi G. Ictal and interictal
hypoactivation of the occipital cortex in migraine with aura. A neuroimaging and
electrophysiological study. FunctNeurol.2005;20(4):169-71.
14. Leon-Sarmiento FE, Bara-Jimenez W, Wassermann EM. Visual deprivation effects
on human motor cortex excitability. NeurosciLett. 2005;389(1):17-20.
15. Headache Classification Subcommittee of the International Headache Society. The
International Classification of Headache Disorders: 2nd edition. Cephalalgia.
2014;24(Suppl 1):9-160.
16. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory.
Neuropsychologia. 1971;9(1):97-113.
17. Sprenger T, Magon S. Can functional magnetic resonance imaging at rest shed light
on the pathophysiology of migraine? Headache. 2013;53(5):723-5.
18. Vincent M, Pedra E, Mourão-Miranda J, Bramati IE, Henrique AR, Moll J. Enhanced
interictal responsiveness of the migraineous visual cortex to incongruent bar stimulation:
a functional MRI visual activation study. Cephalalgia. 2003;23(9):860-8.

19. Hougaard A, Amin FM, Hoffmann MB, Rostrup E, Larsson HB, Asghar MS, et al.
Interhemispheric differences of fMRI responses to visual stimuli in patients with side-
fixed migraine aura. Hum Brain Mapp. 2014;35(6):2714-23.
20. Rocca MA, Colombo B, Pagani E, Falini A, Codella M, Scotti G, et al. Evidence for
cortical functional changes in patients with migraine and white matter abnormalities on
conventional and diffusion tensor magnetic resonance imaging. Stroke. 2003;34(3):665-
70.
21. Colombo B, Dalla Costa G, Dalla Libera D, Comi G. From neuroimaging to clinical
setting: what have we learned from migraine pain? NeurolSci. 2012;33 Suppl 1:S95-7.
Review.
22. Cutrer FM, Smith JH. Human studies in the pathophysiology of migraine: genetics
and functional neuroimaging. Headache. 2013;53(2):401-12. Review.
23. Lakhan SE, Avramut M, Tepper SJ. Structural and functional neuroimaging in
migraine: insights from 3 decades of research. Headache. 2013;53(1):46-66. Review.
24. Mainero C, Boshyan J, Hadjikhani N. Altered functional magnetic resonance
imaging resting-state connectivity in periaqueductal gray networks in migraine. Ann
Neurol. 2011;70(5):838-45.
25. Tedeschi G, Russo A, Tessitore A. Functional neuroimaging in migraine: usefulness
for the clinical neurologist. NeurolSci. 2012;33(Suppl 1):S91-4.Review.
26. Descamps B, Vandemaele P, Reyngoudt H, Deblaere K, Leybaert L, Paemeleire K,
et al. Absence of haemodynamic refractory effects in patients with migraine without
aura: an interictal fMRI study. Cephalalgia. 2011;31(11):1220-31.
27. Maniyar FH, Goadsby PJ. Functional imaging in chronic migraine. Curr Pain
Headache Rep. 2013;17(5):333. Review.

28. Conforto AB, Moraes MS, Amaro E Jr, Young WB, Lois LA, Gonçalves AL, Peres
MF. Increased variability of motor cortical excitability to transcranial magnetic
stimulation in migraine: a new clue to an old enigma. J Headache Pain. 2012;13(1):29-
37.

AO-3719_ TRADUÇÃO PARA PORTUGUÊS
PREPRINT FRAN
Ativação interictal anormal de áreas visuais por ressonância magnética funcional
durante uma tarefa visomotora em indivíduos com enxaqueca
Interictal abnormal fMRI activation of visual areas during a motor task cued by visual
stimuli in migraine
Short title:
Adriana Bastos Conforto1, Khallil Taverna Chaim2, Mario Fernando Prieto Peres1, André
Leite Gonçalves1, Inara Laurindo Siqueira1, Maria Ângela Maramaldo Barreiros1, Edson
Amaro Junior2
1 Hospital Israelita Albert Einstein, São Paulo, SP, Brasil.
2 Instituto Israelita de Ensino e Pesquisa Albert Einstein, Hospital Israelita Albert
Einstein, São Paulo, SP, Brasil.
Autor correspondente: Adriana Bastos Conforto - Avenida Albert Einstein 627/701 -
Bloco A1 - sala 403 - Morumbi - Cep: 05652-900 - São Paulo, SP, Brasil - Telefone: (55
11) 2151- 9205 - E-mail: [email protected]
Data de submissão: 27/05/2016 – Data de aceite: 05/01/2017
Conflito de interesse: não há.
DOI:******

ABSTRACT
Objective: To assess changes in blood-oxygen-level-dependent activity after light
deprivation compared to regular light exposure in subjects with migraine in the interictal
state and in controls. Methods: Ten subjects with migraine and ten controls participated
in two sessions of functional magnetic resonance imaging. In each session, they
performed a finger-tapping task with the right hand, cued by visual stimuli. They were
scanned before and after 30 minutes of light deprivation or light exposure. In subjects
with migraine, functional magnetic resonance imaging was performed interictally.
Analysis of variance was made with the factors time (before or after), session (light
deprivation or exposure), and group (migraine or control). Results: There were
significant “group” effects in a cluster in the bilateral cuneus encompassing the superior
border of the calcarine sulcus and extrastriate cortex. There were no significant effects
of “time”, “session”, or interactions between these factors. Conclusion: The main result
of this study is consistent with aberrant interictal processing of visual information in
migraine. Light deprivation did not modulate functional magnetic resonance imaging
activity in subjects with or without migraine.
Keywords: Visual cortex; Migraine disorders; Brain mapping; Cerebral cortex; Light
RESUMO
Objetivo: Avaliar Avaliar mudanças na atividade cerebral através de ressonância
magnética funcional após privação luminosa mudanças na atividade dependente de
níveis de sangue e oxigênio após privação luminosa, comparada à exposição a luz, em
indivíduos com enxaqueca no estado interictal e em controles. Métodos: Dez
adriana.conforto, 26/01/17,
Em Português, não se traduz o termo “blood-oxygen-level-dependent activity”

indivíduos com enxaqueca e dez controles participaram em duas sessões de
ressonância magnética funcional. Em cada sessão, realizaram uma tarefa motora com
a mão direita guiada por estímulos visuais. Foram colhidas imagens antes e após 30
minutos de privação luminosa ou exposição a luz. Em indivíduos com enxaqueca, a
ressonância funcional foi realizada no período interictal. Foi feita a análise de variância
com fatores tempo (antes ou depois), sessão (privação ou exposição à luz) e grupo
(enxaqueca ou controle). Resultados: Houve efeitos significativos de “grupo” em uma
área no cúneo bilateral, incluindo a borda superior do sulco calcarino e o córtex extra-
estriado. Não houve efeitos significativos de “tempo”, “sessão” ou interações entre
esses fatores. Conclusão: O principal resultado deste estudo sugere um
processamento interictal anormal das informações visuais em indivíduos com
enxaqueca. A privação luminosa não modulou a atividade na ressonância magnética
funcional em indivíduos com ou sem enxaqueca.
Descritores: Córtex visual; Transtornos de enxaqueca; Mapeamento encefálico;
Córtex cerebral; Luz
INTRODUÇÃO
Enxaqueca é uma doença neurológica comum, com uma prevalência média de 12%
em adultos.(1) Um conceito amplamente conhecido descreve a enxaqueca como um
distúrbio do cérebro caracterizado por processamento sensorial paroxístico anormal.(2)
Especialmente Oo processamento visual anormal foi especialmente observado em
portadores de enxaqueca em estudos comportamentais, neurofisiológicos e de
imagem.
O interesse na relação entre a patogênese da enxaqueca e a função visual foi
incentivado pelas semelhanças encontradas entre as crises de enxaqueca e o

fenômeno de depressão alastrante cortical (DAC). Inicialmente descrita em animais, a
DAC começa em áreas visuais do cérebro. Uma onda de depressão neuronal se
alastra do lobo occipital para as regiões anteriores, e é acompanhada em paralelo por
uma breve diminuição inicial, seguida de um aumento, e finalmente, uma depressão
duradoura no fluxo sanguíneo cerebral. Alterações semelhantes no fluxo sanguíneo
foram relatadas no córtex visual durante a crise em pacientes com enxaqueca,
apresentando ou não aura.(3,4) É importante ressaltar que há evidências de as
alterações funcionais em áreas relacionadas ao processamento visual não estarem
apenas temporariamente associadas à aura visual durante uma crise de enxaqueca,
mas também poderem ser observadas na fase interictal.
Entre as crises, pode-se observar amplitudes aumentadas e falta de habituação
de respostas visuais com potenciais evocados em indivíduos que apresentam
enxaqueca, com ou sem aura.(5) Na migrânea enxaqueca com aura, os estudos de
estimulação magnética transcraniana (EMT) interictal indicam um aumento da
excitabilidade cortical visual avaliado por limiares de fosfeno após estímulo de V1.(6) Os
limiares de fosfeno diminuídos obtidos após estímulo de V5,(7) assim como a
responsividade à estimulação transcraniana por corrente contínua de V5,(8) sugerem
hiperexcitabilidade desta área visual não primária na enxaqueca, com ou sem aura.
Outra evidência que favorece um processamento visual secundário anormal é a
observação de que a percepção de movimento está comprometida em indivíduos com
enxaqueca, quando comparados aos controles.(9)
Além disso, a responsividade anormal a estímulos sensoriais foi documentada
por pré-ativação reduzida e falta de habituação aos estímulos aferentes,(5) e também
por desconforto demonstrado aos estímulos visuais, como listras ou quadriculados,(10)
em indivíduos com migrâneaenxaqueca. A sensibilidade aumentada à luz nestes
adriana.conforto, 26/01/17,
É preferível utilizar o termo “enxaqueca” e manter a consistência ao longo do artigo

pacientes e o alívio das crises propiciado pelo descanso em uma sala escura são
também são bem conhecidos.(11)
A privação luminosa (PL) pode modular a resposta hemodinâmica na
ressonância magnética funcional (RMf) no córtex visual primário quando comparado à
exposição à luz.(12) Em indivíduos com enxaqueca, as anormalidades interictais ou ictais
podem ser captadas nas áreas visuais primárias e secundárias, quando os estímulos
visuais são apresentados em paradigmas na RMf.(13) E a PL pode aumentar a
excitabilidade do córtex motor primário à EMT em indivíduos sadios.(14) Ainda não está
definido se a modulação da resposta hemodinâmica na RMf por PL ou exposição à luz
(EL) também é anormal.
OBJETIVO
Nosso objetivo inicial neste estudo de geração de hipótese foi comparar as diferenças
entre as respostas hemodinâmicas avaliadas pela ressonância magnética funcional em
pacientes com enxaqueca episódica no estado interictal, e em controles, antes e após
a privação luminosa ou exposição à luz, durante a realização de uma tarefa motora
com uma mão, guiada por instruções visuais. Levantamos a hipótese de que efeitos de
privação luminosa sobre o sinal dependente do nível de oxigênio seriam diferentes em
pacientes com migrânea enxaqueca e em controles.
MÉTODOS
Participantes
Os indivíduos com ou sem enxaqueca foram submetidos a duas sessões de RMf em
dias separados. Em uma sessão, a RMf foi feita antes e depois da PL, enquanto na
outra sessão, antes e depois da EL. O protocolo foi aprovado pelo Comitê de Ética de

nossa instituição, com protocolo número 06/473, CAAE: 0095.0.028.000-06, e estava
foi conduzido em conformidade conforme com os padrões éticos descritos na
Declaração de Helsinque. Todos os indivíduos forneceram seu Termo de
Consentimento Livre e Esclarecido para participar.
Indivíduos que desejavam participar após receber informações - de seus
médicos, ou dos investigadores - sobre o protocolo de anúncios publicados na mídia
local, foram avaliados por um neurologista. Os critérios de inclusão dos indivíduos
foram diagnóstico de enxaqueca (com aura, sem aura, ou crônica) feito por um
neurologista, segundo os critérios do International Headache Society (IHS),(15) e pelo
menos uma crise de migrânea enxaqueca no mês anterior aos experimentos. Os
critérios de exclusão para todos os indivíduos foram: ser canhoto, de acordo com o
inventário de Oldfield;(16) contraindicações à realização da RM; doenças psiquiátricas
diferentes de ansiedade ou depressão; doenças neurológicas; uso de drogas
profiláticas contra enxaqueca nas quatro semanas anteriores (betabloqueadores,
bloqueadores de canais de cálcio, antidepressivos ou antiepiléticos); ressonância
magnética cerebral anormal: anormalidades vasculares associadas a alterações na
perfusão cerebral, compressão de estruturas venosas, áreas de isquemia recente;
contraindicações à RM [N.T. informação repetida]. Os potenciais indivíduos controle
foram excluídos quando tinham história de qualquer cefaleia durante a vida que
atendesse aos critérios de uma crise de migrâneaenxaqueca, conforme os critérios
IHS, qualquer cefaleia primária diferente da cefaleia tensional episódica, ou qualquer
cefaleia durante o mês anterior aos experimentos. Todos os pacientes com enxaqueca
eram mulheres; assim, o sexo masculino foi um critério de exclusão para os controles,
de modo a evitar diferenças na composição dos grupos em relação ao sexo.

Ressonância magnética funcional
Aquisição de imagens
Ressonância magnética funcional foi realizada em um scanner 3T MR (Tim Trio,
Siemens, Alemanha), equipado com uma bobina de 12 canais. Foram feitas imagens
3D T1 MPRAGE estruturais sagitais do cérebro inteiro (TR= 25 s, TE= 3.45 ms, FA 7o,
voxels isotrópicos de 1-mm) e FLAIR axial (TR= 9000 ms, TE=81 ms, IR=2500 ms, FA
150o, matriz 256 x 239, FOV= 220 mm, espessura de corte 6 mm) em todos os
indivíduos. Dois conjuntos de 150 imagens funcionais (EPI GRE T2* –BOLD; TR
2000 ms, TE 30 ms, FA 90o, voxels isotrópicos de 3.3 mm) foram obtidos em cada
indivíduo antes e após 30 minutes de PL ou EL (Figura 1).
Figura 1. Paradigma experimental. No paradigma motor sinalizado por estímulos
visuais, as batidas oponências de dedos da mão direita com 1 e 2 Hz foram alternadas
com descanso a cada 20s em um desenho em blocos. O tempo total de corrida
apresentação dos estímulos foi 300 s, durante os quais cinco épocas de cada condição
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17) Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

foram amostradas. Os indivíduos foram instruídos a permanecer com os olhos abertos,
fixando o olhar no centro de uma tela, e a manter a mão direita em repouso com leve
flexão do punho. As instruções de opor cada dedo ao polegar seguindo uma ordem
específica foram fornecidas visualmente através de óculos bem ajustados, à prova de
luz. A figura de uma mão foi apresentada e os indivíduos tinham de mover os dedos
coloridos em verde. Durante a condição de repouso, todos os dedos foram realçados.
No paradigma visual, foi apresentado um quadriculado cintilante (frequência, 8 Hz) ao
hemicampo esquerdo por 20 segundos, e ao hemicampo direito, por 20 segundos. Um
ponto central de fixação foi então apresentado por 20 segundos. A ordem do
paradigma visuomotor e do paradigma visual foi randomizada por para todos os
indivíduos.
TRADUÇÃO DA FIGURA 1
Image acquisition Aquisição de imagem
fMRI BEFORE
MOTOR VISUAL
RMf ANTES
MOTOR VISUAL
STRUCTURAL MRI
LD or LE
RM ESTRUTURAL
PL ou EL
fMRI AFTER RMf DEPOIS
Random Aleatório
Between subjects Entre participantes
fMRI acquisition / MOTOR Aquisição rmF / MOTOR
fMRI acquisition / VISUAL Aquisição rmF / VISUAL
Finger-tapping Batida Oponência de dedo
REST REPOUSO
1 or 2 HZ 1 ou 2 Hz
Visual synchronization with volunteer Sincronização visual com voluntário

REST REPOUSO
Óculos à prova de luz foram montados na cabeça antes de iniciar o experimento,
e foram posicionados nos olhos durante PL. Durante EL, os indivíduos foram apenas
expostos a condições padrão de luz ambiente (530 lux). AOs participantes ouviram
músicas selecionadas durante os 30 minutos de PL ou EL, e foram instruídoos a
permanecerem acordados durante o experimento. A ordem das sessões de PL e EL foi
randomizada e contrabalançada por todos os indivíduos.
Estímulos visuais foram apresentados de forma binocular por meio de óculos
(NNL, Noruega) com um algoritmo dedicado (E-prime, Psylab, EUA), que sincroniza a
aquisição de imagem com a apresentação de estímulo. Para poder minimizar o
movimento da cabeça, foram usadas faixas na cabeça. Todos aos participantes
treinaram a tarefa motora por até vinte minutes antes de entrar no scanner.
Paradigma
No paradigma motor guiado por estímulo visual, as batidas oponências dos dedos da
mão direita com 1 e 2 Hz foram alternadas com descanso a cada 20 s, conforme um
desenho em bloco (Figura 1). O tempo total da corridade apresentação dos estímulos
foi 300 s, durante os quais cinco épocas de cada condição foram amostradas. Os
indivíduos foram instruídos a permanecer com os olhos abertos, fixando o centro de
uma tela, e a manter a mão direita em repouso com leve flexão do punho. As
instruções para opor cada dedo ao polegar, em uma ordem específica, foram
fornecidas visualmente por meio de óculos bem ajustados, à prova de luz. A figura de

uma mão foi apresentada em branco (compreendendo 10,6°/7,2° do campo visual –
correspondendo a 90/61% do campo foveal; 100% de contraste com o fundo) e os
participantes tinham de mover os dedos coloridos em verde (Figura 1). Em média,
cada dedo foi projetado em 2,7°/1,3° do campo visual – correspondendo a 23/11% do
campo foveal; 53% de contraste contra o fundo na região foveal.
O dedo que deveria tocar o polegar foi realçado com frequências de 1 e 2 Hz.
Durante a condição de repouso, todos os dedos foram realçados, alternando as
representações das mãos direita e esquerda (a diferença de campo visual mão
direita/esquerda foi de 11,9/6,5; com 94% de contraste contra o fundo na região foveal).
Mostraremos os resultados obtidos durante as batidas oponências de dedo com 2 Hz,
comparadas ao repouso; 1 Hz, comparadas ao repouso.
Ainda foram apresentados blocos de estímulos visuais, antes e após privação
luminosa. Os estímulos visuais consistiram de um padrão quadriculado numa
frequência de 8 Hz, apresentados ao hemicampo esquerdo por 20 segundos, ao
hemicampo direito por 20 segundos, e a um ponto central de fixação por 20 segundos.
Estas condições foram randomizadas por para todos os indivíduos. A ordem de
apresentação de estímulos visuais e visuomotores também foi randomizada.
Análise de imagem
O processamento de imagens e análise de dados foi feito usando o software FMRIB
library package FSL (Analysis group, FMRIB, Oxford, Reino Unido,
http://www.fmrib.ox.ac.uk/fsl/ ). O pré-processamento padrão foi feito com o Motion
Correction FMRIB's Linear Image Registration Tool (MCFLIRT) – correção do tempo de
corte/correção de movimento, Brain Extraction Tool (BET) – extração do cérebro, pré-
branqueamento processamento do time-series, registro e normalização espacial

conforme o modelo Montreal Neurological Institute (MNI) high-resolution 152-T1 2mm
template. As imagens foram novamente amostradas nesse espaço com voxels
isotrópicos de 2 mm. Foi aplicado um filtro de atenuação com um kernel Gaussiano
com largura total no meio-máximo (FWHM=5 mm), para minimizar ruído e diferenças
residuais na anatomia giral. Um filtro passa-banda alta (40 seg) foi usado para remover
ruído de alta frequência. Inferências estatísticas se basearam na teoria de campos
Gaussianos randômicos, e alterações relativas aos paradigmas foram modelados por
convolução de épocas de teste único com a Função de Resposta Hemodinâmica para
aproximar os padrões de ativação com o modelo linear FMRIB melhorado (FILM).
Usando análise de regressão múltipla, foram construídos mapas estatísticos
representando a associação entre as séries de tempo observadas (por ex., sinal BOLD)
e uma combinação linear de regressores para cada indivíduo. Os resultados do
paradigma motor serão apresentados neste artigo. Os resultados do paradigma visual
serão apresentados em outra ocasião.
A análise de grupo foi feita através da ferramenta FEAT de nível mais elevado
para fornecer mapas de parâmetros estatísticos (SPMs), em que todas as análises
subsequentes foram realizadas. A análise ANOVA com fatores TEMPO (antes ou
após), SESSÃO (PL ou EL), e GRUPO (pacientes com enxaqueca ou controles) foi
implementada usando o aspecto do Design Matrix com os contrastes batidas
oponências de dedos e repouso, e SPMs foram os limiares em uma base de voxel a
Z=2,3, e um limiar (corrigido) de significância do cluster de p=0,05. A alteração máxima
no sinal BOLD foi coletada na “máxima local” de áreas em que efeitos significantes ou
interações foram identificadas na análise ANOVA para análise post-hoc. MRI3DXv.
7,63 – foi usado para análise visual e renderizado 3D.

Já que este foi um estudo de geração de hipótese, o tamanho da amostra não
foi determinado. Os resultados deste estudo poderão ser usados para o planejamento
de estudos maiores no futuro.
RESULTADOS
Participantes
Vinte mulheres participaram no estudo: 10 com enxaqueca (idade média ± desvio
padrão, 34,8±7,7 anos) e 10 controles (33,9±12,8 anos). Todas as participantes eram
destras. Os escores do inventário de Oldfield para as pacientes variaram de 58 a 100, e
para controles, de 50 a 100.
Seis pacientes apresentaram enxaqueca sem aura, e quatro, com aura. A
história de enxaqueca tinha, em média, (±desvio padrão) 20,6±9,4 anos, e o número
médio de dias com dor foi de 10,4 ±9,4 por mês. O escore MIDAS (Migraine Disability
Assessment Score) mediano foi de 33,5 (1-80). Escores MIDAS maiores que 20
indicam severa deficiênciaincapacidade. A média de intervalos entre a última crise de
enxaqueca e as sessões de RMf foi de 6,15,1 dias (sessão de exposição à luz) e
8,67,4 dias (sessão de privação luminosa).
Ressonância magnética funcional
A Tabela 1 e a Figura 2 mostram os efeitos ou interações ANOVARM significativos com
2 Hz e 1 Hz. Houve efeitos significativos de “Grupo” em um cluster no cúneo bilateral,
incluindo a borda superior do sulco calcarino (V1, BA 17) e córtex extra-estriado (V2,
BA 18). Não houve nenhum efeito significativo de “Tempo”, “Sessão”, ou interações
entre esses fatores. A Figura 3 mostra os resultados da análise post-hoc.
Francislaine Soriani, 26/01/17,
Simbolo caiu
Francislaine Soriani, 26/01/17,
Símbolo caiu

Tabela 1. Resumo dos efeitos significativos na ativação para o paradigma motor na
ressonância magnética funcional, nas frequências de batidas oponências de dedos
de 1 Hz e 2 Hz. São mostrados áreas, escores Z, volumes (em mm3) e coordenadas da
máxima local de ativação.

Condição Área (Lado) Escore Z mm3 x y z
Efeito de grupo
1 Hz Giro lingual (E) 4,17 5372-14 -92 -6
Giro temporal superior (D) 3,92 4210 52 -12 -8
Lóbulo paracentral (E) 3,76 1770 -14 -24 58
Giro occipital inferior (D) 3,11 729 42 -72 -8
Efeito de grupo
2 Hz Cúneo esquerdo 4,24 4006-1 -90 24


Figura 2. Regiões do cérebro com diferenças significantes para o contraste (batidas oponências de dedos com 2 Hz sinalizadas
por estímulos visuais > repouso) em participantes com e sem enxaqueca: o cluster no cúneo bilateral engloba a borda superior do
sulco calcarino (V1, BA 17) e córtex extra-estriado (V2, BA 18). SPMs foram restritas ao limiar em uma base de voxel a Z=2,3 e
um limiar (corrigido) de significância de cluster de p=0,05
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17). Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

Figura 3. Variação no sinal BOLD (%, contraste entre batidas oponências de dedo e repouso) em pacientes com enxaqueca (à
esquerda) e controles (à direita) antes e após exposição à luz e privação luminosa, durante batidas oponências de dedo com 1 Hz
Francislaine Soriani, 26-01-2017,
A imagem foi encaminhada para a Rudolf verificar se as especificações estão corretas (03/01/17). Deve ser solicitada ao autor caso não esteja com a resolução estipulada pelo pmc.

(A) e 2 Hz (B). A porcentagem média é mostrada por cada barra. Barra de erro = desvio padrão da média. As medidas foram
feitas na máxima local da região englobando a borda superior do sulco calcarino (V1, BA 17) e córtex extra-estriado (V2, BA 18).
x=0 y=-90 z=24
TRADUÇÃO DA FIGURA 3
Change in BOLD signal (%) Variação no sinal BOLD (%)
Migraine Enxaqueca
Controls Controles
LE Before EL antes
LE After EL depois
LD Before PL antes
LD After PL depois


DISCUSSÃO
O principal achado resultado neste estudo foi a diferença significativa entre
indivíduos com enxaqueca no estado interictal e controles, na ativação por RMf
no córtex visual primário e extra-estriado durante uma tarefa de batidas
oponência de dedos, sinalizada por estímulos visuais, relativo ao repouso. Este
achado é compatível com evidências de processamento interictal anormal de
informação visual naqueles que sofrem migrânea. Nossa hipótese de
modulação diferencial do sinal BOLD no córtex visual pela privação luminosa
não foi confirmada. Entretanto, em função do tamanho relativamente pequeno
da amostra, não podemos excluir por completo essa suposição.
A maioria dos estudos funcionais interictais de neuroimagem na
enxaqueca avaliou respostas a estímulos dolorosos.(17) Nosso paradigma não
envolveu apresentação de estímulos dolorosos, e nossos resultados
mostraram, pela primeira vez, atividade interictal anormal nas áreas estriada e
extra-estriada em participantes com enxaqueca, durante uma tarefa motora
sinalizada por estímulos visuais. A atividade realçada em outra área, o córtex
visual peri-estriado, já foi relatada em participantes com enxaqueca com aura
em um paradigma de bloco de RMf, em que linhas incongruentes foram
apresentadas visualmente.(18)Ademais, em pacientes com aura de enxaqueca
de lado fixo, a RMf interictal mostrou respostas BOLD realçadas aumentadas
nos hemisférios sintomáticos durante estimulação visual.(19)
A atividade interictal anormal em áreas do cérebro pode ser específica
de paradigmas empregados para enfocar aspectos particulares do
processamento visual. Por exemplo, nenhuma alteração interictal H215O PET foi

observada em pacientes com enxaqueca no estado interictal, relativo aos
controles, em resposta à fotoestimulação, enquanto ativação aumentada foi
descrita durante as crises.(4) A fotoestimulação é um paradigma robusto para
esclarecer alterações na resposta hemodinâmica no córtex visual, mas poderá
não captar diferenças na operação de redes específicas entre portadores de
enxaqueca e controles.
Não encontramos nenhuma alteração significativa de ativação RMf em
áreas sensório-motoras. A ativação realçada aumentada do córtex
contralateral sensório-motor em participantes com enxaqueca sem aura,
relativo aos controles, foi relatada quando se utilizaou um paradigma motor de
mão em um desenho em blocos.(20) As especificidades do paradigma podem
explicar essa discrepância: Rocca et al.(20) escolheram uma tarefa motora
consistindo de 1 Hz flexão e extensão dos últimos quatro dedos da mão direita,
alternados com repouso. Em contraste com a apresentação visual do estímulo
no nosso paradigma, a sinalização auditiva foi aplicada com um metrônomo
para marcar a frequência do movimento, e a RMf foi feita em um scanner de
1,5 T. Estudos de conectividade interictal com RMf apontam para um distúrbio
na rede interictal na enxaqueca, em vez de uma disfunção restrita a áreas
sensórias primária e secundária.(2, 17, 21-28) Sinalizações auditivas ou visuais
podem engajar diferentes redes, e assim, têm habilidades distintas para
mostrar ativação anômala em áreas visuais ou sensório-motoras, em uma
condição tão complexa quanto a migrâneaenxaqueca.
A ativação “aumentada” ou “diminuída” de áreas visuais pode ser um
excesso de simplificação de mecanismos sutis de desvios da normalidade nos
cérebros de pacientes com enxaqueca. No presente estudo, as alterações de

atividade foram diferentes em indivíduos com enxaqueca e controles nas
medidas de RMf, quando realizadas duas vezes dentro de uma sessão
experimental. Mudanças de ativação ou responsividade ao longo do tempo
podem ser um endpoint mais robusto do que a avaliação destes parâmetros em
um dado momento para comparações entre participantes com ou sem
enxaqueca.
Um exemplo de responsividade diferente ao longo do tempo em
participantes com ou sem enxaqueca é o fenômeno de falta de habituação.
Por exemplo, quando estímulos faciais pareados são apresentados a
participantes sadios, pode-se observar uma diminuição na resposta
hemodinâmica, em comparação com a situação quando uma única face é
mostrada em um desenho relacionado a evento. A RMf interictal relacionada a
evento com estímulo visual pareado revelou um padrão defeituoso de
habituação na resposta hemodinâmica em indivíduos com enxaqueca,(28)
compatível com a já descrita ausência de habituação de respostas evocadas,
relatadas em participantes com enxaqueca, com ou sem aura, entre as crises.(5)
Além disso, as alterações nos limiares motores em repouso na EMT durante
um período de repouso foram relatadas ao longo do tempo em pacientes com
enxaqueca, enquanto nenhuma alteração significativa foi observada em
participantes controle.(27)
Nossos resultados de RMf obtidos através de um paradigma motor não
doloroso, sinalizado por estímulos visuais, sustentam o conceito de função
visual interictal anormal na enxaqueca. Acredita-se que as crises de migrânea
enxaqueca sejam geradas por alterações no cérebro, incluindo excitabilidade
cortical anormal.(5,27) Possivelmente, o processamento anormal em áreas

visuais ou outras áreas sensoriais poderia levar à ativação da “matriz dolorosa”,
envolvendo o tálamo, ínsula, córtex cingulado anterior, córtex pré-frontal, córtex
sensorial primário e secundário, e cerebelo.
A privação luminosa, quando comparada com exposição à luz, não levou
a alterações na ativação na RMf em participantes com ou sem enxaqueca.
Uma duração de 60 minutos de privação luminosa aumentou a ativação de RMf
do córtex visual e diminuiu os limiares de fosfeno, medidos com EMT em
participantes sadios.(12) A escolha por uma duração de 30 minutos no presente
estudo se baseou em um relatório de excitabilidade corticomotora aumentada à
EMT, após 30 minutos de privação luminosa, relativo ao valor inicial.(14)
Todavia, os experimentos de EMT realizados em paralelo ao presente estudo
de RMf não mostraram alterações na excitabilidade corticomotora após 30
minutos de privação luminosa em relação ao valor inicial, quando comparadas
a alterações após exposição à luz relativa no início, em indivíduos com
enxaqueca ou controles.(28) Considerando que o repouso influencia a atividade
basal do cérebro, o período de 30 minutos de relativo repouso durante a
privação luminosa ou exposição à luz pode ter excedido possíveis efeitos de
modulação de luz sobre a ativação na RMf ou a excitabilidade à EMT. Assim,
quaisquer diferenças nos efeitos de privação luminosa, quando comparada à
exposição à luz, podem ter sido obscurecidas.
A principal limitação deste estudo é o tamanho da amostra. Não foi
possível realizar análise de subgrupo para enfocar possíveis diferenças nos
resultados entre pacientes com enxaqueca com ou sem aura, ou se há
correlação com a frequência de crises, extensão da deficiência pela
enxaqueca, e o processamento sensorial anormal. São necessários mais

estudos para esclarecer esses pontos e investigar se os resultados de RMf
podem predizer o risco de cronificação da cefaleia, ou responsividade a
tratamentos específicos.
CONCLUSÃO
A função interictal alterada e as anormalidades estruturais discretas no córtex
visual podem refletir processos plásticos relacionados a repetidas crises de
enxaqueca, além de modificações associadas no fluxo sanguíneo ou
metabolismo. De modo alternativo, a espessura aumentada ou atividade
interictal anormal em áreas sensoriais corticais podem refletir um mecanismo
comum, com um provável forte componente genético, resultando em
enxaqueca e processamento sensorial alterado. São necessários estudos
prospectivos para determinar se os achados estruturais e funcionais já estão
presentes antes da primeira crise, ou se desenvolvem após repetidas crises, ao
longo da vida.
AGRADECIMENTOS
Gostaríamos de agradecer André Amorim, Lais Lois, Mariana S. Moraes e
Marta O. S. de Freitas pelo recrutamento de pacientes. Este projeto teve o
apoio do Instituto Israelita de Ensino e Pesquisa Albert Einstein / Arthur
Goldlust [bolsa número 143-06].
REFERÊNCIAS

10. Stewart WF, Wood C, Reed ML, Roy J, Lipton RB; AMPP Advisory
Group. Cumulative lifetime migraine incidence in women and men. Cephalalgia.
2008;28(11):28:1170-8.
11. Niazi AK, Andelova M, Sprenger T. Is the migrainous brain normal
outside of acute attacks? Lessons learned from psychophysical, neurochemical
and functional neuroimaging studies. Expert Rev Neurother. 2013;13(9):1061-7.
12. Schwedt TJ, Dodick DW. Advanced neuroimaging of migraine. Lancet
Neurol. 2009;8(6):560-8. Review.
13. Denuelle M, Boulloche N, Payoux P, Fabre N, Trotter Y, Géraud G. A
PET study of photophobia during spontaneous migraine attacks. Neurology.
2011;76(3):213-8.
14. Ambrosini A, Magis D, Schoenen J. Migraine - - clinical neurophysiology.
HandbClinNeurol. 2010;97:275-93.
15. Brigo F, Storti M, Tezzon F, Manganotti P, Nardone R. Primary visual
cortex excitability in migraine: a systematic review with meta-analysis.
NeurolSci. 2013;34(6):819-30. Review.
16. Battelli L, Black KR, Wray SH. Transcranial magnetic stimulation of visual
area V5 in migraine. Neurology. 2002;58(7):1066-9.
17. Chadaide Z, Arlt S, Antal A, Nitsche MA, Lang N, Paulus W. Transcranial
direct current stimulation reveals inhibitory deficiency in migraine. Cephalalgia.
2007;27(7):833-9.
18. Antal A, Temme J, Nitsche MA, Varga ET, Lang N, Paulus W. Altered
motion perception in migraineurs: evidence for interictal cortical
hyperexcitability. Cephalalgia. 2005;25(10):788-94.

10. Conforto AB, Lois LA, Amaro E, Paes AT, Ecker C, Young WB, et al.
Migraine and motion sickness independently contribute to visual discomfort.
Cephalalgia. 2010;30(2):161-9.
11. Main A, Dowson A, Gross M. Photophobia and phonophobia in migraineurs
between attacks. Headache. 1997;37(8):492-5.
12. Boroojerdi B, Bushara KO, Corwell B, Immisch I, Battaglia F, Muellbacher
W, et al. Enhanced excitability of the human visual cortex induced by short-term
light deprivation. CerebCortex. 2000;10(5):529-34.
13. Bramanti P, Grugno R, Vitetta A, Marino S, Di Bella P, Nappi G. Ictal and
interictal hypoactivation of the occipital cortex in migraine with aura. A
neuroimaging and electrophysiological study. FunctNeurol.2005;20(4):169-71.
14. Leon-Sarmiento FE, Bara-Jimenez W, Wassermann EM. Visual deprivation
effects on human motor cortex excitability. NeurosciLett. 2005;389(1):17-20.
15. Headache Classification Subcommittee of the International Headache
Society. The International Classification of Headache Disorders: 2nd edition.
Cephalalgia. 2014;24(Suppl 1):9-160.
16. Oldfield RC. The assessment and analysis of handedness: the Edinburgh
inventory. Neuropsychologia. 1971;9(1):97-113.
17. Sprenger T, Magon S. Can functional magnetic resonance imaging at rest
shed light on the pathophysiology of migraine? Headache. 2013;53(5):723-5.
18. Vincent M, Pedra E, Mourão-Miranda J, Bramati IE, Henrique AR, Moll J.
Enhanced interictal responsiveness of the migraineous visual cortex to
incongruent bar stimulation: a functional MRI visual activation study.
Cephalalgia. 2003;23(9):860-8.

26. Hougaard A, Amin FM, Hoffmann MB, Rostrup E, Larsson HB, Asghar MS,
et al. Interhemispheric differences of fMRI responses to visual stimuli in patients
with side-fixed migraine aura. Hum Brain Mapp. 2014;35(6):2714-23.
27. Rocca MA, Colombo B, Pagani E, Falini A, Codella M, Scotti G, et al.
Evidence for cortical functional changes in patients with migraine and white
matter abnormalities on conventional and diffusion tensor magnetic resonance
imaging. Stroke. 2003;34(3):665-70.
28. Colombo B, Dalla Costa G, Dalla Libera D, Comi G. From neuroimaging to
clinical setting: what have we learned from migraine pain? NeurolSci. 2012;33
Suppl 1:S95-7. Review.
29. Cutrer FM, Smith JH. Human studies in the pathophysiology of migraine:
genetics and functional neuroimaging. Headache. 2013;53(2):401-12. Review.
30. Lakhan SE, Avramut M, Tepper SJ. Structural and functional neuroimaging
in migraine: insights from 3 decades of research. Headache. 2013;53(1):46-66.
Review.
31. Mainero C, Boshyan J, Hadjikhani N. Altered functional magnetic resonance
imaging resting-state connectivity in periaqueductal gray networks in migraine.
Ann Neurol. 2011;70(5):838-45.
32. Tedeschi G, Russo A, Tessitore A. Functional neuroimaging in migraine:
usefulness for the clinical neurologist. NeurolSci. 2012;33(Suppl 1):S91-
4.Review.
26. Descamps B, Vandemaele P, Reyngoudt H, Deblaere K, Leybaert L,
Paemeleire K, et al. Absence of haemodynamic refractory effects in patients
with migraine without aura: an interictal fMRI study. Cephalalgia.
2011;31(11):1220-31.

27. Maniyar FH, Goadsby PJ. Functional imaging in chronic migraine. Curr Pain
Headache Rep. 2013;17(5):333. Review.
28. Conforto AB, Moraes MS, Amaro E Jr, Young WB, Lois LA, Gonçalves AL,
Peres MF. Increased variability of motor cortical excitability to transcranial
magnetic stimulation in migraine: a new clue to an old enigma. J Headache
Pain. 2012;13(1):29-37.