TiPs Tocris2 Asthma cs3 RESIZED · targets for asthma therapy. The table summarizes those that are...
1
Mast Cell-Directed Therapies Inhibition of mast cells is another potential asthma treatment. Mast cell activation may be inhibited by blocking IgE binding to the high-affinity IgE receptor (FcεRI), by inhibiting c-Kit, which is activated by stem cell factor (SCF), or by inhibiting Syk kinase. Mast cell stabilizers such as cromones and furosemide may work through specific ion channels for which novel modulators may be developed. Some specific targets and their inhibitors are IgE targeted by IgE antibody (Omalizumab), c-Kit targeted by Masitinib and Imatinib (approved for hematological malignancy and now explored for asthma), Syk kinase targeted by R-343 (in clinical development), and chloride ion channels targeted by cromones and furosemide. Mast cell stabilizers Lipid mediators Cyc-LTs, PGD 2 Degranulation Histamine Proteases Cytokines Cromones Furosemide Novel ion channel modulators? Anti-IgE FCεRI Sensitized mast cell Allergen IgE e.g., Omalizumab c-Kit antagonists e.g., Masitinib Blocking SCF antibody Syk kinase inhibitors e.g., R112 SCF SCF c-Kit c-Kit Syk kinase Syk kinase Lyn kinase Lyn kinase Anti-inflammatory Treatments Inhibition of signal transduction pathways that amplify inflamma- tory gene expression in asthmatic airways is another treatment option under investigation. Selective inhibitors have been developed for enzyme targets of phosphodiesterase-4 (PDE4), which degrades cAMP; inhibitor of inhibitor of NF-κB kinase (IKK2), which activates NF-κB; p38 mitogen-activated protein kinase (MAPK), which activates MAP kinase activated protein kinase 2 (MAPKAPK2); Jun kinase (JNK), which activates activator protein-1 (AP-1); and phosphoinositide-3 kinase (PI3K), which activates Akt. The table summarizes those that are currently in clinical development. INFLAMMATORY GENE EXPRESSION cAMP NF-κB MAPKAPK2 AP-1 AKT - - - - PDE4 IKK2 p38 MAPK JNK PI3Ky/δ Inflammatory stimuli - Selective inhibitors Cytokine Modulators Epithelial cells play an important role in orchestrating the inflammation of asthma through the release of multiple cytokines, including SCF (which maintains mast cells in the airways), TSLP (which acts on dendritic cells to release the Th2 chemoattractants CCL17 and CCL22, which act on CCR4), and several chemokines (particularly CCL11) that attract eosinophils by activating CCR3. Th2 cells orchestrate the inflammatory response in asthma through the release of IL-4 and IL-13 (stimulate B cells to synthesize IgE), IL-5 (necessary for eosinophilic inflammation), IL-9 (stimulates mast cell prolifera- tion), and IL-25, which further enhances cytokine release. Mast cells are thus orchestrated by several interacting cytokines and play an important role in asthma through the release of the bronchoconstrictor mediators histamine, cysteinyl-leukotrienes, and PGD 2 . Several of these cytokines (shown in purple) are now targets for asthma therapy. The table summarizes those that are currently in clinical development. Mast cell Histamine Cyc-LTs PGD 2 Broncho- constriction B-lymphocyte Target IL-4 IL-5 IL-13 CXCR2 Therapy Development status Eosinophils Inhaled allergens Dendritic cell Epithelial cells CCR3 IL-25 CCR4 TSLP Th2 cell CCL11, CCL24, CCL26, CCL5, CCL13 CCL11, CCL24, CCL26, CCL5, CCL13 CCL17, CCL22 CCL17, CCL22 SCF SCF IL-33 IL-33 IL-9 IL-9 IgE IgE IL-5 IL-5 IL-4, IL-13 IL-4, IL-13 Mutated IL-4 (pitrakinra); blocks IL-rRα and IL-13 Blocking antibody to IL-4Rα; also blocks IL-13 (AMG-317) Inhaled oligonucleotide against IL-4Rα; also blocks IL-13 (AIR645) Humanized blocking IL-5 antibody (mepolizumab) IL-5α receptor monoclonal antibody (MEDI-563) Blocking IL-13 monoclonal antibody (CAT-354 and others) Small-molecule antagonists (SCH527123) Reduced allergen responses in asthma; in clinical trials Clinical development Effective in allergen challenge; in clinical development Effective in severe asthma with sputum eosinophilia and exacerbations; in clinical trials Effective in phase II studies; in clinical trials Clinical studies in severe asthmas so far negative Phase II studies; for severe asthma Target Phosphodiesterase-4 p38 MAP kinase Inhibitor of NF-κ B kinase-2 Phosphoinositide-3 kinase Roflumilast SB236063 AS602868 CAL-101 Inhibitor (example) Development Advanced development for COPD; early clinical studies in asthma Several in early clinical development, including inhaled drugs Early clinical development δ-isoenzyme inhibitor in clincal trials for asthma Lipid Mediator Inhibitors (A) Several lipid mediators are involved in asthma. Arachidonic acid is generated from membrane lipids by cytoplasmic or secretory phospholipase A 2 (cPLA 2 , sPLA 2 ). 5 ′ Lipoxygenase (5 ′ LO) generates leukotrienes (LT), including LTB 4 , which acts on BLT 1 receptors, and cysteinyl leukotrienes (LTC 4 , LTD 4 , LTE 4 ), which act on cysLT 1 receptors and to a lesser extent on cysLT 1 receptors. Cyclooxygenases (COX1 and COX2) generate prostaglandins (PGs) and thromboxane (Tx). PGD 2 acts on DP 1 , DP 2 (also known as CRTH2), and TP receptors. Inhibitors and receptor antagonists that may be beneficial in asthma are shown in white boxes. (B) PGD 2 may play an important role in asthma. It is synthe- sized mainly in mast cells by PDGD synthase (PGDS) and acts on DP 1 receptors on vessels to mediate vasodilatation and on dendritic cells to enhance their activation. PGD 2 also acts via DP 2 receptors (CRTH2) to attract Th2 lymphocytes and eosinophils and on TP receptors to cause bronchoconstriction. Antagonists of DP 1 , DP 2 receptors, and inhibitors of PGDS are now in clinical development for asthma therapy. DP 1 antagonist CyaLT 1 antagonist CyaLT 2 antagonist BLT 1 antagonist DP 2 antagonist (CRTH2 antagonist) TP antagonist EP 1-4 CysLT 1 CysLT 2 BLT 1 TP DP 2 DP 1 Membrane phospholipids PLA 2 PGDS 5 LO COX 2 Arachidonic acid PGD 2 TxA 2 PGH 2 LTA 2 PGE 2 CysLT LTB 4 B A Mast cell Th2 cell Eosinophil Airway smooth muscle cell Dendritic cell Bronchial vessel PGDS inhibitors CRTH2 antagonist TP antagonist DP 1 antagonist DP 1 DP 1 DP 2 DP 2 TP cPLA 2 /sPLA 2 inhibitors 5 ′ LO inhibitors FLAP inhibitors New “Dissociated” Corticosteroids Development of “dissociated” steroids is based on the dissociation of the side-effect mechanisms from the anti-inflammatory mechanisms of corticosteroids. This is theoretically possible because side effects are largely mediated via transactivation and binding of glucocorticoid receptor (GR) dimers to glucocorticoid response elements (GREs) in the promoter region of target genes, resulting in gene activation. However, anti-inflammatory effects are largely mediated via transrepression of transcription factors through a nongenomic effect whereby GR monomers interact with coactivator molecules, such as NF-κB and CBP, with recruitment of histone deacetylase 2 (HDAC2). Dissociated steroids or selective glucocorticoid receptor activators (SEGRAs) have a greater effect on the transrepression than transactivation and may therefore have a better therapeutic ratio. However, some of the anti-inflammatory effects of corticosteroids may be due to transactivation of anti-inflammatory genes, such as MAP kinase phosphatase-1 (MKP-1), so SEGRAs may not be as efficacious as existing drugs. New corticosteroid options include flutica- sone furoate, characterized by longer duration of action due to a higher affinity for GR and longer receptor retention; cicleso- nide, a prodrug that is converted to the active form by esterases in the lower airways, giving reduced systemic absorption from the lungs; and AL-438 and ZK-216438, nonsteroidal SEGRAs with reduced gene activation effects in vitro, now in clinical development. Anti-inflammatory proteins (e.g., MKP-1) DNA binding trans-activation histone acetylation Side effects (metabolic, endocrine) Inflammatory proteins (cytokines, enzymes, adhesion molecules, etc.) Corticosteroids Dissociated steroid GLUCOCORTICOID RECEPTORS GRα Inhibition of transcription factors NF-κB, AP-1, etc. trans-repression histone deacetylation NF-κB GR dimer GRE GR monomer HDAC2 Bronchodilators Activation of β 2 adrenoceptors (β 2 AR), vasoactive intestinal peptide (VIP), and prostaglandin E2 (PGE 2 ) receptors results in activation of adenylyl cyclase (AC) via a stimulatory G protein (G s ) and an increase in 3 ′ -5 ′ cyclic adenosine monophosphate (cAMP). This activates protein kinase A (PKA), which then phosphorylates several target proteins, resulting in the opening of calcium-activated potassium channels (KCa ) or Maxi-K channels, decrease in phosphoinositide (PI) hydrolysis, increase in sodium/calcium ion (Na + /Ca 2+ ) exchange, increase in Na + /K + ATPase activity, and decrease in myosin light chain kinase (MLCK) activity, leading to relaxation of airway smooth muscle. β 2 AR may also be coupled directly to K Ca via G s . cAMP is degraded by phosphodiesterases (PDEs) that are inhibited by theophylline and selective PDE3 inhibitors. Current bronchodilators are inhaled β 2 AR agonists, both short acting (salbutamol, terbutaline) and long acting (formoterol, salmeterol), and theophylline. New bronchodilators are once-inhaled daily β 2 AR agonists (indacaterol, carmoterol, GW-642444, and BI-1744), once-daily anticholinergics (tiotropium, glycopyrrolate, daratropium, and aclidinium), PGE 2 , potassium channel openers, vasoactive intestinal peptide analogues (Ro 25-1553), and PDE3 inhibitors. Smooth muscle myosin inhibitors are currently in development. K + Ca 2+ channel K + channel PI/Ca 2+ ATP cAMP AMP PDE MLCK G S PKA PGD 2 AC K + channel openers β 2 Agonist VIP PGE 2 β 2 AR Theophylline PDE3 inhibitors Bronchodilatation Smooth muscle myosin inhibitors Adenosine receptors Fexofenadine Amthamine, Tiotidine Imetit, Thioperamide Histamine receptors H 1 receptor H 2 receptor H 3 receptor 4-Methylhistamine, JNJ 10191584 H 4 receptor β 2 Adrenoceptors Glucocorticoid receptors Chemokine receptors Prostanoid receptors VIP receptors Signal Transduction Signal Transduction API-2, 10-DEBC Celecoxib, SC 560 AKT COX MG 132, Celastrol, IKK 16 NF-κ B MAPK SB 239063, Anisomycin, SP 600125 740 Y-P, LY 294002 PI3K AACOCF3, YM 26734 PLA 2 PDE Cilostamide, Zardaverine, Theophylline, Rolipram Nitric Oxide N ω -Propyl-L-arginine, 1400W, L-NAME, BYK 191023 Leukotriene receptors K + channels Cytokines and cytokine receptors Compounds Acting on Asthma Pathways Available from CGS 21680, 2-CI-IB-MECA, SCH 58261, ZM 241385, MRS 1754 ICI 118,551, Salmeterol, Formoterol Corticosterone, Fluticasone RS 504393, C 021, SB 328437, UCB 35625, SB 265610 Gabexate, Thalidomide, Pirfenidone, GIT 27, YM 90709 MK 886, BAY-u 9773, MK 571, Leukotriene B 4 SC 51089, L-161,982, Prostaglandin E 2 , U 46619, MK 571 VIP (6-28), VIP Iberiotoxin, 1-EBIO Asthma is now one of the most common chronic diseases in the world, affecting over 300 million people, and its prevalence is rising, particularly in develop- ing countries. Chronic inflammation of the airways results in airway hyperresponsiveness (AHR), which makes the airways “twitchy” and causes them to constrict more easily than normal in response to different triggers, such as exercise, cold air, and exposure to allergens and irritants. The inflammation may be worsened by exposure to allergens and by upper respiratory tract virus infections, and it may activate sensory nerves of the airways, resulting in coughing and chest tightness. Asthma symptoms are intermittent and rarely progress. Patients may have differing degrees of severity, ranging from mild intermittent symptoms to severe symptoms and disability. In the past, asthma was viewed as a disease of bronchoconstriction and treated predominantly with bronchodilators. Current therapy for asthma depends on the severity of the condition and is increased in a stepwise manner until asthma control is achieved. Inhaled corticosteroids (ICS) are the mainstay of treat- ment in all patients with persistent asthma, and long-acting β 2 agonists (LABAs) are added in moderate cases. In severe asthma, other add-on therapies may be necessary, and in very severe asthma, anti-IgE and immosuppressants may be used. Additionally, combination inhalers (corticosteroid + LABA) are now commonly prescribed to control asthma since they are more convenient for patients, simplify treatments, improve compliance, and, very importantly, prevent the use of LABAs alone, which is potentially dangerous. Nonetheless, it is now clear that asthma is a complex chronic inflammatory disease of the airways with many potential therapeutic targets, and treatment of the inflammation is now considered to be the key to successful control of symptoms. There is also a real need for new asthma treatments due to poor compliance with current treatments, side effects outside the lungs for the current inhaled treatments, patients’ preference for oral therapy, difficulty in treating severe asthma, and current unavailability of disease-modifying and curative treatments. Here, the focus is placed on new asthma treatment options that are being developed as the understanding of cellular pathways involved in the disease increases. INTRODUCTION Current therapy for asthma with ICS and inhaled LABA is highly effective, safe, and relatively inexpensive, but many patients’ symptoms remain poorly controlled, and severe asthma remains difficult to control with current treatments. Some innovative strategies and cutting-edge issues in asthma research and therapy include the following: developing selective therapies for subphenotypes via yet-to-be-identified discriminatory biomarkers and genetic profiling; treating patients with severe asthma who are relatively corticosteroid resistant by restoring HDAC2 activity via low doses of theophylline; developing an effective oral therapy for patients with mild and moderate disease; and using genetic and pharmacogenomic information to improve understanding of the biology of asthma to develop treatments. None of the currently available treatments for asthma have long-term effects on airway inflammation or remodeling, and therefore they are not disease modifying or curative. The prospects for a cure seem remote until the molecular and genetic causes of asthma are better understood, but there is a possibility that vaccination approaches have the potential to reverse the abnormal inflammation found in asthma. However, the long-term consequences of these approaches need to be carefully evaluated, particularly as they would probably need to be applied in children at the onset of disease. CONCLUSION AND FUTURE DIRECTIONS Further Reading Adcock, I.M., et al. (2006). Kinase inhibitors and airway inflammation. Eur. J. Pharmacol. 533, 118–132. Adcock, I.M., et al. (2008). New targets for drug development in asthma. Lancet 372, 1073–1087. Barnes, P.J. (2006). How corticosteroids control inflammation. Br. J. Pharmacol. 148, 245–254. Barnes, P.J. (2010). New therapies for asthma: Is there any progress? Trends Pharmacol. Sci. doi:10.1016/j.tips.2010.04.009. Barnes, P.J. (2008). Cytokine networks in asthma and chronic obstructive pulmonary disease. J. Clin. Invest. 118, 3546–3556. Barnes, P.J., et al. (2009). Glucocorticoid resistance in inflamma- tory diseases. Lancet 342, 1905–1917. Broide, D.H. (2009). Immunomodulation of allergic disease. Annu. Rev. Med. 60, 279–291. Cazzola, M., et al. (2009). Emerging inhaled bronchodilators: An update. Eur. Respir. J. 34, 757–769. Chung, K.F. (2006). Phosphodiesterase inhibitors in airways disease. Eur. J. Pharmacol. 533, 110–117. Holgate, S.T., et al. (2008). Treatment strategies for allergy and asthma. Nat. Rev. Immunol. 8, 218–230. New Therapies, Challenges, and Breakthroughs in Asthma Peter J. Barnes National Heart and Lung Institute, Imperial College London School of Medicine, Dovehouse Street, London SW3 6LY, UK [email protected] To obtain copies of this poster, please visit TOCRIS at www.tocris.com
Transcript of TiPs Tocris2 Asthma cs3 RESIZED · targets for asthma therapy. The table summarizes those that are...

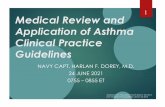
Mast Cell-Directed TherapiesInhibition of mast cells is another potential asthma treatment. Mast cell activation may be inhibited by blocking IgE binding to the high-affinity IgE receptor (FcεRI), by inhibiting c-Kit, which is activated by stem cell factor (SCF), or by inhibiting Syk kinase. Mast cell stabilizers such as cromones and furosemide may work through specific ion channels for which novel modulators may be developed. Some specific targets and their inhibitors are IgE targeted by IgE antibody (Omalizumab), c-Kit targeted by Masitinib and Imatinib (approved for hematological malignancy and now explored for asthma), Syk kinase targeted by R-343 (in clinical development), and chloride ion channels targeted by cromones and furosemide.
Mast cell stabilizers
Lipid mediatorsCyc-LTs, PGD2
DegranulationHistamineProteases
Cytokines
CromonesFurosemideNovel ion channelmodulators?
Anti-IgE
FCεRI
Sensitizedmast cell
AllergenIgE
e.g., Omalizumab
c-Kit antagonistse.g., Masitinib
Blocking SCFantibody
Syk kinaseinhibitorse.g., R112
SCFSCF
c-Kitc-Kit
Syk kinaseSyk kinase
Lyn kinaseLyn kinase
Anti-inflammatory TreatmentsInhibition of signal transduction pathways that amplify inflamma-tory gene expression in asthmatic airways is another treatment option under investigation. Selective inhibitors have been developed for enzyme targets of phosphodiesterase-4 (PDE4), which degrades cAMP; inhibitor of inhibitor of NF-κB kinase (IKK2), which activates NF-κB; p38 mitogen-activated protein kinase (MAPK), which activates MAP kinase activated protein kinase 2 (MAPKAPK2); Jun kinase (JNK), which activates activator protein-1 (AP-1); and phosphoinositide-3 kinase (PI3K), which activates Akt. The table summarizes those that are currently in clinical development.
INFLAMMATORY GENE EXPRESSION
cAMP NF-κB MAPKAPK2 AP-1 AKT
-
-
-
-
PDE4 IKK2 p38 MAPK JNK PI3Ky/δ
Inflammatory stimuli
-
Selectiveinhibitors
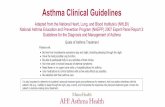
Cytokine ModulatorsEpithelial cells play an important role in orchestrating the inflammation of asthma through the release of multiple cytokines, including SCF (which maintains mast cells in the airways), TSLP (which acts on dendritic cells to release the Th2 chemoattractants CCL17 and CCL22, which act on CCR4), and several chemokines (particularly CCL11) that attract eosinophils by activating CCR3. Th2 cells orchestrate the inflammatory response in asthma through the release of IL-4 and IL-13 (stimulate B cells to synthesize IgE), IL-5 (necessary for eosinophilic inflammation), IL-9 (stimulates mast cell prolifera-tion), and IL-25, which further enhances cytokine release. Mast cells are thus orchestrated by several interacting cytokines and play an important role in asthma through the release of the bronchoconstrictor mediators histamine, cysteinyl-leukotrienes, and PGD2. Several of these cytokines (shown in purple) are now targets for asthma therapy. The table summarizes those that are currently in clinical development.
Mast cell
HistamineCyc-LTsPGD2
Broncho-constriction
B-lymphocyte
Target
IL-4
IL-5
IL-13
CXCR2
Therapy Development status
Eosinophils
Inhaled allergens
Dendritic cell
Epithelialcells
CCR3IL-25
CCR4
TSLP
Th2 cell
CCL11, CCL24,CCL26, CCL5,
CCL13
CCL11, CCL24,CCL26, CCL5,
CCL13
CCL17, CCL22CCL17, CCL22
SCFSCFIL-33IL-33
IL-9IL-9
IgEIgE
IL-5IL-5IL-4,IL-13IL-4,IL-13
Mutated IL-4 (pitrakinra); blocks IL-rRα and IL-13
Blocking antibody to IL-4Rα; also blocks IL-13 (AMG-317)
Inhaled oligonucleotide against IL-4Rα; also blocks IL-13 (AIR645)
Humanized blocking IL-5 antibody (mepolizumab)
IL-5α receptor monoclonal antibody (MEDI-563)
Blocking IL-13 monoclonal antibody (CAT-354 and others)
Small-molecule antagonists (SCH527123)
Reduced allergen responses in asthma; in clinical trials
Clinical development
Effective in allergen challenge; in clinical development
Effective in severe asthma with sputum eosinophilia and exacerbations; in clinical trials
Effective in phase II studies; in clinical trials
Clinical studies in severe asthmas so far negative
Phase II studies; for severe asthma
Target
Phosphodiesterase-4
p38 MAP kinase
Inhibitor of NF-κBkinase-2
Phosphoinositide-3 kinase
Roflumilast
SB236063
AS602868
CAL-101
Inhibitor (example) Development
Advanced development for COPD; early clinical studies in asthma
Several in early clinical development, including inhaled drugs
Early clinical development
δ-isoenzyme inhibitor in clincal trials for asthma
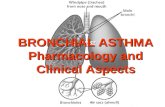
Lipid Mediator Inhibitors(A) Several lipid mediators are involved in asthma. Arachidonic acid is generated from membrane lipids by cytoplasmic or secretory phospholipase A2 (cPLA2, sPLA2). 5′ Lipoxygenase (5′ LO) generates leukotrienes (LT), including LTB4, which acts on BLT1 receptors, and cysteinyl leukotrienes (LTC4, LTD4, LTE4), which act on cysLT1 receptors and to a lesser extent on cysLT1 receptors. Cyclooxygenases (COX1 and COX2) generate prostaglandins (PGs) and thromboxane (Tx). PGD2 acts on DP1, DP2 (also known as CRTH2), and TP receptors. Inhibitors and receptor antagonists that may be beneficial in asthma are shown in white boxes.(B) PGD2 may play an important role in asthma. It is synthe-sized mainly in mast cells by PDGD synthase (PGDS) and acts on DP1 receptors on vessels to mediate vasodilatation and on dendritic cells to enhance their activation. PGD2 also acts via DP2 receptors (CRTH2) to attract Th2 lymphocytes and eosinophils and on TP receptors to cause bronchoconstriction. Antagonists of DP1, DP2 receptors, and inhibitors of PGDS are now in clinical development for asthma therapy.
DP
1 antagonist
CyaLT
1 antagonistC
yaLT2 antagonist
BLT1 antagonist
DP
2 antagonist
(CRTH
2 antagonist)TP
antagonist
EP1-4 CysLT1 CysLT2 BLT1TPDP2DP1
Membrane phospholipids
PLA2
PGDS
5 LOCOX2
Arachidonic acid
PGD2 TxA2
PGH2 LTA2
PGE2 CysLT LTB4
B
A
Mast cell
Th2 cell Eosinophil Airway smoothmuscle cell
Dendriticcell
Bronchialvessel
PGDS inhibitors
CRTH2antagonist TP antagonistDP1 antagonist
DP1 DP1 DP2 DP2 TP
cPLA2/sPLA2 inhibitors
5′ LO inhibitorsFLAP inhibitors
New “Dissociated” CorticosteroidsDevelopment of “dissociated” steroids is based on the dissociation of the side-effect mechanisms from the anti-inflammatory mechanisms of corticosteroids. This is theoretically possible because side effects are largely mediated via transactivation and binding of glucocorticoid receptor (GR) dimers to glucocorticoid response elements (GREs) in the promoter region of target genes, resulting in gene activation. However, anti-inflammatory effects are largely mediated via transrepression of transcription factors through a nongenomic effect whereby GR monomers interact with coactivator molecules, such as NF-κB and CBP, with recruitment of histone deacetylase 2 (HDAC2). Dissociated steroids or selective glucocorticoid receptor activators (SEGRAs) have a greater effect on the transrepression than transactivation and may therefore have a better therapeutic ratio. However, some of the anti-inflammatory effects of corticosteroids may be due to transactivation of anti-inflammatory genes, such as MAP kinase phosphatase-1 (MKP-1), so SEGRAs may not be as efficacious as existing drugs. New corticosteroid options include flutica-sone furoate, characterized by longer duration of action due to a higher affinity for GR and longer receptor retention; cicleso-nide, a prodrug that is converted to the active form by esterases in the lower airways, giving reduced systemic absorption from the lungs; and AL-438 and ZK-216438, nonsteroidal SEGRAs with reduced gene activation effects in vitro, now in clinical development.
Anti-inflammatoryproteins
(e.g., MKP-1)
DNA bindingtrans-activation
histone acetylation
Side effects(metabolic,endocrine)
Inflammatory proteins(cytokines, enzymes,
adhesion molecules, etc.)
CorticosteroidsDissociated
steroidGLUCOCORTICOID RECEPTORS
GRα
Inhibition oftranscription factorsNF-κB, AP-1, etc.trans-repression
histone deacetylation
NF-κBGR dimer
GRE GR monomer
HDAC2
BronchodilatorsActivation of β2 adrenoceptors (β2AR), vasoactive intestinal peptide (VIP), and prostaglandin E2 (PGE2) receptors results in activation of adenylyl cyclase (AC) via a stimulatory G protein (Gs) and an increase in 3′-5′ cyclic adenosine monophosphate (cAMP). This activates protein kinase A (PKA), which then phosphorylates several target proteins, resulting in the opening of calcium-activated potassium channels (KCa) or Maxi-K channels, decrease in phosphoinositide (PI) hydrolysis, increase in sodium/calcium ion (Na+/Ca2+) exchange, increase in Na+/K+ ATPase activity, and decrease in myosin light chain kinase (MLCK) activity, leading to relaxation of airway smooth muscle. β2AR may also be coupled directly to KCa via Gs. cAMP is degraded by phosphodiesterases (PDEs) that are inhibited by theophylline and selective PDE3 inhibitors.
Current bronchodilators are inhaled β2AR agonists, both short acting (salbutamol, terbutaline) and long acting (formoterol, salmeterol), and theophylline. New bronchodilators are once-inhaled daily β2AR agonists (indacaterol, carmoterol, GW-642444, and BI-1744), once-daily anticholinergics (tiotropium, glycopyrrolate, daratropium, and aclidinium), PGE2, potassium channel openers, vasoactive intestinal peptide analogues (Ro 25-1553), and PDE3 inhibitors. Smooth muscle myosin inhibitors are currently in development.
K+
Ca2+ channelK+ channel
PI/Ca2+
ATPcAMPAMPPDE
MLCK
GS
PKA
PGD2
AC
K+ channelopeners
β2 AgonistVIP
PGE2
β2AR
TheophyllinePDE3 inhibitors
Bronchodilatation
Smooth musclemyosin inhibitors
Asthma Poster:Compounds Available
from Tocris
API-2, 1EBIO
Celecoxib, SC 560
Adenosinereceptors
Adrenergic b2 receptors
Fexofenadine
Amthamine, Tiotidine
Imetit, Thioperamide
Glucocorticoidreceptors
Chemokinereceptors
Histaminereceptors
H1 receptor
H2 receptor
H3 receptor
4-Methylhistamine,JNJ 10191584
H4 receptor
SignalTransduction
AKT
COX
740 Y-P, LY 294002PI3K
AACOCF3, YM 26734PLA2
MG 132, Celastrol, IKK 16NF-kB
MAPK
CGS 21680, 2-CI-IB-MECA,SCH 58261, ZM 241385, MRS 1754
ICI 118,551, Salmeterol,Formoterol
Corticosterone,Fluticasone
RS 504393, C 021 dihydro-chloride, SB 328437,UCB 35625, SB 265610
Prostanoidreceptors
SC 51089, L-161,982, Prostaglandin E2, U 46619, MK 571
VIP receptors VIP (6-28) (Human, rat, porcine, bovine)
VIP (Human, rat, mouse, rabbit, canine, porcine)
SB 239063, Anisomycin,SP 600125
PDE Cilostamide, Zardaverine,Theophpylline, Rolipram
Nitric Oxide Nw-Propyl-L-arginine,1400W, L-NAME,BYK 181023
Leukotriene receptors
MK 886, BAY-u 9773,MK 571, Leukotriene B4
K+ channels Iberiotoxin, 1-EBIO
Cytokines and Cytokinereceptors
Gabexate, Thalidomide, Pirfenidone, GIT 27,YM 90709
Adenosinereceptors Fexofenadine
Amthamine, TiotidineImetit, Thioperamide
Histamine receptorsH1 receptor
H2 receptor
H3 receptor
4-Methylhistamine,JNJ 10191584
H4 receptor β2 Adrenoceptors
Glucocorticoidreceptors
Chemokinereceptors
Prostanoidreceptors
VIP receptorsSignal Transduction
Signal Transduction
API-2, 10-DEBCCelecoxib, SC 560
AKT
COX
MG 132, Celastrol, IKK 16NF-κB
MAPK SB 239063, Anisomycin,SP 600125
740 Y-P, LY 294002PI3K
AACOCF3, YM 26734PLA2
PDE Cilostamide, Zardaverine,Theophylline, Rolipram
Nitric Oxide Nω-Propyl-L-arginine,1400W, L-NAME,BYK 191023
Leukotrienereceptors
K+ channels
Cytokines andcytokine
receptors
Compounds Acting on Asthma Pathways Available fromCGS 21680, 2-CI-IB-MECA,SCH 58261, ZM 241385,MRS 1754
ICI 118,551, Salmeterol,Formoterol
Corticosterone,Fluticasone
RS 504393, C 021,SB 328437, UCB 35625, SB 265610
Gabexate, Thalidomide, Pirfenidone, GIT 27,YM 90709
MK 886, BAY-u 9773,MK 571, Leukotriene B4
SC 51089, L-161,982,Prostaglandin E2, U 46619,MK 571
VIP (6-28), VIP
Iberiotoxin, 1-EBIO
Asthma is now one of the most common chronic diseases in the world, affecting over 300 million people, and its prevalence is rising, particularly in develop-ing countries. Chronic inflammation of the airways results in airway hyperresponsiveness (AHR), which makes the airways “twitchy” and causes them to constrict more easily than normal in response to different triggers, such as exercise, cold air, and exposure to allergens and irritants. The inflammation may be worsened by exposure to allergens and by upper respiratory tract virus infections, and it may activate sensory nerves of the airways, resulting in coughing and chest tightness. Asthma symptoms are intermittent and rarely progress. Patients may have differing degrees of severity, ranging from mild intermittent symptoms to severe symptoms and disability.
In the past, asthma was viewed as a disease of bronchoconstriction and treated predominantly with bronchodilators. Current therapy for asthma depends on the severity of the condition and is increased in a stepwise manner until asthma control is achieved. Inhaled corticosteroids (ICS) are the mainstay of treat-ment in all patients with persistent asthma, and long-acting β2 agonists (LABAs) are added in moderate cases. In severe asthma, other add-on therapies may be necessary, and in very severe asthma, anti-IgE and immosuppressants may be used. Additionally, combination inhalers (corticosteroid + LABA) are now commonly prescribed to control asthma since they are more convenient for patients, simplify treatments, improve compliance, and, very importantly, prevent the use of LABAs alone, which is potentially dangerous.
Nonetheless, it is now clear that asthma is a complex chronic inflammatory disease of the airways with many potential therapeutic targets, and treatment of the inflammation is now considered to be the key to successful control of symptoms. There is also a real need for new asthma treatments due to poor compliance with current treatments, side effects outside the lungs for the current inhaled treatments, patients’ preference for oral therapy, difficulty in treating severe asthma, and current unavailability of disease-modifying and curative treatments. Here, the focus is placed on new asthma treatment options that are being developed as the understanding of cellular pathways involved in the disease increases.
INTRODUCTION
Current therapy for asthma with ICS and inhaled LABA is highly effective, safe, and relatively inexpensive, but many patients’ symptoms remain poorly controlled, and severe asthma remains difficult to control with current treatments. Some innovative strategies and cutting-edge issues in asthma research and therapy include the following: developing selective therapies for subphenotypes via yet-to-be-identified discriminatory biomarkers and genetic profiling; treating patients with severe asthma who are relatively corticosteroid resistant by restoring HDAC2 activity via low doses of theophylline; developing an effective oral therapy for patients with mild and moderate disease; and using genetic and pharmacogenomic information to improve understanding of the biology of asthma to develop treatments.
None of the currently available treatments for asthma have long-term effects on airway inflammation or remodeling, and therefore they are not disease modifying or curative. The prospects for a cure seem remote until the molecular and genetic causes of asthma are better understood, but there is a possibility that vaccination approaches have the potential to reverse the abnormal inflammation found in asthma. However, the long-term consequences of these approaches need to be carefully evaluated, particularly as they would probably need to be applied in children at the onset of disease.
CONCLUSION AND FUTURE DIRECTIONS
Further ReadingAdcock, I.M., et al. (2006). Kinase inhibitors and airway inflammation. Eur. J. Pharmacol. 533, 118–132.
Adcock, I.M., et al. (2008). New targets for drug development in asthma. Lancet 372, 1073–1087.
Barnes, P.J. (2006). How corticosteroids control inflammation. Br. J. Pharmacol. 148, 245–254.
Barnes, P.J. (2010). New therapies for asthma: Is there any progress? Trends Pharmacol. Sci. doi:10.1016/j.tips.2010.04.009.
Barnes, P.J. (2008). Cytokine networks in asthma and chronic obstructive pulmonary disease. J. Clin. Invest. 118, 3546–3556.
Barnes, P.J., et al. (2009). Glucocorticoid resistance in inflamma-tory diseases. Lancet 342, 1905–1917.
Broide, D.H. (2009). Immunomodulation of allergic disease. Annu. Rev. Med. 60, 279–291.
Cazzola, M., et al. (2009). Emerging inhaled bronchodilators: An update. Eur. Respir. J. 34, 757–769.
Chung, K.F. (2006). Phosphodiesterase inhibitors in airways disease. Eur. J. Pharmacol. 533, 110–117.
Holgate, S.T., et al. (2008). Treatment strategies for allergy and asthma. Nat. Rev. Immunol. 8, 218–230.
New Therapies, Challenges,and Breakthroughs in Asthma
Peter J. BarnesNational Heart and Lung Institute, Imperial College London School of Medicine, Dovehouse Street, London SW3 6LY, UK
To obtain copies of this poster, please visit TOCRIS at www.tocris.com
C
M
Y
CM
MY
CY
CMY
K
TiPs_Tocris2_Asthma_cs3_RESIZED.pdf 6/2/2010 4:56:53 PM