Title of Presentation - Lieberman's...
36
Jean C. Lee Gillian Lieberman, MD Sarcoidosis Pulmonary and Extrapulmonary Manifestations Jean C. Lee, Harvard Medical School Year III Gillian Lieberman, MD May 2002
-
Upload
trinhkhanh -
Category
Documents
-
view
213 -
download
0
Transcript of Title of Presentation - Lieberman's...

Jean C. LeeGillian Lieberman, MD
Sarcoidosis Pulmonary and Extrapulmonary Manifestations
Jean C. Lee, Harvard Medical School Year IIIGillian Lieberman, MD
May 2002

2
Jean C. LeeGillian Lieberman, MD
Sarcoidosis• A multisystem granulomatous disorder of unknown etiology• Most frequently involves the lung (90%), skin (25%), and eyes (20%) but
extrapulmonary manifestations can also occur• Organs that are most commonly involved are:
– Reticuloendothelial system (40%)– MSK (15%)– Brain (10%)– Heart (5%)– GI (1%)
• Estimated prevalence 5-50 per 100,000• Disease prevalence varies geographically and tends to aggregate within
families• Most commonly presents in young adults 10-40 years old (70-90%)• Men and women affected equally• In U.S., 8 times more common in African Americans than Caucasians• African Americans suffer more severe form of the disease

3
Jean C. LeeGillian Lieberman, MD
Proposed Pathogenic Mechanism
• Widely thought that there may be multiple causes of sarcoidosis, accounting for the different patterns of disease
• Presumably, an unknown antigen initiates the disease and activates macrophages and CD4+ T cells in the lung. Cytokines further stimulate humoral and cellular immunity leading to increased Ab production and granuloma formation.

4
Jean C. LeeGillian Lieberman, MD
Anatomy and Histology
Note that sarcoidosis is an interstitial lung disease that affects the interlobular septae
From: Netter, Atlas of Human Anatomy 2nd ed. 1998
On pathologic specimen, most often see a focal, chronic inflammatory reaction formed by the accumulation of epithelial cells, monocytes, lymphocytes, macrophages, and fibroblasts
From: Burkitt, H. Wheater’s Basic Histopathology, 3rd ed. 1996
5
Jean C. LeeGillian Lieberman, MD
Clinical symptoms• In approximately half of all cases, the disease is discovered
incidentally.• Common presenting symptoms include cough, dyspnea, and chest
pain.• Occasionally, pts present with extrapulmonary symptoms. These
include:– Skin: plaque-like lesions, subcutaneous nodules– Eye: anterior uveitis (iritis), chorioretinitis, keratoconjunctivitis– Reticuloendothelial: LAN, hepatomegaly, splenomegaly– MSK: joint pain– Neurologic: focal neurologic signs – Cardiovascular: arrhythmias, pulm HTN, restrictive cardiomyopathy– GI: epigastric pain, nausea, and vomiting
• Clinical course can vary from indolent to severe with some patients having a very stable course and others developing permanent lung damage with multiple organ involvement.
• 5% total mortality

6
Jean C. LeeGillian Lieberman, MD
Diagnosis
• Diagnostic criteria:1. Compatible clinical or radiologic findings2. Histologic evidence of noncaseating granulomas3. Negative bacterial and fungal studies of tissue biopsy, sputum, or other bodily fluids
• Other useful tests:1. Pulmonary function tests- low FVC with nl FEV1/FVC, decreased DLCO 2. ACE level- 75% of patients with sarcoidosis have elevated levels3. Bronchoalveloar lavage- demonstrates increased number of CD4 T cells, decreased CD8 T cells, and increased immunoglobulins and B cells.

7
Jean C. LeeGillian Lieberman, MD
Patient Presentation* • Ms. B. is a previously healthy 43
year-old white female who presents to the Emergency Room with chief complaint of painful, red eye and blurry vision.
• An ophthalmologic exam done in the ED shows cells in the anterior chamber and small nodules on the surface of the iris (Busacca nodules).
• The DDx of granulomatous iritis (i.e. anterior uveitis)
– Sarcoidosis– Syphilis– Vogt-Koyanagi-Harada syndrome– Sympathetic ophthalmia– Multiple sclerosis– Lyme disease
– Tuberculosis– Herpes zoster– Coccidiomycosis– Brucellosis– Leprosy– Toxoplasmosis– Idiopathic
From: http://www.emedicine.com/oph/topic586.htm
* Note: Clinical presentation has been modified to improve the learning value of the case.

8
Jean C. LeeGillian Lieberman, MD
Initial Chest X-Ray
• Bilateral hilar adenopathy• Right paratracheal node
involvement• Enlarged aortopulmonary
window nodes• Parenchyma showed no
evidence of infiltrates• Pt denies all pulmonary
symptoms including SOB, cough, wheeze
BIDMC
9
Jean C. LeeGillian Lieberman, MD
Differential Diagnosis
• The DDx of mediastinal LAN– Sarcoidosis
– Lymphoma
– Tuberculosis
– Metastatic CA
Note: symmetrical LAN distinguishes sarcoid from lymphoma, mets, and other granulomatous infections. Symmetrical LAN occurs in 95% of cases of sarcoidosis.

10
Jean C. LeeGillian Lieberman, MD
Patient Presentation (cont.)
• Based on clinical history and chest X-Ray, pt was given presumed diagnosis of sarcoidosis.
• Pt was treated with steroid eye drops and recovered fully. • 7 years later, pt came to BIDMC with complaint of increasing
abdominal girth with a recent 8 lb weight gain.• Pt denied symptoms of SOB. A repeat chest X-ray was requested. • Abdominal CT was also performed to evaluate source of abdominal
discomfort.

11
Jean C. LeeGillian Lieberman, MD
Follow up CXR• Bilateral hilar
lymphadenopathy• Diffuse reticular and
nodular interstitial markings in the mid and upper lung zones
BIDMC
12
Jean C. LeeGillian Lieberman, MD
Differential Diagnosis
• The DDx of upper lobe predominant reticular nodular radiographic lesions include:– 5 S’s
• Sarcoidosis• Pneumoconiosis, esp. Silicosis• Ankylosing Spondylitis• “Atypical” Pneumocystis carinii pneumonia • Histiocytosis
– Less common:• Hypersensitivity pneumonitis, aka “Farmer’s lung”• Eosinophilic granuloma• Mycobacterial infection• Fungal infection• Collagen vascular disease

13
Jean C. LeeGillian Lieberman, MD
Abdominal CT
• Multiple low attenuation lesions
• Enlarged spleen
DDx splenic lesions• Granulomatous
disease, incl. sarcoidosis
• Abscess (septic emboli)
• Lymphoma• Metastasis
BIDMC

14
Jean C. LeeGillian Lieberman, MD
Patient Presentation (cont.)
• Bone marrow biopsy was performed and showed non-caseating granulomas, consistent with sarcoidosis.
• PPD and tests for other infectious organisms have been negative.• Pt remains stable from pulmonary perspective and she has been
followed with yearly chest X-rays to evaluate for worsening parenchymal disease.
Jean C. LeeGillian Lieberman, MD
Useful Radiographic Studies in the Evaluation of Sarcoidosis

16
Jean C. LeeGillian Lieberman, MD
Pulmonary• PA and Lateral Chest X-Ray
– Initial study of choice– Useful in diagnosis and monitoring progression of disease (Stage I to Stage
IV)• High Resolution Chest CT
– Obtained when chest X-ray is normal but high clinical suspicion of disease– More accurate in defining adenopathy, infiltrates, and architectural distortion– Can identify areas of reversible vs. irreversible lung damage
• Gallium 67 Scan– A non invasive test that can support diagnosis and assess for progression of
disease– A radioactive compound is injected IV and imaged 1-2 days later– Hypothesized that gallium concentrates in lymphocytes and macrophages and
identifies foci of inflammation– Used less often now since it is not very specific and a negative scan does not
exclude disease
Extrapulmonary• Studies dictated by extrapulmonary symptoms
– MRI/CT- brain involvement– Barium studies- GI involvement– Echo- cardiac involvement
17
Jean C. LeeGillian Lieberman, MD
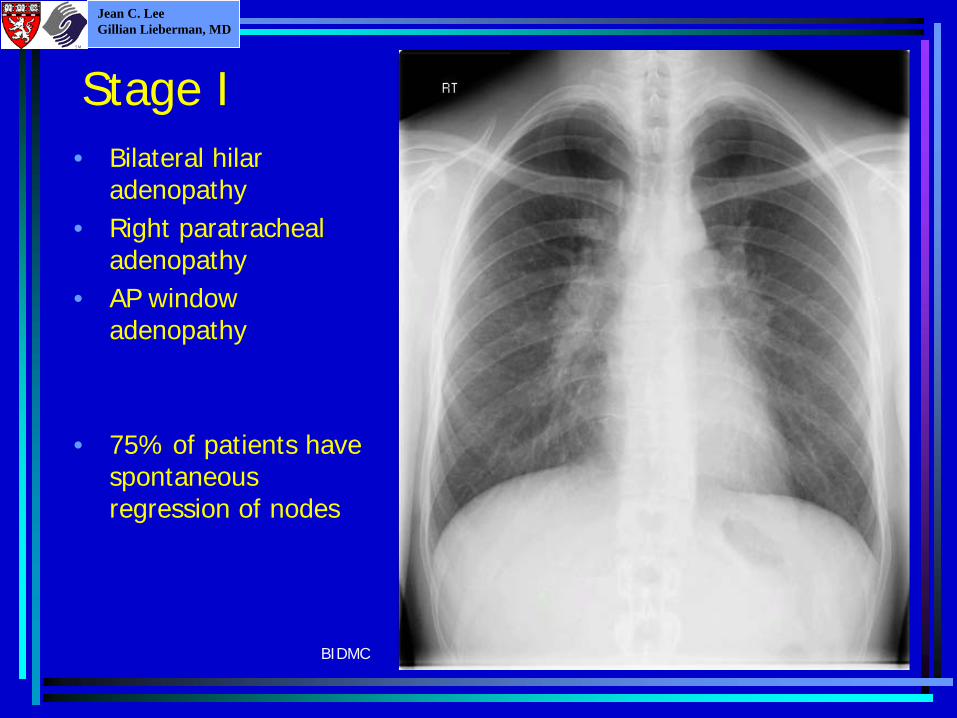
Stage I• Bilateral hilar
adenopathy• Right paratracheal
adenopathy• AP window
adenopathy
• 75% of patients have spontaneous regression of nodes
BIDMC
18
Jean C. LeeGillian Lieberman, MD
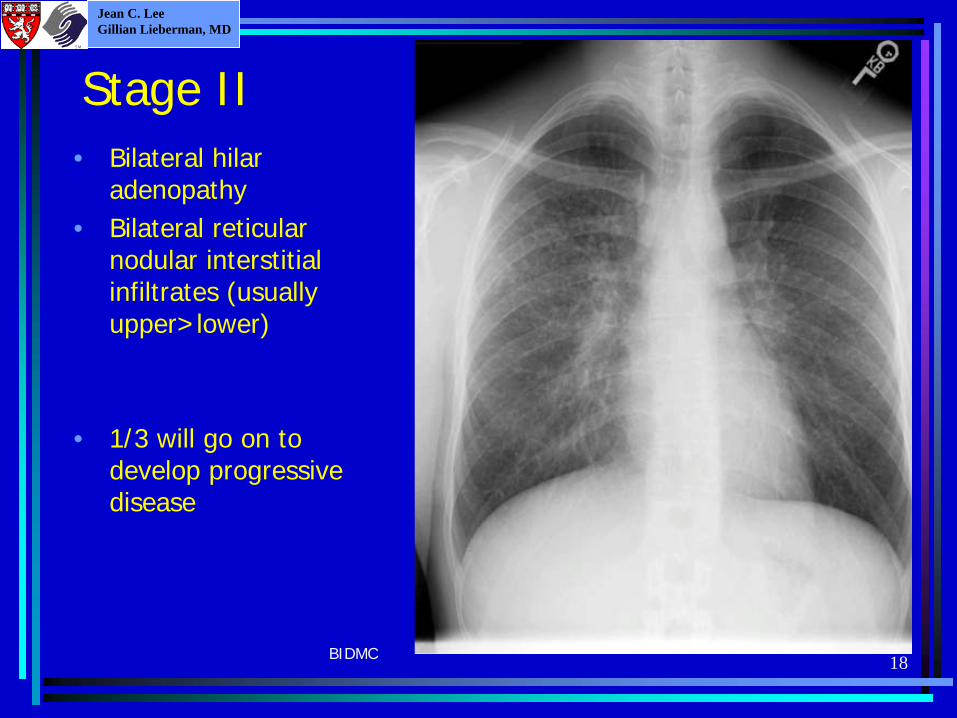
Stage II• Bilateral hilar
adenopathy• Bilateral reticular
nodular interstitial infiltrates (usually upper>lower)
• 1/3 will go on to develop progressive disease
BIDMC
19
Jean C. LeeGillian Lieberman, MD
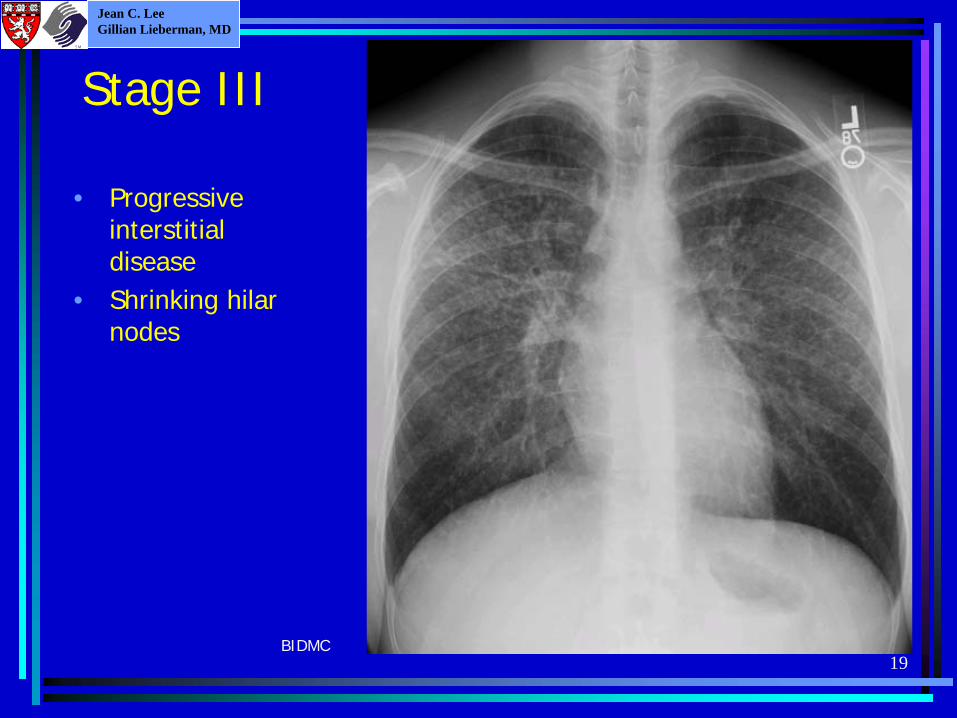
Stage III
• Progressive interstitial disease
• Shrinking hilar nodes
BIDMC

20
Jean C. LeeGillian Lieberman, MD
Stage IV
• Advanced fibrosis in reticular nodular pattern
• Cystic abnormalities• Upper lung volume
loss• Relative sparing in
lower lobes
BIDMC

21
Jean C. LeeGillian Lieberman, MD
High Res CT
• R paratracheal lymph nodes
• Subcarinal lymph nodes 4.5X2.3 cm
• Bulky hilar lymph nodes
BIDMC

22
Jean C. LeeGillian Lieberman, MD
High Res CT• Micronodules• Ground glass
opacities are suggestive of active disease
BIDMC

23
Jean C. LeeGillian Lieberman, MD
High Res CT• Diffuse
reticular opacities
• Micronodules• Conglomerate
areas of fibrosis
BIDMC

24
Jean C. LeeGillian Lieberman, MD
High Res CT• Traction
bronchiectasis causing architectural distortion
• Ground glass opacities
• Bullous changes at periphery
BIDMC

25
Jean C. LeeGillian Lieberman, MD
Gallium Scans• Radioactive isotope accumulates
in inflammatory cells, especially macrophages and lymphocytes
• Thought to correlate with areas of active disease
• “Panda sign” refers to accumulation in the parotid or lacrimal glands
• Note increased uptake in the hilar nodes
• Uptake in liver is normal and not indicative of disease
BIDMC
A P

Jean C. LeeGillian Lieberman, MD
Radiographic Findings of Extrapulmonary Sarcoidosis

27
Jean C. LeeGillian Lieberman, MD
Reticuloendothelial system (40%)
• Diffuse lymphadeno- pathy
• Splenic enlargement with granulomas
• Hepatomegaly• Large mass of lymph
tissue at the portahepatis
Ddx:• Lymphoma
BIDMC

28
Jean C. LeeGillian Lieberman, MD
Reticuloendothelial System (cont.)• Multiple hypointense
lesions in spleen following Gadolinium administration on MRI
Ddx• Lymphoma• Pyogenic abscess• Other granulomatous
infections: MAC, Histoplasmosis,etc.
• Metastasis
BIDMC

29
Jean C. LeeGillian Lieberman, MD
Cutaneous Sarcoid (25%)Subcutaneous nodules“Erythema nodosum”
Lupus pernio
From: http://www.medic.mie- u.ac.jp/derm/bilddb/bilder/cd4/img0067.htm
From: Fitzpatrick, T. “Color Atlas and Synopsis of Clinical Dermatology: Common and Serious Diseases”, 4th ed. 2000

30
Jean C. LeeGillian Lieberman, MD
Eye/Orbit (20%)• Soft tissue density L orbital lesion
extends along the lateral and superior orbit and under the posterior orbital roof
• Extraconal in location and closely associated with the lacrimal gland and extraocular muscles
Ddx:• Inflammation• Infection• Neoplasia- pleomorphic
adenoma, lymphoma
BIDMC
BIDMC

31
Jean C. LeeGillian Lieberman, MD
Musculoskeletal system (15%)• Chronic arthritis
with trabecular bone resorption
• Note “lacy destruction” of distal and middle phalanx
Ddx:• Rheumatoid
arthritis• Tuberous
sclerosis• Enchondromas• Xanthomatosis• TB• Fungal infection• Gout
From: Teaching files of Ferris Hall, MD

32
Jean C. LeeGillian Lieberman, MD
CNS disease (10%)• Multiple small foci of
hyperintensity in white matter on MRI, thought to represent vasculitis
• Note that the most common CNS lesions are localized to the meninges
Ddx:• Chronic ischemia or gliosis• CNS sarcoid• SLE• Lyme disease
BIDMC

33
Jean C. LeeGillian Lieberman, MD
GI disease (1%)• Stomach is most
frequently involved• Narrowing of antrum• Nodular mucosal
irregularitiesDdx:• Gastric CA, Lymphoma • Metastatic disease • Peptic ulcer disease • Crohn’s disease • Tuberculosis • Sarcoidosis• Syphilis • Eosinophilic gastritis • Gastritis- XRT, corrosive • Amyloidosis
From: Teaching files of Herbert Gramm, MD

34
Jean C. LeeGillian Lieberman, MD
Summary• A multisystem granulomatous disease of unknown etiology• Most common presentation in young adults with cough, dyspnea,
fatigue• Characteristically affects the lung, but can also affect the eyes,
skin, and multiple other organ systems• Diagnosis depends on:
– Characteristic clinical symptoms and radiographic findings– Ruling out infection, esp. TB– Securing histologic evidence of noncaseating granulomas
• Chest X-Rays and Chest CT are most widely used studies for evaluation of disease
• Treatment: Steroids and immunosupressives for symptomatic or extrapulmonary disease. Lung transplant with immunosupression for severe lung disease.

35
Jean C. LeeGillian Lieberman, MD
Acknowledgements• Phillip Boiselle, MD• Steven Weinberger, MD• Joseph Makris, MD • Herbert Gramm, MD• Steve Reddy, MD• Ferris Hall, MD• J. Anthony Parker, MD Ph.D.• Larry Barbaras and Cara Lyn D’amour, our Webmasters• Gillian Lieberman, MD• Pamela Lepkowski

36
Jean C. LeeGillian Lieberman, MD
References• Clark, D et al. The Radiology of Sarcoidosis. Sarcoidosis 1994; 11: 90-99.• Hommeyer, SH et al. Computed tomography in chronic interstitial lung
disease. Radiologic Clinics of North America 1991; 29(5): 1085-1093.• King, TE. “Overview of sarcoidosis” on Up to Date 2002.• “Statement on Sarcoidosis. Joint Statement of the American Thoracic
Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG)” in American Journal of Respiratory and Critical Care Medicine 1999; 160:736.
• Weinberger, Steven. Principles of Pulmonary Medicine 3rd ed. Saunders, W.B. 1998.
• Zinck, SE et al. CT of noninfectious granulomatous lung disease. Radiologic Clinics of North America 2001; 39(6): 1189-1209.